")
Back to Journals » Journal of Inflammation Research » Volume 17
A Nomogram-Based Prognostic Model for Lymphoma Patients Initially Presenting with Fever of Unknown Origin
Authors Shen L, Young W, Wu M, Xie Y
Received 26 August 2024
Accepted for publication 4 November 2024
Published 7 November 2024 Volume 2024:17 Pages 8445—8469
DOI https://doi.org/10.2147/JIR.S493158
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Adam Bachstetter
Lin Shen,* Wenjing Young,* Min Wu, Yanhui Xie
Department of Hematology, Huadong Hospital Affiliated with Fudan University, Shanghai, 200040, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Min Wu; Yanhui Xie, Email [email protected]; [email protected]
Background: Patients with lymphoma who present with fever of unknown origin (FUO) as an initial symptom lack specific clinical feature analysis, prognostic factor analysis, and existing prognostic models. We aim to create a prognostic model for these patients to improve prognosis and risk assessment.
Methods: A total of 555 lymphoma patients with FUO as initial symptom studied at Huadong Hospital affiliated with Fudan University. Univariable Cox regression identified outcome predictors, analyzed by LASSO Cox. Multifactorial Cox on screened coefficients determined independent prognostic factors and nomogram model. The validity of the nomogram was evaluated through bootstrap sampling, calibration curves for model calibration, time-dependent ROC curve analysis for discrimination assessment, and decision curve analysis for evaluating clinical usefulness. Further validation involved utilizing Kaplan-Meier curves and Log rank tests. Lastly, X-tile software determined the optimal cutoff point for the nomogram score by comparing it with the traditional International Prognostic Index (IPI) scoring system.
Results: The entire cohort was divided into a training cohort (n=388) and a validation cohort (n=167). These risk factors (cell pathologic type, performance status score, Ann Arbor staging, thrombocytopenia, and raised direct bilirubin) were used to construct a web-based dynamic survival rate calculator for lymphoma patients initially presenting with FUO. The lymphoma-specific nomogram demonstrated good consistency and efficacy in predicting the model’s risk stratification. Compared to the IPI scoring system, the nomogram model had higher AUC values for different clinical endpoints. The new nomogram prognostic model showed better differentiation of risk groups compared to traditional IPI scoring.
Conclusion: Our study developed and validated a prognostic nomogram for lymphoma patients initially presenting with FUO, demonstrating robust predictive efficacy and risk stratification ability. Furthermore, we have successfully implemented this model into a web-based dynamic survival rate calculator.
Keywords: fever, lymphoma, prognosis, IPI, nomogram
Introduction
Lymphoma is a highly heterogeneous group of malignant tumors originating from the lymphatic hematopoietic system, primarily classified into Hodgkin’s lymphoma (HL) and non-Hodgkin’s lymphoma (NHL).1 In China, lymphoma is among the common malignancies, with an incidence of 0.46% for HL and 4.29% for NHL per 100,000 population.2 Most lymphoma patients, especially those with NHL, present with persistent, painless lymphadenopathy prior to diagnosis, and some exhibit symptoms like night sweats, persistent fever of unknown origin (FUO), and unexplained weight loss.3 Fever is a common clinical symptom, and among causes of FUO in oncology, lymphoma is one of the most frequent.4 The regulation of fevers and pathogenesis of lymphomas is centrally influenced by various factors, including cytokines such as interleukin-1, interleukin-6, tumor necrosis factor, and interferons. Furthermore, the development of T-cell follicular helper-type Peripheral T-cell lymphomas (TCLs) relies significantly on granulocyte-driven inflammation, cytokine-induced interactions between granulocytes and CD4+ TCLs, as well as an intact JAK/STAT signaling pathway.4 Patients initially presenting with FUO often exhibit complex clinical manifestations, making differentiation difficult. While C-reactive protein (CRP), procaicitonin (PCT), and erythrocyte sedimentation rate (ESR) are commonly used as markers of infection, they are not specific for distinguishing between infectious and neoplastic fevers. The close relationship between FUO and lymphoma further complicates diagnosis and treatment.
The diagnosis of lymphoma relies on tissue biopsy, and positron emission tomography / computed tomography (PET/CT) scans, which measure the uptake of deoxyglucose, serve as a valuable indicator of the biological activity associated with this disease.5 Meta-analyses revealed that PET/CT exhibits high sensitivity but low specificity in diagnosing FUO.6,7 However, due to its limited specificity for malignancies, distinguishing lymphomas using this approach in cases of FUO remains challenging. HL and has since been recognized as having wide applicability to NHL. Additionally, the research focuses on the International Prognostic Index (IPI), which was derived from this staging system.8,9 While traditional scoring systems include symptoms like prolonged fever, weight loss exceeding 10% of body weight over a 6-month period, and drenching night sweats, they fall short in capturing the comprehensive analysis of lymphoma cases where fever is the presenting symptom. Furthermore, these systems do not address the exploration of contributory factors, the development of prognostic models, nor the subsequent validations that are critical to understanding and managing these cases effectively.
In previous article, we explored the clinical characteristics and prognostic factors of lymphoma patients presenting with fever of unknown origin. However, with the widespread application of nomograms in lymphoma research and clinical practice, this has brought about a challenge of convenience for clinical researchers.10,11 In the present study, the development of survival rate calculators was based on the construction of nomogram models, which, after manually adjusting parameters, automatically plot survival curves and calculate survival rates for patients, greatly improving the models’ applicability and ease of use.12 Hence, the objective of this study is to methodically compile clinical data from lymphoma patients who initially present with (FUO). We aim to delve into their unique clinical features and corresponding prognoses, as well as to investigate innovative clinical and molecular prognostic models for these patients within the Chinese context. The insights garnered from this research will furnish clinicians with invaluable references to enhance their precision in evaluating patient risk and forecasting outcomes.
Materials and Methods
Study Population and Clinical Data Collection
Between January 2013 and December 2021, 555 newly diagnosed lymphoma patients presenting with FUO as the initial symptom were admitted to the Department of Hematology at Huadong Hospital. A confirmed pathological diagnosis was required for all cases, either from the pathology department of our hospital or with a definitive pathology report provided by an external institution. Fever was defined as a body temperature of ≥37.3°C. Lymphoma staging was determined using the Ann Arbor system,13 and pathological classification was conducted according to the World Health Organization (WHO) classification of hematopoietic and lymphoid tissue tumors.14 Performance status was scored based on the Eastern Cooperative Oncology Group (ECOG) performance status scale.15
Clinically Relevant Parameters
Data were collected via review of the electronic medical record system at Huadong Hospital, supplemented by telephone follow-ups. Information collected included age, gender, clinical symptoms, location of diagnostic biopsy, pathological results, extranodal involvement sites, IPI score,8 and baseline laboratory tests at admission encompassing complete blood counts, liver and kidney function tests, lactate dehydrogenase levels, erythrocyte sedimentation rate, blood lipids, C-reactive protein, and ferritin.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: 1) explicit pathological diagnosis of lymphoma; 2) initial symptom of fever; and 3) complete clinical and pathological information for all patients involved. The exclusion criteria were: 1) clear clinical or substantial evidence of infection; 2) presence of immunodeficiency disorders; 3) incomplete data collection. Out of 563 potential participants, 4 patients were excluded due to HIV infection, 2 due to an immunodeficiency diagnosis, and 2 due to loss to follow-up, resulting in incomplete data. A total of 555 patients (388 in the training set group and 167 in the validation set group) were included in the research cohort.
