")
Back to Journals » Journal of Inflammation Research » Volume 18
A Multicenter Study for Establishing Reference Intervals of Serum GDF-15 Levels Based on the Chinese Population
Authors Chen K, Fan X, Wu J, Chen S, Yang J, Shen L, Liu Z, Yuan H
Received 10 March 2025
Accepted for publication 12 July 2025
Published 18 July 2025 Volume 2025:18 Pages 9495—9504
DOI https://doi.org/10.2147/JIR.S523980
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Ke Chen,1 Xuesong Fan,1,2 Junyi Wu,1 Siyu Chen,1 Jiashu Yang,1 Linlin Shen,1 Zihan Liu,1 Hui Yuan1
1Department of Clinical Laboratory, Beijing Anzhen Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Neurological Surgery, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA
Correspondence: Hui Yuan, Department of Clinical Laboratory, Beijing Anzhen Hospital, Capital Medical University, Anzhen Road No. 2, Chaoyang District, Beijing, 100029, People’s Republic of China, Email [email protected]
Purpose: Growth differentiation factor 15 (GDF-15) is a stress-responsive cytokine mostly linked to pathological conditions including inflammation, myocardial ischemia, and cancer. We aimed to establish reference intervals (RIs) for GDF-15 in a large, multicenter cohort of apparently healthy Chinese individuals.
Patients and Methods: Adopting unified and stringent criteria, 8,488 eligible subjects from six representative cities in China were enrolled. Serum GDF-15 concentrations were measured with the Maccura Biotechnology i3000 automatic chemiluminescence analyzer and its corresponding reagents. Outliers were identified using the Tukey’s test. To determine the need for partitioning by age and sex, we conducted a two-level nested analysis of variance (ANOVA), considering an standard deviation ratio (SDR) > 0.3 as indicative of notable subgroup differences. The 2.5th and 97.5th percentiles of the RIs were established using non-parametric statistical methods, with 90% confidence interval.
Results: A total of 7,764 participants were included in the data analysis, with 724 outliers excluded. GDF-15 levels displayed a skewed distribution as confirmed by the Kolmogorov–Smirnov test. GDF-15 levels increased with age (All P < 0.001) and were higher in males than in females (all P < 0.001, except 18– 29 years, P = 0.373). The SDR from the two-level nested ANOVA for different age intervals and sex were 0.83 and < 0.01. Age- and sex-specific RIs for serum GDF-15 were established based on the study cohort.
Conclusion: Our study indicates that GDF-15 levels in the Chinese population are comparable to those observed in European populations, with the exception of sex-based differences.
Keywords: growth differentiation factor 15, non-parametric method, reference intervals
Introduction
Growth differentiation factor 15 (GDF-15) is a member of the transforming growth factor-β (TGF-β) cytokine superfamily and is secreted into the circulation as a homodimer.1 Under physiological conditions, GDF-15 is expressed at low levels in most tissues except the placenta and its levels can vary with factors such as exercise, pregnancy, and aging.2,3 However, GDF-15 can be markedly upregulated in response to inflammatory cytokines, oxidative stress, and hypoxia in various cell types, functioning as a stress-inducible cytokine.4
Recently, interest in GDF-15 as a prognostic marker for cardiovascular disease has grown, with studies demonstrating that GDF-15 provides incremental prognostic value independent of traditional risk factors and established biomarkers.5–8 Additionally, two prespecified GDF-15 cut-off levels—1200 and 1800 ng/L—have shown promise for risk stratification and guiding invasive treatment strategies in patients with non-ST-elevation acute coronary syndrome (NSTE-ACS).9 These thresholds are based on tertiles of GDF-15 levels in NSTE-ACS patients,5 with the 1200 ng/L threshold also corresponding to the 90th percentile and proposed as the upper reference limit in a study of 429 apparently healthy elderly individuals.10 Elevated levels of GDF-15 have been associated with poor cardiovascular health, subclinical disease, and increased all-cause, cardiovascular, and non-cardiovascular mortality in community-dwelling individuals, supporting its potential role as a biological marker of aging.11,12 Therefore, it is important to characterize the distribution of GDF-15 in healthy populations. Most existing research on GDF-15 reference intervals (RIs) is based on data from Western populations, which limits the direct applicability of these RIs to non-Western populations such as China.13–15 Additionally, genetic differences contribute to inter-individual variations in GDF-15 levels.16
In this study, we aimed to establish RIs for GDF-15 in a large, multicenter cohort of apparently healthy Chinese individuals. Additionally, we sought to explore age- and sex-stratified reference ranges for GDF-15 to better understand its distribution across demographic subgroups within this population.
