")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 18
A Bidirectional Two-Sample Mendelian Randomization Study of Genetic Causality Between Vitamin D Levels and Pemphigus
Authors Wang Y , Cheng S , Que H
Received 16 February 2025
Accepted for publication 5 May 2025
Published 10 May 2025 Volume 2025:18 Pages 1167—1176
DOI https://doi.org/10.2147/CCID.S523136
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Yanchun Wang,1 Shiping Cheng,2 Huafa Que3
1College of Clinical Medicine, Jiangxi University of Chinese Medicine, Nanchang, Jiangxi Province, People’s Republic of China; 2Department of Dermatology, the Affiliated Hospital of Jiangxi University of Chinese Medicine, Nanchang, Jiangxi Province, People’s Republic of China; 3Traditional Chinese Medicine Surgery, Longhua Hospital Affiliated to Shanghai University of Chinese Medicine, Shanghai, People’s Republic of China
Correspondence: Huafa Que, Traditional Chinese Medicine Surgery, Longhua Hospital Affiliated to Shanghai University of Chinese Medicine, No. 725 Wanping South Road, Shanghai, 200032, People’s Republic of China, Email [email protected]
Background: Pemphigus, a B-cell-mediated autoimmune disease, has been hypothesized to involve vitamin D due to its immunomodulatory effects on B-cell activity. However, observational studies on this association remain inconclusive due to confounding factors. This study used genome-wide association study (GWAS) data for bidirectional two-sample Mendelian randomization (MR) analysis to clarify causality.
Materials and Methods: Genetic instruments for serum vitamin D levels (61 SNPs) and pemphigus (3 SNPs) were analyzed via inverse variance weighting (IVW), weighted median, and MR-Egger regression. Forward MR analysis revealed no causal effect of vitamin Don pemphigus risk [IVW OR=0.835 (95% CI:0.318– 2.189), P=0.623], consistent across sensitivity analyses. Conversely, reverse MR showed pemphigus did not influence vitamin D levels [IVW OR=1.000 (95% CI:0.993– 1.006), P=0.867]. Heterogeneity (Cochran Q test) and pleiotropy (MR-Egger intercept) tests confirmed robustness of results.
Results: Our findings challenge the presumed causal link between vitamin D and pemphigus, suggesting observed associations may arise from confounding factors. This underscores the need for mechanistic studies to explore alternative pathways in pemphigus pathogenesis.
Keywords: vitamin D, pemphigus, Mendelian randomization analysis, genome-wide association study
Introduction
Pemphigus is an autoimmune bullous disease involving the mucosa. Based on its unique clinical features and pathophysiology, several subtypes of pemphigus are currently identified, among which PV and PF are the two main types of pemphigus. PV is characterized by mucosal involvement and anti-desmoglein 1 autoantibodies and anti-desmoglein 3 autoantibodies, while PF is mainly characterized by skin involvement and anti-desmoglein 1 autoantibodies.1,2 In recent years, genetics has played a key role in the development, severity, and prognosis of pemphigus. Single nucleotide polymorphisms (SNPs), the most common form of genetic variation in the human genome, can affect gene expression through changes in promoter activity, messenger RNA stability, and protein function.3 Genetic studies have identified unique SNPs associated with PV and PF, suggesting that different subtypes of pemphigus have different pathogenic pathways.4,5 However, it is worth noting that studies have found that there is a decrease in vitamin D levels in both patients with PV and PF,6,7 which indicates that vitamin D seems to be a common pathogenic pathway for both.
Vitamin D is a fat-soluble vitamin with pleiotropic effect. It regulates autoimmunity through adaptive immunity that inhibits the activity of T lymphocytes and B lymphocytes.8 Some scholars have found a large number of B lymphocytes in pemphigus skin lesion. Activated by autoreactive T cells, B lymphocytes differentiate into plasma cells, produce anti-Dsg1 and anti-Dsg3 antibodies, and then bind to desmosomes on epidermal cells, causing blisters.9,10 Vitamin D prevents B cells from differentiating into plasma cells and producing antibodies.11 On the other hand, vitamin D can also enhance the adhesion between keratinocytes and promote wound healing by upregulating the expression of desmoglein Dsg1.12 In addition, SNP variants in genes associated with vitamin D metabolism, such as GC(rs2282679), CYP2R1(rs10741657), and CYP27B1(rs10877012), have been shown to be associated with serum vitamin D levels. These SNP variants may lead to reduced vitamin D levels in individuals’ serum by affecting the metabolic process of vitamin D.13 Several observational studies have reported a positive correlation between decreased serum 25(OH)D concentration and pemphigus.7,14 Therefore, patients with these genetic variants may be more likely to develop pemphigus due to vitamin D deficiency. However, Moravvej H reported that there was no association between serum 25(OH)D levels and pemphigus compared with the healthy population.15 Moreover, vitamin D does not play a major role in the treatment of pemphigus.1,16 The causal relationship between the two requires further study.