Treatment Regimens
Most patients in our study received first-line therapy with cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) or CHOP-like chemotherapy. Relapsed or refractory lymphoma patients were treated with salvage regimens such as ifosfamide, carboplatin, and etoposide (ICE), dexamethasone, high-dose cytarabine, and oxaliplatin (GDP), and other guideline-recommended second-line therapies. Some high-risk patients were treated with autologous hematopoietic stem cell transplantation or maintenance therapy with lenalidomide or thalidomide.
Clinical Endpoints
The clinical endpoints included complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). The primary outcome was overall survival (OS), and the secondary endpoint was progression-free survival (PFS). OS was defined as the interval from diagnosis to death from any cause or to the last follow-up date. PFS was defined as the interval from diagnosis to disease progression or death from any cause. The last follow-up date was December 31, 2021.
Construction of Nomograms
Random group allocation for all patients was conducted using the “sample” function in the R programming language, dividing the 555 patients with FUO-associated lymphoma into modeling (training set) and validation set groups in a 7:3 ratio, with 388 (70%) and 167 (30%) patients, respectively. For the identification of prognostic factors related to OS and PFS in fever-associated lymphoma patients, univariate Cox regression analysis (p<0.05) was performed as a screening, followed by the least absolute shrinkage and selection operator (LASSO)-Cox regression model using “typ.measure” set to “deviance” and 10-fold cross-validation to determine the optimal penalization coefficient. Variables identified were further analyzed using multivariate Cox regression with a stepwise method to explore independent risk factors (p<0.05). Models were visualized using R Studio for plotting nomograms.
Evaluation of Nomogram Discrimination Efficacy and Clinical Utility
The discriminative ability of the nomograms was assessed using the Harrell’s concordance index (C-index) and the area under the receiver operating characteristic (ROC) curve (AUC). The nomogram models were evaluated for calibration with bootstrap sampling and calibration curve plotting. The C-index is the measure of prediction accuracy, with values closer to 1 indicating better predictive ability and values around 0.5 indicating no discriminative power. Calibration curves were used to verify model calibration. Decision Curve Analysis (DCA) quantified the net benefit within a range of threshold probabilities to assess clinical usefulness. The validation of the models, including both internal and external validations, was performed in terms of discrimination and calibration. For internal validation within the modeling cohort, the C-index for survival, ROC curve, and calibration curve were calculated to validate discrimination and calibration, respectively. In the validation cohort, the preconstructed nomogram was tested by calculating the C-index, generating ROC curves, and drawing calibration curves.
Survival Analysis
PFS and OS were used as clinical endpoints in the validation group. Survival cut-off points in the nomogram model were calculated using the “surv_cutpoint” function from the “survminer” package in R, with patients stratified into low and high-risk groups accordingly. Kaplan-Meier survival curves were generated and compared using the Log rank test to validate the nomogram model. The optimal risk group stratifications and cutoff points were further calculated using X-tile, followed by Kaplan-Meier survival analysis and log-rank comparison between risk groups.
Statistical Analysis
This analysis was performed using R software (version 4.2.2) with the “glmnet” package for LASSO regression analysis, “rms” package for nomogram construction, “riskRegression”, “ggprism”, and “ggplot2” packages for plotting ROC curves, “ggDCA” for Decision Curve Analysis, and “survminer” for survival analysis. All tests conducted were two-sided, and a p-value of less than 0.05 was considered statistically significant.
Results
Baseline Characteristics of the Enrolled Cohort
A total of 555 patients with lymphoma, who initially presented with FUO, was divided into a training set comprising 388 patients and a validation set consisting of 167 patients. The respective clinicopathological characteristics of the cohorts are presented in Table 1. A significant proportion of the patients (305 individuals, accounting for 54.95%) were aged ≤60 years, with a majority being male (336 individuals, accounting for 60.4%). The majority of the patients (390 out of 553, accounting for 70.45%) showed B-cell type pathology. At presentation, splenic involvement was observed in 209 patients (37.66%), hepatic involvement in 67 patients (12.07%), and bone marrow involvement in 155 patients (27.93%). During the course of the disease, hemophagocytic syndrome manifested itself in a total of 101 patients (18.20%). Coinfection with HBV was identified in 47.21% of patients (n=262), EBV infection in 26.31% (n=146), leukopenia in 25.05% (n=139), neutropenia in 7.39% (n=41), anemia in 53.87% (n=299), thrombocytopenia in 20.90% (n=116), and hypercholesterolemia in 33.51% (n=186). Elevated alanine aminotransferase (ALT) was observed in 16.94% of cases (n=94), while aspartate aminotransferase (AST) was increased in 19.10% (n=106). A total of 20.36% of patients (n=113) demonstrated raised total bilirubin levels, with direct hyperbilirubinemia occurring in 24.86% (n=138). Alkaline phosphatase levels were elevated in 16.40% of the cohort (n=91). Hypoalbuminemia was noted in 35.68% of patients (n=198), elevated LDH in 54.95% (n=305), increased β2-microglobulin (β2MG) in 38.92% (n=216), heightened CRP at presentation in 40.54% (n=225), accelerated erythrocyte sedimentation rate (ESR) in 31.71% (n=176), and elevated ferritin levels in 27.03% (n=150). Upon enrollment, 9.55% of the patients (n=53) exhibited an ECOG performance status score of 0, whereas 40.00% (n=222) had a score of 1. Regarding the stage of disease at diagnosis, 20.35% of patients (n=113) presented with Ann Arbor stages I or II. The distribution of the IPI scores revealed that the most prevalent score was 3, occurring in 28.65% of patients (n=159), followed by scores of 2 in 21.80% (n=121), 4 in 19.82% (n=110), 1 in 17.84% (n=99), 5 in 6.49% (n=36), and 0 in 5.41% (n=30).
 |
Table 1 Clinicopathological Characteristics of the Training and Validation Cohorts |
Analysis of Prognostic Factors Using Univariate Cox Regression
The clinical data of the collected patients, including clinical variables known to potentially impact lymphoma prognosis, were subjected to univariate Cox regression analysis. These variables encompassed both traditional prognostic factors outlined by the IPI and NCCN-IPI (age, Ann Arbor stage, lactate dehydrogenase level, patient performance status, and sites of extranodal involvement) and additional factors cited in contemporary research such as gender, pathological type, EBV load, concurrent HBV infection, and various hematologic and biochemical markers. The univariate Cox regression analysis revealed that pathological type, organ involvement (liver, spleen, bone marrow), hemophagocytic syndrome, baseline performance status, IPI score, EBV load, and abnormalities in hematological parameters (white blood cell, hemoglobin, platelet, and neutrophil counts) and biochemical markers (liver enzymes, alkaline phosphatase, bilirubin, cholesterol, albumin, lactate dehydrogenase, beta-2 microglobulin, CRP, and ferritin) were significantly correlated with PFS (Table 2). Similarly, variables including gender, pathological type, organ involvement at diagnosis, hemophagocytic syndrome, performance status, Ann Arbor stage, IPI score, EBV infection, hematologic parameters (neutrophil counts, hemoglobin, and platelet levels), and biochemical markers (aspartate and alanine aminotransferase, cholesterol, bilirubin, alkaline phosphatase, albumin, lactate dehydrogenase, beta-2 microglobulin, CRP, and ferritin) were significantly associated with OS (Table 3).