Materials and Methods
Study Population
This multicenter study was conducted across six cities in China, namely Changsha, Shenyang, Ningxia, Chengdu, Hangzhou, and Nanning, over the period from June to December 2020 with a total of 10,618 adults was recruited into the cohort. The study population was derived from a previously published study,17 which focused on establishing RIs for blood lipids and homocysteine in the Chinese population. However, the inclusion and exclusion criteria were specifically refined in the present study to align with the objective of evaluating GDF-15 as a biomarker. Eligible participants were 18 years or older with a body mass index (BMI) between 18.5 and 28 kg/m². Exclusion criteria included a medical history of diabetes mellitus, hypertension, coronary artery disease, stroke, liver or kidney diseases, or cancer; any surgery within the past six months; active infections; recent or continued use of alcohol, tobacco, or oral contraceptives; medication use in the past two weeks; hospitalization within the past month; and pregnancy within the past year. Participants with abnormal blood lipid or glucose concentrations were excluded from the study. In contrast to previous research,17 which applied more comprehensive exclusion criteria based on an extended lipid profile, the present study excluded only individuals with conventional dyslipidemia. The study adhered to the principles of the Declaration of Helsinki, with approval from the Ethics Committee of Beijing Anzhen Hospital, Capital Medical University (KS2020005), and informed consent was waived by the ethics board.
Sample Collection
Following a standardized protocol, blood samples were collected. Participants fasted for at least 8 hours and remained seated for 15 minutes prior to sample collection. Blood was drawn from the elbow vein and left at room temperature for a minimum of 30 minutes before centrifugation at 2,980 × g for 10 minutes to obtain serum. The samples were stored at −80 °C and transported at −20 °C to the central laboratory of Beijing Anzhen Hospital for analysis.
GDF-15 Measurement
Serum GDF-15 levels were measured using the i3000 automatic chemiluminescence analyzer (Maccura Biotechnology, Chengdu, China) along with the manufacturer’s reagents (GDF-15 Chemiluminescent Immunoassay Kit) and quality control materials. At present, GDF-15 lacks certified reference materials and does not have an established reference measurement procedure. The metrological traceability available for GDF-15 measurements relies on the calibrator provided by the manufacturer. This assay demonstrated a strong correlation with a previously validated enzyme-linked immunosorbent assay (ELISA, R&D) method (y = 0.9542x + 57.741, r = 0.9418). It has a linear range of 100–30,000 ng/L (r = 0.9997) and offers high precision, with intra-assay coefficients of variation of 3.4% at 779 ng/L and 4.6% at 2147 ng/L, and inter-assay coefficients of 3.2% at 775 ng/L and 2.0% at 2155 ng/L. The limit of detection (LoD) of this assay is 25 ng/L.
Statistical Analysis
All statistical analyses were conducted with R software for macOS (Version 4.2.1, https://www.r-project.org/). Outliers were identified following the Clinical and Laboratory Standards Institute/International Federation of Clinical Chemistry (CLSI/IFCC) guideline using the Tukey’s test, and GDF-15 values exceeded the lower and upper boundaries were excluded. The Kolmogorov–Smirnov test was applied to assess the normality of GDF-15 distribution. For skewed data, a nonparametric approach was used to establish RIs.18 To visualize the data distribution and GDF-15 levels with age, a histogram and scattergram with a fitted curve were used. Percentile curves were plotted using the least mean square (LMS) method. To assess whether stratification by sex and age was necessary, a two-level nested analysis of variance (ANOVA) was employed following Ichihara’s approach, considering an standard deviation ratio (SDR) > 0.3 as indicative of notable subgroup differences.19 For further analysis of significant differences among age groups, the Tukey HSD post hoc test was used. Based on World Health Organization (WHO) age classification standards, individuals were classified into five age groups: 18–29, 30–44, 45–59, 60–74, and ≥ 75 years, ensuring a consistent 15-year range. Given that physiological markers can vary in minors, the initial age group was set to start at 18 years. A P-value < 0.05 was deemed significant for all tests.
