")
Back to Journals » Clinical Ophthalmology » Volume 18
A 6-Month Follow-Up Comparative Study of Single-Step Transepithelial Photorefractive Keratectomy (Trans-PRK) Using the StreamLight Software with and without Epithelial Thickness Customization
Authors Aramberri J, Lauzirika G , Illarramendi I, Mendicute J
Received 27 August 2024
Accepted for publication 30 September 2024
Published 9 October 2024 Volume 2024:18 Pages 2831—2841
DOI https://doi.org/10.2147/OPTH.S487627
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jaime Aramberri,1,2 Gorka Lauzirika,1,3 Igor Illarramendi,1 Javier Mendicute1,4
1Anterior Segment Department, Miranza Begitek, Donostia-San Sebastián, Spain; 2Anterior Segment Department, Miranza Ókular, Vitoria-Gasteiz, Spain; 3R&D Department, Miranza Group, Barcelona, Spain; 4Ophthalmology Service, Hospital Universitario Donostia, Donostia-San Sebastián, Spain
Correspondence: Gorka Lauzirika, Miranza Begitek, Plaza Teresa Calcuta 7, Donostia-San Sebastián, 20012, Spain, Email [email protected]
Purpose: To compare corneal aberrometry, densitometry, and refractive outcomes of single-step Transepithelial Photorefractive Keratectomy (Trans-PRK) with and without epithelial thickness customization.
Patients and Methods: This was a prospective, interventional, randomized controlled study. Patients undergoing Trans-PRK using the WaveLight EX500 laser with StreamLight software (Alcon Laboratories, Forth Worth, TX, USA) were randomly assigned to control (55 μm standard epithelial thickness) or customized (thinnest point of epithelial thickness for each patient) groups. MS-39 (CSO, Italy) anterior segment optical coherence tomography was used to measure the epithelial thickness. Inclusion criteria were spherical equivalent < 6 diopters (D), astigmatism < 4D, and CDVA 20/25 or better. The assessments were at baseline and 6 months post-op: visual acuity, refraction, aberrometry, and corneal densitometry.
Results: 108 eyes were enrolled, [control group (n=56) and customized group (n=52)]. Mean epithelial ablation thickness in the customized group was 54.81± 3.56μm (p=0.470 vs control group). Both groups experienced significant postoperative increases in higher-order aberrations (HOA) and spherical aberrations, with no significant intergroup differences. Mean HOA RMS (μm) of the frontal cornea and total cornea increased by 0.27, and 0.29, respectively, in the control group, and 0.26 and 0.28, respectively, in the customized group (p< 0.001 for all). Mean change in spherical aberrations in the frontal cornea and total cornea was 0.23μm (p< 0.001) and 0.25μm (p< 0.001), in the control group, and 0.19μm (p< 0.001) and 0.20μm (p< 0.001), in the customized group. Mean corneal densitometry in anterior cornea decreased by 0.63GSU (p=0.021) and 1.18GSU (p< 0.001) in the control and customized groups. In the posterior cornea, it increased by 1.67GSU (p=0.004) and 0.38GSU (p=0.006).
Conclusion: No significant differences in refractive and aberrometry outcomes between control and customized Trans-PRK groups, with corneal densitometry changes not affecting visual acuity.
Keywords: Trans-PRK, corneal epithelial thickness, corneal aberrometry, corneal densitometry, corneal refractive surgery
Introduction
Transepithelial photorefractive keratectomy (Trans-PRK), initially introduced by Alió et al in the early 1990s,1 gained considerable recognition following research conducted by Aron-Rosa et al2 and Gimbel et al3,4 This technique was introduced as an alternative to conventional PRK, and involves ablation of the corneal epithelium and stroma in a single step using an excimer laser, effectively eliminating the need for mechanical or chemical debridement.4 Notably, Trans-PRK has shorter surgical time, reduced postoperative pain, accelerated wound healing, and faster recovery in comparison to conventional PRK, while maintaining comparable visual and refractive outcomes.5,6 Similarly, studies have demonstrated that Trans-PRK is a safe, effective, and predictable alternative to LASIK (laser-assisted in-situ keratomileusis).7,8 It eliminates the need for creating a corneal flap and provides greater stability in postoperative corneal biomechanics.
