")
Back to Journals » Journal of Inflammation Research » Volume 17
A Novel Inflammatory Indicator for Tuberculosis-Associated Obstructive Pulmonary Disease (TOPD): The Systemic Inflammatory Response Index (SIRI)
Authors Hu S, Yu Q, Liu F, Gong F
Received 11 March 2024
Accepted for publication 12 June 2024
Published 2 July 2024 Volume 2024:17 Pages 4219—4228
DOI https://doi.org/10.2147/JIR.S468232
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Shengling Hu, Qi Yu, Fenfang Liu, Fengyun Gong
Department of Infectious Diseases, Wuhan Jinyintan Hospital, Tongji Medical College of Huazhong University of Science and Technology; Hubei Clinical Research Center for Infectious Diseases; Wuhan Research Center for Communicable Disease Diagnosis and Treatment, Chinese Academy of Medical Sciences; Joint Laboratory of Infectious Diseases and Health, Wuhan Institute of Virology and Wuhan Jinyintan Hospital, Chinese Academy of Sciences, Wuhan, 430023, People’s Republic of China
Correspondence: Fengyun Gong, Department of Infectious Diseases, Wuhan Jinyintan Hospital, Tongji Medical College of Huazhong University of Science and Technology; Hubei Clinical Research Center for Infectious Diseases; Wuhan Research Center for Communicable Disease Diagnosis and Treatment, Chinese Academy of Medical Sciences; Joint Laboratory of Infectious Diseases and Health, Wuhan Institute of Virology and Wuhan Jinyintan Hospital, Chinese Academy of Sciences, Wuhan, 430023, People’s Republic of China, Email [email protected]
Background: The development of chronic obstructive pulmonary disease (COPD) following tuberculosis (TB) is known as tuberculosis-associated obstructive pulmonary disease (TOPD). This study aimed to explore the predictive value of inflammatory indicators for TOPD in TB patients.
Methods: Data for this cross-sectional study were collected between January 2014 and January 2022 at Wuhan Jinyintan Hospital. The ratio of inflammatory indicators, including Systemic Inflammatory Response Index (SIRI), C-reactive protein-to-lymphocyte ratio (CLR), eosinophil count-to-lymphocyte count ratio (ELR), were calculated. Univariate and multivariate logistic regression analyses were conducted to explore the association between the ratio of inflammatory indicators and TOPD. Furthermore, the relationship between the ratio of inflammatory indicators and TOPD was investigated using propensity score matching (PSM) and receiver operating characteristic (ROC) curve analysis was performed to evaluate their predictive value for TOPD.
Results: The present study included a total of 737 patients, of whom 83 participants (11.26%) had TOPD. Sixty-nine TOPD patients and 69 non-TOPD (NTOPD) patients were successfully matched. Univariate and multivariable logistics regression analysis, conducted before and after PSM, revealed that SIRI was independently significantly associated with an increased risk of TOPD. The area under curve (AUC) of SIRI were 0.702 and 0.668 before and after PSM, respectively. Additionally, patients were stratified into four different groups based on SIRI quartiles for further analysis. The prevalence of TOPD in TB patients showed an increase with higher SIRI values, both before and after PSM.
Conclusion: Levels of inflammatory indicators were higher in TOPD patients when compared to NTOPD patients. SIRI may be a simple and useful inflammatory index for assessing TOPD, and TB patients with higher values of SIRI are more likely to be high-risk group for TOPD.