Results
Out of the 10,618 apparently healthy individuals, 8,488 (79.9%) were eligible for the study. The Tukey’s test identified 724 outliers in GDF-15. A total of 7,764 participants were included in the data analysis (Figure 1). Median age of participants was 41 (25th-75th percentiles, 30–60) years, and 3423 (44.1%) participates were male. The participants were distributed as follows: 1,304 (16.8%) from Changsha, 1,438 (18.5%) from Shenyang, 1,460 (18.8%) from Ningxia, 1,480 (19.1%) from Chengdu, 1,315 (16.9%) from Hangzhou, and 767 (9.9%) from Nanning (Table 1).
 |
Table 1 Frequency Distributions of GDF-15 in 7764 Healthy Individuals by Gender, Age Groups and Six Regions of China |
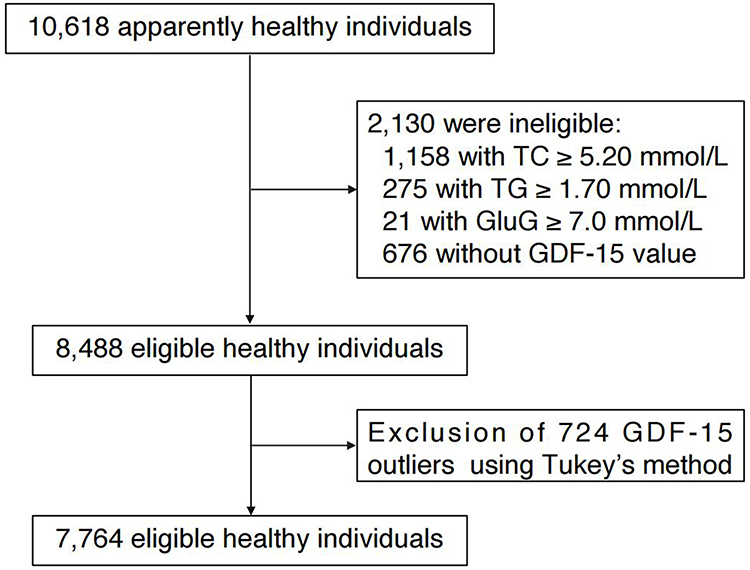 |
Figure 1 Recruitment schematic to establish reference intervals for GDF-15 in a Chinese population. Abbreviations: TG, triglycerides; TC, total cholesterol; Glu, glucose. |
The association between age and GDF-15 levels displayed a similar trend in both sexes: a gradual increase up to age 40, followed by a more pronounced rise thereafter, with GDF-15 levels consistently higher in males than in females (Figure 2). The percentile curves in Figure 3 further highlight this age-related trend, with the median GDF-15 levels showing an approximately three-fold increase from youngest to oldest participants. Additionally, the percentile distribution broadened significantly in older age groups, with the difference between the 2.5th and 97.5th percentiles nearly doubling with age.