The discovery of non-uniform thickness in the epithelium has significant implications for corneal refractive surgery. The average central thickness of the epithelium is 53.4 µm, with variations observed in different regions. The inferior region is found to be 5.7 µm thicker than the superior region, and the nasal region is 1.2 µm thicker than the temporal region.9–11 The utilization of a standard epithelial ablation protocol may result in excessive stromal ablation in specific eyes or corneal regions, irrespective of the epithelial mapping. Conversely, in other eyes or corneal areas, insufficient epithelium removal may occur.12 Therefore, understanding epithelial thickness is crucial because it affects the surgical planning and outcomes. Anterior Segment Optical Coherence Tomography (AS-OCT) provides consistent and reliable information on epithelial thickness.13 By incorporating this information, surgeons can make more informed decisions regarding the surgical procedure, including determining the appropriate depth of ablation and managing post-operative outcomes.
The aim of this study was to compare corneal aberrometry, corneal densitometry, and visual and refractive outcomes of single-step Trans-PRK using the WaveLight EX500 excimer laser with the StreamLight software (Alcon Laboratories), with and without epithelial thickness customization.
Materials and Methods
Study Design and Patients
A prospective, interventional, and randomized controlled study was performed to evaluate surgical outcomes of single-step Trans-PRK with and without epithelial thickness customization. The study participants were enrolled from October 2021 to November 2022 at Miranza Begitek clinic at Donostia-San Sebastián, Spain. The study adhered to the principles of the Declaration of Helsinki and institutional review board approval was granted (code: STREAM21) by Instituto de Microcirugía Ocular (IMO Miranza Barcelona). Moreover, the purpose of the study and policy on the protection of personal data were explained in detail to all participants, and informed consent was obtained.
Consecutive patients undergoing Trans-PRK that met the following criteria were included: simple and compound myopic astigmatism, spherical equivalent (SE) less than 6 diopters (D), astigmatism less than 4 D, older than 20 years of age, and a corrected distance visual acuity better than or equal to 0.8 decimal (20/25 Snellen equivalent). Patients with ophthalmological pathologies or previous surgeries were excluded from the study. Patients were randomized into two groups: the control group, with a 55 µm standard epithelial ablation, and the customized group, with epithelial thickness ablation customized to the thinnest point of epithelial thickness for each patient for the entire optical zone measured by MS-39 anterior segment optical coherence tomography (CSO, Italy) device.
Baseline and Postoperative Assessment
All patients underwent examination at preoperative and 6-month postoperative visits, including: uncorrected distance visual acuity (UDVA) and corrected distance visual acuity (CDVA); subjective refraction with (only at preoperative visit) and without cycloplegia with Snellen chart (decimal notation) in photopic conditions. Anterior and total corneal aberrations as well as corneal densitometry were measured using the Pentacam AXL device (Oculus Optikgeräte GmbH, Wetzlar, Germany) without room light in scotopic conditions. Corneal densitometry for quantitative evaluation of corneal light backscattering was measured over concentric annular areas (0–2 mm, 2–6 mm, 6–10 mm, 10–12 mm, and total diameter) the anterior layer (anterior 120 µm), central layer (from the first 120 µm to the posterior 60 µm), and posterior layer (posterior 60 µm), and total corneal depths. Densitometry values were expressed in standardized grayscale units (GSU). The GSU scale is calibrated by proprietary software, which defines a minimum light scatter of 0 (maximum transparency) and maximum light scatter of 100 (minimum transparency).14
Data collected from anterior and total corneal aberration measurements included the root mean square (RMS) of total and higher-order aberrations (HOA), the vertical and horizontal coma, and the spherical aberration at 6 mm corneal diameter.