Mendelian randomization (MR) is a method that uses genetic variation as an instrumental variable to infer causality, avoiding the biases inherent in observational studies due to confounding and measurement errors. In view of the conflicting observational reports on vitamin D and pemphigus, this study proposes the hypothesis that vitamin D may modulate pemphigus susceptibility or progression through bidirectional two-sample MR.
Research Methods and Data
Research Design
We followed the STROBE-MR (Report on Strengthening Mendel’s Randomized Epidemiological Observational Study) and used the two-sample Mendelian randomization method for analysis to explore the causal association between vitamin D and pemphigus.17 In the forward MR analysis, serum 25-hydroxyvitamin D levels were used as the exposure factor, SNPs significantly related to vitamin D were selected as instrumental variables, and pemphigus was selected as the outcome. In the reverse MR analysis, pemphigus was used as the exposure factor, SNPs associated with pemphigus were selected as instrumental variables, and serum 25-hydroxyvitamin D levels were regarded as the outcome. The two-sample MR analysis method was used to exclude heterogeneity by Cochran Q test, and the sensitivity analysis was performed on the obtained results to verify its reliability. In addition, the following three key assumptions are adopted in this paper. First of all, there’s a significant association between the instrumental variable and the exposure factor. Secondly, the instrumental variable was not correlated with all confounding factors associated with the exposure-outcome. Thirdly, the instrumental variable can only affect the outcome through its association with the exposure (Figure 1).18
 |
Figure 1 Key assumptions diagram for bidirectional MR analysis. Notes: Green represents forward MR analysis, Serum 25-Hydroxyvitamin D levels are exposure, Pemphigus is the result, and red represents reverse MR analysis, where Pemphigus is exposure and Serum 25-Hydroxyvitamin D levels are the result. |
Data Sources
We selected serum 25-hydroxyvitamin D levels as the genetic data for vitamin D. because both vitamin D2 and D3 are converted into 25-hydroxyvitamin D in the liver by the action of 25-hydroxylase from a metabolic perspective.19 From the point of view of concentration, 25-hydroxyvitamin D is the main form of vitamin D in the bloodstream, and its half-life is relatively long, providing stability in the blood.20 Therefore, we obtained the genetic data of serum 25-hydroxyvitamin D levels from GWAS summary data with 4,225,238 SNPs, including 496,946 European male and female descendants.
To match the genetic background of the study population, we selected the International Guidelines for the Management of Pemphigus developed by the European Forum of Dermatology and the European Society of Dermatology and Venereology,21 and combined with the suggestions proposed by a Delphi process involving 39 international pemphigus experts.22 We defined pemphigus as a rare vesicular autoimmune disease affecting the skin and mucosa, and selected the Finn Gen Biobank as the genetic data source. It included 451,899 European male and female descendants, with 208 SNPs. The genetic backgrounds of the study populations in both datasets were of European origin, which could minimize the bias caused by ethnic-related confounding factors. The basic information is shown in Table 1.
 |
Table 1 Brief Description of Data Sources Involved in Mendelian Randomization Studies |
Ethical Statement
All the data used are publicly available, so no additional ethical approval is required.
Instrumental Variable Selection
To determine the appropriate instrumental variables, we took a series of quality control measures to ensure the robustness and reliability of the analysis. SNPs with significant significance (P < 5 × 10⁻10) were selected as IVs. If no SNPs met the genome-wide significance level, P < 1×10⁻5 was taken as the lower threshold. It is due to strict thresholds that may make it difficult to find enough SNPs for MR Analysis, but lowering the threshold increases the risk of false-positive results as well as reducing the strength of instrumental variables, while also making interpretation of the results more complex. We set the parameters to r² = 0.001 and kb = 10000 to exclude the interference of linkage disequilibrium (LD) and ensure the independence of each SNP to avoid the risk.23 For SNPs missing from the outcome, SNPs with strong linkage disequilibrium (r² > 0.8) were used to fill in the missing values. The F statistic was calculated to assess the degree of association among the IV and the exposure risk and the instrument strength, with an F statistic greater than 10 defined as a strong instrument. The F value was statistically processed using SPSS23.0 statistical software package and expressed as ( ±s). Finally, the effective SNPs related to the exposure factor were obtained as IVs for the two-sample MR analysis through the above methods.
