")
Back to Journals » Journal of Pain Research » Volume 18
A Bidirectional Mendelian Randomization Study of Causal Relationships Between Migraine and White-Matter Structural Connectivity
Authors Tong D, Zhang X, Xiao Z, Taothong S, Teeravarunyou P, Wu W, Wu S, Chen N, Tao S, Zhou J, Song Q, Liang F , Li Z
Received 23 February 2025
Accepted for publication 14 June 2025
Published 9 July 2025 Volume 2025:18 Pages 3429—3438
DOI https://doi.org/10.2147/JPR.S521100
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rune Häckert Christensen
Dan Tong,1,2,* Xinyue Zhang,1,2,* Zhiyong Xiao,1,3,* Supattra Taothong,1,2 Prapawee Teeravarunyou,1,2 Wanxia Wu,1,2 Sai Wu,1,2 Nuo Chen,1,2 Siyuan Tao,1,2 Jun Zhou,1,2 Qian Song,4 Fanrong Liang,1,2 Zhengjie Li1,2,4 On behalf of International Headache Genetics Consortium (IHGC)
1Acupuncture and Tuina School, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China; 2Key Laboratory of Acupuncture for Senile Disease (Chengdu University of TCM), Ministry of Education, Chengdu, Sichuan, People’s Republic of China; 3Sichuan Jinxin Xinan Women’s & Children’s Hospital (Bisheng), Chengdu, People’s Republic of China; 4National Clinical Research Center for Chinese Medicine Acupuncture and Moxibustion, First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhengjie Li, Email [email protected]
Objective: This study aims to investigate the potential causal relationship between migraine and white matter (WM) structural connectivity using genetic data and the Mendelian randomization (MR) analyses method.
Methods: Genome-wide association study (GWAS) summary statistics for migraine (48,975 cases/540,381 controls) and 206 WM structural connectivity related imaging-derived phenotypes (IDPs) (26,333 samples) were collected. Based on instrumental variables (IVs) selected from the GWAS summary statistics, the bidirectional two-sample MR analyses were conducted to infer bidirectional causal associations between migraine and WM structural connectivity. The inverse variance-weighted (IVW) method served as the primary approach for analyzing causality.
Results: In the forward MR analysis, it was found that migraine had a significant effect on right hemisphere somatomotor network to amygdala WM structural connectivity (IVW-derived β = 0.11, 95% CI = [0.04, 0.17], p = 1.02e-03, FDR p = 0.04). While in the reverse MR analysis, no causal link was detected between WM structural connectivity and migraine.
Conclusion: This study provides genetic evidences for a causal relationship between migraine and WM structural connectivity. These findings provide new perspectives for the understanding of neuropathology and symptomatology in migraine and might provide a potential therapeutic target for future migraine treatment research.
Keywords: migraine, white matter structure connectivity, imaging-derived phenotype, neuroimaging, causal relationship, Mendelian randomization
Introduction
Migraine is a complex neurovascular disorder that is characterized by moderate-to-severe pulsating and usually one-sided headache that may be aggravated by physical activity, often accompanied by symptoms such as nausea, vomiting, photophobia, phonophobia, as well as various autonomic, cognitive, and emotional symptoms.1 Migraine affects approximately 15% of the global population and is ranked as the second largest contributor to years lived with disability worldwide, leading to a significant socio-economic burden.2 However, the available treatments for migraine are not fully satisfactory,3 largely due to the poor understanding of its complex pathophysiology.
Migraine is a heritable disease, highlighting the contribution of genes in migraine pathophysiology.4,5 Current gene studies revealed that only a rare subtype of migraine (familial hemiplegic migraine) is monogenic, for which three ion transporter genes (CACNA1A, ATP1A2, and SCN1A) have been identified.6 The other forms of migraine instead have a complex polygenic architecture. A recent genome-wide association study (GWAS) of 102,084 migraine cases and 771,257 controls identified 123 risk loci, which were enriched in both vascular and central nervous system tissue/cell types, explaining the complicated pathology and symptomatology in migraine patients.7 Although the exact pathophysiology of migraine is unknown, migraine is believed to involve the activation and sensitization of the trigemino-vascular system, brainstem, diencephalic and brain cortical areas. In recent decades, many neuroimaging studies have explored the mechanisms underlying migraine headache and non-headache symptoms in vivo. For example, functional neuroimaging studies have reported widespread functional abnormalities in cortical, subcortical regions and brainstem (most are pain sensation, pain affection, descending pain modulation system, motor, autonomy, and cognition related brain areas or networks) in migraine during different phases.8,9 In addition to functional alterations, structure neuroimaging studies have also shown both brain gray matter and white matter (WM) structural abnormalities in migraine patients.10,11 However, most of them are observational studies and whether these brain changes are a cause or consequence of migraine is unclear.