Keywords: tuberculosis-associated obstructive pulmonary disease, systemic inflammatory response index, ratio inflammatory indicator, propensity score matching
Introduction
Chronic obstructive pulmonary disease (COPD) is now ranked as the third leading cause of death following cardiovascular disease and stroke,1 which is characterized by persistent, progressive and exacerbated airflow obstruction along with chronic systemic inflammation.2 Although smoking is a conventional risk factor for COPD, a history of pulmonary tuberculosis has been reported as a risk factor for chronic airflow obstruction, particularly in developing countries.3–5 Even after adjusting for age, gender and smoking history, previous tuberculosis infection remains independently associated with airflow obstruction.6,7 Globally, tuberculosis (TB) ranks as the second most deadly infectious disease after COVID-19. In 2022, an estimated 10.6 million individuals worldwide contracted tuberculosis.8 Unlike many other respiratory infections, TB tends to cause permanent damage or destruction to host tissues, transforming it from a treatable infectious ailment into a chronic condition.9 COPD could arise during the course of tuberculosis or following completion of tuberculosis treatment. The term of tuberculosis-associated obstructive pulmonary disease (TOPD) was first coined by Allwood et al10 Histological study in TOPD patients confirmed distortion in small pathways and blood vessels, indicating a phenotype other than smoking-associated COPD.5,11
Although the pathogenesis of TOPD remains unclear, there has been a growing focus on inflammation in its development. Multiple studies have highlighted tuberculosis as a factor independently elevating the risk of COPD onset, with a direct association with inflammatory levels.12–14 A study has shown that patients with TOPD have higher levels of IL-6 and CRP than those with smoking-associated COPD.2 Furthermore, concentrations of sIL-2R, IL-6, and TNF-α were found to be elevated in TB patients with COPD in comparison to TB patients without COPD.15
Recently, in addition to the commonly used systemic inflammatory biomarkers Erythrocyte Sedimentation Rate (ESR) and C-reactive Protein (CRP), attention has turned to novel markers such as the Systemic Inflammatory Response Index (SIRI), C-reactive Protein-to-Lymphocyte Ratio (CLR), and Eosinophil Count-to-Lymphocyte Count Ratio (ELR). These markers have been found to be related to numerous diseases, including metabolic disorders, and inflammatory diseases.16–18 TOPD may be associated with systemic inflammation,2,19,20 however, there is limited knowledge about systemic inflammatory markers and risk factors for TOPD. Thus, the purpose of this study was to evaluate the correlation between systemic inflammatory markers and patients with TOPD, to help understand the pathogenesis of TOPD and to aid clinicians in early identification of high-risk TOPD patients, and to carry out appropriate prevention and treatment measures in time to alleviate the social and economic burden of TOPD.
Materials and Methods
Patients and Study Design
This cross-sectional study recruited patients with TB from January 2014 to January 2022 at the Wuhan Jinyintan Hospital, Tongji Medical College of Huazhong University of Science and Technology. Considering that there are no diagnostic criteria for TOPD, referring to the Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) criteria3 and combining the definition of post-tuberculosis lung disease (PTLD),9 TOPD in the present study was defined as evidence of chronic airflow limitation attributable at least in part to previous pulmonary tuberculosis.
Participants meeting the following inclusion criteria were enrolled in this study: (1) All patients with positive mycobacterial tuberculosis cultures or/and Xpert MTB/RIF (previous or current); (2) patients in TOPD group with airflow limitation (post-bronchodilator spirometry with FEV1/FVC<70%) and without any history of COPD or asthma or chronic cough, expectoration and wheezing before diagnosis of tuberculosis. (3) no acute exacerbation. (4) Patients in the non-TOPD (NTOPD) group without COPD, chronic bronchitis, bronchiectasis, severe interstitial disease and other diseases that could lead to airflow obstruction. The exclusion criteria were as follows: (1) age <18 years old; (2) no information available; (3) extrapulmonary TB.
Data Collection
Baseline data, including demographic characteristics (age, sex and education level), history of treatment, smoking, resistance, complications (diabetes mellitus, hypertension) and routine laboratory parameters (leukocyte count, neutrophil count, serum albumin, C-reactive protein and erythrocyte sedimentation rate), were retrieved from the electronic medical record (EMR) system. Additionally, ratio inflammatory indicators, such as Systemic Inflammation Index (SII), Systemic Inflammatory Response Index (SIRI), neutrophils-to-lymphocyte ratio (NLR), monocyte count-to-lymphocyte count ratio (MLR), platelet count-to-lymphocyte count ratio (PLR), derived neutrophil-to-lymphocyte ratio (dNLR), C-reactive protein-to-serum albumin ratio (CAR), C-reactive protein to serum pre-albumin ratio (CPR), C-reactive protein-to-lymphocyte ratio (CLR), eosinophil count-to-lymphocyte count ratio (ELR), were calculated and included for subsequent analysis. The computing methods for these indicators are detailed in Supplementary Table 1.