Surgical Protocol
The Trans-PRK were carried out using the WaveLight EX500 excimer laser equipped with StreamLight software (Alcon Laboratories, Forth Worth, TX, USA). In both groups, the procedure began with wavefront-optimized epithelial ablation, followed by a brief 10-second pause (as recommended by the manufacturer) to allow for corneal cooling before transitioning to stromal treatment, which was performed over a 6.5 mm optical zone to complete the procedure.6,15 For the control group, a standardized epithelial ablation depth of 55 µm was applied across all patients. In the customized group, the epithelial ablation depth was adjusted based on the thinnest point of epithelial thickness, which had been measured by MS-39 (CSO, Italy) anterior segment optical coherence tomography. To prevent haze, a 0.02% mitomycin-C (MMC) solution was topically administered on the stromal bed for a duration of 40 seconds when the central stromal ablation exceeded 65 μm.16 Finally, a soft bandage contact lens (LC Balafilcon A, PureVision, Bausch & Lomb, Rochester, New York, USA) was placed for three to four days until epithelialization was achieved. Meanwhile, patients received ciprofloxacin eye drops (Oftacilox, Alcon Cusí, S.A)., four times daily, and artificial tears. Then, the patients initiated treatment with fluorometholone 0.1% eye drops, applying them four times daily and gradually reducing the frequency over a period of four weeks.
Statistical Analysis
The data were collected in a Microsoft Excel (Microsoft, Redmond, USA) spreadsheet and were analyzed using SPSS 22.0 software (SPSS Statistics, Version 22.0, IBM Corp., Armonk, NY, USA). For such analysis, only one eye per patient was selected (right eye) in order to avoid the bias associated to the inclusion of both eyes from the same patient in the analysis. Quantitative variables were described using mean and standard deviation (SD). Difference between group means was evaluated by Mann–Whitney U and Wilcoxon signed-rank test. A value of p<0.05 was considered statistically significant.
Results
Demographics
One-hundred and eight eyes of 108 patients were enrolled: 56 eyes (51.85%; mean age 36.90±6.90 years) in the control group and 52 eyes (48.15%; mean age 34.90±8.35 years) in the customized group. There was no statistically significant difference (p=0.470) in mean epithelial ablation thickness in both groups (55 µm and 54.81±3.56 µm in the control and customized group, respectively). Baseline sphere, cylinder, and spherical equivalent, as well as frontal and total corneal HOA, were similar between groups. There was a statistically significant difference (p=0.001) in baseline CDVA between groups. Patient characteristics at baseline are detailed in Table 1.
 |
Table 1 Patient Demographic and Baseline Ocular Characteristics |
Visual and Refractive Outcomes
Postoperatively, mean UDVA (decimal notation) was 1.09±0.18 in the customized group and 1.07±0.23 in the control group with no significant difference between the groups (p=0.760). Postoperative UDVA of 20/20 or better was seen in 85% of the eyes in the customized group and 77% of the eyes in the control group, compared to 88% and 89%, respectively, with preoperative CDVA of 20/20 or better (Figure 1).
 |
Figure 1 Visual outcome- Standard graphs: (A) and (B) represents cumulative distribution of visual acuity; (C) and (D) represents changes in lines of visual acuity. |
The gain/loss of VA lines was similar in both groups. CDVA remained the same in 29 eyes (57%) in the customized group and in 27 eyes (48%) in the control group. There was a gain of VA lines in 23 eyes (44%) in the customized group and 29 eyes (52%) in the control group. No eyes lost lines of CDVA (Figure 1).
Figure 2 shows the refractive outcomes in both groups; similar refractive accuracy regarding spherical equivalent and astigmatism was observed between both groups.
 |
Figure 2 Refractive outcome- Standard graphs: (A) and (B) represents attempted vs achieved spherical equivalent line regression; (C) and (D) represents the ranges of percentage of postoperative spherical equivalent; and (E) and (F) represents the percentage of postoperative cylinder. |
Corneal Aberrometry
Regarding frontal corneal aberrations, there was a significant postoperative increase in HOA in both groups (p<0.001), from 0.39±0.11 µm to 0.66±0.18 µm and from 0.37±0.11 µm to 0.63±0.18 µm in the control and customized group, respectively. This increment was mainly due to an increase in spherical aberration in both groups, from 0.25±0.07 µm to 0.48±0.14 µm (p<0.001) and from 0.26±0.10 µm to 0.45±0.13 µm (p<0.001) in the control and customized group, respectively. Likewise, there was an increase in horizontal coma only in the customized group, from −0.02±0.12 µm to 0.07±0.24 µm (p=0.003). On the contrary, there was a decrease in vertical coma in the control group, from −0.01±0.17 µm to −0.07±0.25 µm (p=0.013) (Table 2).