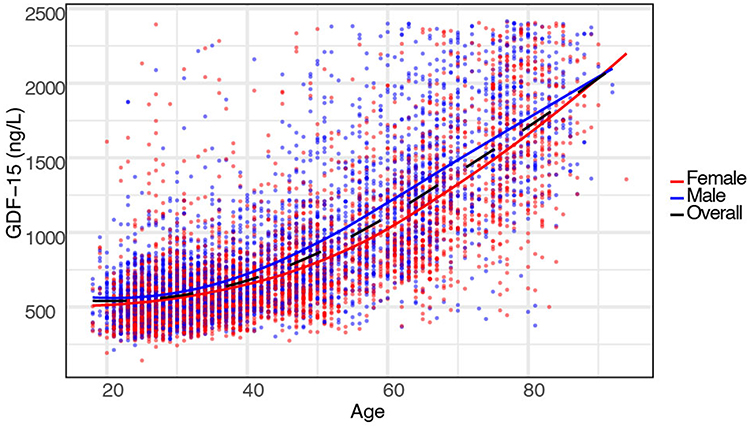 |
Figure 2 Scattergram with smoothed curves of GDF-15 across age. The blue spots and solid line represent individual data of males. The red spots and solid line represent individual data of females. The black solid line represent all participants. |
 |
Figure 3 Smoothed percentile curves showing serum GDF-15 concentration by age in apparently healthy participants. (A) All participants; (B) Male participates; (C) Female participates. |
The frequency distribution of GDF-15 in the reference population was shown to be non-Gaussian (Figure 4). The Kolmogorov–Smirnov test rejects normality (P <0.001). In the whole cohort, median GDF-15 was 696 (25th-75th percentiles: 522–1,096) ng/L. The two-level nested ANOVA analysis revealed an SDR of 0.83 for age intervals, while the SDR < 0.3 for sex. The Tukey HSD post hoc test revealed no significant difference in GDF-15 levels between males and females within the 18–29 age group (P = 0.373). However, in all other age groups, GDF-15 levels were significantly higher in males than in females (All P < 0.001) (Figure 5).
 |
Figure 4 GDF-15 reference population histogram. Green bars represent males; Blue bars represent females. |
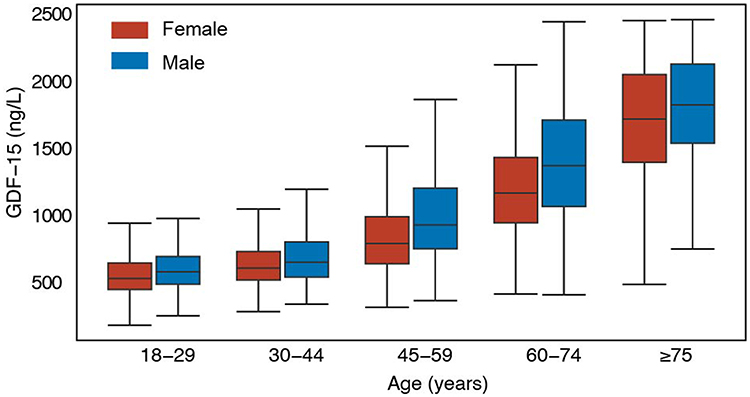 |
Figure 5 Box plot of GDF-15 levels across age and sex Groups. The box plot illustrates the distribution of GDF-15 levels across different age and sex groups. Each box represents the interquartile range (IQR), showing the 25th to 75th percentiles of GDF-15 levels. The horizontal line within each box marks the median value. Whiskers extend to the smallest and largest values within 1.5 times the IQR. Blue box: male; Red box: Female. |
The non-parametric method was used to establish RIs for GDF-15, with partitioning according age interval (18–29, 30–44, 45–59, 60–74, and ≥ 75 years) and sex (male and female). The defined RIs for each subgroup are summarized in Table 2 and Table 3.
 |
Table 2 Age-Specific and Sex-Specific Reference Intervals for GDF-15 (ng/L) in China |
 |
Table 3 Reference Intervals of GDF-15 with Different Gender and Age Interval |
Discussion
Our study established RIs for GDF-15, stratified by age and sex, using data from apparently healthy adults across six representative regions of China. Results indicate that GDF-15 levels increase with age and are generally higher in men than in women.
