")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
A Cost-Effectiveness Analysis of Mosunetuzumab vs Tisagenlecleucel for Treatment of Third- or Higher-Line (3L+) Relapsed or Refractory (R/R) Follicular Lymphoma (FL) in Italy
Authors Luminari S, Pinto A, Puccini B, D’Arpino A, Omodeo Salè E, Bellone M , Pradelli L , Sabinot A
Received 17 December 2024
Accepted for publication 25 March 2025
Published 16 April 2025 Volume 2025:17 Pages 335—348
DOI https://doi.org/10.2147/CEOR.S509907
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Stefano Luminari,1,2 Antonio Pinto,3 Benedetta Puccini,4 Alessandro D’Arpino,5 Emanuela Omodeo Salè,6 Marco Bellone,7,* Lorenzo Pradelli,7 Alice Sabinot7,*
1Hematology, Azienda USL IRCCS of Reggio Emilia, Reggio Emilia, Italy; 2CHIMOMO Department, University of Modena and Reggio Emilia, Modena, Italy; 3Hematology-Oncology and Stem Cell Transplantation Unit, Istituto Nazionale Tumori-IRCCS-Fondazione ‘G. Pascale’, Naples, Italy; 4Hematology, Careggi Hospital and University, Florence, Italy; 5Pharmacy Unit, Santa Maria Della Misericordia Hospital, Perugia, Italy; 6Division of Pharmacy, IEO European Institute of Oncology IRCCS, Milan, Italy; 7Department of Health Economics and Outcome Research, AdRes Health Economics and Outcome Research, Turin, Italy
*These authors contributed equally to this work
Correspondence: Marco Bellone, Department of Health Economics and Outcome Research, AdRes Health Economics and Outcome Research, Via Vittorio Alfieri, 17, Turin, 10121, Italy, Tel +39 011 7651239, Email [email protected]
Purpose: To compare the cost-effectiveness of mosunetuzumab with tisagenlecleucel for treating patients with relapsed or refractory follicular lymphoma (R/R FL 3L+) from the perspective of the Italian National Health Service (NHS).
Patients and Methods: The analysis employs a weekly cycle partitioned survival model (PSM) with a lifetime horizon. The PSM model tracks patient outcomes based on time-to-event data, including progression-free survival (PFS) and post-progression survival (PPS). A matching-adjusted indirect treatment comparison (MAIC) approach was used to account for differences in trial population characteristics on the relative efficacy of mosunetuzumab to tisagenlecleucel. PFS and overall survival (OS) were extrapolated beyond the trial period by applying the hazard ratios from the MAIC to mosunetuzumab’s parametric survival curves. Utility values and patient data are retrieved from the GO29781 trial. Economic inputs, from the perspective of the Italian NHS, include direct medical costs such as drugs, administration, monitoring, adverse event (AE) management, therapy following FL progression. Discontinuation and terminal care costs were also considered. Probabilistic sensitivity (PSA) and scenario analyses were conducted.
Results: Mosunetuzumab was found to be dominant compared to tisagenlecleucel, resulting in an increase of 0.98 life years (LYs) and 0.70 quality-adjusted life years (QALYs), while also being associated with lower overall costs. The sensitivity analysis consistently favored mosunetuzumab, with 94% of simulations demonstrating its cost-effectiveness based on the Italian WTP threshold of € 40,000/QALY. Even in a scenario where tisagenlecleucel maintained a PFS advantage with assumed equivalence in OS, mosunetuzumab still showed a favorable cost-saving profile due to its lower incremental costs.
Conclusion: In the Italian setting, mosunetuzumab is a cost-effective treatment option compared to tisagenlecleucel for adult patients with R/R 3L+ FL, presenting favourable outcomes from the perspective of the NHS. Future research and data collection efforts are crucial to validate these findings and reduce uncertainties regarding long-term clinical and economic implications.
