")
Back to Journals » Journal of Inflammation Research » Volume 17
A Challenging Diagnosis of Behçet’s Disease Starting from Unexplained Fever Recurrence with Pulmonary Embolism: A Case Report
Authors Liu R, Ji T , Jiang Y, Li H
Received 19 March 2024
Accepted for publication 22 August 2024
Published 29 August 2024 Volume 2024:17 Pages 5801—5805
DOI https://doi.org/10.2147/JIR.S466840
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Rong Liu,1,* Tingfen Ji,1,2,* Yixia Jiang,1 Hequan Li1
1Department of Respiratory Medicine, The First Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Respiratory and Critical Care Medicine, Lishui People’s Hospital, Lishui, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hequan Li, Email [email protected]
Purpose: Recurrent inflammatory fevers with multisystem involvement occur clinically and may indicate an autoimmune disease.
Case: We present a young male diagnosed with pulmonary embolism who experienced recurrent fever during hospitalization and was unresponsive to antibiotics and antipyretics. A follow-up history revealed chronic oral and genital ulcers, leading to a final diagnosis of Behçet’s disease.
Conclusion: The patient’s temperature normalized rapidly after corticosteroid therapy, and infection markers returned to normal. Complete remission was achieved with immunosuppression and glucocorticoid therapy. Reporting characteristics, treatment experience, and outcomes of such cases are essential to inform future diagnosis and management strategies.
Keywords: fever, Behçet’s disease, pulmonary embolism, atrial mass
Introduction
Recurrent inflammatory fevers with multisystem involvement occur clinically, and autoimmune diseases are important diagnoses to consider in such patients. Behçet’s disease (BD) is a chronic systemic inflammatory vasculitis affecting arterial and venous vessels across various organs.1 The disease presents with a wide range of clinical manifestations, including cutaneous, joint, digestive, pulmonary, and cardiovascular manifestations.2 This variability necessitates the involvement of physicians from multiple specialties, making early diagnosis challenging.
We describe the unusual case of a young male who was initially presented with fever and pulmonary embolism. His fever persisted despite treatment with antibiotics, antipyretics, and other conventional therapies, leading to a final clinical diagnosis of BD.
Case Presentation
A 35-year-old male with a 2-day history of chest tightness and fever was admitted to the emergency department on July 13, 2022. His medical history included lower extremity venous thrombosis, pulmonary nodules, cardiac surgery, and hypertension. Two days ago, he experienced significant dyspnea accompanied by intermittent fever and chills. His physical examination revealed a temperature of 38.7°C, with rapid respiration but no other obvious abnormalities. The laboratory results were as follows: WBC, 12.65 × 109/L; neutrophils, 85%; CRP, 65 mg/L; ESR, 55 mm/h; and D-dimer, 26.12 mg/L. Venous ultrasound revealed thrombosis in the common femoral vein, bilateral external iliac veins, and left superficial femoral vein in both lower limbs. ECG indicated sinus tachycardia. Pulmonary CTA indicated embolism in both lower pulmonary artery branches, a new embolus in the right lower pulmonary artery branch, and exudative changes in the lower lobes of both lungs (Figure 1a and b).