±s). Finally, the effective SNPs related to the exposure factor were obtained as IVs for the two-sample MR analysis through the above methods.
The calculation formula for total F is:

N is the sample size of the included exposure factors, K is the number of SNPs in the databases, and R² is the cumulative explanatory variance of the selected SNPs in the exposure.
The calculation formula for  is:
is:

EAF is the effector allele frequency, SE is the standard error, SD is the standard deviation, and β is the allele effect value.
Mendelian Randomization Analysis
Firstly, the collected SNP data were harmonized, and SNPs with incompatible genes and palindromic SNPs with intermediate gene frequencies were deleted.24 Then, MR analysis was performed using the “TwoSampleMR” (version 0.6.7) in “R version 4.4.1”. The main analysis method was the inverse variance weighted (IVW). The MR results were cross-validated by MR-Egger regression, weighted median and other methods to ensure the validity and robustness of the research results.
IVW is an instrumental variable that is valid across all genetic variants and has a strong ability to detect causality. It obtains the overall estimate of the effect of exposure on the outcome by combining the Wald estimate of causality for each IV.25 MR-Egger regression can identify and correct pleiotropy when the estimates of the instrumental variables are biased, and can provide relatively robust estimates. At the same time, an intercept term is added in the regression to determine the presence or absence of pleiotropy.26 The weighted median method (WME) can obtain robust results when more than 50% of the weights come from invalid IVs. If there is horizontal pleiotropy, it can reduce Type I error to evaluate a more accurate causal association.27 In addition, the Cochran’s Q test in the IVW method is used for heterogeneity analysis, and P < 0.05 is considered as heterogeneity28 (Supplementary Code S1 and S2).
Sensitivity Analysis
The sensitivity study included the pleiotropy test using the MR-Egger intercept and the leave-one-out sensitivity test. Under the InSIDE assumption, the intercept of MR-Egger can be interpreted as the average pleiotropic effect of the genetic variants included in the analysis. If the average pleiotropic effect is zero, the IVW method can give a consistent estimate of the causal effect. Conversely, if the intercept of the MR-Egger analysis is not equal to zero, there will be directed pleiotropy or a violation of the InSIDE hypothesis.26 The leave-one-out test is to exclude each SNP in turn and then re-analyze the combined effect of the remaining SNPs to observe whether there is a large change in the result. The purpose is to explore whether there is a single SNP that will cause a deviation in the overall causal effect.17
Results
Instrumental Variables
In the forward MR analysis, after screening the serum 25-hydroxyvitamin D levels by the genome-wide significance threshold (P<5×10⁻10), there were a total of 9262 SNPs. After linkage disequilibrium correction, we obtained 62 independent SNPs. After coordinating and merging with the outcome data, 61 SNPS except rs1841850 were obtained as IVs (Supplementary Figure S1 and Table S1). In the reverse MR, the pemphigus data could not obtain enough SNPS after the same threshold screening, so P<1×10⁻5 was used for screening, and we obtained 11 independent SNPs. After merging with the outcome, 3 SNPs were obtained as IVs. The average F values of serum 25-hydroxyvitamin D levels and pemphigus were 181.599 and 21.867, respectively (Supplementary Figure S2 and Table S2), indicating that the bias of weak IVs in this study could be negligible, and it was more likely to detect the true causal relationship between the exposure and the outcome.
The Effect of Vitamin D on Pemphigus
In the forward MR analysis, there was no significant correlation between serum 25-hydroxyvitamin D levels and pemphigus [OR (95% CI) = 0.835 (0.318–2.189), P = 0.623] (Table 2). In addition, the MR-Egger and WME tests also cross-verify that there was no association between the two (Figure 2a). We used the Cochran Q test and MR-Egger method to perform heterogeneity tests on the two, and no heterogeneity was found (Table 3). Similarly, the intercept test also did not find pleiotropy (Table 4). After the SNPs were successively excluded by the leave-one-out method, the IVW analysis results of the remaining 60 SNPs were similar to those of all SNPs included, indicating no sensitivity (Figure 3a). The funnel plot result showed that when each SNP was used as a variable, the scatter of the causal association effect was basically symmetrically distributed, and there was no potential bias in the result (Figure 3c).