Keywords: economic evaluation, oncology, social cost, hospital cost
Introduction
Follicular lymphoma (FL) is a systemic indolent neoplasm of the lymphoid tissue displaying germinal center B cell differentiation. It represents roughly 20–25% of all newly diagnosed non-Hodgkin lymphoma cases in Western countries.1 Even though the 5-year survival rates for FL have been increasing globally, FL remains an incurable disease.2–4
The occurrence and development of FL often go unnoticed, since most patients are asymptomatic in the early stages of the disease. Therefore, patients are often diagnosed with advanced-stage disease,5 leading to early disease progression.6
The Follicular Lymphoma International Prognostic Index (FLIPI) is a useful tool for predicting disease course, and the diagnostic approach to FL has recently evolved, with a focus on understanding its biological and clinical heterogeneity.7,8 Commonly, patients affected by FL experience a reduced quality of life (QoL). Notwithstanding the impact of FL symptoms on physical, emotional, functional, and social well-being – some treatments, particularly chemotherapy, can exacerbate the negative effects.9 A study on health-related QoL in FL patients revealed that those in the “relapsed” category had the lowest well-being scores across various aspects.9
Patients with advanced-stage disease and in need of therapy (Groupe d’Etude des Lymphomes Folliculaires, ie GELF, criteria) are usually treated with anti-CD20 monoclonal antibodies and chemotherapy.10 Currently, there exists a significant medical need for relapsed/refractory (R/R) patients who have undergone extensive treatments. Approximately 20% of FL patients treated with chemo-immunotherapy experience relapse within two years (Progression of Disease-POD24). The occurrence of POD24 is associated with a significant reduction in overall survival (OS), further highlighting the need for highly effective interventions for patients with RR-FL.11
A noteworthy breakthrough in Advanced Therapy Medicinal Products (ATMP) for R/R FL is the approval of tisagenlecleucel, a chimeric antigen receptor T-cell therapy (CAR-T). Despite its high therapeutic potential, CAR-T face challenges related to logistics, accessibility and the necessity for close monitoring for adverse events (AEs) (p3).12 Among the emerging therapeutic options for R/R FL, mosunetuzumab, a novel CD3xCD20 bispecific monoclonal antibody, shows high and durable response rates, achieves quickly and sustained over time.13 Both mosunetuzumab and tisagenlecleucel display a promising benefit profile. Nevertheless, with its intravenous (IV) ready-to-use formulation and manageable safety profile, mosunetuzumab facilitates outpatient administration, avoiding the need for hospitalization.
Due to the lack of randomized comparative trials, an unanchored Matching-Adjusted Indirect Comparison (MAIC)14 was performed and recently updated.15 The relative clinical effectiveness was, thus, calculated by pseudo-randomizing patients from both ELARA and GO29781 trials.13,16
Using data derived from the indirect treatment comparison (ITC), available literature, and regulatory dispositions, a cost-effectiveness analysis was conducted. By using a partitioned survival model (PSM) the aim was to compare cost and effects of mosunetuzumab and tisagenlecleucel for the treatment of R/R FL 3L+ adult patients in the Italian National Health Service (NHS).
Methods
The present cost-effectiveness (CE) analysis compares the lifetime costs and clinical outcomes of mosunetuzumab IV and tisagenlecleucel for the treatment of R/R FL previously treated patients. The CE analysis was conducted via a weekly cycle PSM, consisting of three health states: Progression-free (PF), Post-progression (PP), and Death. The discount rate of future costs and health effects was set at 3.00%17 and a half-cycle correction was applied to the model. By using time-to-event data, the model depicts the proportion of patients in distinct states, such as progression-free, post-progression, and death, relative to the time elapsed since the initiation of a trial. The OS outcome is partitioned into PFS and post-progression survival (PPS) using the PFS curve. All patients that enter the PFS states can either progress to the PPS state or reach the end-of-life, all patients eventually progress to the absorbing death state (Figure 1).
 |
Figure 1 Model Diagram. |
Population
This study was based on patients’ characteristics from the GO29781 trial: adults affected by FL who have previously received at least two lines of therapy but have relapsed or were refractory to previous treatments.13 The CE model considers a population with 61% men, 60 years of age, and an average weight of 81 kg. These data were crucial for estimating life expectancy and the consumption of medications potentially administered based on patient weight.
Clinical Inputs
Time to event data inputs for mosunetuzumab and tisagenlecleucel were derived from the GO29781 trial and ELARA study, respectively.13,16 In the absence of head-to-head clinical trial comparing mosunetuzumab vs tisagenlecleucel, an unanchored MAIC was employed to estimate hazard ratio (HR) with 95% credible interval (CrI) of mosunetuzumab vs tisagenlecleucel for PFS and OS outcomes.15 The Kaplan-Meier (KM) of PFS and OS for mosunetuzumab were based on the individual patient-level data after matching and adjusting for differences in trial population baseline characteristics. These include the proportion of ECOG 1 vs 0, FLIPI ≥3, Ann Arbor Stage III–IV, number of prior therapies, the proportion of refractory to last line, prior anti-CD20 regimen, High LDH, POD24, bulky disease, and prior autologous stem cell transplant (ASCT). A series of parametric distributions were fitted to extrapolate survival beyond the trial period. For tisagenlecleucel, PFS and OS were estimated by applying the HRs from the ITC to the mosunetuzumab survival curves, intended as reference treatment. In particular, the best fitting, according to Akaike (AIC) and Bayesian Information Criterion (BIC) and visual inspection, was reached by lognormal and exponential parametric distribution functions to the PFS and OS KM data for mosunetuzumab treatments, respectively. The ITC results (OS: 0.86, 95% CrI: 0.15–1.93; PFS: 1.73, 95% CrI: 1.10–2.75; Table 1 and Figure 2) were used to obtain tisagenlecleucel survival curves.14,15 The model also accounts for age- and gender-specific Italian background mortality.
 |
Table 1 MAIC Results Presented as Hazard Ratio |
 |
Figure 2 Modelled Progression-Free Survival and Overall Survival Curves. Notes: (a) Modelled PFS curves for mosunetuzumab (mosu) and tisagenlecleucel (tisag); (b) Modelled OS curves for mosunetuzumab (mosu) and tisagenlecleucel (tisag). |
Time-to-off treatment (TTOT) defines the proportion of patients in PFS vs those who interrupted the treatment for any reason. For mosunetuzumab, the TTOT estimate was derived from survival trends observed in GO29781 trial,13 whereas tisagenlecleucel is administered as a one-time treatment.