Statistical Analysis
All statistical analyses were performed using SPSS version 26.0 and R software (version 4.2.3). Categorical variables were presented as frequencies and percentages and were analyzed using the Chi-square test and Fisher’s exact test. Meanwhile, continuous variables were presented as mean ± standard deviation (SD) or median (1st quartile, 3rd quartile) and compared by Student’s t-test or Mann–Whitney U-test based on data normality and distribution. Univariate and multivariable logistic regression analyses were executed to explore the relationship between influencing factors with the risk of the presence of TOPD. Receiver Operating Characteristic (ROC) curves were used to evaluate the diagnostic value of the novel inflammatory biomarkers selected by multivariate regression analysis, and patients were divided into four different groups according to their quartiles. The Chi-Square test was used to compare the incidence rate of TOPD in tuberculosis patients in subgroups of selected inflammatory biomarkers. The Jonckheere–Terpstra test was performed for trend analysis. In addition, 1:1 propensity score matching (PSM) was implemented using the nearest-neighbor method, with a caliper size of 0.02 to further identify the impact of selected inflammatory biomarkers on TOPD. The propensity score was computed using logistic regression analysis. P-value <0.05 based on a two-sided hypothesis was considered statistically significant.
Results
Clinical Data and Laboratory Indicators
A total of 737 patients were included in the present study, of whom 83 participants (11.26%) had TOPD. The baseline clinical and laboratory characteristics of participants are shown in Table 1 and Figure 1. Patients in the TOPD group exhibited a higher mean age compared to those in the NTOPD group (P<0.001). The proportion of males (P<0.001), people with low education levels (P<0.010), smokers (P<0.001) and patients with a history of irregular treatment (P=0.001) was significantly higher in the TOPD group compared to the NTOPD group. The levels of inflammatory indicators, including SII, SIRI, NLR, MLR, PLR, dNLR, CAR, CPR, CLR, ELR, ESR and CRP in TOPD group were significantly higher than those in NTOPD group (Figure 1A). No significant differences were observed in complications such as diabetes mellitus and hypertension (P>0.05).
 |
Table 1 The Baseline Demographic and Clinical Characteristics of Study Participants |
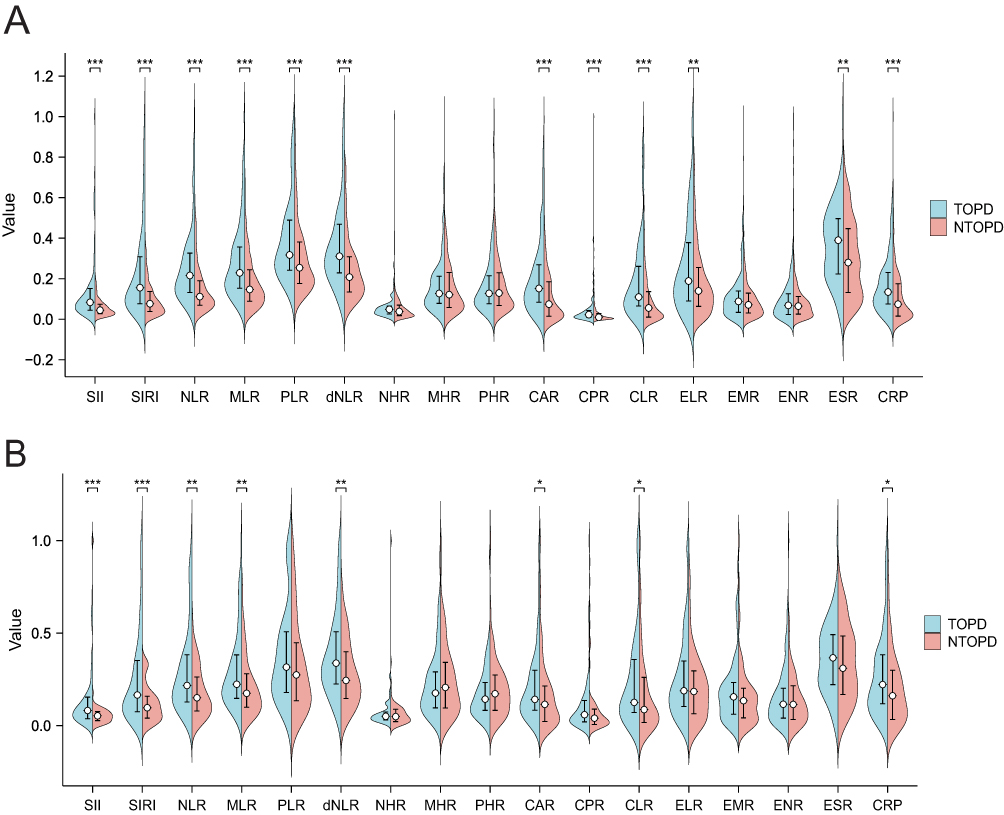 |
Figure 1 The comparison of inflammatory indicators between TOPD and NTOPD groups. (A) The comparison of 17 inflammatory indicators before PSM, where blue and red denote the TOPD and NTOPD groups, respectively. **P < 0.01 and ***P<0.001. (B) The comparison of 17 inflammatory indicators after PSM, where blue and red denote the TOPD and NTOPD groups, respectively. *P < 0.05, **P < 0.01 and ***P<0.001. Abbreviations: PSM, Propensity Score Matching; SII, Systemic Inflammation Index; SIRI, Systemic Inflammatory Response Index; NLR, Neutrophil count to lymphocyte count ratio; MLR, Monocyte count to lymphocyte count ratio; PLR, Platelet count to