 |
Table 2 Univariate Cox Regression Analysis of PFS in Lymphoma Patients with FUO |
 |
Table 3 Univariate Cox Regression Analysis of OS in Lymphoma Patients with FUO |
LASSO Regression and Multivariate Cox Regression Analyses
Within the training set of lymphoma patients initially presenting with FUO, LASSO Cox regression analysis identified nine risk factors significantly associated with PFS, as shown in Figure 1A. These factors encompassed the cell pathological type at diagnosis, ECOG performance status score, Ann Arbor staging, concurrent EBV infection, granulocytopenia (absolute neutrophil count < 0.5 × 10^9/L), anemia (hemoglobin < 120 g/L for males and < 110 g/L for females), thrombocytopenia (platelet count < 100 × 10^9/L), elevated direct bilirubin (DBIL > 6.8 µmol/L), and increased lactate dehydrogenase (LDH > 245 U/L), and ferritin levels (> 500 ng/mL). Using 10-fold cross-validation, optimal parameters were identified, selecting variables based on the lambda value yielding the minimum deviance (Figure 1B). Multivariable Cox regression with a stepwise selection confirmed cell pathological type, ECOG performance status, Ann Arbor staging, thrombocytopenia, and elevated DBIL as independent predictors of PFS in FUO lymphoma cases (Figure 2A).
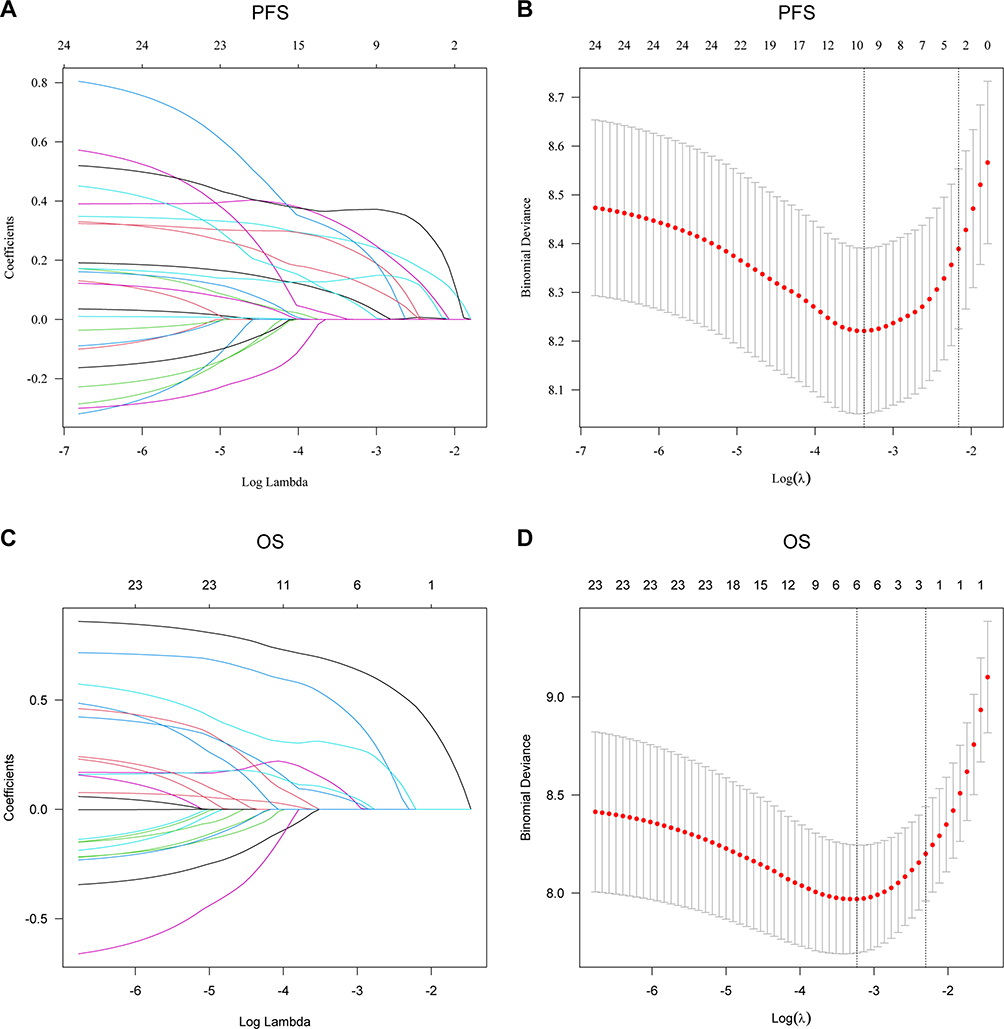 |
Figure 1 Risk factor screening and cross-validation using the LASSO regression model. (A) A LASSO regression model was employed in the training set to select risk factors for PFS. (B) Cross-validation of LASSO for PFS. (C) A LASSO regression model was employed in the training set to select risk factors for OS. (D) Cross-validation of LASSO for OS. LASSO, least absolute shrinkage and selection operator. |
 |
Figure 2 Multivariate cox regression Analysis model. (A) Multivariate cox regression Analysis model for PFS. (B) Multivariate cox regression Analysis model for OS. * means P< 0.05; ** means P< 0.01; *** means P< 0.001. |
For OS analyses in FUO lymphoma patients, LASSO Cox regression revealed six significant factors, including ECOG performance status score at diagnosis, concurrent EBV infection, granulocytopenia, elevated alanine transaminase (ALT > 40 U/L), elevated aspartate transaminase (AST > 40 U/L), and heightened ferritin levels (> 500 ng/mL) (Figure 1C). Selection of these variables was again based on the lambda associated with the lowest deviance (Figure 1D). Further stepwise multivariable Cox regression analysis identified ECOG performance status score, simultaneous EBV infection at diagnosis, and ferritin elevation as independent determinants of OS in patients with FUO lymphoma (Figure 2B).
Establishment of the Nomogram Prediction Model
Multivariate analysis revealed that several factors had statistically significant prognostic implications for PFS and OS, including cellular pathology classification, performance status (ECOG), Ann Arbor staging, thrombocytopenia (platelet count (PLT) < 100 × 10^9/L), elevated direct bilirubin (DB > 6.8 μmol/L), concurrent EBV infection at diagnosis, and raised ferritin levels (>500 ng/mL). These factors were integrated into predictive nomograms for PFS (Figure 3A) and OS (Figure 3B), plotted using R Studio. The nomograms assign points for each prognostic indicator based on its regression coefficient in the multivariate model, culminating in a total score that correlates with individual survival probabilities. For illustrative purposes, a patient with Diffuse Large B-Cell Lymphoma, an ECOG score of 1, a non-stage IV Ann Arbor classification, a PLT count of 90 × 10^9/L, and a DB level of 7.6 μmol/L would accrue 28 points for cellular pathology, 16 for ECOG score, 0 for Ann Arbor stage, 22 for PLT, and 22 for DB, resulting in an aggregate score of 88. The corresponding PFS probabilities for this cumulative score would be approximately 84%, 67%, and 58% at 1, 3, and 5 years, respectively. If this patient also presents with concurrent EBV infection and a ferritin level exceeding 500 ng/mL, the additional 20 points for each would revise the total score to 128. In this scenario, the nomogram predicts approximately 86%, 80%, and 75% probabilities of 1-year, 3-year, and 5-year OS respectively.