Utility Values
The results of EuroQoL 5 Dimension-5 Level (EQ-5D-5L) analysis from the GO29781 study, by applying Italian population tariffs,18 informed the PFS and PPS utility values in the model.13 These estimates were also adjusted by applying the health state utility values coefficient for capturing age-related utility losses and determining quality-adjusted life years (QALYs) for each cycle in each treatment in the Italian context. Utility values are also modelled according to the on/off treatment status of patients, as well as adapted to severe AEs (grade > 3) to appraise disutilities (Table 2).
 |
Table 2 Utilities |
Economic Inputs
Being the perspective of the analysis of the Italian NHS, the model considered direct medical costs only, namely drugs, administration, monitoring, AEs management, therapy following FL progression, and end-of-life costs. Drug costs were derived from their specific ex-factory net prices with confidential rebates (maximum hospital tender price). For mosunetuzumab IV, drug costs were calculated based on its dosage – as defined in the Summary of Product Characteristics (SPC).19 More specifically, mosunetuzumab was IV administered for a fixed duration of 8 cycles for patients who achieved a complete response, up to a maximum of 17 cycles for those who achieved a partial response or maintained a stable disease. Tisagenlecleucel is administered as a single infusion20 (Table 3). As per mosunetuzumab administration costs, it was valued with a reduction of 90% in the Disease-Related Group (DRG) 410 tariff, as recommended in the Regional Directorate Decree No. 26/35 of 6.07.2010.21 Conversely, due to the presence of overlapping patient management aspects (ie apheresis procedures, conditioning therapies, and in-hospital infusions) the DRG481, which is specific to bone marrow transplantation, was applied for tisagenlecleucel infusion (Table 4).22
 |
Table 3 Dosing Schedules |
 |
Table 4 Costs of Drug Administration, Adverse-Event Management, Post Progression Therapy, and Terminal Care |
Disease and therapy monitoring was valued according to the Nomenclatore Specialistico, and their resource consumption, based on Associazione Italiana di Oncologia Medica (AIOM) guidelines.22,25 As per AEs’ management costs, were calculated on the average number of events per patient-week and their cost, as retrieved from individual DRGs and literature (Table 4).22,23 Post-progression discontinuation costs were applied as one-offs, based on individual treatment utilization rates – prevalence rates were estimated from a market analysis conducted in Italy (data on file) – and their average duration as found in literature. Similarly, terminal care costs were valued according to a literature estimate.24
Outcome Measures
Results are presented as three main outcome measures. Whereas the incremental cost-effectiveness ratio (ICER) quantifies costs associated per life-years (LYs) gained, the incremental cost–utility ratio (ICUR) associates economic implications to QALYs.
Sensitivity Analysis
Deterministic sensitivity (DSA) and probabilistic sensitivity (PSA) analyses were conducted to assess the robustness of the base-case results.
The DSA results are presented on the tornado diagram to determine how sensitive the results are to deviations in the input parameters. As per the main outcome of interest, while performing the DSA, the Incremental Net Monetary Benefit (INMB) was considered. The core calculation behind of INMB multiplies incremental QALYs by the Italian willingness-to-pay threshold (arbitrarily fixed at €40,000) and incremental costs. Applying INMB it is possible to determine which intervention offers the most value for money within a given budget constraint. If the INMB is >0, the treatment of interest results cost-effective; if <0 it is not cost-effective vs the comparator.
PSA was conducted on 1000 iterations to assess the uncertainty around the ICER in the base case scenario and it is represented on the incremental CE-plane. In this regard, the incremental CE-plane shows the dispersion of the 1000 incremental cost-effectiveness ratios, intended as the ratio between the incremental costs and incremental benefits between mosunetuzumab IV and tisagenlecleucel. To determine the CE of mosunetuzumab IV versus tisagenlecleucel, the Italian Willingness to Pay (WTP) threshold was set at €40,000 per health benefit gained.
Furthermore, a series of scenario analyses were conducted. The first analysis aimed to assess the OS equivalency assumption (HROS=1). Secondly, a bidirectional analysis was performed by varying the clinical efficacy values simultaneously, applying the maximum, minimum, and a mix of their extreme values within the HR variability range of PFS and OS. Results were displayed on the incremental CE plane.
The third type of scenario analyses – aimed at inspecting results over time – dealt with conducting the cost-effectiveness analysis at different time-points (1, 5, 10 and 30 years).