 |
Table 2 MR Analysis of the Causal Relationship Between Vitamin D Levels and Pemphigus |
 |
Table 3 Heterogeneous Test Between Vitamin D and Pemphigus |
 |
Table 4 Pleiotropy Test Between Vitamin D and Pemphigus |
 |
Figure 2 The scatter plot for MR analyses. Notes: (a) scatter plot of the causal effect of vitamin D on pemphigus risk. (b) scatter plot of the causal effect of pemphigus on vitamin D risk. |
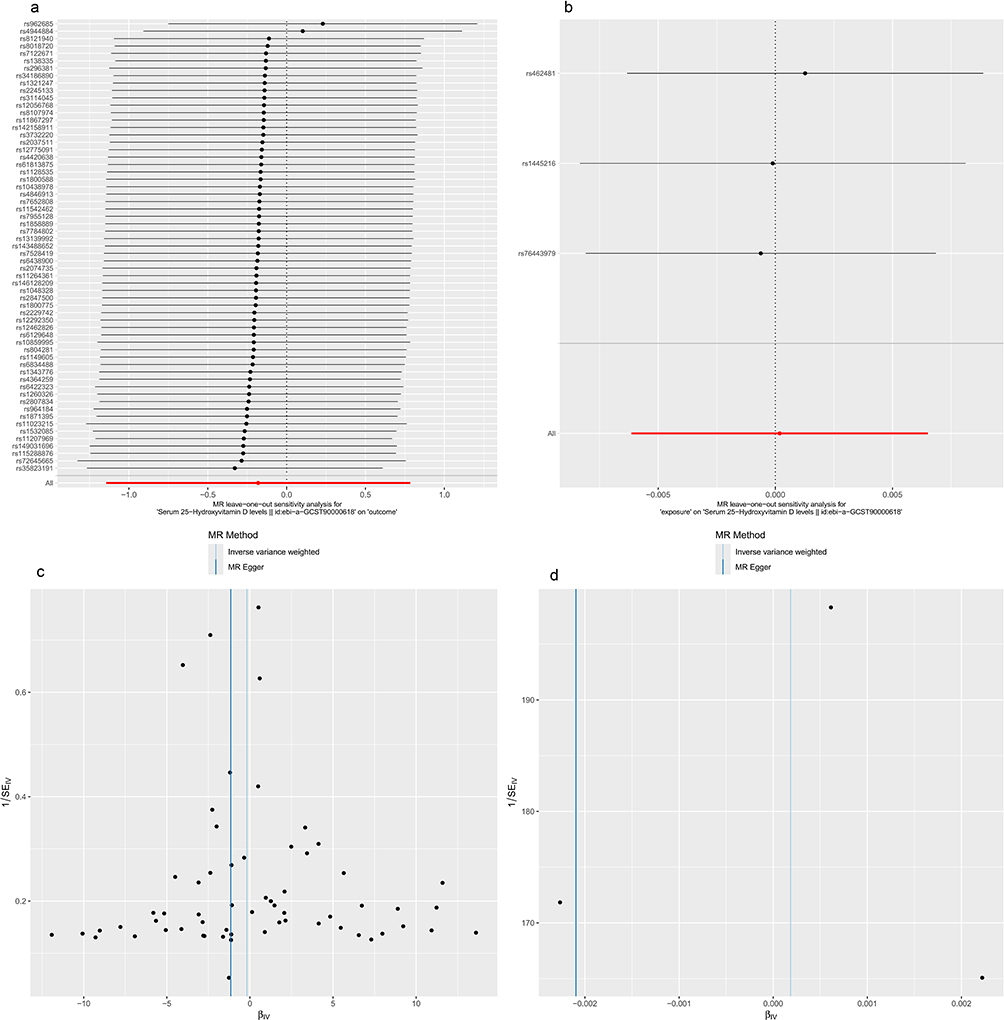 |
Figure 3 Sensitivity analysis and funnel plot for MR analysis. Notes: (a): “Leave out one”sensitivity analysis of vitamin D to pemphigus. (b) “Leave out one” sensitivity analysis of pemphigus to vitamin D. (c) Causality funnel plot of vitamin D to pemphigus risk. (d) Causality funnel plot of pemphigus to vitamin D risk. |
The Effect of Pemphigus on Vitamin D
As shown in Table 2, the IVW method did not find a significant relationship between pemphigus and serum 25-hydroxyvitamin D levels [OR (95% CI) = 1.000 (0.993–1.006), P = 0.867]. And there was also no significant association in other models (Figure 2b). MR-Egger, the Cochran Q test in the IVW method, and the intercept test confirmed that there was no heterogeneity and pleiotropy between the two (Tables 3 and 4). The leave-one-out method and funnel plot (Figure 3b and 3d) further showed that the results of this study had no sensitivity and were robust.