 |
Figure 3 Nomogram-based prediction of 1-year, 3-year, and 5-year survival in patients with lymphoma initially presenting with FUO. (A) Nomogram-based prediction of 1-year, 3-year, and 5-year PFS. (B) Nomogram-based prediction of 1-year, 3-year, and 5-year OS. FUO, fever of unknown origin. |
Validation of the Nomogram Prediction Model
The discriminative ability of the prediction model was evaluated using ROC curves for PFS and OS at 1, 3, and 5 years in both training and validation cohorts. The AUC for the training cohort were 0.861, 0.861, and 0.732 for 1-, 3-, and 5-year PFS, respectively (Figure 4A), and for the validation cohort were 0.777, 0.747, and 0.654 (Figure 4B). For OS in the training cohort, the AUC values were 0.831, 0.853, and 0.842 at 1, 3, and 5 years, respectively (Figure 4C), whereas in the validation cohort, the AUC values were 0.878, 0.898, and 0.902 (Figure 4D). These data suggest that the prediction model demonstrates good discriminative and predictive capabilities.
 |
Figure 4 ROC curves for 1-year, 3-year, and 5-year survival of patients with lymphoma initially presenting with FUO. (A) ROC curves were plotted for the training set to assess 1-year, 3-year, and 5-year PFS. (B) ROC curves were plotted for the validation set to assess 1-year, 3-year, and 5-year PFS. (C) ROC curves were plotted for the training set to assess 1-year, 3-year, and 5-year OS. (D) ROC curves were plotted for the validation set to assess 1-year, 3-year, and 5-year OS. ROC, receiver operating characteristic curve; AUC, area under curve. |
Calibration curves for 1- and 3-year PFS showed excellent agreement with the 45-degree line in both the training (Figure 5A) and validation (Figure 5B) cohorts. Likewise, remarkable consistency was noted for the 1-, 3-, and 5-year OS calibration curves in both the training and validation cohorts (Figure 5C and D). These results confirm that the predictive model is well-calibrated with robust predictive performance. The clinical utility of the prediction model was assessed by DCA, which evaluates the net benefits across various threshold probabilities. For PFS predictions at 1-year, significant net benefits were observed within the threshold ranges of 8–95% in the training cohort (Figure 6A) and 2–90% in the validation cohort (Figure 6B). For the 3-year PFS, the respective threshold ranges were 10–80% and 2–99%, while for the 5-year PFS, they were 25–99% and 20–99%. For OS predictions at 1-year, considerable net benefits were noted within thresholds of 2–80% for the training cohort (Figure 6C) and 5–80% for the validation cohort (Figure 6D). The thresholds for 3-year OS were 5–95% and 2–99%, and for 5-year OS, they were 8–99% and 5–99%. The results illustrate that the model is clinically useful.
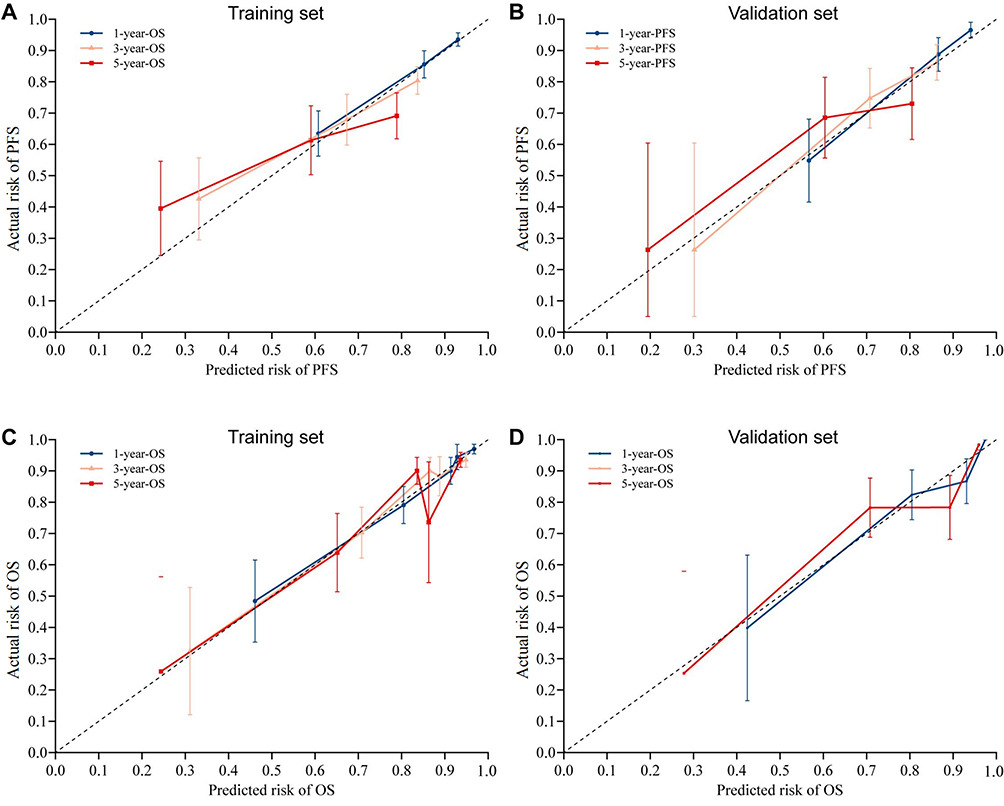 |
Figure 5 The calibration curves were generated for the 1-year, 3-year, and 5-year survival models. The PFS combination curve was plotted using both the training set (A) and the verification set (B). The OS combination curve was constructed using the training set (C) and the validation set (D). |
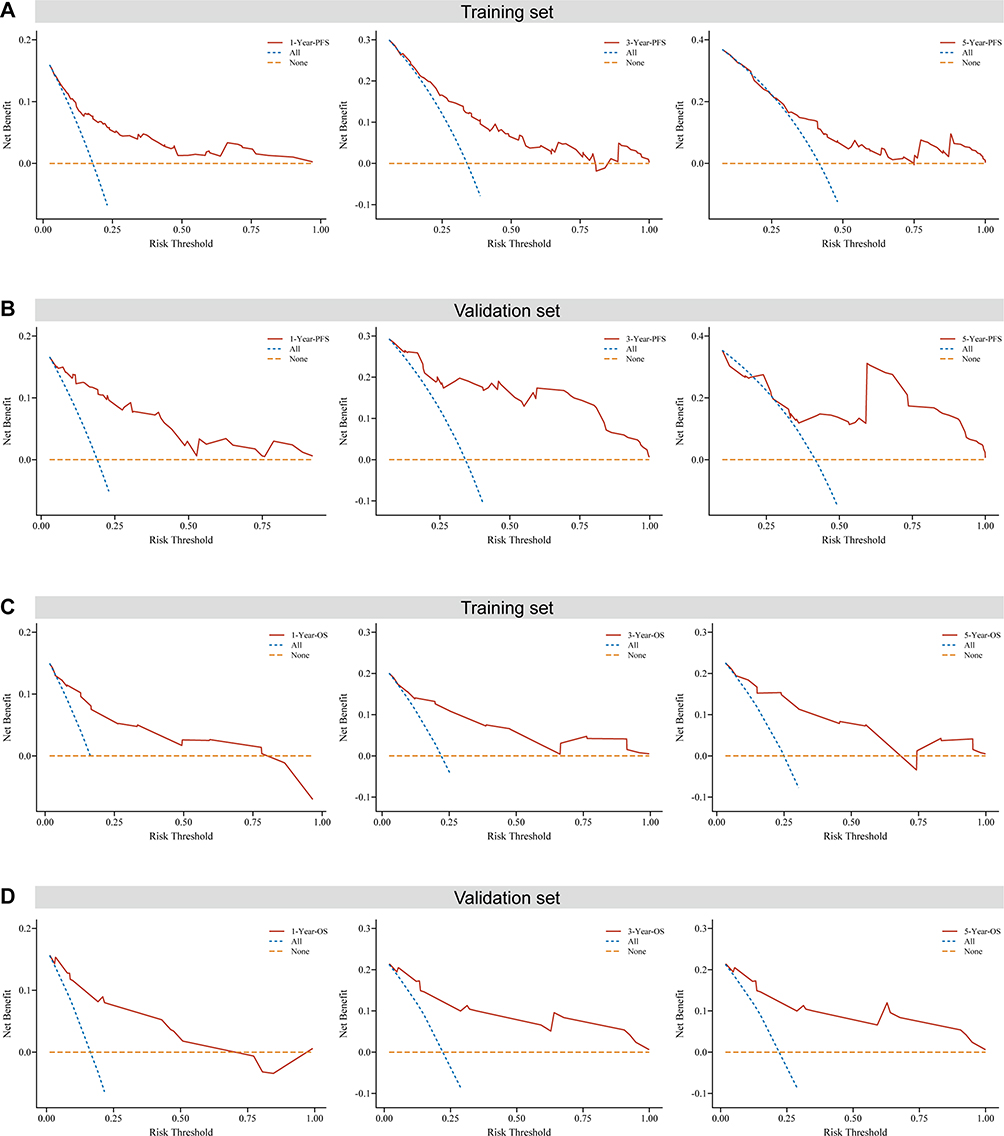 |
Figure 6 DCA for predicting 1-year, 3-year, and 5-year survival in lymphoma patients initially presenting with FUO: (A) Training set and (B) Validation set for the prediction model of PFS, and (C) Training set and (D) Validation set for the predictive models of 1-, 3-, and 5-year OS. DCA, Decision curve analysis. |
Survival Curves Stratified by Risk Levels Using the Kaplan-Meier Method
