")
Back to Journals » Clinical Ophthalmology » Volume 18
A Novel Corneal Remodeling Technique of Laser Asymmetric Keratectomy in Keratoconus Suspect: A Retrospective Case Control Study
Received 16 August 2024
Accepted for publication 24 October 2024
Published 1 November 2024 Volume 2024:18 Pages 3125—3131
DOI https://doi.org/10.2147/OPTH.S486687
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ji Sang Min,1 Byung Moo Min2
1Department of Ophthalmology, The Institute of Vision Research, Yonsei University College of Medicine, Seoul, 03722, Republic of Korea; 2Woori Eye Clinic, Affiliated Clinical Professor to Department of Ophthalmology, Yonsei University College of Medicine, Daejon, 35229, Republic of Korea
Correspondence: Byung Moo Min, Woori Eye Clinic, Affiliated Clinical Professor to Department of Ophthalmology, Yonsei University School of Medicine, Daeduk Daero 219 (Dunsan-dong), Seo-gu, Daejon, 35229, Republic of Korea, Tel +82-42-476-1675, Fax +82-42-476-1670, Email [email protected]
Purpose: This retrospective case control study report includes 4 eyes of 4 patients (aged from 37 to 44 years) with keratoconus suspect (KCS) who underwent laser epithelial keratomileusis linked laser asymmetric keratectomy (L-LAK) as corneal remodeling technique in order to avoid postoperative corneal ectasia.
Patients and Methods: Four eyes of 4 patients showed corneal topography findings with abnormal localized steep keratometric curvature greater than 47.0 D and peripheral corneal thickness asymmetry (Total corneal central thickness deviations in four directions on Orbscan map (SUM)≥ 80 μm). L-LAK could be performed both the original ablation of refractive errors (SE from − 1.25 to − 5.50 D) and the customized ablation (selective ablation of the thicker peripheral cornea averaging:64 μm selectively and the central cornea of the myopic shift due to LAK averaging-1.50D. The main outcome measures between preoperative and postoperative 2 year were refraction, visual acuity (UDVA), keratometry, corneal symmetry evaluating SUM.
Results: After 2 years, SEs (D, average) were − 0.34, UDVA (LogMAR) was 0.00. keratometry including Kmax was markedly decreased, SUM had diminished markedly. There were no case of postoperative adverse effects.
Conclusion: L-LAK resulted in a decreased SUM, increased corneal symmetry, and no postoperative corneal ectasia with good visual outcomes in myopic patients with KCS.
Keywords: keratoconus suspect, corneal remodeling, L-LAK, KCS, linked laser asymmetric keratectomy
Introduction
Keratoconus suspect (KCS) has been one type of three earliest stage keratoconus. Referring to the earliest stage keratoconus, three names were widely encountered in the literature: forme fruste keratoconus (FFKC), preclinical or subclinical keratoconus, and KCS. For KCS, until now not defined definition, but focal steepening of the cornea over +47.0 D or slight bowing on topography, and asymmetric corneal thickness were important findings in diagnosis, and other several opinions were showed.1
True KCS is an absolute contraindication to laser refractive surgery (LRS) due to postoperative corneal ectasia,2 possibly due to the thinner corneal steepening as an interaction of intraocular pressure, corneal stiffness and corneal thickness.3
Laser asymmetric keratectomy (LAK) as biomechanical customized method, linked with Vision Up software (Well C, approved FDA of Republic of Korea) has reported good results and the improvement of corneal symmetry because it could ablate only thicker peripheral cornea selectively.3–6 In evaluating corneal symmetry, SUM (The sum of corneal central thickness deviations in four directions on Orbscan map) as a new evaluation index was reported and very useful.3–6
And also, LAK, so called, crescent keratectomy was reported to be good surgical results as corneal remodeling technique in patients with KCS, keratoconus.6,7
Laser epithelial keratomileusis linked laser asymmetric keratectomy (L-LAK) corrected refractive powers and also reduced SUM; it showed good surgical outcomes without postoperative adverse effects such as myopic regression in myopic patients with KCS.6
In this brief report, we will present the surgical techniques and outcomes of L-LAK as customized method to correct the refractive powers and also decrease the SUM in order to avoid LRS adverse effects.