Discussion
This is the first study to examine the association between vitamin D and pemphigus using GWAS data. Our study did not find a causal relationship between vitamin D levels and pemphigus.
In recent years, some studies have noted an association between vitamin D levels and pemphigus, which is contrary to our findings. A positive cohort study on pemphigus patients showed that these patients had vitamin D deficiency and decreased CYP27B1 expression. The defect in the expression of this metabolic enzyme may lead to a reduction in the production of locally synthesized active vitamin D, thereby impairing immune function. In addition, these patients were routinely given vitamin D2 supplementation, but serum levels remained below the normal range, raising doubts about the adjuvant therapeutic effect of vitamin D6. To further study of the connection between the two, some scholars selected a case-control study including 239 pemphigus patients for Meta-analysis, and the results showed that the serum 25-hydroxyvitamin D levels of these patients were decreased.29
A retrospective study in North India found that pemphigus patients showed a deficiency in vitamin D (11.1 ± 5.8ng/mL), indicating that vitamin D deficiency may be a risk factor for pemphigus in the North Indian population. However, there was no statistical significance between the vitamin D level of the control group (12.1 ± 9.2ng/mL) and that of the pemphigus patients (P = 0.6958). The researchers believed that it may be related to the fact that vitamin D deficiency is common in the North Indian population.30 However, it also illustrates the inherent limitations of retrospective studies, although these studies have taken measures such as matching age and ethnicity to minimize confounding effects.
To further explore the above controversial content, we reviewed the relevant literature and concluded that several reasons may be responsible for the link between vitamin D and pemphigus.
Firstly, from a social point of view, pemphigus patients have a worse quality of life than healthy people, resulting in significantly lower self-image satisfaction and reduced daily activities.31,32 Insufficient sunlight exposure is the main factor leading to vitamin D deficiency, and the synthesis of vitamin D mainly depends on sun exposure. Studies have shown that occasional exposure to sunlight is not enough to raise and maintain the concentration of serum 25(OH)D.33 It is possible that pemphigus patients have a lack of vitamin D synthesis pathway due to reduced outdoor activities, thus forming a vicious cycle of continuous reduction. However, these speculations need to be confirmed by further studies.
Secondly, from the immunological aspect, the pathogenesis of pemphigus is caused by autoantibodies targeting desmosomal core glycoprotein. B cells are a reservoir of cells that produce large amounts of secreted antibodies while eliminating cells with self-reactive antigen-specificity.34 B cells can produce antibodies targeting desmosomal core glycoprotein, leading to loss of cell adhesion and blister formation.35 It indicates that B cell activation plays an important role in pemphigus. At the level of immune regulation, vitamin D inhibits auto-reactive B cell activation through a dual pathway. First of all, vitamin D acts directly on B cells, which can promote the apoptosis of activated B cells, regulate class switching, inhibit the production of plasma cells and post-switched memory B cells, and inhibit immune diseases caused by B cell formation.36 On the other hand, vitamin D promotes the transition of CD4 + T cells from pro-inflammatory Th1 phenotype to anti-inflammatory Th2 phenotype, promotes Treg cell expansion and inhibits Th17 cell differentiation through VDR, and reduces the secretion of pro-inflammatory factors such as IL-17 and IL-21.37,38 Some scholars have found a significant increase in Th17 cells and a decrease in Treg cells in the blood of PV patients, which may lead to insufficient inhibition of Treg cells to over-activation of B cells, and further differentiation into plasma cells to produce autoantibodies against keratin cell adhesion proteins.39 It suggests that vitamin D can also indirectly regulate B cell function by regulating T cell subset balance. However, there is currently a lack of experimental evidence for the direct intervention of vitamin D in pemphigus patients, and the correlation between the two cannot be further confirmed.