Results
Base Case
Mosunetuzumab exhibits a superior efficacy over tisagenlecleucel in terms of discounted LYs and QALYs, with observed increases of 0.98 LYs and 0.70 QALYs in patients that are first administered with the bispecific monoclonal antibody. The monoclonal antibody dominated the comparator in the base-case scenario (Table 5 and Table 6).
 |
Table 5 Base-Case LYs, QALYs, and Costs |
 |
Table 6 Base-Case Results |
Sensitivity Analyses
The tornado diagram – yielded from the DSA – shows the key drivers influencing the per-patient INMB of mosunetuzumab vs tisagenlecleucel, with a base case INMB of €181,804. The most impacting contributor to INMB variation is the cost of tisagenlecleucel, ranging from -€32,334 to €32,334. This shows that, as the cost of tisagenlecleucel increases, mosunetuzumab becomes more favorable. Utility values in PPS and PFS states also impact INMB, ranging from -€22,401 to €22,401, and -€16,758 to €16,758, respectively. Lesser but notable factors to consider are mosunetuzumab post-discontinuation therapy cost (-€15,219 to €15,219) and tisagenlecleucel infusion cost (-€9755 to €9755). Costs related to post-discontinuation therapy for tisagenlecleucel, percentage discounts, and AE management had a marginal impact on the INMB (Figure 3).
 |
Figure 3 Deterministic Sensitivity Analysis. Abbreviations: INMB, Incremental Net Monetary Benefit; AE, adverse event. |
In the PSA, the base-case is located in the fourth quadrant of the cost-effectiveness plane, representing mosunetuzumab dominance over tisagenlecleucel. Applying a conventional WTP threshold of €40,000 per unit of gained benefit, mosunetuzumab is dominant in 57%, cost-effective in 37%, and not cost-effective in 6% of simulations (Figures 4 and 5).
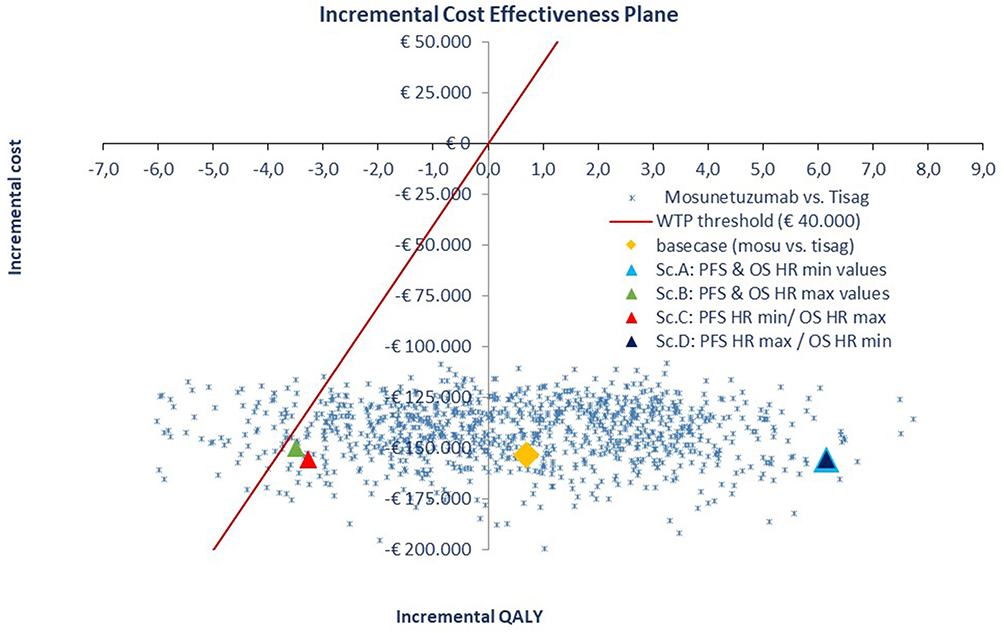 |
Figure 4 Incremental Cost-Effectiveness Plane. Abbreviations: Sc, Scenario; WTP, willingness- to-pay. Notes: The yellow diamond represents the deterministic case (base case). Scenario A (light blue icon) represents both minimum values of HR for PFS and OS; Scenario B (green icon) represents both maximum values of HR for PFS and OS; Scenario C (red icon) represents the minimum value of HR for PFS and the maximum for OS; Scenario D (blue icon) represents the maximum value of HR for PFS and the minimum for OS. |
 |
Figure 5 Probability of Being the Most Cost-Effective Treatment. Abbreviation: WTP, willingness- to-pay. Notes: (a) Base-Case, (b) Scenario Analysis. |
Scenario Analyses
In the scenario analysis maintaining tisagenlecleucel’s advantage in prolonging PFS yet assuming OS equivalence, mosunetuzumab is associated with lower costs (Table 7). Instead, results of bidirectional sensitivity analyses were presented in the CE plane: the distribution of these scenario results demonstrates their variability, which is strongly influenced by the modeled relative efficacy.