Patients and Methods
This pilot study short report is about the surgical technology and postoperative results of L-LAK and included 4 eyes of 4 myopic patients with KCS. This study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 1983, and approved by the Korean National Institute for Bioethics Policy (approval No P01-202,101-21-004) as retrospective study. Written informed consent was obtained from all subjects involved in the study for publication of the details of their medical case and any accompanying images.
L-LAK was performed 4 patients with KCS by Min BM at the Woori Eye Clinic between January 2018 and July 2018. KCS was diagnosed as corneal topography findings with abnormal localized steep keratometric curvature greater than 47.0 D or an asymmetric bowtie pattern, a normal-appearing cornea on slit lamp biomicroscope, and at least 1 of the following signs: peripheral corneal thickness asymmetry (SUM≥80 µm), oblique cylinder greater than 1.50 D, central corneal thickness less than 500 µm, or clinical KC in the fellow eye.6,8–10
The Vision-Up software3–6 was used to improve corneal shape (Figure 1A). The ablation amount, the direction, range of thicker cornea, and the amount of myopic shift due to LAK were evaluated with the Vision-Up software3–6 we could ablate the thicker cornea selectively with the excimer laser machine interfaced the Vision Up software, so the cornea could be become symmetric cornea without refractive errors (customized ablation, Figure 2), as determined by LAK. In four myopic patients (SE from −1.25 to −5.50 D, age from 37 to 44 years) with KCS manifesting focal corneal steepening over +47 diopters (average:48.30D) and a SUM of ≥ 80 µm (average:157 µm), L-LAK was recommended to improve corneal shape (Table 1). The 7.0 mm optic zone and 7–9 mm in transitional zone were ablated for correcting refractive errors without epithelium of a 10.0–10.5-mm in diameter for LASEK.
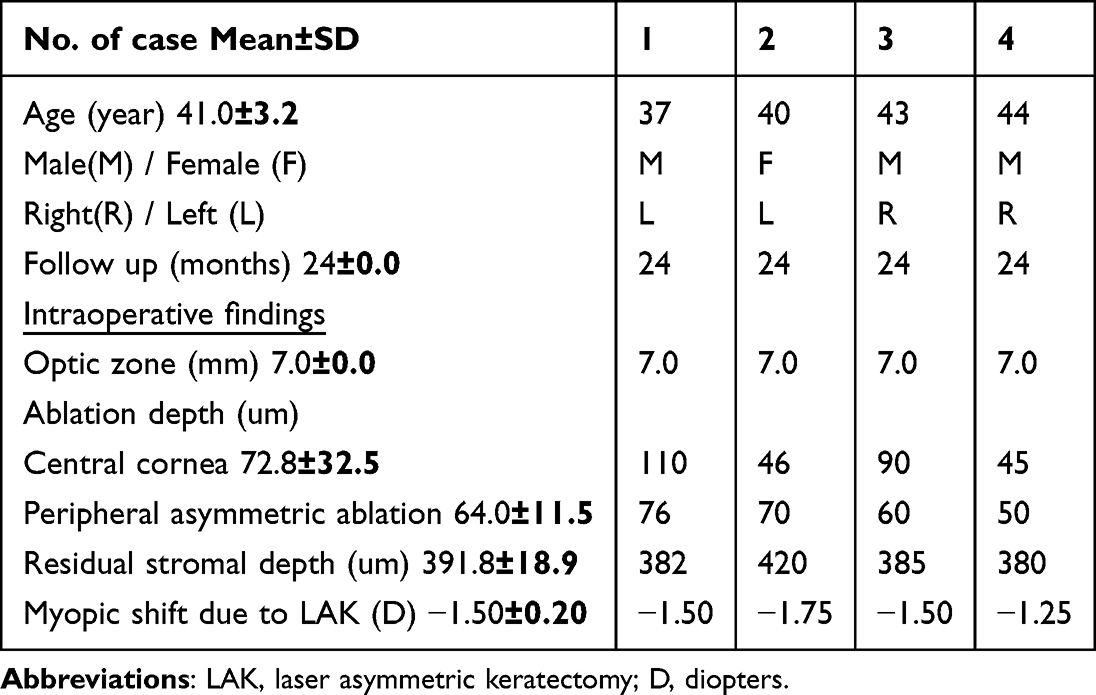 |
Table 1 Patients Findings |
 |
Figure 1 Pre and post-L-LAK Orbscan map of case 1. (A) Pre-L-LAK Orbscan map of case 1. Right bottom shows a pachymetric map: an example of measuring the differences in thickness between symmetrically opposed points is shown on the pachymetric map (0–180°, 45–225°, 90–270°, and 135–315°): 0–180°: 33 µm; 45–225°: 17µm; 90–270°: 8 µm; 135–315°:46 µm; total (SUM): 104 µm. (B) Post-L-LAK Orbscan map of case 1. Right bottom shows a pachymetric map: an example of measuring the differences in thickness between symmetrically opposed points is shown on the pachymetric map (0–180°, 45–225°, 90–270°, and 135–315°): 0–180°: 11 µm; 5–225°: 20µm; 90–270°: 6 µm; 135–315°:13 µm; total (SUM): 50 µm. |
 |
Figure 2 L-LK ablation planning of case 1. (A) Original ablation plan of refractive errors (−3.50=−4.00,180°) of case 1 (B) LAK customized ablation of the thicker peripheral cornea evaluated by Vision Up software (Well C, Republic of Korea) on Orbscan II (Bausch & Lomb, Bridgewater, NJ, USA) corneal maps. (C) L-LAK ablation plan (total ablation= original ablation + customized ablation+ ablation of induced myopic shift due to LAK). |