In addition, glucocorticoids are the preferred treatment for pemphigus. However, long-term use of glucocorticoids can lead to bone damage, characterized by decreased bone density and increased risk of pathological fractures.40 In experimental studies, glucocorticoids directly counteract the effect of 1,25(OH)2D₃ by reducing the expression of TRPV6, calbindin, and PMCA 1b, thereby down-regulating the active intestinal absorption of calcium and having a negative impact on bone density.41 Among them, cadherin, as a membrane-bound cell adhesion protein, is the core of adhesion connections in the epithelial cell layer, and is also the target of pemphigus autoantibodies.42 When calcium is poorly absorbed, it can lead to structural instability and decreased expression of cadherin, leading to acantholysis and blister formation between epithelial cells in pemphigus.43,44 Vitamin D receptor deficiency leads to a reduction in the cadherin complex, which in turn affects the activation and migration of stem cells, resulting in delayed wound healing.45 Therefore, high doses of glucocorticoids may have contributed to the reduction of vitamin D levels in Pemphigus patients by counteracting vitamin D and reducing the absorption of calcium in the intestine. And it may be exacerbated by abnormal expression of cadherin in some pemphigus patients who are not sensitive to glucocorticoid therapy. However, the current interpretation of vitamin D in the treatment of pemphigus is only from the perspective of osteoporosis prevention, and there is no evidence to suggest that vitamin D can be used as a target for intervention in pemphigus pathogenesis. Future researchers may need to pay more attention to the usage regimen of vitamin D, including the duration and dosage.
In summary, existing observational studies are susceptible to confounding factors, making it difficult to define the causal relationship between vitamin D and pemphigus. These findings should be interpreted with caution. In this study, the MR analysis has the advantages of using genetic information as IVs and a large sample size, and the results are more robust and reliable. Moreover, the GWAS data of pemphigus and vitamin D are both from the European population, which reduces the possibility of population stratification bias and improves the rationality of the two-sample MR hypothesis. In addition, we also adopted different estimation models and sensitivity analyses to cross-validate the obtained results, obtaining reliable and robust results. At the same time, there are still some limitations in the results of our study. First of all, this study only includes people of European ancestry, and the representativeness of the results needs to be further verified in other ethnic groups. Furthermore, we also need larger sample sizes in the future, especially in pemphigus, to improve the accuracy of the estimation and reduce the contingency of the research results.
Conclusion
The MR analysis of this study found no evidence of a causal effect of vitamin D levels on pemphigus risk, challenging the associations reported in observational studies. Meanwhile, future research based on higher quality GWAS data and more advanced methods are needed.
Data Sharing Statement
The data used in this study could be found at GWAS studies we mentioned and The Finn Gen Biobank (https://www.finngen.fi/en/).
Ethics Statement
According to Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Beings adopted by the National Science and Technology Ethics Committee of the People’s Republic of China, ethical review can be exempted because the data used in this study do not cause any harm to human beings, do not involve any sensitive personal information or commercial interests, and the databases selected are open and legal.
Acknowledgments
We acknowledge the investigators of the original GWAS studies and UK Biobank. In addition, the author thanks Ms. Zhong Haiqiao for translating.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not sponsored by any organization.
Disclosure
All authors declare no financial or personal relationships that could be construed as a potential conflict of interest.
References
1. Malik AM, Tupchong S, Huang S, Are A, Hsu S, Motaparthi K. An updated review of pemphigus diseases. Medicina-Lithuania. 2021;57(10). doi:10.3390/medicina57101080