lymphocyte count ratio; dNLR, derived neutrophil-to-lymphocyte ratio; NHR, Neutrophil count to high-density lipoprotein ratio; MHR, Monocyte count to high-density lipoprotein ratio; PHR, Platelet count to high-density lipoprotein ratio; CAR, C-reactive protein to serum albumin ratio; CPR, C-reactive protein to serum pre-albumin ratio; CLR, C-reactive protein to lymphocyte count; ELR, Eosinophil count to lymphocyte count ratio; EMR, Eosinophil count to monocyte count ratio; ENR, Eosinophil count to neutrophil count ratio; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein. |
Age, gender, resistance, irregular treatment, educational level, smoking and complications were used as matching variables for PSM, and 69 TOPD patients and 69 NTOPD patients were successfully matched. After PSM, there was no significant difference in the above variables between the two groups (P>0.05) (Table 1). Furthermore, Figure 1B showed that SII, SIRI, NLR, MLR, dNLR, CAR, CLR, CRP remained significantly different between the TOPD group and NTOPD group, whereas PLR, CPR, ELR and ESR were not significantly different between the two groups after PSM.
Evaluation of the Impact of Inflammatory Indicators on TOPD
Before PSM, on univariate analysis, age, gender, irregular treatment, educational level, smoking, SII, SIRI, NLR, MLR PLR, dNLR, CAR, CLR, ELR, ESR, CRP were significantly associated with TOPD (P<0.01). Age, irregular treatment, SIRI, CLR and ELR were independent influencing factors of TOPD on multivariate analysis (P<0.01), as given in Table 2.
 |
Table 2 Univariate and Multivariate Logistic Analysis of Factors Associated with TOPD Before PSM |
To further explore the impact of inflammatory indicators on TOPD, univariate and multivariate Logistic Analysis were performed on significant factors (SII, SIRI, NLR, MLR, dNLR, CAR, CLR, CRP) after PSM (Table 3). The univariate logistic regression analysis showed that SII, SIRI, NLR, MLR, dNLR were significantly associated with TOPD (P<0.05). And SIRI remained independently significantly associated with an increased risk of TOPD on multivariable analysis. After adjusting for confounding factors, SIRI still showed significant statistical differences, indicating the robustness of SIRI as a predictor of TOPD in TB patients.
 |
Table 3 Univariate and Multivariate Logistic Analysis of Significant Factors Associated with TOPD After PSM |
ROC curve analysis was performed to assess the efficiency of inflammatory indicators. As shown in Figure 2, the AUC of SIRI, CLR and CRP were 0.702, 0.665 and 0.640 before PSM, whereas, their AUC were 0.668, 0.601 and 0.608 after PSM. The AUC of ELR and ESR were 0.596 and 0.607 before PSM, however, there was no significant difference in the diagnostic effect of ELR and ESR in predicting the outcome (P>0.05). SIRI was found to be superior in diagnosing TOPD than CLR and CRP before and after PSM. As shown in Supplementary Tables 2 and 3, the optimum truncation Value for SIRI to predict TOPD was 3.19 (sensitivity: 0.801, specificity: 0.506) and 3.38 (sensitivity: 0.783, specificity: 0.493) before and after PSM, respectively.