Kaplan-Meier survival curves were generated in R studio to stratify patients into two risk categories (high-risk vs low-risk) based on cutoff values for the PFS and OS. For PFS, the median duration in the entire cohort was 6.583 months for the low-risk group and significantly reduced to 0.583 months for the high-risk group (Figure 7A). The one-year PFS rates were 88.3% for low-risk and 41.3% for high-risk patients. Moreover, the three-year PFS rates were 72.9% for low-risk and 20.8% for high-risk, and the five-year rates were 64.9% compared to 13.8%. In the training set, median PFS was 5.917 months for the low-risk group and 0.583 months for the high-risk group (Figure 7B). The one, three, and five-year PFS rates were 88.3% vs 42.0%, 73.0% vs 20.8%, and 65.3% vs 10.4% for low-risk and high-risk groups, respectively. Moreover, validation set results demonstrated a median PFS of 8.0 months for the low-risk group and 0.5 months for the high-risk group (Figure 7C). One-year PFS rates were 88.4% in low-risk and 39.9% in high-risk patients, with three and five-year rates at 73.2% vs 24.0%, and 64.4% vs 24.0%, respectively. In each group, low-risk patients showed significantly better survival rates compared to high-risk patients (p < 0.001).
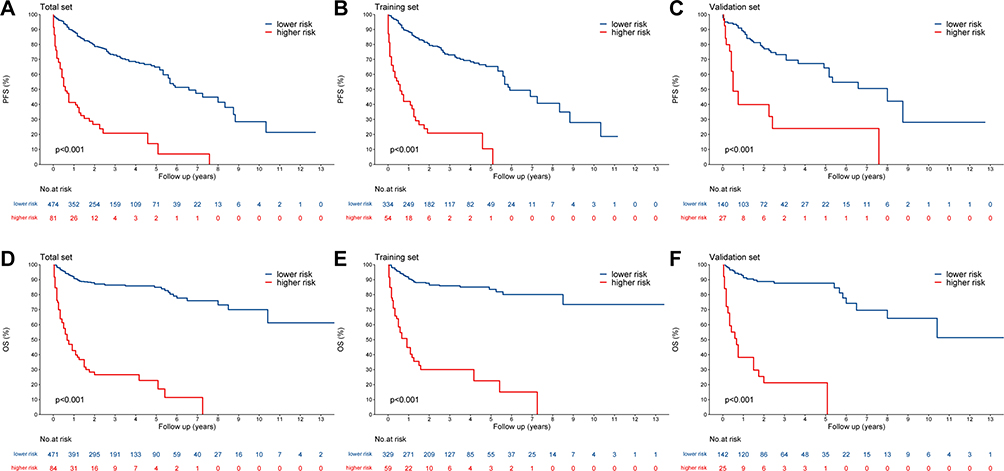 |
Figure 7 Survival curves were stratified by risk for lymphoma patients initially presenting with FUO. The entire population (A), training group (B), and validation group (C) were stratified by risk for PFS survival curve. The entire population (D), training group (E), and validation group (F) were stratified by risk for OS survival curve. |
For OS, the one-year survival rate in the entire cohort was 90.7% for low-risk patients versus 42.7% for high-risk patients (Figure 7D). The low-risk group also showed higher three and five-year rates at 86.4% and 84.9% compared to 26.6% and 22.8% for the high-risk group. In the training set, the one-year OS rates were 90.5% for low-risk versus 44.7% for high-risk (Figure 7E). The three and five-year OS rates were more favorable for the low-risk group at 85.9% and 83.5% against 30.0% and 22.5% for the high-risk group. Finally, in the validation group, the one-year OS rates were 91.2% for low-risk patients contrasted with 38.1% for high-risk (Figure 7F). The three-year OS rate for low-risk was 87.6% as opposed to 21.2% for high-risk, with both groups recording the same five-year OS rate of 87.6% and 21.2%. Across all cohorts, low-risk groups experienced significantly better OS compared to high-risk groups (p < 0.001).
Comparison of Traditional IPI Scoring with the Novel Nomogram Prognostic Model Risk Stratification
Participants were stratified into three risk categories based on the IPI scores: low-risk (0–1 points), intermediate-risk (2–3 points), and high-risk (4–5 points). Kaplan-Meier survival curves for both PFS (Figure 8A) and OS (Figure 8B) were generated according to IPI scores for the entire cohort, as well as separately for the training and validation sets. A novel nomogram-based prediction model was developed for the entire cohort, with optimal cutoff values and threshold scores for risk groups determined by X-tile software. For the PFS nomogram in the training set, participants were classified into low-risk (scores <107.31, n=236, 60.82%), intermediate-risk (scores 107.59 to 151.37, n=102, 26.29%), and high-risk (scores 153.09 to 254.97, n=50, 12.89%). Similarly, for the OS nomogram, the low-risk group scored <40.00 (n=229, 59.02%), intermediate-risk scored 52.93 to 79.87 (n=100, 25.77%), and high-risk scored 80.00 to 132.93 (n=59, 15.21%). As shown in Figure 8A and B, the Kaplan-Meier curves for PFS and OS predicted by the IPI demonstrated no significant distinction between the intermediate-risk and high-risk groups. The AUCs for various clinical endpoints were higher for the nomogram model than for the IPI scoring system in both the training and validation sets (Figure 8C and D). Overall, the nomogram-based prediction models for PFS and OS performed better than the traditional IPI scoring system in risk stratification for lymphoma patients initially presenting with FUO. These results suggest that the novel nomogram model provides improved prediction and prognostic accuracy across different clinical endpoints, surpassing or matching the traditional IPI system’s performance.