 |
Table 2 Patient Pre- and Postoperative Aberrations of A) Frontal and B) Total Cornea |
Regarding total corneal aberrations, changes were similar to those observed in frontal cornea. There was an increase in HOA and spherical aberrations in both groups. HOA increased from 0.38±0.14 µm to 0.67±0.20 µm (p<0.001) and from 0.36±0.12 µm to 0.64±0.20 µm (p<0.001) in the control and customized group, respectively. Spherical aberration increased from 0.20±0.08 µm to 0.45±0.15 µm (p<0.001) and from 0.22±0.11 µm to 0.42±0.14 µm (p<0.001), respectively. A decrease in vertical coma in the control group from −0.05±0.17 µm to −0.11±0.27 µm (p=0.016) and an increase in horizontal coma in the customized group from −0.02±0.11 µm to 0.08±0.26 µm (p=0.004) were noticed (Table 2).
Corneal Densitometry
Table 3 and Figure 3 show baseline and postoperative densitometry values for both groups. In the anterior cornea, the mean corneal densitometry (CD) decreased by 0.63 GSU (p=0.021) in the control group and 1.18 (p<0.001) in the customized group. In posterior cornea, the mean CD increased by 1.67 GSU (p=0.004) and 0.38 GSU (p=0.006), respectively.
 |
Table 3 Patient Pre- and Postoperative Corneal Densitometry Values |
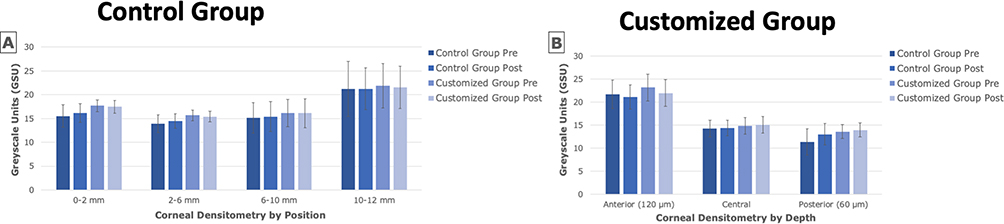 |
Figure 3 Corneal densitometry results. (A): according to corneal rings position. (B): according to depth. |
The customized group showed marginally higher CD values in 0–2 mm and 2–6 mm regions in anterior, central, posterior, and total cornea. In the control group, a small (not clinically significant) but statistically significant decrease in the 6–10 mm concentric area of the anterior cornea (120 µm) was observed, along with a decrease in total anterior densitometry. Conversely, there was a small significant increase in all concentric areas of the posterior cornea (60 µm) and in the total posterior densitometry. Interestingly, there were no significant changes observed in the central cornea (Table 3). However, in the customized group, all concentric areas of the anterior cornea, except for 10–12 mm, exhibited a significant decrease. In the posterior cornea, there was a slight increase in densitometry in the 2–6 mm, 6–10 mm, and total diameter areas. The central cornea did not show significant change, while in the total thickness aberrometry, only the 2–6 mm region showed a small significant reduction (Table 3).
Discussion
To the best of our knowledge, this is the first study that compares the refractive, HOA, and corneal densitometry outcomes of single-step Trans-PRK using the WaveLight EX500 excimer laser with StreamLight software (Alcon Laboratories, Forth Worth, TX, USA) with and without epithelial thickness customization. Trans-PRK eliminates the need for mechanical epithelial scraping or chemical debridement using dilute ethanol.4,5 This could result in a less painful postoperative period, quicker re-epithelialization, and the avoidance of any complication related to traditional epithelial debridement.4,6,17 As mentioned before, understanding the epithelial thickness is crucial in corneal refractive surgery as it has an impact on surgical planning and outcomes.9–11,18 Theoretically, performing customized Trans-PRK by measuring the individual’s epithelial thickness could lead to improved outcomes. In that regard, the study aimed to evaluate the surgical outcomes of Trans-PRK with and without epithelial thickness customization. Instead of relying on the standard 55 µm thickness, a patient-specific approach was employed (54.81±3.56 µm) to observe if this led to better results.