After analyzing the thicker corneal regions with the Vision-Up software (WellC, Republic of Korea) on topography (Figure 1),3–6 we performed original ablation (Figure 2A) and customized ablation (Figure 2B) (selective ablation of the thicker peripheral cornea (average:64 µm) and the central cornea of the myopic shift (average:-1.50D) due to LAK with the same laser machine of a 193-nm ISO-D 200 laser (Kera Harvest Inc., Taiwan) interfaced with the Vision-Up software (WellC, Republic of Korea). So, the cornea was improved shape to be symmetric without the refractive errors (Figure 1B and Figure 2C). The following variables were analyzed: the pre- and 2-year postoperative L-LAK spherical equivalent (SE), sphere, cylinder, uncorrected distance visual acuity (UDVA, LogMAR), intraocular pressure (IOP), pupil size, MeanK, Kmax, central pachymetry (CP), SUM (µm). The refraction was measured using an auto refractometer/keratometer and was calculated as the SE. UDVA was measured at a distance of 3m using the Han Chun Suk visual distance acuity chart, and was converted to the logarithm of the minimum angle of resolution (LogMAR). IOPs were measured by applanation tonometer. CP, pupil size were measured on Orbscan II. Pre- and postoperative corneal symmetry were evaluated by SUM on Orbscan maps3–6 (Figure 1).
Results
Four eyes of four myopic patients (SE:-3.25±1.81 from −1.25 to −5.50 D, age: 41.0±3.2 from 37 to 44 years) underwent the L- LAK because of SUM ≥80 µm on Orbscan maps and Kmax ≥47.0D. Three male patients and 1 female patient. Intraoperatively, ablation depths (µm) of center and periphery were 72.8±32.5(45–110), 64.0±11.5(50 −76), respectively for L- LAK, myopic changes (D) after LAK were −1.50±0.20(−1.25 – −1.75), residual stromal depth (µm) was 391.8±18.9(380–420) at L- LAK (Table 1). After 2 years, the UDVA (LogMAR) was better from 0.53 preoperatively to 0.00 postoperatively; hence, the L- LAK exhibited good visual results, and there was no postoperative cylindrical axial changes, the intraocular pressures and pupil size of the patients were similar between pre- and postoperative 2 year. Keratometry (MeanK, Kmax) (diopters) had decreased from +45.40±0.76 to +42.7±1.7, +48.30±0.26 to +44.03±1.29, respectively and the CP (µm) had changed from 577.8±18.9 to 513.8±43.8. There were no postoperative complications such as, myopic changes, severe dry eye, and halos etc. Further, SUM (µm) had diminished markedly from 156.8±42.1 preoperative to 59.0±6.1 postoperative (Table 2).
 |
Table 2 Pre- and Post-Operative Findings |
Postoperative 2 year later the SUM and Kmax markedly decreased postoperatively 59.0±6.1 µm, +44.03±1.29D, respectively). Good visual outcomes were showed without corneal ectasia after L-LAK (Table 2).