2. Kridin K, Schmidt E. Epidemiology of pemphigus. Jid Innov. 2021;1(1):100004. doi:10.1016/j.xjidi.2021.100004
3. Shastry BS. SNPs: impact on gene function and phenotype. Methods Mol Biol. 2009;578:3–22. doi:10.1007/978-1-60327-411-1_1
4. Mahmoudi H, Ebrahimi E, Daneshpazhooh M, et al. Single-nucleotide polymorphisms associated with pemphigus vulgaris: potent markers for better treatment and personalized medicine. Int J Immunogenet. 2020;47(1):41–49. doi:10.1111/iji.12451
5. Salviano-Silva A, Farias T, Bumiller-Bini V, et al. Genetic variability of immune-related lncRNAs: polymorphisms in LINC-PINT and LY86-AS1 are associated with pemphigus foliaceus susceptibility. Exp Dermatol. 2021;30(6):831–840. doi:10.1111/exd.14275
6. Tahri S, Elloumi N, Khabou B, et al. Exploring the role of vitamin D-VDR pathway in pemphigus foliaceous: a novel perspective on disease pathogenesis. Arch Dermatol Res. 2024;316(7):449. doi:10.1007/s00403-024-03192-w
7. Dhaffouli F, Elloumi N, Tahri S, et al. Unraveling the role of the vitamin D-VDR pathway in pemphigus vulgaris from Tunisian patients. Steroids. 2024;209:109454. doi:10.1016/j.steroids.2024.109454
8. Martens PJ, Gysemans C, Verstuyf A, Mathieu AC. Vitamin D’s effect on immune function. Nutrients. 2020;12(5):1248. doi:10.3390/nu12051248
9. Yuan H, Zhou S, Liu Z, et al. Pivotal role of lesional and perilesional T/B lymphocytes in pemphigus pathogenesis. J Invest Dermatol. 2017;137(11):2362–2370. doi:10.1016/j.jid.2017.05.032
10. Yamagami J. B-cell targeted therapy of pemphigus. J Dermatol. 2023;50(2):124–131. doi:10.1111/1346-8138.16653
11. Fenercioglu AK. The anti-inflammatory roles of vitamin D for improving human health. Curr Issues Mol Biol. 2024;46(12):13514–13525. doi:10.3390/cimb46120807
12. Oda Y, Hu L, Nguyen T, Fong C, Tu CL, Bikle DD. Combined deletion of the vitamin D receptor and calcium-sensing receptor delays wound re-epithelialization. Endocrinology. 2017;158(6):1929–1938. doi:10.1210/en.2017-00061
13. Ruiz-Ballesteros AI, Meza-Meza MR, Vizmanos-Lamotte B, Parra-Rojas I, de la Cruz-Mosso U. Association of vitamin D metabolism gene polymorphisms with autoimmunity: evidence in population genetic studies. Int J Mol Sci. 2020;21(24):9626. doi:10.3390/ijms21249626
14. Marzano AV, Trevisan V, Eller-Vainicher C, et al. Evidence for vitamin D deficiency and increased prevalence of fractures in autoimmune bullous skin diseases. Brit J Dermatol. 2012;167(3):688–691. doi:10.1111/j.1365-2133.2012.10982.x
15. Moravvej H, Mozafari N, Younespour S. Serum 25-hydroxy vitamin D level in patients with pemphigus and its association with disease severity. Clin Exp Dermatol. 2016;41(2):142–147. doi:10.1111/ced.12733
16. Yuan H, Pan M, Chen H, Mao X. Immunotherapy for pemphigus: present and future. Front Med-Lausanne. 2022;9:901239. doi:10.3389/fmed.2022.901239
17. Skrivankova VW, Richmond RC, Woolf B, et al. Strengthening the reporting of observational studies in epidemiology using Mendelian randomization: the STROBE-MR statement. JAMA-J Am Med Assoc. 2021;326(16):1614–1621. doi:10.1001/jama.2021.18236
18. Chen Y, Xu Z, Zhang Z, Wang X, Dong M. No genetic causal association between human papillomavirus and lung cancer risk: a bidirectional two-sample Mendelian randomization analysis. Trials. 2024;25(1):582. doi:10.1186/s13063-024-08366-5
19. Liberman U, Bikle DD. Disorders in the action of vitamin D. 2000.
20. Schottker B, Jorde R, Peasey A, et al. Vitamin D and mortality: meta-analysis of individual participant data from a large consortium of cohort studies from Europe and the United States. BMJ-Brit Med J. 2014;348(jun17 16):g3656. doi:10.1136/bmj.g3656
21. Hertl M, Jedlickova H, Karpati S, et al. Pemphigus. S2 Guideline for diagnosis and treatment--guided by the European dermatology forum (EDF) in cooperation with the European Academy of dermatology and venereology (EADV). J Eur Acad Dermatol. 2015;29(3):405–414. doi:10.1111/jdv.12772
22. Murrell DF, Pena S, Joly P, et al. Diagnosis and management of pemphigus: recommendations of an international panel of experts. J Am Acad Dermatol. 2020;82(3):575–585.e1. doi:10.1016/j.jaad.2018.02.021
23. Aissani B. Confounding by linkage disequilibrium. J Hum Genet. 2014;59(2):110–115. doi:10.1038/jhg.2013.130
24. Yavorska OO, Burgess S. MendelianRandomization: an R package for performing Mendelian randomization analyses using summarized data. Int J Epidemiol. 2017;46(6):1734–1739. doi:10.1093/ije/dyx034