 |
Table 7 Scenario (HROS=1) Analysis Results |
The results of time horizon scenarios align with those of the base-case. Indeed, mosunetuzumab held an INMB>0 at all timepoints, which suggests its favorable cost-saving profile is maintained over time (Table 8).
 |
Table 8 Scenario Analysis Results at Different Timepoints |
Discussion
The present study is the first cost-effectiveness analysis that compares mosunetuzumab and tisagenlecleucel from the Italian NHS perspective. Our research is supported by a US-payer perspective study, which provides insights from a different healthcare setting, yet applies the same clinical efficacy data derived from the ITC.15 Findings remain consistent, indicating that mosunetuzumab is a more cost-effective alternative than tisagenlecleucel in both the Italian and US settings, despite the differences between the two healthcare systems and the high variability of the effectiveness input data.
A reliance solely on the outcomes of the ITC14 is the primary contributor to heterogeneity, and it presents the main limitation of the present study by potentially introducing quality biases.26 To address this risk, the present analysis comprises a PSA that combines a range of plausible values for the clinical parameters. The result of the PSA, a horizontally elongated iteration cloud, is indicative of the variability and non-significance of the clinical input data. Nevertheless, the positioning of the cloud in the lower quadrants of the cost-effectiveness plane shows mosunetuzumab as a considerably less expensive alternative. This renders mosunetuzumab cost-effective vs tisagenlecleucel in >90% of simulations in the base-case scenario, according to the Italian WTP threshold.
When it comes to corroborating existing evidence, OS data immaturity remains a significant consideration.27 Overall, the intrinsic characteristics of indolent diseases are the main plausible driver of the uncertainty of OS estimates. More precisely, in the ongoing mosunetuzumab trial GO2971, the OS data employed in the current model is deemed immature, with only 11% of events recorded at the latest data cut-off.13 To address the robustness of our evaluation, a scenario analysis that assumes equivalence between mosunetuzumab and tisagenlecleucel in terms of OS was also conducted. Even in this simulation, mosunetuzumab preserves a favorable cost-saving profile.
The present analysis was carried out on the best attainable data, despite its limitations. Overall, mosunetuzumab was proven to be a valid alternative to tisagenlecleucel. From a clinical standpoint, mosunetuzumab demonstrates non-inferiority to tisagenlecleucel in terms of OS, despite the observed differences in PFS.
The ITC results reporting that mosunetuzumab improves overall survival – yet not PFS – can be explained by the nature of FL. A recent literature review found a weak correlation between PFS and OS in FL,28 suggesting that factors beyond initial treatment response play a significant role in long-term outcomes. Indeed, in hematology-oncology, patients receive multiple subsequent therapies, which can mitigate initial differences in PFS and influence OS outcomes over time. The higher PFS observed for tisagenlecleucel may therefore be reflective not only of treatment efficacy but also of differences in patient risk profiles, rather than the intrinsic superiority of one therapy over the other. This distinction plays an important role in cost-effectiveness assessments, as our analysis accounts for the costs of subsequent therapies. While tisagenlecleucel shows an initial advantage in PFS, mosunetuzumab maintains a favorable cost-effectiveness profile over time.
Mosunetuzumab’s administration is also noteworthy, which underlines its cost distinction from tisagenlecleucel. Though CAR-T is administered as a single infusion, it requires a lengthy timeline for manufacturing and administration (vein-to-vein time). This process can last up to a month, not to mention the need for close monitoring, which can lengthen the patient’s pathway to a year-long process.29 Objective patient access barriers still exist related to CAR-T therapy slots availability, which may also vary across different Italian geographic areas. Also, requiring patients to reside within a specific radius from the CAR-T delivery center may contribute to logistical issues in making these treatments more accessible nationwide.
Conversely, mosunetuzumab – administered for a fixed duration of 8 up to a maximum of 17 cycles – may eliminate the need for hospitalization and issues related to the geographical proximity of ATMP centers. Precisely, as per the SmPC label, mosunetuzumab is given for 8 cycles unless toxicity or disease progression occurs. Patients with a complete response stop treatment, while those with a partial response or stable disease continue up to 17 cycles.19 This treatment dynamic is already reflected in the model, as it follows TTOT, PFS, and OS curves from the trial GO2971.13 As seen in a previous per-patient cost of therapy analysis and available literature,30 CAR-T therapies are associated with issues in patient accessibility, especially in the Italian NHS context.31,32 Due to limited availability of ATMP-specialized centers, Italian patients may have to bear additional costs, mostly related to relocation and accommodation expenses. It is estimated that the need for relocation can extend up to 130 days29 which has, undoubtedly, an impact on costs, especially for those living in more remote regions. Furthermore, patients may incur transportation costs for hospital visits, along with productivity losses for hospital stays, post-infusion monitoring, and managing adverse events. Hence, while clinical efficacy remains crucial, it is not the sole determinant to consider when comparing therapeutic options with similar efficacy profiles.