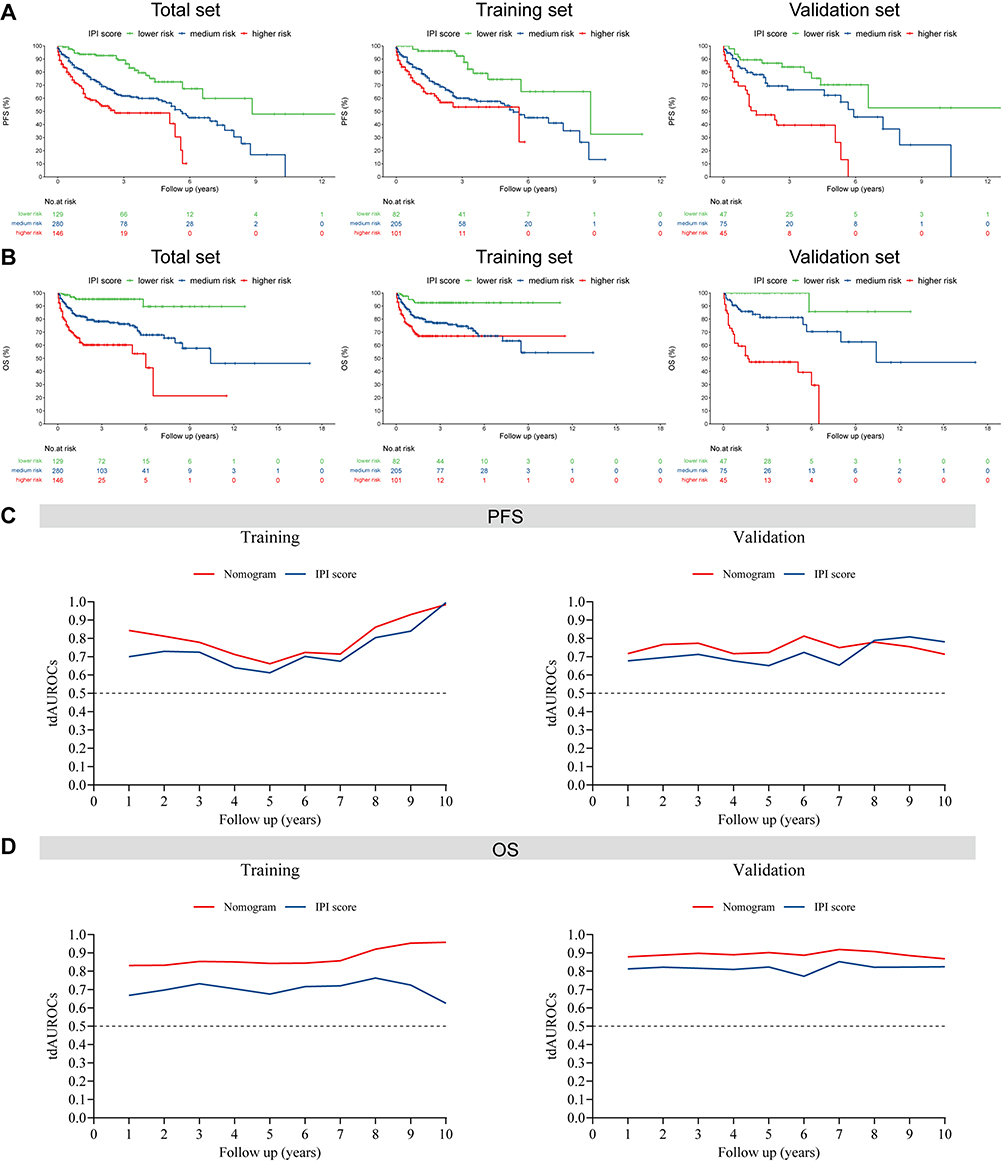 |
Figure 8 Comparison of the IPI Scoring system with a novel nomogram prognostic model for risk stratification in predicting 1-year, 3-year, and 5-year survival rates among lymphoma patients initially presenting with FUO. Kaplan-Meier curves for PFS (A) and OS (B) are examined based on risk stratification using the IPI scoring system, including the entire population, training group, and validation group. The training set and the validation set were compared using time-dependent ROC analysis for PFS (C) and OS (D), assessing the performance of the IPI Scoring system in comparison to a novel nomogram prognostic model. |
Construction of a Website Featuring Dynamic Survival Rate Calculators for Lymphoma Patients
In Figure 9, we successfully developed web-based calculators for estimating the survival rates of patients with FUO lymphoma by integrating nomogram prognostic models using the “shiny” and “DynNom” packages in R. The online availability of these calculators enables the dynamic calculation of OS (https://yangwenjing1997.shinyapps.io/DynNomapp-OS/) and PFS (https://yangwenjing1997.shinyapps.io/DynNomapp-PFS/). Users can enter multiple prognostic factors that influence survival outcomes on the left side of the webpage. For predicting OS, the calculator incorporates the ECOG performance status, EBV infection status, and serum ferritin levels. In contrast, the PFS calculator includes variables such as cytopathology type, ECOG performance status, Ann Arbor stage, platelet count, and direct bilirubin levels. Additionally, the user interface provides graphical representations of survival curves, estimated survival percentages, and detailed summaries of survival outcomes and model specifications. Upon entering individual patient data and requesting a prediction, the interface generates real-time survival curves, illustrated in Figure 9A, which show the differing probabilities of OS over selected time periods. Figure 9B and C illustrate the corresponding 95% CI for these survival probabilities and the numerical prediction of the 2-year OS with its 95% CI, providing a clear quantitative overview for clinicians.
 |
Figure 9 Web-based dynamic calculator for estimating survival rates: (A) (left) Patient information data, (right) patient survival curve over time; (B) (left) Patient information data, (right) 95% confidence interval of the survival rate; and (C) (left) Patient information data, (right) specific numerical values representing the 95% confidence interval of the survival rate. |
Discussion
Lymphoma is a heterogeneous group of hematologic malignancies arising from lymphocytes, broadly categorized into HL, accounting for approximately 10% of cases, and NHL making up the remaining 90%.16 Notably, lymphoma stands as a predominant cause of fever among neoplastic disorders. For some individuals, fever may be the primary symptom of presentation, at times resulting in extended periods of febrile illness.17,18 In the early stages of the disease, some patients may primarily present with FUO without other typical symptoms, and hallmark symptoms may only appear when there is systemic organ involvement, significantly worsening the condition.19,20 Consequently, misdiagnosis or delayed diagnosis will potentially leading to treatment delays. Therefore, the investigation into lymphomas with fever as the initial symptom is imperative and warrants prompt attention.