Discussion
All patients with KCS showed steep keratometric curvature greater than 47D, and SUM ≥ 80μm, which was one of the most important criteria of KCS. If patients with asymmetric cornea (the SUM ≥80 µm), the thinner corneal portion became easily protruded postoperatively due to biomechanical reactions, causing to corneal ectasia.3–6 It is explained that asymmetric corneal thickness and uneven curvature could be caused by biomechanical property distribution.3–6
In the patients SUM showed 157 μm in average preoperatively that showed higher than that of the symmetric cornea (SUM <80 μm). So Kmax showed over 47.0D. But at postoperative 2 year, SUM, and Kmax showed 59 μm, 44.03D, respectively Postoperative even cornea after decreasing corneal steepening over +47D is different than the previous our studies of LASIK with LAK in asymmetric cornea, and also in Min JS & Min BM ‘s study, LASIK with LAK reduced total corneal thickness deviation, improved corneal symmetry, and reduced blurring scores significantly than in LASIK without LAK in patients with SUM 80≥ µm.3
We employed the Orbscan maps for corneal topography visualization rather than the current Sheimpflug techniques. SUM can be calculated only on an Orbscan map because these maps feature a central visual axis and, thus, they are very useful for measuring symmetry.
Vision-Up software (Well C, Republic of Korea) was newly developed and approved in Republic of Korea, FDA and calculated corneal customized ablation plan (amounts of thicker cornea, the direction and range of laser ablation, and induced myopia due to LAK), so could be possible to be symmetric cornea and also correct the original refractive errors simultaneously.3–6 L-LAK could correct refractive errors (original ablation) and also improve corneal symmetry with reducing SUM (crescentic customized ablation), and also could avoid post-LASIK adverse effects including corneal ectasia in myopic patients with asymmetric corneal thickness (SUM Orbscan maps >80 µm).3–6 LAK could be new corneal remodeling method to make symmetric cornea on KCS or keratoconus with peripheral asymmetry of corneal thickness.6
LAK reduced SUM, improved corneal symmetry, could resolve shortcomings of LRS, It is a customised biomechanical asymmetric corneal ablation method that has been recently introduced; this method aims to achieve central-symmetric corneal thickness, and the improved corneal shape is maintained long-term without deformation, thus preventing visual abnormalities and increases corneal symmetry by decreasing SUM, and thereby, it is expected to prevent postoperative corneal changes to avoid postoperative LRS adverse effects such as reduced visual acuity due to postoperative myopic shift, blurring vision, etc.3 So it will be safe in correct myopic patients with KCS, especially with asymmetric cornea (SUM >80 µm) and focal steepening over +47.0 diopters. Additionally, it has been reported that LAK, in which only the thick parts of the cornea are cut to create central symmetry, can be a good method to: 1) avoid LRS's adverse effects;3 2) treat the distorted cornea after ocular surgeries, reduce the incidence of optical aberrations;4,6,11 and 3) reduce the effects of IOP pushing outward on the thin parts of the cornea in early KC or KCS with peripheral asymmetry of the corneal thickness.5,6 In addition, further research on LAK and treatment indications needs to be conducted.
L-LAK could be a new corneal remodeling method,3–6 to make the cornea be symmetric in patients with KCS (SUM ≥80 µm and Kmax ≥ 47D),3–6without postoperative corneal ectasia. It indicated in order to avoid LRS adverse effects,3 a new enhancement method in patients with adverse effects after LRS,4 management of postoperative LRS or ocular surgery adverse effects,5,7 and a new corneal remodeling technique in KCS without postoperative corneal ectasia.6
But in this study, the number of cases is very limited, relative short follow up periods and not copmpative, so need large cases study, long term follow up and comparative study including combined corneal collagen crosslinking technique.