On a general note, equivalent results are attained in a similar therapeutic indication in two non-sponsored studies assessing the cost-effectiveness of CAR-T vs intravenous monoclonal antibodies. When administered to advanced multiple myeloma patients, CAR-T therapies are known to cost up to seven times more than belamaf.33 As of now, CAR-T-cell therapy is unlikely to be cost-effective in respect to the current standard of care in R/R 3L+ FL indication too due to the high pharmaceutical costs.34 This is also shown in our DSA analysis, where the primary driver of INMB for mosunetuzumab variation is the cost of tisagenlecleucel. Overall, this finding aligns with Lin et al’s work as well,35 in which mosunetuzumab stands out as a more cost-effective option compared to both tisagenlecleucel and axicabtagene ciloleucel as treatment for R/R FL 3L+. More specifically, mosunetuzumab not only had lower overall costs but also provided better QALYs vs tisagenlecleucel, leading to a net monetary benefit that was 16-fold higher than that of tisagenlecleucel over a ten-year period. Conversely, another cost-effectiveness analysis comparing mosunetuzumab and axicabtagene ciloleucel presents conflicting results.36 The survival data from a MAIC statistically favors CAR-T compared to mosunetuzumab in terms of PFS27 and – even when assuming equivalent OS for both treatments – CAR-T proved to be cost-effective.36 However, this result excluded a portion of patients in PFS who received CAR-T and were no longer at risk of progression or death from lymphoma after 5 years. Nonetheless, just as in Lin35 and the present study, the uncertainty around OS data led Oluwole et al36 to rely on assumptions. Despite this, the consistent aspect is the significant costs associated with CAR-T therapy throughout all the studies.
Conclusion
In conclusion, ITC results and the high variability in relative effectiveness suggest that the cost savings associated with mosunetuzumab could be a key factor in decision-making, given the current clinical evidence. Such considerations and results underline the need for long-term data collection on both therapies to more precisely define their clinical and cost-effectiveness outcomes.
Abbreviations
AEs, adverse events; AE3+, adverse events grade ≥3AIC, Akaike’s information criterion; AIOM, Associazione Italiana di Oncologia Medica ASCT, Autologous stem cell transplant; ATMP, Advanced Therapy Medicinal Products; BIC, Bayesian information criterion; CAR-T, Chimeric Antigens Receptor Cells-T; CE, cost-effectiveness; CrI, credible interval; DSA, deterministic sensitivity analysis; DRG, disease-related group; DSA, deterministic sensitivity analysis; EQ-5D-5L, EuroQol 5-Dimension 5-level; FL, follicular lymphoma; FLIPI, Follicular Lymphoma International Prognostic Index; HR, hazard ratio; ICER, incremental cost-effectiveness ratio; ICUR, incremental cost-utility ratio; INMB, incremental net monetary benefit; ITC, indirect treatment comparison; IV, intravenous; KM, Kaplan-Meier; LYs, life-years; MAC, macroattivita’ ambulatoriale complessa; MAIC, Matching-Adjusted Indirect Comparison; NHS, Italian National Health Service ; OS, overall survival; PF, progression-free; PFS, progression-free survival; PP, post progression; PPS, post-progression survival; PSA, probabilistic sensitivity analysis; PSM, partitioned survival model; QALYs, quality-of-life adjusted life-years; QoL, Quality of Life; R/R FL 3L+, refractory follicular lymphoma at the second or higher line of therapy; SE, standard error; SPC, Summary of Product Characteristics; TTOT, time-to-off-treatment; WTP, willingness-to-pay.
Acknowledgments
The authors would like to thank Daniela Ghislieri (Market Access Roche SpA Italy) and Alessandra Monguzzi (Medical Affairs Roche SpA Italy) for the contribution provided during the conduction of this research.
Funding
This study was funded by Roche S.p.A.
Disclosure
Dr Marco Bellone and Alice Sabinot are employees of AdRes, which has received project funding from Roche SpA for the development of this research. Marco Bellone reports grants from Sanofi, Fresenius Kabi, Novartis, CSL, and Johnson and Johnson, outside the submitted work. Dr Lorenzo Pradelli is a co-owner and employee of AdRes, which has received project funding from Roche SpA for the development of this research. He also reports grants from Biogen, Sanofi, Fresenius Kabi, Novartis, CSL and Johnson and Johnson, outside the submitted work. Dr Antonio Pinto has received honoraria/consulting fees from Abbvie, BeiGene, Bristol Myers Squibb, Eli Lilly, Hoffmann-La Roche AG, Incyte, Kite-Gilead, Merck Sharp and Dohme and SOBI. Dr Stefano Luminari has received honoraria/consulting fees from BeiGene, Roche, Incyte, Kite-Gilead, Regeneron, Incute, AbbVie, Novartis. Dr Benedetta Puccini, Dr Emanuela Omodeo Salè and Dr Alessandro D’Arpino have received consulting fee from AdRes srl for manuscript writing. The authors report no other conflicts of interest in this work.