To our knowledge, this is the first study to explore GDF-15 concentrations in the apparently healthy Chinese population. Previous related studies primarily involved White participants of European ancestry, limiting the applicability of those findings to other racial and ethnic groups.13–15,20,21 Although approximately 40% of GDF-15 levels are genetically determined, our results indicate that GDF-15 levels in the Chinese population are comparable to those observed in European populations.16 A prior study involving 15,948 individuals from the general population reported age-specific upper reference limits for GDF-15. For males, the upper reference limits were 1,094, 1,400, 1,740, 2,194, 2,704 and 3,065 ng/L for the age groups < 30, 30–39, 40–49, 50–59, 60–69 and 70–79 years, respectively. For females, the corresponding limits were 1,738, 1,541, 1,595, 1,920, 2,326 and 3,066 ng/L.20 These results are slightly higher than those observed in our study, particularly among younger women and older adults. We speculate that this difference may be attributed to lax selection criteria, as well as the potential inclusion of pregnant participants.22
An earlier study assessing GDF-15 concentrations utilized an automated electrochemiluminescence immunoassay (Elecsys®) in a cohort of 739 apparently healthy individuals, reporting age-specific upper reference limits for GDF-15.13 The LoD for this assay was 400 ng/L, with more than 10% of participants presenting GDF-15 concentrations at or below this threshold. In contrast, we employed a different automated electrochemiluminescence immunoassay (Maccura) with a LoD of 25 ng/L, and no individual in our study had a GDF-15 concentration below this level. Given that GDF-15 is a predictor of future cardiovascular events in apparently healthy individuals, it is crucial to capture the full range of GDF-15 concentrations expected in a healthy population.21,23
Consistent with previous research, GDF-15 levels increased with age in our study. Some researchers have suggested that individuals with GDF15 concentrations at the higher end of the range may have asymptomatic cardiovascular disease. Indeed, elevated GDF-15 concentrations in community-dwelling individuals are associated with subclinical vascular and cardiac pathologies.24 However, we believe other factors may also explain this finding, as the correlation between GDF-15 concentration and age is also observed in carefully characterized cohorts of apparently healthy individuals.10,15 Aging is frequently associated with a chronic, low-grade inflammatory state—referred to as inflammaging—which has been shown to induce the expression of GDF-15.25 Unlike previous studies, although the two-level nested ANOVA suggested that sex-based stratification was unnecessary, post hoc analysis showed no sex difference in the 18–29 age group but significant differences in older groups. Therefore, we applied sex stratification within the adult and elderly age groups. In vitro, estradiol significantly decreased GDF-15 expression by activating estrogen receptors, which subsequently increased DNA methyltransferase 1 (DNMT1) expression.26,27 This upregulation of DNMT1 enhanced methylation in the TP53 promoter, leading to the downregulation of GDF-15.2 Additionally, circulating levels of GDF-15 were lower in menopausal women treated with estrogen compared to those given a placebo.28 These results support our finding that GDF-15 levels in women increase rapidly during menopause.
The strength of our study lies in our participant cohort. First, we included 7,764 healthy Chinese adults from six representative cities. Second, the large sample size and broad age range enable stratified analysis of the reference ranges. Third, our stringent inclusion criteria ensured data quality: in addition to self-reported medical history, all participants underwent testing for blood glucose and lipid levels to confirm health status, as reflected by the narrow 95% CI of our RIs. Furthermore, GDF-15 concentrations were measured using the same equipment across all samples, ensuring consistency in data collection.
There are some limitations in our study. GDF-15 was measured in frozen serum samples after a second thaw; however, previous data suggests that GDF-15 is stable through up to four freeze-thaw cycles.13 Additionally, we considered only gender and age as influencing factors, without collecting information on other potential confounders such as BMI, dietary habits, and socioeconomic status, which may also impact GDF-15 levels. Previous research has suggested that while BMI may influence GDF-15 levels in cohort with disease, this relationship may be less pronounced in generally healthy populations.29 Besides, we partly attributed sex- and age-related reference values in women to effects of estrogen, but no supporting data about GDF-15 values for pre- and post-menopausal women have been provided. Finally, despite applying selection criteria, the authors identified 8.5% outliers, which is relatively high. Further analysis of the age distribution of these outliers revealed that the median age was 79 years. Notably, our study included approximately 350 participants aged 80 and above, and China has the largest population of individuals aged 80 and above. In contrast, previous studies often included smaller samples of elderly individuals or younger populations, which may explain some of the discrepancies.
Conclusion
In conclusion, our study is the first to establish RIs for serum GDF-15 based on a large, multicenter sample of apparently healthy individuals from six representative cities across China. We found that serum GDF-15 levels increase progressively with age and are generally higher in males than in females. Accordingly, we developed age- and sex-specific RIs of GDF-15 to reflect these physiological variations in the Chinese population. Furthermore, the similar distribution patterns of GDF-15 observed across different ethnic populations support the applicability of the proposed clinical decision thresholds of 1200 and 1800 ng/L within the Chinese population.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study adhered to the principles of the Declaration of Helsinki, with approval from the Ethics Committee of Beijing Anzhen Hospital, Capital Medical University (KS2020005), and informed consent was waived by the ethics board.