Mendelian randomization (MR) is a widely used epidemiological method that introduces genetic variants as instruments to draw causal inferences from observational data.12,13 MR could avoid reverse causation bias and confounding in observational data because genetic variants are innate and relatively independent of self-selected behaviors.14,15 Furthermore, recent large-scale GWAS on both neuroimaging parameters (such as brain imaging-derived phenotypes, IDPs) and neuropsychiatric disorders provide opportunities to explore the causality between brain IDPs and neuropsychiatric diseases such as migraine.16 In the last two years, researchers have preliminary used MR method to explore the causal relationship between migraine and many brain IDPs, such as intracranial volume,17,18 gray matter volume,19 brain resting-state functional activities,20 and WM microstructural properties.21 However, an important brain IDP in migraine, WM structural connectivity, has not been explored using MR so far. Unlike WM microstructural properties that reflect the health of WM,22 WM structural connectivity quantifies the strength of structural connections between brain regions through fiber tracking or tractography to better understand how the brain is connected.23,24 Fiber tracking or tractography has already implicated connectomic disturbances in diverse psychiatric disorders,25 chronic pain conditions,26,27 and etc. Recent diffusion MRI studies have also reported that migraine patients had WM structural connectivity changes in the limbic and sensory systems (such as sensory/motor regions, orbitofrontal cortex, temporal pole, amygdala, accumbens, and caudate nuclei).28,29 However, all of these studies are observational, whether these limbic and sensory systems WM structural connectivity changes are a cause or consequence of migraine is unclear.
Thus, in this study, we tried to carry out a two-sample and bidirectional MR study to explore the causal association between WM structural connectivity and migraine risk using the largest GWAS data to date. Given the high prevalence and significant disease burden of migraine, as well as the clinical challenges in migraine management, we hope that this study will lead to a better understanding of the neuropathology or symptomatology in migraine and provide potential targets for more precise and effective interventions to improve patient outcomes.
Materials and Methods
This study utilized bidirectional two-sample MR analyses. Firstly, the linkage disequilibrium score regression (LDSC) was used to estimate the genetic correlations between migraine and each phenotype of WM structural connectivity IDPs. Then, based on the GWAS summary statistics of migraine and the screened WM structural connectivity IDPs, a two-sample MR analysis was used to infer the bidirectional causal relationships. All the statistical analyses above were performed using LDSC Version 1.0.1, along with the TwoSampleMR (https://github.com/MRCIEU/TwoSampleMR/tree/master) and MR-PRESSO (https://github.com/rondolab/MR-PRESSO) packages in R software (Version 4.3.2). The study flowchart is presented in Figure 1.
 |
Figure 1 Flowchart of the genetic correlation analysis and Mendelian randomization analysis. Abbreviations: GWAS, genome-wide analysis study; IHGC, International Headache Genetics Consortium; LDSC, linkage disequilibrium score regression; SNP, single nucleotide polymorphism; IVs, instrumental variables. |
Datasets
The GWAS summary statistics data for migraine were derived from the International Headache Genetics Consortium (IHGC),7 representing the largest migraine GWAS meta-analysis to date. In light of privacy concerns for participants in the 23andMe cohort, this study excluded the samples from the 23andMe cohort. Among the data collected, the evaluation of participants’ migraine is either conducted by physicians following the criteria outlined in the second edition of the International Classification of Headache Disorders or based on the participants’ self-reported conditions. The summary data includes 589,356 individuals from European ancestry, comprising 48,975 migraine cases and 540,381 controls.
Based on the most recent study,30 the GWAS summary statistics data for WM structural connectivity are derived from diffusion magnetic resonance imaging tractography conducted on 26,333 participants from the UK Biobank. The statistics data yielded 206 WM structural connectivity IDPs, with each measure representing the density of myelinated connections within or between a pair of cortical networks, subcortical structures or cortical hemispheres.31 The raw data could be downloaded from the European Bioinformatics Institute GWAS Catalog (https://www.ebi.ac.uk/gwas) using the accession numbers GCST90302648 to GCST90302853. Detailed descriptions are shown in Supplementary Table 1.
Genetic Correlation Analysis
This study used LDSC for genetic correlation analysis, as it only requires GWAS summary statistics and does not produce bias due to sample overlap.32 By examining the relationship between the test statistics and LDSC, the contribution of each factor could be quantified, and it has been widely used to analyze many complex diseases.33 We utilized the LDSC software (https://github.com/bulik/ldsc)33 to analyze the genetic correlations between migraine and 206 WM structural connectivity IDPs. Based on the data from the HapMap-3 project as a reference, the GWAS summary statistics were filtered, excluding variations which were not single nucleotide polymorphisms (SNPs) (eg, indels), SNPs with ambiguous strand orientation, repeated, or with a minor allele frequency (MAF) lower than 0.01. Since the migraine and WM structural connectivity IDPs data both originate from European populations, the linkage disequilibrium (LD) score estimates calculated based on the 1000 Genomes data for European populations were used as the reference panel for performing LDSC analysis. In addition, to retain suggestive evidence for potential genetic correlations, we set a significance threshold of p < 0.05.