The etiology of fever in lymphoma remains debated, with several potential mechanisms implicated. One proposed mechanism is the production of endogenous pyrogens by tumor cell nuclei and mononuclear phagocytes, which affect the central thermoregulatory system, leading to an increase in body temperature. This process involves various cytokines including IL-1, IL-6, interferons, tumor necrosis factor, and macrophage inflammatory protein-1 (MIP-1).21 Additionally, lymphoma patients often exhibit compromised immunity due to myriad factors, predisposing them to bacterial, viral, and fungal infections that can induce fever. Another consideration is the direct invasion of the thermoregulatory centers by the tumor cells, contributing to febrile symptoms. Consequently, FUO presentations in lymphoma are not uniformly caused by a single mechanism but appear to result from a complex interplay of multifaceted factors. This suggests that personalized approaches to diagnostic evaluation and therapeutic intervention are warranted, as the underlying cause of fever in lymphoma patients can vary widely. Established prognostic indices, such as the IPI, its revised form (R-IPI), and the National Comprehensive Cancer Network IPI (NCCN-IPI), integrate risk factors like age, performance status, Ann Arbor stage, LDH levels, and the number of extranodal sites involved. However, these models have recognized limitations. The R-IPI offers enhanced predictive performance over the IPI in distinguishing between patients with favorable and adverse long-term outcomes, yet it lacks detail. The NCCN-IPI is noted for its simplicity and better performance in identifying patients at risk of poor outcomes, but it underperforms in detecting those at the highest risk with substantially low survival rates, which is especially relevant for lymphomas associated with FUO. These lymphomas, characterized by rapid progression and poor survival, tend to be underestimated by existing prognostic models. To address this, our study aimed to establish a prognostic scoring system tailored for FUO lymphomas to improve risk stratification, ultimately enhancing patient-specific and standardized clinical decision-making.
In this study, we conducted a retrospective review of 555 lymphoma cases with FUO as an initial symptom admitted to the Hematology Department at Huadong Hospital from January 2013 to December 2021. We compiled a dataset inclusive of clinical presentations, diagnostic information, treatment choices, and survival data pertinent to FUO lymphoma patients. By employing univariate and multivariate Cox proportional hazards regression models, we identified significant prognostic factors, laying the foundation for future clinical trials and risk management strategies. Our analysis identified a higher incidence of FUO lymphoma in female patients. Consistent with prior work, our study shows that patients with lymphoma presenting as FUO frequently have advanced disease stages, a poor performance status, and high IPI scores. The outlook is especially poor for individuals with liver, spleen, and bone marrow involvement. NK/T-cell lymphoma patients have worse outcomes than those with other histological subtypes. These patients often present with leukopenia, anemia, thrombocytopenia, increased LDH, high ferritin, rapid erythrocyte sedimentation rates, low albumin, and elevated β2-microglobulin. It has been noted in prior research that peripheral blood smear analyses may fail to detect abnormal cells in the early phases of certain hematological malignancies characterized by fever.21 As a result, a thorough diagnostic approach, including whole-body CT, PET/CT, and bone marrow biopsy, is critical for accurate diagnosis.5 There is a substantial gap in the understanding of hematological malignancies among patients, complicating the diagnostic and treatment process. Therefore, achieving timely detection, precise diagnostics, and accurate treatment strategies are both challenging and vital in the management of lymphoma.
Multiple prognostic factors influence lymphoma outcomes, but the IPI is particularly seminal, providing pre-treatment outcome estimations and facilitating clinical treatment stratification. The IPI encompasses age, performance status (ECOG), Ann Arbor stage, serum LDH levels, and extranodal disease, assisting in timely response evaluations. Though the R-IPI and NCCN-IPI have demonstrated considerable predictive accuracy across various lymphomas, their performance in lymphoma-associated FUO warrants further examination. Despite the traditional IPI’s focus on prognostic indicators in lymphoma, its applicability to FUO lymphoma—characterized by complexity and aggressiveness—is limited. It overlooks the role of immune responses to both tumor cells and pyrogenic stimuli, like tumor necrosis factor-alpha and interleukins, which can induce fever via hypothalamic pathways.22 In the age of rituximab and targeted immunotherapies, these treatments have markedly enhanced some lymphoma patients’ prognoses, challenging the traditional IPI’s precision in these cohorts.23 Consequently, for lymphoma initially presenting with FUO, pinpointing optimal treatments is crucial, as is the development of clinically viable prognostic tools for early intervention in high-risk patients. This approach could lead to improved management and treatment outcomes.
In the development of prognostic models for lymphoma, various scoring systems have emerged to stratify patients with fever-associated lymphoma, differentiating those at higher risk and with poor prognosis at an early stage. For instance, Schwartz et al (2017) analyzed data from 1,103 young Hodgkin lymphoma patients to construct a model predicting event-free survival, where fever was identified as an independent risk factor with notable predictive accuracy.24 As targeted and immunotherapies evolve, the adequacy of classical scoring systems, such as the IPI and its R-IPI, to reflect disease progression changes is questioned. Modern approaches consider factors like predictive genomic mutations and functional alterations in genes such as JAK1, JAK2, and B2M that influence clinical outcomes and necessitate a reevaluation of prognostic models. Lim et al (2022) employed next-generation sequencing on 260 lymphoma samples to establish a genomic prognostic model (GPM) using LASSO Cox regression.25 This model identified mutations in pivotal genes, including PD-L1, DDX3X, and TP53, which are involved in critical pathways of lymphomagenesis. As such, the GPM enhances existing systems by providing an improved prediction of adverse event risk. In our database of FUO lymphoma patients, we have developed new models for PFS and OS. These models integrate traditional IPI variables, such as performance status and Ann Arbor staging, with novel prognostic indicators. The PFS model incorporates factors like cell pathology type, platelet count, and direct bilirubin level, whereas the OS model includes concurrent EB virus infection and ferritin levels. Given the heterogeneity among patients, the variability in treatment responses, and differences in therapeutic choices, the impact on prognosis may differ across studies. Nevertheless, the ECOG performance status at diagnosis consistently remains a critical prognostic element for fever-presenting lymphoma patients, applicable across both traditional IPI and our novel prognostic models.
Elevated ferritin levels, known as an iron storage protein associated with inflammation, were found to be an independent risk factor for overall survival in lymphoma patients initially presenting with FUO.26 Although serum ferritin levels were not previously evaluated in the IPI score, research has shown a significant association between elevated serum ferritin levels in malignant tumor patients and disease progression.27 While some reports have suggested that high serum ferritin levels are indicative of poor prognosis in lymphoma patients, its specific significance in lymphoma patients initially presenting with FUO is still unclear.28 Hence, this study included ferritin as an independent prognostic factor in the risk prediction model. The potential mechanism behind the elevated ferritin in lymphoma patients initially presenting with FUO is currently uncertain and this study aims to explore its relationship with poor prognosis in these patients. It is suggested that iron, crucial for cell proliferation, is required in larger quantities by tumor cells.25 Additionally, ferritin is highly expressed in tumor-associated macrophages, which have been linked to tumor cell proliferation and treatment resistance. Therefore, effectively reducing ferritin levels in the serum of lymphoma patients may disrupt the immune microenvironment, which is favorable for tumor cell growth, and aid in killing the tumor cells. Strengths and Clinical Implications of the Study: In an era of rapid advancements in targeted and immunotherapies, the prognostic performance of the traditional IPI has been outpaced, necessitating novel prognostic tools. This study retrospectively examined lymphoma patients with fever as an initial symptom and identified independent risk factors pertinent to several clinical outcomes. Unlike other models that employ generic statistical techniques, our approach utilized the LASSO method, leveraging its shrinkage attributes for enhanced variable selection. This process has enhanced the model’s reliability and stability, as the factors included are not limited to statistical significance. Additionally, the parameters of our prognostic model consist of widely accessible clinical factors, offering clinicians a practical tool for prognosis assessment and risk stratification in this subset of lymphoma patients.
There are some limitations in our current study. Small sample size and incomplete clinical data collection restricted our analysis. Cost and complexity of diagnostics like cytokine assays and FISH led to data gaps, hindering detailed study of pathological factors in FUO lymphoma patients. Additionally, determining baseline viral loads in Epstein-Barr virus co-infected patients was challenging. Future work, with adequate resources, should include pathological and genetic data to evaluate the impact of the immune microenvironment and molecular features on prognosis.