Consent for Publication
This study was approved by the Ethics Committee of Beijing Anzhen Hospital, Capital Medical University, and written informed consent for publication was waived due to the retrospective nature of the study. The data was anonymized, and no personally identifiable information is included in the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Key Research and Development Program (2022YFC2009600)(2022YFC2009602).
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
1. Wischhusen J, Melero I, Fridman WH. Growth/differentiation factor-15 (GDF-15): from biomarker to novel targetable immune checkpoint. Front Immunol. 2020;11:951. doi:10.3389/fimmu.2020.00951
2. Wollert KC, Kempf T, Wallentin L. Growth differentiation factor 15 as a biomarker in cardiovascular disease. Clin Chem. 2017;63(1):140–151. doi:10.1373/clinchem.2016.255174
3. Galliera E, Lombardi G, Marazzi MG, et al. Acute exercise in elite rugby players increases the circulating level of the cardiovascular biomarker GDF-15. Scand J Clin Lab Invest. 2014;74(6):492–499. doi:10.3109/00365513.2014.905697
4. Adela R, Banerjee SK. GDF-15 as a target and biomarker for diabetes and cardiovascular diseases: a translational prospective. J Diabetes Res. 2015;2015:490842. doi:10.1155/2015/490842
5. Wollert KC, Kempf T, Peter T, et al. Prognostic value of growth-differentiation factor-15 in patients with non-ST-elevation acute coronary syndrome. Circulation. 2007;115(8):962–971. doi:10.1161/CIRCULATIONAHA.106.650846
6. Widera C, Pencina MJ, Bobadilla M, et al. Incremental prognostic value of biomarkers beyond the GRACE (Global Registry of Acute Coronary Events) score and high-sensitivity cardiac troponin T in non-ST-elevation acute coronary syndrome. Clin Chem. 2013;59(10):1497–1505. doi:10.1373/clinchem.2013.206185
7. Haller PM, Jarolim P, Palazzolo MG, et al. Heart Failure Risk assessment using biomarkers in patients with atrial fibrillation: analysis from COMBINE-AF. J Am Coll Cardiol. 2024;84(16):1528–1540. doi:10.1016/j.jacc.2024.07.023
8. Bouabdallaoui N, Claggett B, Zile MR, et al. Growth differentiation factor-15 is not modified by sacubitril/valsartan and is an independent marker of risk in patients with heart failure and reduced ejection fraction: the PARADIGM-HF trial. Eur J Heart Fail. 2018;20(12):1701–1709. doi:10.1002/ejhf.1301
9. Wollert KC, Kempf T, Lagerqvist B, et al. Growth differentiation factor 15 for risk stratification and selection of an invasive treatment strategy in non ST-elevation acute coronary syndrome. Circulation. 2007;116(14):1540–1548. doi:10.1161/CIRCULATIONAHA.107.697714
10. Kempf T, Horn-Wichmann R, Brabant G, et al. Circulating concentrations of growth-differentiation factor 15 in apparently healthy elderly individuals and patients with chronic heart failure as assessed by a new immunoradiometric sandwich assay. Clin Chem. 2007;53(2):284–291. doi:10.1373/clinchem.2006.076828
11. Xanthakis V, Enserro DM, Murabito JM, et al. Ideal cardiovascular health: associations with biomarkers and subclinical disease and impact on incidence of cardiovascular disease in the Framingham Offspring Study. Circulation. 2014;130(19):1676–1683. doi:10.1161/CIRCULATIONAHA.114.009273
12. Daniels LB, Clopton P, Laughlin GA, Maisel AS, Barrett-Connor E. Growth-differentiation factor-15 is a robust, independent predictor of 11-year mortality risk in community-dwelling older adults: the Rancho Bernardo Study. Circulation. 2011;123(19):2101–2110. doi:10.1161/CIRCULATIONAHA.110.979740
13. Wollert KC, Kempf T, Giannitsis E, et al. An automated assay for growth differentiation factor 15. J Appl Lab Med. 2017;1(5):510–521. doi:10.1373/jalm.2016.022376
14. Doerstling S, Hedberg P, Ohrvik J, Leppert J, Henriksen E. Growth differentiation factor 15 in a community-based sample: age-dependent reference limits and prognostic impact. Ups J Med Sci. 2018;123(2):86–93. doi:10.1080/03009734.2018.1460427
15. Krintus M, Braga F, Kozinski M, et al. A study of biological and lifestyle factors, including within-subject variation, affecting concentrations of growth differentiation factor 15 in serum. Clin Chem Lab Med. 2019;57(7):1035–1043. doi:10.1515/cclm-2018-0908
16. Ho JE, Mahajan A, Chen MH, et al. Clinical and genetic correlates of growth differentiation factor 15 in the community. Clin Chem. 2012;58(11):1582–1591. doi:10.1373/clinchem.2012.190322
17. Fan X, Wang X, Zhao H, et al. Reference intervals for cardiometabolic risk factors in China: a national multicenter cross-sectional study on an adult population sample. Cardiovasc Diagn Ther. 2024;14(1):174–192. doi:10.21037/cdt-23-369
18. EP28-A3C C. Defining, establishing, and verifying reference intervals in the clinical laboratory. Available from: https://clsi.org/standards/.