Laser refractive surgery involves removing part of the corneal stroma, which reduces corneal thickness. The alteration in corneal shape primarily manifests as displacements of the front and back surfaces of the cornea. Meanwhile, changes in the refractive capacity can mainly be observed through wavefront aberrations induced following conventional laser refractive surgery. Essentially, the displacement can be translated into aberrations.19
The current study assessed corneal aberrations as an indicator of corneal optical quality. Both the control and customized groups exhibited a significant increase in HOA and spherical aberrations postoperatively on total and frontal corneal aberrometry, as expected from the findings of previous studies.7,20 Zhang et al documented a comparable preoperative total corneal HOA value of 0.40 µm, which aligns with our findings of 0.38±0.14 µm and 0.36±0.12 µm.7
Preoperative vertical and horizontal coma as well as spherical aberration in our study were also consistent with the findings of Zhang et al. In contrast, our study demonstrated a significantly lower total corneal HOA at 6 months after the surgery, with values of 0.67±0.20 µm and 0.64±0.20 µm for the control and customized groups, respectively, compared to 1.04 µm in their study. A similar difference is also observed in terms of postoperative spherical aberration and vertical coma. This can be explained by the difference in degree of preoperative myopia, as in our study we included patients who had a mean spherical equivalent of −3.64±1.37D and −3.63±1.56 D vs −7.59 ± 0.84 D in Zhang et al’s study. Another possible explanation is that prior to laser ablation, a wet sponge was used to wipe the corneal surface to prevent uneven wetting, and thus, uneven ablation. However, both studies showed similar levels of horizontal coma at the 6-month mark.7
When anterior corneal aberrations were compared to total corneal aberrations, we found that the mean change of HOA RMS in frontal cornea was similar to the mean change of HOA RMS in total cornea for both groups (0.27 µm vs 0.29 µm, respectively, in control group and 0.26 µm vs 0.28 µm, respectively, in customized group). Similar findings were observed for vertical and horizontal coma, as well as spherical aberration.
In a finite element model of the human eye, the biomechanical effects-induced aberrations after conventional laser refractive surgery were primarily a combination of defocus and primary spherical aberrations.19 This pattern aligned with the findings related to the anterior corneal surface. Notably, the aberrations introduced by the posterior corneal surface were less impacted compared to those from the anterior surface. Nevertheless, there was evidence of a partially compensatory mechanism between the wavefront aberrations induced by the posterior corneal surface and those induced by the anterior corneal surface. This observation suggests that the refractive shift generated by the excimer laser occurs on the anterior surface of the cornea, so the pattern of changes in the HOAs is similar between frontal surface and total corneal thickness, as observed in our study.
The results of this study suggest that Trans-PRK surgery induces changes in corneal aberrations regardless of whether epithelial thickness customization is performed. However, it is important to note that the customized group showed an increase in horizontal coma, while the control group exhibited a decrease in vertical coma. These aberration changes have implications for visual quality and should be considered in the post-operative management and optimization of Trans-PRK outcomes.
Corneal densitometry (CD) values, used to assess corneal transparency and optical density, can change significantly after corneal refractive surgery including PRK,21 affecting the overall visual quality.14,22 Accordingly, by monitoring and analyzing CD, healthcare professionals can gain valuable insights into the impact of corneal refractive surgery on corneal health and visual outcomes.22 Corneal densitometry allows us to assess corneal haze following PRK.21 In Trans-PRK, the cornea is exposed to laser ablation for a longer period of time than in conventional PRK, which hypothetically can cause corneal inflammation and scarring, reducing corneal transparency. Significant differences in corneal densitometry following Trans-PRK were observed in our study: the control group had lower postoperative densitometry in the central regions (0–2 mm and 2–6 mm regions). However, this did not affect postoperative UDVA, which did not show significant differences between both groups.