Selection of Instrumental Variables (IVs)
The MR study is predicated on three predominant assumptions: (1) IVs are strongly associated with the exposure. (2) IVs are not associated with any potential confounders, ensuring the validity of the causal inference in the analysis. (3) IVs directly impact the outcome only through the exposure. To test the initial assumption, a stringent genome-wide significance threshold of p < 5×10−8 was selected to evaluate the IVs associated with the exposure variable. To avoid bias from correlated IVs, SNPs in LD, defined by an r2 threshold of 0.001 within a 10,000 kb window, were excluded. The strength of the IVs using the F-statistic formula (F = beta2/se2) was assessed to avoid bias associated with weak instruments.34 A threshold of F-statistic >10 for SNPs was applied. To minimize the potential for horizontal pleiotropy, LD trait (https://ldlink.nci.nih.gov/?tab=ldtrait)35 was used to exclude SNPs associated with potential confounding factors such as smoking, drinking, and insomnia.36,37 If the included SNPs were not present in the outcome dataset, proxy SNPs would not be identified. Finally, the retained SNPs were used as the IVs of MR analysis.
Two-Sample MR Analysis
In this study, five MR methods were employed, namely random-effects IVW,38,39 weighted median,40 simple mode, weighted mode,41 and MR-Egger method.42 Among them, IVW was used as the primary method for causal inference due to its strong ability to detect causal relationships. The other four methods served as complements to enhance the reliability of the results. The Wald ratio approach served as the primary MR analysis when solely a single SNP IV was accessible. In the forward MR analysis, where migraine is the exposure and WM structural connectivity serves as the outcome, the beta value (β) was employed to quantify the causal effect. Conversely, in the reverse MR analysis, the odds ratio (OR) was utilized. The β represents the change in the standard deviation (SD) of WM structural connectivity caused by migraine, while the OR indicates the change in the risk of migraine for every 1 SD increase in WM structural connectivity. We used the Benjamini-Hochberg43 method for false discovery rate (FDR) correction to reduce the risk of multiple comparisons resulting in an increased overall false positive rate. IVW results with an FDR-corrected p value of less than 0.05 were considered as significant causal associations. In situations of p < 0.05, but not corrected by FDR, they were considered as suggestive causal associations.
Sensitivity Analysis
To bolster the robustness of the findings, sensitivity analyses were performed. Specifically, MR-Egger regression was utilized to assess the presence of potential pleiotropy.42 Given that one of the fundamental assumptions of MR is the “no horizontal pleiotropy” assumption, which posits that IVs used in MR analysis should only exert their effects on the outcome through the exposure,44 the MR-PRESSO Global test was employed to detect potential horizontal pleiotropy.45 Furthermore, Cochran’s Q statistic was utilized to quantify the degree of heterogeneity among SNPs,39 and a leave-one-out (LOO) analysis was performed to evaluate whether the observed causal relationship was predominantly influenced by a solitary SNP exhibiting substantial horizontal pleiotropy.
Results
Genetic Correlations
LDSC analysis of migraine with 206 WM structural connectivity IDPs yielded 26 phenotypes with potential genetic correlations. Detailed results are shown in Supplementary Table 2.
Two-Sample MR Analysis
Bidirectional two-sample MR analyses suggest that migraine is causally associated with two WM structural connectivity IDPs in the forward analysis, with one association being significant after FDR correction. In the reverse analysis, no causal link was detected between WM structural connectivity and migraine. See Figures 2 and 3 for the details.