19. Ichihara K. Statistical considerations for harmonization of the global multicenter study on reference values. Clin Chim Acta. 2014;432:108–118. doi:10.1016/j.cca.2014.01.025
20. Welsh P, Kimenai DM, Marioni RE, et al. Reference ranges for GDF-15, and risk factors associated with GDF-15, in a large general population cohort. Clin Chem Lab Med. 2022;60(11):1820–1829. doi:10.1515/cclm-2022-0135
21. Hamon SM, Griffin TP, Islam MN, Wall D, Griffin MD, O’Shea PM. Defining reference intervals for a serum growth differentiation factor-15 (GDF-15) assay in a Caucasian population and its potential utility in diabetic kidney disease (DKD). Clin Chem Lab Med. 2019;57(4):510–520. doi:10.1515/cclm-2018-0534
22. Moore AG, Brown DA, Fairlie WD, et al. The transforming growth factor-ss superfamily cytokine macrophage inhibitory cytokine-1 is present in high concentrations in the serum of pregnant women. J Clin Endocrinol Metab. 2000;85(12):4781–4788. doi:10.1210/jcem.85.12.7007
23. Brown DA, Breit SN, Buring J, et al. Concentration in plasma of macrophage inhibitory cytokine-1 and risk of cardiovascular events in women: a nested case-control study. Lancet. 2002;359(9324):2159–2163. doi:10.1016/S0140-6736(02)09093-1
24. Andersson C, Enserro D, Sullivan L, et al. Relations of circulating GDF-15, soluble ST2, and troponin-I concentrations with vascular function in the community: the Framingham Heart Study. Atherosclerosis. 2016;248:245–251. doi:10.1016/j.atherosclerosis.2016.02.013
25. Pence BD. Growth differentiation factor-15 in immunity and aging. Front Aging. 2022;3:837575. doi:10.3389/fragi.2022.837575
26. Liu H, Dai W, Cui Y, Lyu Y, Li Y. Potential associations of circulating growth differentiation factor-15 with sex hormones in male patients with coronary artery disease. Biomed Pharmacother. 2019;114:108792. doi:10.1016/j.biopha.2019.108792
27. Chen YC, Young MJ, Chang HP, et al. Estradiol-mediated inhibition of DNMT1 decreases p53 expression to induce M2-macrophage polarization in lung cancer progression. Oncogenesis. 2022;11(1):25. doi:10.1038/s41389-022-00397-4
28. Faubion L, White TA, Peterson BJ, et al. Effect of menopausal hormone therapy on proteins associated with senescence and inflammation. Physiol Rep. 2020;8(16):e14535. doi:10.14814/phy2.14535
29. Wiklund FE, Bennet AM, Magnusson PK, et al. Macrophage inhibitory cytokine-1 (MIC-1/GDF15): a new marker of all-cause mortality. Aging Cell. 2010;9(6):1057–1064. doi:10.1111/j.1474-9726.2010.00629.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.