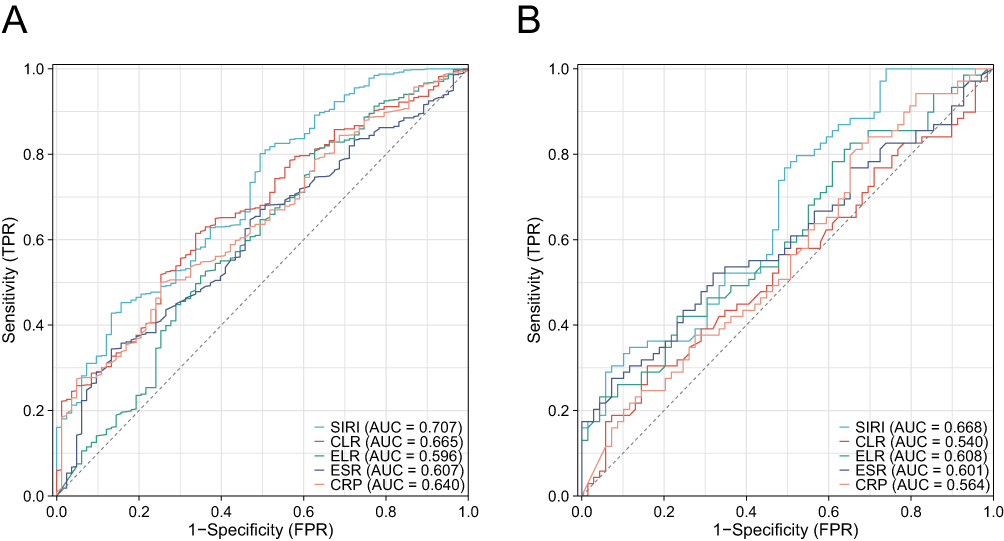 |
Figure 2 Receiver operating characteristic (ROC) curve analysis of SIRI, CLR, ELR, ESR and CRP before Propensity Score Matching (PSM) (A) and after PSM (B). Abbreviations: SIRI, Systemic Inflammatory Response Index; CLR, C-reactive protein to lymphocyte count; ELR, Eosinophil count to lymphocyte count ratio; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein. Note: There was no significant difference in the diagnostic effect of ELR and ESR in predicting the outcome after PSM (P>0.05). |
The Prevalence of TOPD Among Different Quartiles of SIRI
Patients were divided into four different groups based on the SIRI quartiles. As illustrated in Figure 3, the prevalence of TOPD among tuberculosis patients exhibited a rising trend corresponding to increasing SIRI values both before and after PSM and Jonckheere–Terpstra test showed that the trend was statistically significant (P<0.001), which suggested that tuberculosis patients with higher SIRI values are at greater risk of TOPD.
 |
Figure 3 The prevalence of TOPD patients among different quartiles of SIRI before Propensity Score Matching (PSM) (A) and after PSM (B). Abbreviation: SIRI, Systemic Inflammatory Response Index. |
Discussion
Although the exact mechanism of obstructive airways in post-TB patients remains unclear, the development of TOPD might be influenced by mechanisms of chronic inflammation. Several studies have indicated that the inflammatory response following tuberculosis infection drives leukocyte aggregation, tissue destruction and remodeling, forming lung tissue granulomas and lung cavities, leading to chronic airway obstruction and chronic inflammation.21,22 Previous studies demonstrated that inflammatory cytokines levels remained high and lung remodeling and chronic inflammatory response may persist after curing tuberculosis.23–25 Immunologic mechanisms may also be involved in subsequent systemic inflammation after treatment of tuberculosis.5,14,19 Additionally, pulmonary inflammation serves as root cause of systemic inflammation, as it can release cytokines such as TNF-a, IL-6, IL-8, etc. These pro-inflammatory mediators may be released into the systemic circulation when passing through the pulmonary circulation and contribute to the activation of systemic inflammatory cells.26 Therefore, systemic inflammatory markers can be used to predict TOPD to facilitate the early identification of high-risk TOPD patients, and enable the implementation of appropriate treatments to control the systemic inflammatory response of TOPD.