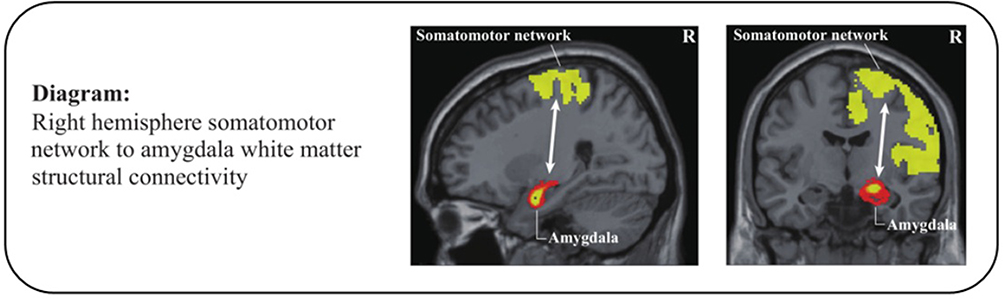 |
Figure 2 The causal relationships between migraine and WM structural connectivity in the forward MR analysis. Abbreviations: MR, Mendelian randomization; R, right. Notes: Migraine had a significant causal effect on the right hemisphere somatomotor network to amygdala WM structural connectivity. |
 |
Figure 3 The results of the MR analysis. Abbreviations: β, beta values; IVs, instrumental variables; MR, Mendelian randomization; WM, white matter. Notes: The causal effects of migraine on WM structural connectivity using two-sample Mendelian randomization methods in the forward MR analysis. No causal link was detected in the reverse MR analysis. |
Based on MR design criteria in this study, 12 confounding SNPs were excluded, and 22 SNPs were selected as IVs for analyzing the relationship between migraine and WM structural connectivity IDPs (Supplementary Table 3). The analysis showed that migraine had significant causal associations with right hemisphere somatomotor network to amygdala WM structural connectivity (IVW-derived β = 0.11, 95% CI = [0.04, 0.17], p = 1.02e-03, FDR p = 0.04) and a suggestive causal association with right hemisphere limbic network to accumbens WM structural connectivity (IVW-derived β = 0.06, 95% CI = [0, 0.12], p = 3.90e-02, FDR p = 0.78).
Sensitivity Analysis
MR-Egger regression and MR-PRESSO Global test were used to assess pleiotropy among genetic instruments, and no pleiotropy was found (Table 1). The results of Cochran’s Q statistic and LOO analysis indicated no heterogeneity or single-SNP-driven effects, suggesting a robust causal relationship (Figure 4).
 |
Table 1 The Results of Sensitivity Analysis |
 |
Figure 4 LOO sensitivity analysis. Abbreviations: β, beta values; LOO, leave-one-out. Notes: (A) Forward LOO sensitivity analysis for the right hemisphere somatomotor network to amygdala WM structural connectivity. (B) Forward LOO sensitivity analysis for the right hemisphere limbic network to accumbens WM structural connectivity. |
Discussion
To the best of our knowledge, this is the first MR study to explore the causal link between migraine and WM structural connectivity IDPs using the largest migraine GWAS meta-analysis to date. Using genetic variants and a bidirectional two-sample MR approach, this study found that migraine was genetically correlated with 26 WM structural connectivity IDPs. Specifically, migraine had a significant causal effect on WM structural connectivity IDPs between the right hemisphere somatomotor network and amygdala. While, in reverse, WM structural connectivity alternations do not appear to raise the risk of migraine.
In the forward MR analysis, it was found that migraine risk is causally associated with increased WM structural connectivity IDPs between the right hemisphere somatomotor network and amygdala. The somatomotor network is a brain network mainly composing the bilateral precentral and postcentral gyri,46 which is participating in pain perception and pain modulation.47 The amygdala is located in the medial temporal lobe, which is involved in emotion, pain affection and pain modulation.48 Previous studies have found that a stronger functional connectivity of the amygdala to the primary somatosensory cortex (S1), primary motor cortex (M1), secondary somatosensory cortex (S2), central operculum, and posterior parietal cortex characterized healthy individuals who showed greater facilitation of pain by negative emotions.49 Specifically in migraine patients, thickening of the somatosensory cortex is found to be associated with a prolonged course of the disease and an increased frequency of headaches.50 An fMRI study also reported that migraine patients showed enhanced intrinsic connectivity between the pons and the contralateral primary somatosensory cortex during an attack, potentially linking to the onset of pain.51 Interestingly, no abnormalities in intrinsic brain connectivity were observed during the interictal phase of migraine with aura.52 Therefore, we infer that the structural changes in somatomotor network are more likely a consequence of chronic pain rather than its cause, as these structural alterations are reversible and can be normalized when pain is alleviated through effective treatments.53,54 Recent research reveals an inverse correlation between the severity of migraines and the volume of the right amygdala, suggesting that increased migraine severity is associated with a smaller volume in this brain region.55 Given that migraine is a repeated and chronic brain disorder, the enhanced structural connectivity between the right hemisphere somatomotor network and amygdala might be resulted from repeated headache attacks and negative emotions in migraine patients. Longitudinal studies may help to clarify this issue in the future. It is worth noting the significant role of extracranial vascular abnormalities in the pathophysiology of migraine.56 However, it remains unclear whether and how pathological changes in extracranial vessels affect WM structure. Therefore, future research could be conducted to investigate the dynamic relationship between vascular factors and changes in WM structure to gain a more comprehensive understanding of the pathogenesis of migraine. In the present study, reverse MR analysis did not detect a causal relationship, suggesting that migraine-induced enhancement of WM structural connectivity from the right hemisphere somatosensory motor network to the amygdala is not affected by reverse causality.