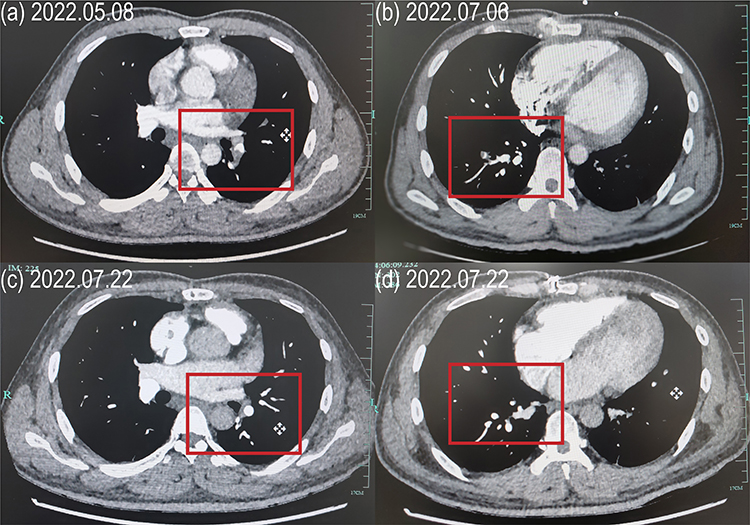 |
Figure 1 Imaging changes in CTA contrast enhancement of the pulmonary artery at the same level before and after treatment. (a and b) CTA images indicating occlusion of the lower lobe branches of the right and left pulmonary arteries before treatment. (c and d) CTA images after two weeks of hormonal and immunosuppressive therapy. |
The patient was transferred to the respiratory department with a diagnosis of pulmonary embolism (PE). During the night, his temperature spiked to 39.5°C, accompanied by chills. Despite an empirical escalation of anti-infective therapy with meropenem and linezolid, his fever persisted, reaching a peak of 39.8°C on the fifth day of hospitalization. Blood and sputum cultures were negative. The patient reported experiencing a similar high fever two months earlier following cardiac surgery, which had subsided with anti-infective and antipyretic treatment. Two months earlier, an esophageal echocardiogram had indicated a hyperechoic right atrium with a widened coronary sinus (Figure 2a). On May 13, 2022, he underwent surgery to remove an intracardiac mass. Intraoperative findings revealed a 3 × 3 cm cystic mass containing yellow cloudy fluid in the coronary sinus of the right atrium. Intraoperative cryopathologic analysis indicated inflammatory exudation with necrotic tissue and infiltration of inflammatory cells (Figure 2b). The cardiology department consulted with hematology, infection, and vascular departments before and after the surgery, suspecting tuberculosis and fungal infection; however, a definitive diagnosis was not reached. Physical examination revealed multiple ulcers (0.2–0.8 cm in diameter) on the patient’s bilateral lower extremities, groin, and scrotum, along with scattered old rashes. Examination of the oropharynx indicated multiple ulcers on the tongue and labium.
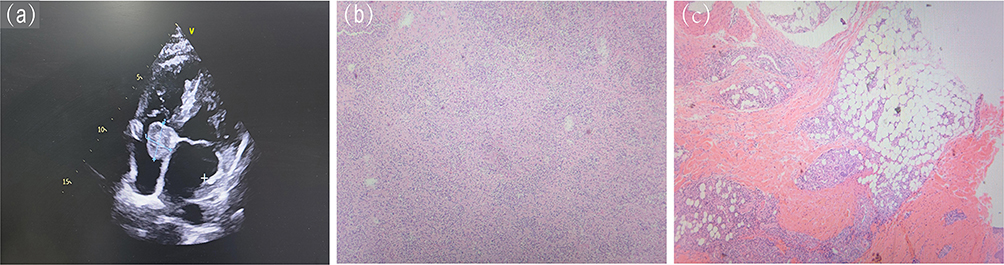 |
Figure 2 (a) Ultrasound imaging of the right atrial mass. (b) Postoperative pathology of the atrial mass. (c) Skin biopsy: epidermal ulceration with lipofuscinosis. |
On the 7th day of hospitalization, the patient underwent a skin biopsy, which revealed epidermal ulceration with lipofuscinosis (Figure 2c). BD was diagnosed after a multidisciplinary discussion involving rheumatology, cardiac microvascular surgery, pathology, dermatology, vascular surgery, and ultrasonography, based on the International Criteria for Behçet’s Disease (ICBD). After multidisciplinary consultation, a treatment plan was initiated, including methylprednisolone at 80 mg per day for two weeks, with 60 mg per day for three months (reduced by 5 mg weekly to reach 5 mg daily), cyclosporine at 200 mg per day, and warfarin to maintain a target international normalized ratio of 2.0–3.0. The patient’s temperature normalized rapidly after starting treatment, with ESR and CRP levels returning to the normal range. He was discharged 14 days after admission without significant adverse reactions. Two weeks post-treatment, pulmonary artery CTA indicated the disappearance of emboli in the right lower pulmonary branch and a reduction in the size of emboli in the left lower pulmonary branch (Figure 1c and d). The patient remained in remission during nine months of follow-up, with regular adjustments to his medication by rheumatology.