References
1. Carbone A, Roulland S, Gloghini A, et al. Follicular lymphoma. Nat Rev Dis Primers. 2019;5(1):1–20. doi:10.1038/s41572-019-0132-x
2. Cerhan JR. Epidemiology of Follicular Lymphoma. Hematol/Oncol Clin North America. 2020;34(4):631–646. doi:10.1016/j.hoc.2020.02.001
3. Bachy E, Seymour JF, Feugier P, et al. Sustained progression-free survival benefit of rituximab maintenance in patients with follicular lymphoma: long-term results of the PRIMA study. J Clin Oncol. 2019;37(31):2815–2824. doi:10.1200/JCO.19.01073
4. Pulsoni A, Assanto GM, Salvatori M, et al. Achieving the cure of follicular lymphoma: is it time to finalize treatment strategies to reach this goal in a subset of patients? Mediterr J Hematol Infect Dis. 2023;15(1):e2023018. doi:10.4084/MJHID.2023.018
5. Pulsoni A, Assanto GM, Salvatori M, et al. Treatment, and follow-up. Dtsch Arztebl Int. 2021;118(18):320–325. doi:10.3238/arztebl.m2021.0022
6. Casulo C. Upfront identification of high-risk follicular lymphoma. Hematol Oncol. 2021;39(S1):88–93. doi:10.1002/hon.2852
7. Randall C, Fedoriw Y. Pathology and diagnosis of follicular lymphoma and related entities. Pathology. 2020;52(1):30–39. doi:10.1016/j.pathol.2019.09.010
8. Relander T, Johnson NA, Farinha P, Connors JM, Sehn LH, Gascoyne RD. Prognostic factors in follicular lymphoma. J Clin Oncol. 2010;28(17):2902–2913. doi:10.1200/JCO.2009.26.1693
9. Pettengell R, Donatti C, Hoskin P, et al. The impact of follicular lymphoma on health-related quality of life. Ann Oncol. 2008;19(3):570–576. doi:10.1093/annonc/mdm543
10. Dreyling M, Ghielmini M, Rule S, et al. Newly diagnosed and relapsed follicular lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2021;32(3):298–308. doi:10.1016/j.annonc.2020.11.008
11. Rodgers TD, Casulo C, Boissard F, Launonen A, Parreira J, Cartron G. Early relapse in first-line follicular lymphoma: a review of the clinical implications and available mitigation and management strategies. Oncol Ther. 2021;9(2):329–346. doi:10.1007/s40487-021-00161-5
12. EMA. GU. C 349/1. 2018. Available from: https://eur-lex.europa.eu/legal-content/IT/TXT/PDF/?uri=uriserv:OJ.C_.2018.349.01.0001.01.ITA.
13. Genentech, Inc. An open-label, multicenter, Phase I/II trial evaluating the safety, efficacy, and pharmacokinetics of escalating doses of mosunetuzumab (BTCT4465A) as a single agent and combined with atezolizumab in patients with relapsed or refractory B-cell non-Hodgkin’s lymphoma and chronic lymphocytic leukemia. clinicaltrials.gov. 2023. Available from: https://clinicaltrials.gov/study/NCT02500407.
14. Bosch F, Kuruvilla J, Vassilakopoulos TP, et al. Indirect treatment comparisons of mosunetuzumab with third- and later-line treatments for relapsed/refractory follicular lymphoma. Clin Lymphoma Myeloma Leuk. 2024;24(2):105–121. doi:10.1016/j.clml.2023.09.007
15. Matasar M, Sanchez Alvarez J, Parisé H, et al. Cost-effectiveness analysis of mosunetuzumab for treatment of relapsed or refractory follicular lymphoma after two or more lines of systemic therapy in the United States. J Med Economics. 2024;(ja):1–36. doi:10.1080/13696998.2024.2352820
16. Fowler NH, Dickinson M, Ghosh M, et al. Assessment of healthcare resource utilization and costs in patients with relapsed or refractory follicular lymphoma undergoing CAR-T cell therapy with tisagenlecleucel: results from the ELARA study. Blood. 2021;138(Supplement 1):3533. doi:10.1182/blood-2021-145741
17. Attema AE, Brouwer WBF, Claxton K. Discounting in economic evaluations. PharmacoEconomics. 2018;36(7):745–758. doi:10.1007/s40273-018-0672-z
18. Scalone L, Cortesi PA, Ciampichini R, et al. Italian population-based values of EQ-5D health states. Value Health. 2013;16(5):814–822. doi:10.1016/j.jval.2013.04.008
19. EMA. Mosunetuzumab. Available from: https://www.ema.europa.eu/en/documents/product-information/lunsumio-epar-product-information_en.pdf.