Currently, there are no universally established benchmarks for CD due to variations influenced by factors such as ethnicity and age.22 One significant study conducted in Belgium provides insights into CD measurements, reporting a total CD value of 19.74 GSU for the entire 12-mm area.14 In our study, preoperatively, the control group exhibited a mean total CD of 15.78±2.35 GSU, while the customized group showed a mean total CD of 17.21±1.95 GSU. Additionally, the Belgian study found that the anterior cornea displayed the highest CD, which aligns with the findings of our study. Previous studies have mentioned that CD typically increases after PRK.23,24 However, in our study, only the posterior cornea showed an increase in CD, which contrasts with the findings of Montorio et al, where an increase in CD in the anterior cornea was observed with no significant change in CD in posterior layers.24 Notably, Montorio et al’s study was performed on patients that underwent PRK more than 22 years before the study. Instead, the present study revealed a decrease in the CD values of the anterior cornea and an increase in the posterior cornea. This phenomenon can be explained by several factors related to the corneal structure and healing processes. Firstly, the anterior cornea experiences a more pronounced healing response due to the larger wound area caused by Trans-PRK. This leads to increased epithelial-stromal interactions and the presence of myofibroblasts, which aid in tissue remodeling.25 The anterior stroma’s structure, with undulating and interwoven collagen bundles, supports this healing process, helping maintain or even improve transparency.26 In contrast, the posterior cornea, especially in higher myopic corrections, may respond less favorably. Differences in the behavior of keratocytes between the anterior and posterior cornea make the posterior keratocytes more susceptible to transformation into myofibroblasts, which can increase light scatter.25 This transformation may explain the worsening posterior CD values after surgery. The posterior cornea’s orthogonally arranged collagen lamellae, which are less cohesive, may be more vulnerable to disorganization, further contributing to increased light scatter.27 Additionally, the natural decrease in the corneal refractive index from anterior to posterior plays a role in these observations.28 The anterior stroma scatters twice as much light as the posterior, making improvements in anterior densitometry more noticeable. Conversely, the posterior stroma, with its lower scatter and structural differences, may recover transparency more slowly, leading to a decline in CD values.29
Secondly, swelling patterns also differ between the anterior and posterior stroma. Swelling primarily occurs in the posterior-anterior direction,27 with the anterior cornea experiencing the least swelling due to its lower hydrophilicity.30–32 This resistance to swelling in the anterior stroma may help preserve its transparency post-surgery. Factors like the extent of attempted correction (especially in higher myopic treatments), patient age, and the structural differences between anterior and posterior stroma likely contribute to these empirical observations.25 Overall, the differential healing capacities and structural organization of the cornea account for the improved anterior CD values and worsened posterior CD values after Trans-PRK.
To further explain the improvement in anterior CD values, it is important to consider the role of MMC, which was used in cases where central stromal ablation exceeded 65 μm. MMC primarily affects the anterior keratocytes, reducing scar formation and potentially enhancing transparency in the anterior stroma.16 This could explain the significant improvement in anterior CD values after Trans-PRK. However, because MMC does not impact the deeper posterior layers of the cornea, the worsening of posterior CD could be unrelated to its use. Lastly, it is possible that these effects, particularly the increase in posterior CD, could decrease over time as the cornea continues to heal. Further long-term studies are needed to evaluate the impact of refractive surgeries on both anterior and posterior CD values and to assess whether the changes observed in the posterior cornea are temporary or sustained over longer follow-up periods.
Contrary to the initial hypothesis that a customized Trans-PRK approach would result in superior outcomes compared to the standard thickness profile of 55 µm, the observed variations in epithelial thickness did not lead to statistically significant differences in the outcomes between the two groups regarding corneal densitometry, higher-order aberrations, and visual and refractive outcomes.
Conclusions
Overall, the study aimed to provide in-depth insights into the impact of epithelial customization approach on various outcome parameters, shedding light on its effectiveness in corneal refractive surgery. The results indicate that both control and customized groups experienced similar changes in corneal aberrations, suggesting that the surgical technique itself may have a more dominant influence on these parameters. However, corneal densitometry changes differed between the two groups, without affecting visual acuity. After Trans-PRK, anterior corneal densitometry improves due to a stronger healing response and structural differences in the anterior stroma. In contrast, posterior densitometry worsens, likely due to the cornea’s less cohesive lamellar structure and increased light scatter. These structural factors contribute to the differential healing between anterior and posterior cornea. These findings emphasize that single-step Trans-PRK with and without customization of the thickness of epithelial ablation is safe, effective, and repeatable, highlighting the need for further research and optimization to enhance surgical outcomes and patient satisfaction.
Acknowledgments
The authors would like to thank everyone at Miranza Begitek who helped with data collection as well as GP Communications for support with the medical writing.
Funding
This study was partially funded by a Medical Writing Grant (no. 87398601) from Alcon. The results of the study and the revision of the manuscript were conducted independently of any influence from Alcon. Moreover, none of the authors have received payments from Alcon for this study.