In the last decades, neuroimaging studies of migraine have multiplied, offering not only a more profound comprehension of migraine’s neural pathophysiology but also help to improve the understanding of how migraine treatments work and develop more precise and effective interventions. Especially, recent migraine neuroimaging MR findings have offered more directed and specific insights, aiding in the interpretation of therapeutic targets and the development of innovative treatment strategies for migraine. For example, the non-invasive brain neurostimulation technique Transcranial Magnetic and Direct Current Stimulation (TMS/tDCS) has developed rapidly these years and has shown good potential in alleviating migraine symptoms, including pain severity, headache days and headache related disability, depressive and anxiety symptoms.57 These common targets of TMS/tDCS include the left dorsolateral prefrontal cortex (DLPFC), bilateral DLPFC, left motor cortex, right motor cortex, occipital cortex, and the area of perceived pain, etc.58,59 It is important to note that migraine treatment exploration also includes complementary alternative therapies and physical therapy.60,61 Combined with previous neuroimaging studies and our genetic findings, we further hypothesize that TMS/tDCS treatments targeting the left and right motor cortex might act to alleviate headache symptoms primarily by modulating these migraine-related WM structural connections. Future randomized controlled trials (RCTs) could focus on examining the response to these targeted neuromodulation strategies for more precise individualized treatment. Additionally, more detailed and comprehensive migraine neuroimaging MR studies are encouraged to be conducted in the future, providing more ideas and guidance for the development of precision treatment measures for migraine patients.
Limitations
This study has the following limitations. First, since the GWAS dataset is derived from individuals of European ancestry, we cannot rule out potential biases introduced by differences in other ethnic populations. Therefore, it is necessary to extend and validate the findings in samples from different ethnic populations in future studies. Second, due to limited statistical power in existing GWAS datasets for migraine subtypes (fewer than 10,000 cases), no further analysis was conducted on causal relationships between migraine subtypes (eg migraine with or without aura) and WM structural connectivity. Future studies with larger subtype-specific samples may provide more detailed insights for this topic. Third, whether these connectivity alterations are migraine-specific manifestations worth to be explored in the future. Fourth, because the GWAS data are cross-sectional, it is not possible to infer the temporal dimensions of disease progression (eg, the dynamics of disease stage and WM structural connectivity) in this study, and future longitudinal studies combining multiple time-point neuroimaging assessments might be needed to validate this point.
Conclusion
This study provides genetic evidences for a causal relationship between migraine and WM structural connectivity. These findings provide new perspectives for the understanding of neuropathology and symptomatology in migraine and might provide a potential therapeutic target for future migraine treatment research.
Data Sharing Statement
All data used in the current study are publicly available GWAS data. And the pooled data used and analyzed in the present study are available from the article or supplemental materials.
Ethics
The data used in this study were obtained from anonymized public databases and were fully compliant with the exemption criteria specified in Article 32, item 1 and 2 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (issued by the National Health Commission of China, effective February 18, 2023). Consequently, our study does not require additional informed consent or ethical review.
Acknowledgments
The authors would like to thank the International Headache Genetics Consortium for providing the GWAS summary statistics of migraine, and the UK Biobank participants and researchers for their assistance with the structural connectivity GWAS. The members of the International Headache Genetics Consortium are listed in the Supplementary Table 4.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by funds from the National Natural Science Foundation of China (82474657, 81973958), Distinguished Young Scholars Project of Science and Technology Department of Sichuan Province (No.2025NSFJQ0056), Open Project of National Clinical Research Center for Chinese Medicine Acupuncture and Moxibustion (NCRCOP20230011), and Natural Science Foundation of Sichuan (No.2023NSFSC1820).
Disclosure
The authors disclose no conflicts of interest in this work.
References
1. Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202.
2. Steiner TJ, Stovner LJ. Global epidemiology of migraine and its implications for public health and health policy. Nat Rev Neurol. 2023;19(2):109–117. doi:10.1038/s41582-022-00763-1
3. Robbins MS. Diagnosis and management of headache: a review. JAMA. 2021;325(18):1874–1885. doi:10.1001/jama.2021.1640
4. Polderman TJ, Benyamin B, De leeuw CA, et al. Meta-analysis of the heritability of human traits based on fifty years of twin studies. Nat Genet. 2015;47(7):702–709. doi:10.1038/ng.3285
5. Ulrich V, Gervil M, Kyvik KO, Olesen J, Russell MB. The inheritance of migraine with aura estimated by means of structural equation modelling. J Med Genet. 1999;36(3):225–227.