Discussion
BD is a chronic, relapsing, autoimmune vasculitis that affects multiple systems and is characterized by recurrent oral and genital aphthous ulcers, ocular disease, and skin lesions. No single presentation is definitive for its diagnosis.1 BD predominantly affects young adult males and is most commonly observed along the Silk Road, with prevalence rates ranging from 20 to 420 per 100,000 in Turkey and 80 per 100,000 in Iran, to 0.64 per 100,000 in the UK.3
In our clinical case, the patient had a history of recurrent mucocutaneous lesions, including oral and genital ulcers, which are key clinical features of BD. In retrospect, he met the diagnostic criteria for BD (ICBD score ≥ 4 points4), but the diagnosis was delayed for many years due to the patient’s lack of attention to these symptoms. This case underscores the importance of conducting a comprehensive physical examination. When a patient presents with specific symptoms, a thorough physical examination, coupled with a detailed medical history, can guide the physician toward the correct diagnosis.
Fever was a recurrent symptom in this patient, and repeated unexplained high fevers should raise concern. The patient was presented with a fever during both hospitalizations at our facility. Based on his clinical presentation and examination findings, we identified common causes of fever, such as sepsis, lymphoma, and common connective tissue diseases. PE was another significant manifestation in this case, making septic pulmonary embolism (SPE) a consideration. In patients with a systemic acute inflammatory response or sepsis, SPE should be suspected if there are signs and symptoms of pulmonary involvement.5 The focus of SPE is on identifying the primary source of infection and initiating appropriate anti-infective therapy.6 Although infectious fever was initially considered, and symptomatic treatment with antipyretics and antibiotics was administered, escalating antibiotics failed to reduce the fever. This indicated the need for further clinical evaluations and additional considerations, especially when the patient lacks a history of trauma or other factors typically associated with PE. Ultimately, BD-associated vasculitis explained the patient’s condition.
The thrombotic manifestations of BD are believed to result from active vasculitis in the affected vascular bed, most commonly in the venous vessels of the lower extremities, though the cardiovascular system can also be involved.7,8 Our patient initially presented with lower extremity venous thrombosis, and subsequent treatments with warfarin and rivaroxaban yielded unsatisfactory results. Systemic anticoagulation is the cornerstone of treatment for venous thromboembolism, regardless of the underlying cause. However, in this case, the thrombosis was due to BD-induced vasculitis, and anticoagulation alone was insufficient to control the disease. The patient was later found to have an atrial heart mass and PE, which is relatively uncommon in BD. When a young patient presents with a right atrial mass, it is important to identify not only myxoma but also malignancy, infectious vegetation, and intra-atrial thrombus. Additionally, in cases of unexplained PE with uncertain risk factors and a poor response to anticoagulation, considerations should include thrombotic disorders, infectious diseases, autoimmune diseases, and cancer (Figure 3). Autoimmune disorders such as systemic lupus erythematosus (SLE) and antiphospholipid antibodies (APLA) can be present with thrombotic events. SLE patients, particularly those under 35 years old, have an elevated risk of deep vein thrombosis and PE.9 Acquired thrombophilia, such as APLA, plays a significant role in the development of chronic thromboembolic pulmonary hypertension.10 Young patients who experience unprovoked PE or PE triggered by minor risk factors should be tested for autoantibodies, including APLA.10 PE may also indicate underlying thrombotic disorders, possibly related to a hypercoagulable state, such as the Factor V Leiden mutation.11 Therefore, systematic testing of the coagulation system and gene sequencing are warranted when necessary. The right atrial mass, in this case, was determined to be an intracardiac thrombus after multidisciplinary consultation. Patients who are initially present with cardiac or cardiovascular manifestations often undergo multiple visits or referrals before a diagnosis of BD is made. The high rates of underdiagnosis and misdiagnosis of BD, particularly when it involves the cardiovascular and pulmonary systems, should be taken seriously.