25. Lin Z, Deng Y, Pan W. Combining the strengths of inverse-variance weighting and Egger regression in Mendelian randomization using a mixture of regressions model. PLoS Genet. 2021;17(11):e1009922. doi:10.1371/journal.pgen.1009922
26. Burgess S, Thompson SG. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur J Epidemiol. 2017;32(5):377–389. doi:10.1007/s10654-017-0255-x
27. Bowden J, Davey SG, Haycock PC, Burgess S. Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. 2016;40(4):304–314. doi:10.1002/gepi.21965
28. Burgess S, Bowden J, Fall T, Ingelsson E, Thompson SG. Sensitivity analyses for robust causal inference from Mendelian randomization analyses with multiple genetic variants. Epidemiology. 2017;28(1):30–42. doi:10.1097/EDE.0000000000000559
29. Yang M, Wu H, Zhao M, Long H, Lu Q. Vitamin D status in patients with autoimmune bullous dermatoses: a meta-analysis. J Dermatol Treat. 2022;33(3):1356–1367. doi:10.1080/09546634.2020.1810606
30. Joshi N, Minz RW, Anand S, Parmar NV, Kanwar AJ. Vitamin D deficiency and lower TGF-beta/IL-17 ratio in a North Indian cohort of pemphigus vulgaris. Bmc Res Notes. 2014;7(1):536. doi:10.1186/1756-0500-7-536
31. White MA, Hoffman VM, Yale M, Strong R, Tomayko MM. Psychosocial burden of autoimmune blistering diseases: a comprehensive survey study. J Eur Acad Dermatol. 2024. doi:10.1111/jdv.20156
32. Ghodsi SZ, Asadi A, Ghandi N, et al. Family impact of pemphigus disease in an Iranian population using the family dermatology life quality index. Int J Womens Dermatol. 2020;6(5):409–413. doi:10.1016/j.ijwd.2020.09.004
33. Wimalawansa SJ. Physiology of vitamin D-focusing on disease prevention. Nutrients. 2024;16(11). doi:10.3390/nu16111666
34. Raza I, Clarke AJ. B cell metabolism and autophagy in autoimmunity. Front Immunol. 2021;12:681105. doi:10.3389/fimmu.2021.681105
35. Khan A, Singh A, Madke B, Bhatt DM, Jangid SD. A comprehensive review on the efficacy of anti-CD20 therapies in pemphigus treatment. Cureus J Med Sci. 2024;16(4):e58834. doi:10.7759/cureus.58834
36. Daryabor G, Gholijani N, Kahmini FR. A review of the critical role of vitamin D axis on the immune system. Exp Mol Pathol. 2023;132–133:104866. doi:10.1016/j.yexmp.2023.104866
37. de Carvalho JF, Skare TL, Martinez A, Shoenfeld Y. Anti-vitamin D antibodies. Autoimmun Rev. 2025;24(2):103718. doi:10.1016/j.autrev.2024.103718
38. Bastyte D, Tamasauskiene L, Stakaitiene I, et al. Relation of T cell profile with vitamin D receptor and vitamin D-binding protein gene polymorphisms in atopy. Int J Mol Sci. 2024;25(16):9021. doi:10.3390/ijms25169021
39. Ansari MA, Singh PK, Dar SA, et al. Deregulated phenotype of autoreactive Th17 and Treg clone cells in pemphigus vulgaris after in-vitro treatment with desmoglein antigen (Dsg-3). Immunobiology. 2023;228(2):152340. doi:10.1016/j.imbio.2023.152340
40. Chovatiya R, Silverberg JI. Association of pemphigus and pemphigoid with osteoporosis and pathological fractures. Arch Dermatol Res. 2020;312(4):263–271. doi:10.1007/s00403-019-02010-y
41. Aberger S, Schreiber N, Pilz S, Eller K, Rosenkranz AR, Kirsch AH. Targeting calcitriol Metabolism in acute vitamin D toxicity-A comprehensive review and clinical insight. Int J Mol Sci. 2024;25(18):10003. doi:10.3390/ijms251810003
42. Amber KT, Valdebran M, Grando SA. Non-desmoglein antibodies in patients with pemphigus vulgaris. Front Immunol. 2018;9:1190. doi:10.3389/fimmu.2018.01190
43. Alshami ML, Aswad F, Abdullah B. Desmogleins 1, 3, and E-cadherin immunohistochemical expression within mucocutaneous pemphigus vulgaris. Pan Afr Med J. 2022;42:186. doi:10.11604/pamj.2022.42.186.35429
44. Sivasankar S, Xie B. Engineering the interactions of classical cadherin cell-cell adhesion proteins. J Immunol. 2023;211(3):343–349. doi:10.4049/jimmunol.2300098
45. Bikle DD. Role of vitamin D and calcium signaling in epidermal wound healing. J Endocrinol Invest. 2023;46(2):205–212. doi:10.1007/s40618-022-01893-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Causal Relationship Between Immune Cells and Venous Thromboembolism: A Bidirectional Two-Sample Mendelian Randomization Study
Su Q, Li Y, Wen C, Li L, Ye Q, Chen M, Xie L, Hu C, Wu H
Vascular Health and Risk Management 2025, 21:181-195
Published Date: 25 March 2025