6. Grangeon L, Lange KS, Waliszewska-Prosół M, et al. Genetics of migraine: where are we now? J Headache Pain. 2023;24(1):12. doi:10.1186/s10194-023-01547-8
7. Hautakangas H, Winsvold BS, Ruotsalainen SE, et al. Genome-wide analysis of 102,084 migraine cases identifies 123 risk loci and subtype-specific risk alleles. Nat Genet. 2022;54(2):152–160. doi:10.1038/s41588-021-00990-0
8. Schwedt TJ, Chiang CC, Chong CD, Dodick DW. Functional MRI of migraine. Lancet Neurol. 2015;14(1):81–91. doi:10.1016/s1474-4422(14)70193-0
9. Messina R, Gollion C, Christensen RH, Amin FM. Functional MRI in migraine. Curr Opin Neurol. 2022;35(3):328–335. doi:10.1097/wco.0000000000001060
10. Zhang X, Zhou J, Guo M, et al. A systematic review and meta-analysis of voxel-based morphometric studies of migraine. J Neurol. 2023;270(1):152–170. doi:10.1007/s00415-022-11363-w
11. Zhang W, Cheng Z, Fu F, Zhan Z. Prevalence and clinical characteristics of white matter hyperintensities in migraine: a meta-analysis. Neuroimage Clin. 2023;37:103312. doi:10.1016/j.nicl.2023.103312
12. Sekula P, Del Greco MF, Pattaro C, Köttgen A. Mendelian randomization as an approach to assess causality using observational data. J Am Soc Nephrol. 2016;27(11):3253–3265. doi:10.1681/asn.2016010098
13. Emdin CA, Khera AV, Kathiresan S. Mendelian randomization. JAMA. 2017;318(19):1925–1926. doi:10.1001/jama.2017.17219
14. Davies NM, Holmes MV, Davey Smith G. Reading Mendelian randomisation studies: a guide, glossary, and checklist for clinicians. BMJ. 2018;362:k601. doi:10.1136/bmj.k601
15. Besser LM, Brenowitz WD, Meyer OL, Hoermann S, Renne J. Methods to address self-selection and reverse causation in studies of neighborhood environments and brain health. Int J Environ Res Public Health. 2021;18(12):6484. doi:10.3390/ijerph18126484
16. Guo J, Yu K, Dong SS, et al. Mendelian randomization analyses support causal relationships between brain imaging-derived phenotypes and risk of psychiatric disorders. Nat Neurosci. 2022;25(11):1519–1527. doi:10.1038/s41593-022-01174-7
17. Daghlas I, Rist PM, Chasman DI. Effect of genetic liability to migraine on cognition and brain volume: a Mendelian randomization study. Cephalalgia. 2020;40(9):998–1002. doi:10.1177/0333102420916751
18. Mitchell BL, Diaz-Torres S, Bivol S, et al. Elucidating the relationship between migraine risk and brain structure using genetic data. Brain.;145(9):3214–3224. doi:10.1093/brain/awac105.
19. Guo X, Wang D, Ying C, Hong Y. Association between brain structures and migraine: a bidirectional Mendelian randomization study. Front Neurosci. 2023;17:1148458. doi:10.3389/fnins.2023.1148458
20. Lu Q, Jia Z, Gu H. Association between brain resting-state functional activities and migraine: a bidirectional Mendelian randomization study. Sci Rep. 2024;14(1):23901. doi:10.1038/s41598-024-74745-2
21. Zhao L, Zhao W, Cao J, Tu Y. Causal relationships between migraine and microstructural white matter: a Mendelian randomization study. J Headache Pain. 2023;24(1):10. doi:10.1186/s10194-023-01550-z
22. Kochunov P, Thompson PM, Lancaster JL, et al. Relationship between white matter fractional anisotropy and other indices of cerebral health in normal aging: tract-based spatial statistics study of aging. Neuroimage. 2007;35(2):478–487. doi:10.1016/j.neuroimage.2006.12.021
23. Conturo TE, Lori NF, Cull TS, et al. Tracking neuronal fiber pathways in the living human brain. Proc Natl Acad Sci U S A. 1999;96(18):10422–10427. doi:10.1073/pnas.96.18.10422
24. Jeurissen B, Descoteaux M, Mori S, Leemans A. Diffusion MRI fiber tractography of the brain. NMR Biomed. 2019;32(4):e3785. doi:10.1002/nbm.3785
25. Zhang F, Daducci A, He Y, et al. Quantitative mapping of the brain’s structural connectivity using diffusion MRI tractography: a review. Neuroimage. 2022;249:118870. doi:10.1016/j.neuroimage.2021.118870
26. Mao CP, Wilson G, Cao J, Meshberg N, Huang Y, Kong J. Abnormal anatomical and functional connectivity of the thalamo-sensorimotor circuit in chronic low back pain: resting-state functional magnetic resonance imaging and diffusion tensor imaging study. Neuroscience. 2022;487:143–154. doi:10.1016/j.neuroscience.2022.02.001