20. EMA. Kymriah. EMA/CHMP/167689/2022. 2022. Available from: https://www.ema.europa.eu/en/documents/smop/chmp-post-authorisation-summary-opinion-kymriah-ii-44_en.pdf.
21. Conferenze Stato Regioni e Unificata. Available from: http://archivio.statoregioni.it/DettaglioDoc6671.html?IDDoc=28019&IdProv=8583&tipodoc=2&CONF=CSR.
22. Ministero della Salute. Ministero della Salute. Decreto 18 ottobre 2012. Remunerazione prestazioni di assistenza ospedaliera per acuti, assistenza ospedaliera di riabilitazione e di lungodegenza post acuzie e di assistenza specialistica ambulatoriale. (13A00528) (GU Serie Generale n.23 del 28-01-2013 - Suppl. Ordinario n. 8). Available from: https://www.gazzettaufficiale.it/eli/id/2013/01/28/13A00528/sg.
23. Lazzaro C, Bordonaro R, Cognetti F, et al. An Italian cost-effectiveness analysis of paclitaxel albumin (nab-paclitaxel) versus conventional paclitaxel for metastatic breast cancer patients: the COSTANza study. Clinicoecon Outcomes Res. 2013;5:125–135. doi:10.2147/CEOR.S41850
24. Scaccabarozzi G, Limonta F, Amodio E. Hospital, local palliative care network and public health: how do they involve terminally ill patients? Eur J Public Health. 2016;27(1):25–30. doi:10.1093/eurpub/ckw152
25. Associazione Italiana Oncologia Medica, AIOM. Linee guida Linfomi. Edizione 2018. Italian. Available from: https://www.aiom.it/linee-guida-aiom/.
26. Phillippo DM, Dias S, Elsada A, Ades AE, Welton NJ. Population adjustment methods for indirect comparisons: a review of national institute for health and care excellence technology appraisals. Int J Technol Assess Health Care. 2019;35(3):221–228. doi:10.1017/S0266462319000333
27. Ray MD, Kanters S, Beygi S, et al. Matching-adjusted indirect comparisons of axicabtagene ciloleucel to mosunetuzumab for the treatment of relapsed/refractory follicular lymphoma. Transplant Cell Ther. 2024;30(9):885.e1–885.e11. doi:10.1016/j.jtct.2024.06.016
28. Milrod CJ, Kim KW, Raker C, Ollila TA, Olszewski AJ, Pelcovits A. Progression-free survival is a weakly predictive surrogate end-point for overall survival in follicular lymphoma: a systematic review and meta-analysis. Br J Haematol. 2024;204(6):2237–2241. doi:10.1111/bjh.19449
29. Jagannath S, Joseph N, Crivera C, et al. Component Costs of CAR-T Therapy in Addition to Treatment Acquisition Costs in Patients with Multiple Myeloma. Oncol Ther. 2023;11(2):263–275. doi:10.1007/s40487-023-00228-5
30. Bellone M, Sabinot A, D’Arpino A, Omodeo Salè E, Ghislieri D, Pradelli L. A one-year per-patient cost of therapy administration analysis of mosunetuzumab and tisagenlecleucel in relapsed or refractory follicular lymphoma patients receiving two or more lines of systemic therapy. Glob Reg Health Technol Assess. 2024;11:239–247. doi:10.33393/grhta.2024.3170.
31. Cavallo MC, Cavazza M, Bonifazi F, et al. Cost of implementing CAR-T activity and managing CAR-T patients: an exploratory study. BMC Health Serv Res. 2024;24(1):121. doi:10.1186/s12913-023-10443-5
32. Foglia E, Garagiola E, Ladisa V, et al. Multidimensional results and reflections on CAR-T: the Italian evidence. Int J Environ Res Public Health. 2023;20(5):3830. doi:10.3390/ijerph20053830
33. Kapinos KA, Hu E, Trivedi J, Geethakumari PR, Kansagra A. Cost-effectiveness analysis of CAR T-cell therapies vs antibody drug conjugates for patients with advanced multiple myeloma. Cancer Control. 2023;30:10732748221142945. doi:10.1177/10732748221142945
34. Potnis KC, Di M, Isufi I, et al. Cost-effectiveness of chimeric antigen receptor T-cell therapy in adults with relapsed or refractory follicular lymphoma. Blood Adv. 2023;7(5):801–810. doi:10.1182/bloodadvances.2022008097
35. Lin MH. Cost effectiveness of mosunetuzumab and CAR-T cell therapy in relapsed/refractory follicular lymphoma. 2023. Available from: https://ash.confex.com/ash/2023/webprogram/Paper182244.html.
36. Oluwole OO, Ray MD, Zur RM, et al. Cost-effectiveness of treating relapsed or refractory 3L+ follicular lymphoma with axicabtagene ciloleucel vs mosunetuzumab in the United States. Front Immunol. 2024;15:1393939. doi:10.3389/fimmu.2024.1393939
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.