 |
Figure 3 Flow diagram of diagnostic ideas and differential diagnosis in the manifestation of right atrial mass and pulmonary embolism in our case. |
Conclusion
Our report underscores that recurrent, unexplained fever and PE, particularly in a young male, should prompt strong suspicion of BD or other autoimmune disorders. A thorough history, including inquiries about oral and genital ulcers as well as skin conditions, should be obtained, and a comprehensive physical examination should be conducted. Immunosuppressive therapy combined with anticoagulation is currently the preferred treatment approach. Further dissemination of clinical experiences and studies is essential to enhance clinicians’ understanding of BD and explore treatment options in greater depth.
Abbreviations
BD, Behçet’s disease; PE, Pulmonary embolism; SPE, Septic pulmonary embolism; SLE, Systemic lupus erythematosus; APLA, antiphospholipid antibodies.
Ethics Statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article. Ethical review and approval were not required to publish the case details in accordance with the institutional requirements.
Acknowledgments
We thank the Home for Researchers editorial team (www.home-for-researchers.com) for language editing service.
Funding
The National Natural Science Foundation of China (81970015) and Zhejiang Province Social Welfare Project (2023C03161).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Saadoun D, Wechsler B. Behçet’s disease. Orphanet J Rare Dis. 2012;7(1):20.
2. Tong B, Liu X, Xiao J, Su G. Immunopathogenesis of Behcet’s Disease. Front Immunol. 2019;10:665. doi:10.3389/fimmu.2019.00665
3. Davatchi F, Chams-Davatchi C, Shams H, et al. Behcet’s disease: epidemiology, clinical manifestations, and diagnosis. Expert Rev Clin Immunol. 2017;13(1):57–65. doi:10.1080/1744666X.2016.1205486
4. International Study Group for Behçet’s Disease. Criteria for diagnosis of Behçet’s disease. International study group for Behçet’s disease. Lancet. 1990;335(8697):1078–1080.
5. Sheikh Najeeb M, Alshwaiki A, Martini N, Alsuliman T, Alkharat B, Alrstom A. Acute osteomyelitis, thrombophlebitis, and pulmonary embolism: a case report. J Med Case Rep. 2023;17(1):471. doi:10.1186/s13256-023-04172-w
6. Valerio L, Baddour LM. Septic pulmonary embolism: a contemporary profile. Semin Thromb Hemost. 2023;49(8):840–847. doi:10.1055/s-0042-1758742
7. Calamia KT, Schirmer M, Melikoglu M. Major vessel involvement in Behçet’s disease: an update. Curr Opin Rheumatol. 2011;23(1):24–31. doi:10.1097/BOR.0b013e3283410088
8. Geri G, Wechsler B, Huong D Le T, et al. Spectrum of cardiac lesions in Behçet disease: a series of 52 patients and review of the literature. Medicine. 2012;91(1):25–34. doi:10.1097/MD.0b013e3182428f49
9. Zhao Y, Huang C, You H, et al. Prognostic factors of systemic lupus erythematosus patients with pulmonary embolism: an 11-year cohort study. Lupus. 2022;31(7):885–890. doi:10.1177/09612033221095149
10. Zhu R, Cheng GY, Denas G, Pengo V. Antiphospholipid antibodies in chronic thromboembolic pulmonary hypertension. Eur J Intern Med. 2023;111:1–4. doi:10.1016/j.ejim.2023.01.012
11. El Marraki Z, Bouzhir A, Eddhima Z, El Bouanani AE, Mouine N, Benyass A. Homozygous factor V Leiden mutation: rare etiology of pulmonary embolism. Ann Med Surg. 2022;82:104569. doi:10.1016/j.amsu.2022.104569
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.