27. Xu H, Seminowicz DA, Krimmel SR, Zhang M, Gao L, Wang Y. Altered structural and functional connectivity of salience network in patients with classic trigeminal neuralgia. J Pain. 2022;23(8):1389–1399. doi:10.1016/j.jpain.2022.02.012
28. Planchuelo-Gómez Á, García-Azorín D, Á l G, Aja-Fernández S, Rodríguez M, de Luis-García R. Structural connectivity alterations in chronic and episodic migraine: a diffusion magnetic resonance imaging connectomics study. Cephalalgia. 2020;40(4):367–383. doi:10.1177/0333102419885392
29. Noh E, Namgung JY, Jang Y, Park Y, Lee MJ, Park BY. Shifts in structural connectome organization in the limbic and sensory systems of patients with episodic migraine. J Headache Pain. 2024;25(1):99. doi:10.1186/s10194-024-01806-2
30. Wainberg M, Forde NJ, Mansour S, et al. Genetic architecture of the structural connectome. Nat Commun. 2024;15(1):1962. doi:10.1038/s41467-024-46023-2
31. Yeo BT, Krienen FM, Sepulcre J, et al. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J Neurophysiol. 2011;106(3):1125–1165. doi:10.1152/jn.00338.2011
32. Bulik-Sullivan B, Finucane HK, Anttila V, et al. An atlas of genetic correlations across human diseases and traits. Nat Genet. 2015;47(11):1236–1241. doi:10.1038/ng.3406
33. Bulik-Sullivan BK, Loh PR, Finucane HK, et al. LD Score regression distinguishes confounding from polygenicity in genome-wide association studies. Nat Genet. 2015;47(3):291–295. doi:10.1038/ng.3211
34. Burgess S, Thompson SG. Avoiding bias from weak instruments in Mendelian randomization studies. Int J Epidemiol. 2011;40(3):755–764. doi:10.1093/ije/dyr036
35. Lin SH, Brown DW, Machiela MJ. LDtrait: an online tool for identifying published phenotype associations in linkage disequilibrium. Cancer Res. 2020;80(16):3443–3446. doi:10.1158/0008-5472.Can-20-0985
36. Seng EK, Martin PR, Houle TT. Lifestyle factors and migraine. Lancet Neurol. 2022;21(10):911–921. doi:10.1016/s1474-4422(22)00211-3
37. Zhao L, Matloff W, Ning K, Kim H, Dinov ID, Toga AW. Age-related differences in brain morphology and the modifiers in middle-aged and older adults. Cereb Cortex. 2019;29(10):4169–4193. doi:10.1093/cercor/bhy300
38. Burgess S, Scott RA, Timpson NJ, Davey Smith G, Thompson SG. Using published data in Mendelian randomization: a blueprint for efficient identification of causal risk factors. Eur J Epidemiol. 2015;30(7):543–552. doi:10.1007/s10654-015-0011-z
39. Burgess S, Butterworth A, Thompson SG. Mendelian randomization analysis with multiple genetic variants using summarized data. Genet Epidemiol. 2013;37(7):658–665. doi:10.1002/gepi.21758
40. Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. 2016;40(4):304–314. doi:10.1002/gepi.21965
41. Hartwig FP, Davey Smith G, Bowden J. Robust inference in summary data Mendelian randomization via the zero modal pleiotropy assumption. Int J Epidemiol. 2017;46(6):1985–1998. doi:10.1093/ije/dyx102
42. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44(2):512–525. doi:10.1093/ije/dyv080
43. Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J Royal Stat Soc Series B. 2018;57(1):289–300. doi:10.1111/j.2517-6161.1995.tb02031.x
44. Ebrahim S, Davey Smith G. Mendelian randomization: can genetic epidemiology help redress the failures of observational epidemiology? Hum Genet. 2008;123(1):15–33. doi:10.1007/s00439-007-0448-6
45. Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet. 2018;50(5):693–698. doi:10.1038/s41588-018-0099-7
46. Li D, Liu R, Meng L, et al. Abnormal ventral somatomotor network homogeneity in patients with temporal lobe epilepsy. Front Psychiatry. 2022;13:877956. doi:10.3389/fpsyt.2022.877956
47. Gim S, Hong SJ, Reynolds Losin EA, Woo CW. Spatiotemporal integration of contextual and sensory information within the cortical hierarchy in human pain experience. PLoS Biol. 2024;22(11):e3002910. doi:10.1371/journal.pbio.3002910
48. Veinante P, Yalcin I, Barrot M. The amygdala between sensation and affect: a role in pain. J Mol Psychiatry. 2013;1(1):9. doi:10.1186/2049-9256-1-9