Leukocyte, platelets, high-density lipoproteins and albumin play roles in the inflammatory response, making their ratio crucial for the indirect assessment of inflammatory status.17,27–30 For example, NLR, PLR, dNLR, MLR, SII and SIRI are useful indicators of systemic inflammation and disease severity in psoriasis.31 MHR, NHR, CLR, and CAR could be used for assessing type 2 diabetes mellitus in active pulmonary tuberculosis.16 In the present study, we observed that the levels of SII, SIRI, NLR, MLR, dNLR, CAR, CLR and CRP in the TOPD group were higher than those in the NTOPD group before and after PSM, suggesting that TOPD patients have higher levels of inflammation than NTOPD patients. Univariate and multivariate logistic regression analysis before and after PSM showed an association between SIRI and TOPD. Moreover, we also found that age and irregular treatment were independent risk factors for TOPD, which is roughly the same as that reported in some previous studies.32,33 The results of multivariate regression of ELR and CLR before and after PSM in this study were different. A possible reason for this is that the single index of peripheral blood is easily affected by individual differences and confounding factors, and the composite index can better reflect the clinical status of TOPD patients than the single index. Additionally, when this study population was divided by SIRI quartiles, the prevalence of TOPD increased with the increase of SIRI level, indicating that TB patients with higher values of SIRI are more likely to be high-risk group for TOPD. In this study, we found that SIRI was elevated in TOPD patients, and SIRI had good predictive efficacy and robustness, which could help in understanding the inflammatory response involved in TOPD.
SIRI can reflect the state of neutrophils, lymphocytes and monocytes simultaneously, which more comprehensively reflects the inflammatory state and immune balance of the body than NLR or MLR alone. The possible reasons for the increase of SIRI in TOPD patients are that inflammation induces the increase of neutrophils,34 and COPD leads to abnormal respiration, which makes the tissues and organs in a hypoxic state, affects the development and maturation of immune cells, and the lymphocyte count gradually decreases.35 Furthermore, previous studies have shown that COPD and TB have different degrees of lymphocyte immune dysfunction.36,37 Alex Kayongo et al have described immune pathways potentially driving the immunopathogenesis of TOPD, involving interactions of neutrophils, monocyte-derived macrophages, and lymphocytes with airway epithelial cells, fibroblasts, and extracellular matrix, ultimately causing persistent lung inflammation, tissue necrosis, and airway remodeling.36
Nevertheless, the current study is not exempt from some limitations. Firstly, the present study was retrospective, there may have been some unavoidable bias in the study. Secondly, all enrolled patients were from a single center, which might limit the extrapolation of our findings to other regions. Therefore, future research will need to confirm and improve our conclusions through larger samples and multi-center prospective studies.
Conclusion
In conclusion, the levels of inflammatory indicators were higher in patients with TOPD than in those with NTOPD, and SIRI may be a simple and useful inflammatory index for assessing TOPD. Additionally, TB patients with higher values of SIRI are more likely to be high-risk group for TOPD. Therefore, TB patients could be monitored for systemic inflammation and much more attention should be paid to SIRI in the examination of TB to identify high-risk patients with TOPD early, and to carry out appropriate prevention and treatment measures in time to reduce the social and economic burden of TOPD.
Data Sharing Statement
The datasets used in this study can be obtained from the corresponding author upon request.
Ethics Statement
This study was conducted in adherence to the guidelines of Good Clinical Practice and the Declaration of Helsinki. The study protocol was reviewed and approved by the Ethics Committee of Wuhan Jinyintan Hospital (KY-2022-06.01).
Consent to Participate
The ethics committee of Wuhan Jinyintan Hospital waived the requirement for participant consent due to the retrospective nature of the study and the use of anonymized data.