Disclosure
Jaime Aramberri and Javier Mendicute are consultants to Alcon. Jaime Aramberri also reports personal fees from Alcon, Staar Surgical, Johnson and Johnson, Heidelberg Eng., and Schwind, outside the submitted work. The remaining authors have nothing to declare for this work. In addition, the authors have no financial or proprietary interests in the medical field or products involved in this manuscript.
References
1. Alio JL, Ismael MM, Artola A. Laser epithelium removal before photorefractive keratectomy. Refract Corneal Surg. 1993;9(5):395. doi:10.3928/1081-597X-19930901-16
2. Aron-Rosa DS, Colin J, Aron B, et al. Clinical results of excimer laser photorefractive keratectomy: a multicenter study of 265 eyes. J Cataract Refract Surg. 1995;21(6):644–652. doi:10.1016/S0886-3350(13)80560-3
3. Gimbel HV, DeBroff BM, Beldavs RA, Westenbrugge JA, Ferensowicz M. Comparison of laser and manual removal of corneal epithelium for photorefractive keratectomy. J Refract Surg. 1995;11(1):36–67. doi:10.3928/1081-597X-19950101-10
4. Adib-Moghaddam S, Soleyman-Jahi S, Moghaddam AS, et al. Efficacy and safety of transepithelial photorefractive keratectomy. J Cataract Refract Surg. 2018;44(10):1267–1279. doi:10.1016/j.jcrs.2018.07.021
5. Alasbali T. Transepithelial photorefractive keratectomy compared to conventional photorefractive keratectomy: a meta-analysis. J Ophthalmol. 2022;2022:3022672. doi:10.1155/2022/3022672
6. Gaeckle HC. Early clinical outcomes and comparison between trans-PRK and PRK, regarding refractive outcome, wound healing, pain intensity and visual recovery time in a real‐world setup. BMC Ophthalmol. 2021;21(1):1–9. doi:10.1186/s12886-021-01941-3
7. Zhang J, Feng Q, Ding W, Peng Y, Long K. Comparison of clinical results between trans-PRK and femtosecond LASIK for correction of high myopia. BMC Ophthalmol. 2020;20(1):1–10. doi:10.1186/s12886-020-01515-9
8. Chang JY, Lin PY, Hsu CC, Liu CJL. Comparison of clinical outcomes of LASIK, Trans-PRK, and SMILE for correction of myopia. J Chin Med Assoc. 2022;85(2):145–151. doi:10.1097/JCMA.0000000000000674
9. Reinstein DZ, Archer TJ, Vida RS. Epithelial thickness mapping for corneal refractive surgery. Curr Opin Ophthalmol. 2022;33(4):258–268. doi:10.1097/ICU.0000000000000867
10. Reinstein DZ, Silverman RH, Coleman DJ. High-frequency ultrasound measurement of the thickness of the corneal epithelium. Refract Corneal Surg. 1993;9(5):385–387. doi:10.3928/1081-597X-19930901-12
11. Reinstein DZ, Archer TJ, Gobbe M, Silverman RH, Coleman DJ. Epithelial thickness in the normal cornea: three-dimensional display with Artemis very high-frequency digital ultrasound. J Refract Surg. 2008;24(6):571–581.