49. Gandhi W, Rosenek NR, Harrison R, Salomons TV. Functional connectivity of the amygdala is linked to individual differences in emotional pain facilitation. Pain. 2020;161(2):300–307. doi:10.1097/j.pain.0000000000001714
50. Kim JH, Kim JB, Suh SI, Seo WK, Oh K, Koh SB. Thickening of the somatosensory cortex in migraine without aura. Cephalalgia. 2014;34(14):1125–1133. doi:10.1177/0333102414531155
51. Hougaard A, Amin FM, Larsson HB, Rostrup E, Ashina M. Increased intrinsic brain connectivity between pons and somatosensory cortex during attacks of migraine with aura. Hum Brain Mapp. 2017;38(5):2635–2642. doi:10.1002/hbm.23548
52. Hougaard A, Amin FM, Magon S, Sprenger T, Rostrup E, Ashina M. No abnormalities of intrinsic brain connectivity in the interictal phase of migraine with aura. Eur J Neurol. 2015;22(4):702–e46. doi:10.1111/ene.12636
53. Rodriguez-Raecke R, Niemeier A, Ihle K, Ruether W, May A. Brain gray matter decrease in chronic pain is the consequence and not the cause of pain. J Neurosci. 2009;29(44):13746–13750. doi:10.1523/jneurosci.3687-09.2009
54. Obermann M, Nebel K, Schumann C, et al. Gray matter changes related to chronic posttraumatic headache. Neurology. 2009;73(12):978–983. doi:10.1212/WNL.0b013e3181b8791a
55. Kosuge S, Masaoka Y, Kasai H, et al. The right amygdala and migraine: analyzing volume reduction and its relationship with symptom severity. PLoS One. 2024;19(4):e0301543. doi:10.1371/journal.pone.0301543
56. R E, E G, N A, et al. Proteomic analysis of vessels in migraine surgery. Plast Reconstr Surg Glob Open. 2023;11(10 Suppl):76–77. doi:10.1097/01.GOX.0000992272.93365.45
57. Bharath MM, Paliwal VK, Batra S, Mishra P, Mishra N, Saini R. Repetitive transcranial magnetic stimulation in new daily persistent headache patients: a single arm open label study. J Headache Pain. 2024;25(1):155. doi:10.1186/s10194-024-01866-4
58. Stilling JM, Monchi O, Amoozegar F, Debert CT. Transcranial magnetic and direct current stimulation (TMS/tDCS) for the treatment of headache: a systematic review. Headache. 2019;59(3):339–357. doi:10.1111/head.13479
59. Shirahige L, Melo L, Nogueira F, Rocha S, Monte-Silva K. Efficacy of noninvasive brain stimulation on pain control in migraine patients: a systematic review and meta-analysis. Headache. 2016;56(10):1565–1596. doi:10.1111/head.12981
60. Tedeschi R, Pillastrini P, Pierangeli G, Favoni V, Cortelli P, Cevoli S. Is physiotherapy in migraines known to sufferers? A cross-sectional study. Neurol Sci. 2024;45(4):1669–1674. doi:10.1007/s10072-023-07195-9
61. Tedeschi R. Exploring the efficacy of plantar reflexology as a complementary approach for headache management: a comprehensive review. Int J Ther Massage Bodywork. 2024;17(3):31–40. doi:10.3822/ijtmb.v17i3.971
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Causal Relationship Between Gastroesophageal Reflux Disease and Chronic Obstructive Pulmonary Disease: A Bidirectional Two-Sample Mendelian Randomization Study
Liu B, Chen M, You J, Zheng S, Huang M
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:87-95
Published Date: 10 January 2024
Exploring a Potential Causal Link Between Dietary Intake and Chronic Obstructive Pulmonary Disease: A Two-Sample Mendelian Randomization Study
Zhang C, Yu L, Xiong T, Zhang Y, Liu J, Zhang J, He P, Xi Y, Jiang Y
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:297-308
Published Date: 26 January 2024
Genomics-Microbiome Based Assessment of Bidirectional Causality Between Gut Microbiota and Psoriasis
Gao Q, Liu JH, Ma WY, Cheng ZL, Hao PS, Luo NN
Clinical, Cosmetic and Investigational Dermatology 2024, 17:435-445
Published Date: 13 February 2024
Mendelian Randomization Analysis of Circulating Cytokines and Risk of Autoimmune Neuroinflammatory Diseases

Tao SS, Cao F, Zhang RD, Xu SZ, Li XX, Tang J, Yang XK, Pan HF
ImmunoTargets and Therapy 2024, 13:273-286
Published Date: 10 June 2024
A Bidirectional Mendelian Randomization Study Investigating the Causal Relationship Between Ankylosing Spondylitis and Chronic Obstructive Pulmonary Disease
Pan D, Dai X, Li P, Xue L
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:259-271
Published Date: 8 February 2025