Conclusion
L-LAK, a new corneal remodeling method, resulted in a decreased SUM, increased corneal symmetry, and no postoperative corneal ectasia with good visual outcomes in myopic patients with KCS manifesting peripheral corneal asymmetry (SUM) ≥80 µm) and focal steep keratometric curvature greater than 47D.
Abbreviations
KCS, keratoconus suspect; UDVA, uncorrected distance visual acuity; LAK, laser asymmetric keratectomy; FFKC, forme fruste keratoconus; LRS, laser refractive surgery; SE, spherical equivalent; IOP, intraocular pressure.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 1983, and approved by the Korean National Institute for Bioethics Policy (approval No P01-202101-21-004) as retrospective study. Written informed consent for participation was obtained from all subjects involved in the study.
Consent for Publication
Written informed consent was obtained from all subjects involved in the study for publication of the details of their medical case and any accompanying images.
Acknowledgments
We would like to thank Editage (www.editage.co.kr) for English language editing, and Hye Won Jung, Rag Seon Han, Eun Mi Jang, Ji Yeon Choi, Mi Kyung Kim, Ji Suk Kwon, and Sun Hee Lee at the Woori Eye Clinic for assisting with the ocular examinations. Authors have no financial or proprietary interest in any material or method mentioned.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shi Y. Strategies for improving the early diagnosis of keratoconus. Clin Optom. 2016;8:13–21. doi:10.2147/OPTO.S63486
2. Randleman JB. Post-laser in-situ keratomileusis ectasia: current understanding and future directions. Curr Opin Ophthalmol. 2006;17(4):406–412. doi:10.1097/01.icu.0000233963.26628.f0
3. Min JS, Min BM. Comparison between surgical outcomes of LASIK with and without laser asymmetric keratectomy to avoid conventional laser refractive surgery adverse effects. Sci Rep. 2020;10(1):10446. doi:10.1038/s41598-020-67269-y
4. Min JS, Min BM. A novel approach to enhancement linked laser asymmetric keratectomy using semi-cylindrical ablation pattern in patients with myopic regression after laser refractive surgery. Clin Ophthalmol. 2021;15:1751–1758. doi:10.2147/OPTH.S306636
5. Min JS, Min BM. Clinical outcomes of laser asymmetric keratectomy to manage postoperative adverse effects-A retrospective clinical trial. TOOPHTJ. 2021;15(1):171–177. doi:10.2174/1874364102115010171
6. Min JS, Lee DC, Lee SS, Min PM. A novel approach for corneal remodeling of laser asymmetric keratectomy with collagen cross linking in patients with keratoconus suspect. TOOPHTJ. 2024;18(1):e18743641282093. doi:10.2174/0118743641282093231228053309
7. Carriazo C, Cosentino MJ. A novel corneal remodeling technique for the management of keratoconus. J Refract Surg. 2017;33(12):854–856. doi:10.3928/1081597X-20171004-05
8. Klyce SD. Chasing the suspect: keratoconus. Br J Ophthalmol. 2009;93(7):845–847. doi:10.1136/bjo.2008.147371
9. Li X, Yang H, Rabinowitz YS. Keratoconus: classification scheme based on videokeratography and clinical signs. J Cataract Refract Surg. 2009;35(9):1597–1603. doi:10.1016/j.jcrs.2009.03.050
10. Schlegel Z, Hoang-Xuan T, Gatinel D. Comparison of and correlation between anterior and posterior corneal elevation maps in normal eyes and keratoconus-suspect eyes. J Cataract Refract Surg. 2008;34(5):789–795. doi:10.1016/j.jcrs.2007.12.036
11. Min JS, Jin YJ, Min BM. Early postoperative topographic changes after laser asymmetric keratectomy for the management of adverse effects after photorefractive keratectomy. J Ophthalmol. 2020;1:1–7.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.