12. Mosquera SA, Awwad ST. Theoretical analyses of the refractive implications of transepithelial PRK ablations. Br J Ophthalmol. 2013;97(7):905–911. doi:10.1136/bjophthalmol-2012-302853
13. Haque S, Jones L, Simpson T. Thickness mapping of the cornea and epithelium using optical coherence tomography. Optom Vis Sci. 2008;85(10):E963–E976. doi:10.1097/OPX.0b013e318188892c
14. Ní Dhubhghaill S, Rozema JJ, Jongenelen S, Ruiz Hidalgo I, Zakaria N, Tassignon MJ. Normative values for corneal densitometry analysis by scheimpflug optical assessment. Invest Ophthalmol Vis Sci. 2014;55(1):162–168. doi:10.1167/iovs.13-13236
15. Abdel-Radi M, Shehata M, Mostafa MM, Aly MOM. Transepithelial photorefractive keratectomy: a prospective randomized comparative study between the two-step and the single-step techniques. Eye. 2023;37(8):1545–1552. doi:10.1038/s41433-022-02174-4
16. Charpentier S, Keilani C, Maréchal M, et al. Corneal haze post photorefractive keratectomy. J Fr Ophtalmol. 2021;44(9):1425–1438. doi:10.1016/j.jfo.2021.05.006
17. Fadlallah A, Fahed D, Khalil K, et al. Transepithelial photorefractive keratectomy: clinical results. J Cataract Refract Surg. 2011;37(10):1852–1857. doi:10.1016/j.jcrs.2011.04.029
18. Asroui L, Dupps WJ, Randleman JB. Determining the utility of epithelial thickness mapping in refractive surgery evaluations. Am J Ophthalmol. 2022;240:125–134. doi:10.1016/j.ajo.2022.02.021
19. Fang L, Ma W, Wang Y, Dai Y, Fang Z. Theoretical analysis of wave-front aberrations induced from conventional laser refractive surgery in a biomechanical finite element model. Invest Ophthalmol Vis Sci. 2020;61(5):34. doi:10.1167/iovs.61.5.34
20. Al-Mohaimeed MM. Factors affecting single-step transepithelial photorefractive keratectomy outcome in the treatment of mild, moderate, and high myopia: a cohort study. Int J Ophthalmol. 2022;15(5):786–792. doi:10.18240/ijo.2022.05.15
21. Poyales F, Garzón N, Mendicute J, et al. Corneal densitometry after photorefractive keratectomy, laser-assisted in situ keratomileusis, and small-incision lenticule extraction. Eye. 2017;31(12):1647–1654. doi:10.1038/eye.2017.107
22. He Y, Ma BS, Zeng JH, Ma DJ. Corneal optical density: structural basis, measurements, influencing factors, and roles in refractive surgery. Front Bioeng Biotechnol. 2023;11:1144455. doi:10.3389/fbioe.2023.1144455
23. Cennamo G, Forte R, Aufiero B, La Rana A. Computerized scheimpflug densitometry as a measure of corneal optical density after excimer laser refractive surgery in myopic eyes. J Cataract Refract Surg. 2011;37(8):1502–1506. doi:10.1016/j.jcrs.2011.03.037
24. Montorio D, Cennamo G, Menna F, et al. Evaluation of corneal structures in myopic eyes more than twenty‐two years after photorefractive keratectomy. J Biophotonics. 2020;13(10):e202000138. doi:10.1002/jbio.202000138
25. Mohan RR, Hutcheon AEK, Choi R, et al. Apoptosis, necrosis, proliferation, and myofibroblast generation in the stroma following LASIK and PRK. Exp Eye Res. 2003;76(1):71–87. doi:10.1016/S0014-4835(02)00251-8
26. Radner W, Zehetmayer M, Aufreiter R, Mallinger R. Interlacing and cross-angle distribution of collagen lamellae in the human cornea. Cornea. 1998;17(5):537–543. doi:10.1097/00003226-199809000-00012
27. Muller LJ. The specific architecture of the anterior stroma accounts for maintenance of corneal curvature. Br J Ophthalmol. 2001;85(4):437–443. doi:10.1136/bjo.85.4.437
28. Patel S, Marshall J, Fitzke FW. Refractive index of the human corneal epithelium and stroma. J Refract Surg. 1995;11(2):100–105. doi:10.3928/1081-597X-19950301-09
29. Freund DE, McCally RL, Farrell RA, Cristol SM, L’Hernault NL, Edelhauser HF. Ultrastructure in anterior and posterior stroma of perfused human and rabbit corneas. Relation to transparency. Invest Ophthalmol Vis Sci. 1995;36(8):1508–1523.
30. Bettelheim FA, Plessy B. The hydration of proteoglycans of bovine cornea. Biochim Biophys Acta. 1975;381(1):203–214. doi:10.1016/0304-4165(75)90202-0
31. McCally RL, Farrell RA. Light Scattering from Cornea and Corneal Transparency. In: Masters BR, editor. Non-Invasive Diagnostic Techniques in Ophthalmology. Springer; 1990:189–210.
32. Gallagher B, Maurice D. Striations of light scattering in the corneal stroma. J Ultrastruct Res. 1977;61(1):100–114. doi:10.1016/S0022-5320(77)90009-0
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.