Conclusion
In conclusion, this study has delineated valuable instruments for the clinical management of lymphoma patients initially presenting with FUO. Predictive nomograms for PFS and OS have been devised, along with a user-friendly survival rate calculator. These tools enable clinicians to accurately assess prognosis and customize treatment strategies for lymphoma patients initially presenting with FUO, thereby enhancing individualized precision medicine in clinical practice.
Data Sharing Statement
The corresponding author are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All data are provided in this study, and raw data can be requested to the corresponding author.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by Institutional Review Board of Huadong Hospital Affiliated with Fudan University (No. 20210021). All the study subjects provided informed consent.
Author Contributions
Lin Shen and Wenjing Young share the first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was approved by the Shanghai Science and Technology Committee(19DZ1910300).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Fridrik MA. ASCO update on lymphoma. Memo. 2017;Vol. 10(4):218–219.
2. Liu W, Liu J, Song Y, et al. Burden of lymphoma in China, 2006-2016: an analysis of the global burden of disease study 2016. J Hematol Oncol. 2019;12(1):115. doi:10.1186/s13045-019-0785-7
3. Ansell SM. Non-Hodgkin lymphoma: diagnosis and treatment. Mayo Clin Proc. 2015;90(8):1152–1163. doi:10.1016/j.mayocp.2015.04.025
4. Cunha BA, Chawla K. Fever of unknown origin (FUO): CMV infectious mononucleosis or lymphoma? Eur J Clin Microbiol Infect Dis. 2018;37(7):1373–1376. doi:10.1007/s10096-018-3262-2
5. El-Galaly TC, Villa D, Gormsen LC, et al. FDG-PET/CT in the management of lymphomas: current status and future directions. J Intern Med. 2018;284(4):358–376. doi:10.1111/joim.12813
6. Besson FL, Chaumet-Riffaud P, Playe M, et al. Contribution of (18)F-FDG PET in the diagnostic assessment of fever of unknown origin (FUO): a stratification-based meta-analysis. Eur J Nucl Med Mol Imaging. 2016;43(10):1887–1895. doi:10.1007/s00259-016-3377-6
7. Takeuchi M, Nihashi T, Gafter-Gvili A, et al. Association of 18F-FDG PET or PET/CT results with spontaneous remission in classic fever of unknown origin: a systematic review and meta-analysis. Medicine. 2018;97(43):e12909. doi:10.1097/MD.0000000000012909
8. Zhou Z, Sehn LH, Rademaker AW, et al. An enhanced international prognostic index (NCCN-IPI) for patients with diffuse large B-cell lymphoma treated in the rituximab era. Blood. 2014;123(6):837–842. doi:10.1182/blood-2013-09-524108
9. Jacobsen E. Follicular lymphoma: 2023 update on diagnosis and management. Am J Hematol. 2022;97(12):1638–1651. doi:10.1002/ajh.26737
10. Chen F, Long H, Ding J, et al. Prognostic nomogram for primary splenic lymphoma: a SEER database-based study. Am J Cancer Res. 2023;13(12):5825–5845.
11. Wu M, Wulipan F, Ma J, et al. Clinical characteristics and prognostic factors of lymphoma patients initially presenting with fever of unknown origin. Am J Transl Res. 2022;14(4):2625–2636.
12. Wang G, Jiang X, Fu Y, et al. Development and validation of a nomogram to predict the risk of sepsis-associated encephalopathy for septic patients in PICU: a multicenter retrospective cohort study. J Intensive Care. 2024;12(1):8. doi:10.1186/s40560-024-00721-7
13. Johnson SA, Kumar A, Matasar MJ, et al. Imaging for staging and response assessment in lymphoma. Radiology. 2015;276(2):323–338. doi:10.1148/radiol.2015142088
14. Alaggio R, Amador C, Anagnostopoulos I, et al. The 5th edition of the World Health Organization classification of haematolymphoid tumours: lymphoid neoplasms. Leukemia. 2022;36(7):1720–1748. doi:10.1038/s41375-022-01620-2
15. Azam F, Latif M, Farooq A, et al. Performance status assessment by using ECOG (Eastern Cooperative Oncology Group) score for cancer patients by oncology healthcare professionals. Case Rep Oncol. 2019;12(3):728–736. doi:10.1159/000503095
16. Mugnaini EN, Ghosh N. Lymphoma. Prim Care. 2016;43(4):661–675. doi:10.1016/j.pop.2016.07.012
17. Kaya A, Ergul N, Kaya SY, et al. The management and the diagnosis of fever of unknown origin. Expert Rev Anti Infect Ther. 2013;11(8):805–815. doi:10.1586/14787210.2013.814436
18. Ruppert AS, Dixon JG, Salles G, et al. International prognostic indices in diffuse large B-cell lymphoma: a comparison of IPI, R-IPI, and NCCN-IPI. Blood. 2020;135(23):2041–2048. doi:10.1182/blood.2019002729
19. Pasikhova Y, Ludlow S, Baluch A. Fever in patients with cancer. Cancer Control. 2017;24(2):193–197. doi:10.1177/107327481702400212
20. Søgaard KK, Farkas DK, Leisner MZ, et al. Fever of unknown origin and incidence of cancer. Clin Infect Dis. 2022;75(6):968–974. doi:10.1093/cid/ciac040
21. Jaeger A, Gambheer SMM, Sun X, et al. Activated granulocytes and inflammatory cytokine signaling drive T-cell lymphoma progression and disease symptoms. Blood. 2023;141(23):2824–2840. doi:10.1182/blood.2022015653
22. Lee D, Ryu H, Jung E. Effect of Fever on the Clinical Outcomes of Traumatic Brain Injury by Age. Medicina. 2022;58(12):1860.
23. Jurczak W, Długosz Danecka M, Buske C. Rituximab biosimilars for lymphoma in Europe. Expert Opin Biol Ther. 2019;19(10):1045–1056. doi:10.1080/14712598.2019.1665017
24. Schwartz CL, Chen L, McCarten K, et al. Childhood Hodgkin International Prognostic Score (CHIPS) predicts event-free survival in Hodgkin lymphoma: a report from the children’s oncology group. Pediatr Blood Cancer. 2017;64(4):e26278. doi:10.1002/pbc.26278
25. Lim JQ, Huang D, Chan JY, et al. A genomic-augmented multivariate prognostic model for the survival of natural-killer/T-cell lymphoma patients from an international cohort. Am J Hematol. 2022;97(9):1159–1169. doi:10.1002/ajh.26636
26. Yoh KA, Lee HS, Park LC, et al. The prognostic significance of elevated levels of serum ferritin before chemotherapy in patients with non-Hodgkin lymphoma. Clin Lymphoma Myeloma Leuk. 2014;14(1):43–49. doi:10.1016/j.clml.2013.09.008
27. Karakatsanis S, Panitsas F, Arapaki M, et al. Serum ferritin levels in previously untreated classical Hodgkin lymphoma: correlations and prognostic significance. Leuk Lymphoma. 2022;63(4):799–812. doi:10.1080/10428194.2021.2010054
28. Tachibana T, Andou T, Tanaka M, et al. Clinical significance of serum ferritin at diagnosis in patients with acute myeloid leukemia: a YACHT multicenter retrospective study. Clin Lymphoma Myeloma Leuk. 2018;18(6):415–421. doi:10.1016/j.clml.2018.03.009
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.