Acknowledgments
We thank Jisong Yan for the support with data acquisition.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Soriano JB, Kendrick PJ, Paulson KR.; GBD Chronic Respiratory Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
2. Oh JY, Lee YS, Min KH, et al. Difference in systemic inflammation and predictors of acute exacerbation between smoking-associated COPD and tuberculosis-associated COPD. Int J Chron Obstruct Pulmon Dis. 2018;13:3381–3387. doi:10.2147/COPD.S177371
3. Agustí A, Celli BR, Criner GJ, et al. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Eur Respir J. 2023;61(4):2300239. doi:10.1183/13993003.00239-2023
4. Allwood BW, Gillespie R, Galperin-Aizenberg M, et al. Obstructive pulmonary disease in patients with previous tuberculosis: pathophysiology of a community-based cohort. South Afr Med J. 2017;107(5):440–445. doi:10.7196/SAMJ.2017.v107i5.12118
5. Alvarado González A. Tuberculosis Obstructive Pulmonary Disease (TOPD). Clin Res Trials. 2021;7(4). doi:10.15761/CRT.1000351
6. Lee SW, Kim YS, Kim DS, Oh YM, Lee SD. The risk of obstructive lung disease by previous pulmonary tuberculosis in a country with intermediate burden of tuberculosis. J Korean Med Sci. 2011;26(2):268–273. doi:10.3346/jkms.2011.26.2.268
7. Xing Z, Sun T, Janssens JP, et al. Airflow obstruction and small airway dysfunction following pulmonary tuberculosis: a cross-sectional survey. Thorax. 2023;78(3):274–280. doi:10.1136/thoraxjnl-2021-218345
8. World Health Organization. Global Tuberculosis Report 2023. World Health Organization; 2023. Available from: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2023.
9. Allwood BW, van der Zalm MM, Amaral AFS, et al. Post-tuberculosis lung health: perspectives from the First International Symposium. Int J Tuberc Lung Dis. 2020;24(8):820–828. doi:10.5588/ijtld.20.0067
10. Allwood BW, Gillespie R, Galperin-Aizenberg M, et al. Mechanism of airflow obstruction in Tuberculosis-Associated Obstructive Pulmonary Disease (TOPD). In:
11. Allwood BW, Rigby J, Griffith-Richards S, et al. Histologically confirmed tuberculosis-associated obstructive pulmonary disease. Int J Tuberc Lung Dis. 2019;23(5):552–554. doi:10.5588/ijtld.18.0722
12. Shahana MP, Mohanty Mohapatra M, Mahesh Babu V, Rajaram M, Rajaa S, Gandhipuram Periyasamy SK. Metabolic syndrome in post-pulmonary tuberculosis-associated obstructive airway disease: a cross-sectional analytical study. Cureus. 2022;14(3):e23640. doi:10.7759/cureus.23640
13. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/S0140-6736(22)00470-6
14. Jiang M, Pang N, Wang J, et al. Characteristics of serum autoantibody repertoire and immune subgroup variation of tuberculosis-associated obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2023;18:2867–2886. doi:10.2147/COPD.S434601
15. Tang S, Cui H, Yao L, et al. Increased cytokines response in patients with tuberculosis complicated with chronic obstructive pulmonary disease. PLoS One. 2013;8(4):e62385. doi:10.1371/journal.pone.0062385
16. Yu Q, Weng W, Luo H, Yan J, Zhao X. The novel predictive biomarkers for type 2 diabetes mellitus in active pulmonary tuberculosis patients. Infect Drug Resist. 2022;15:4529–4539. doi:10.2147/IDR.S377465
17. Jiang Y, Tu X, Liao X, et al. New inflammatory marker associated with disease activity in gouty arthritis: the systemic inflammatory response index. J Inflamm Res. 2023;16:5565–5573. doi:10.2147/JIR.S432898
18. Li J, Zhang X, Zhang Y, et al. Increased systemic immune-inflammation index was associated with type 2 diabetic peripheral neuropathy: a cross-sectional study in the Chinese Population. J Inflamm Res. 2023;16:6039–6053. doi:10.2147/JIR.S433843
19. Malefane L, Maarman G. Post-tuberculosis lung disease and inflammatory role players: can we characterise the myriad inflammatory pathways involved to gain a better understanding? Chem Biol Interact. 2024;387:110817. doi:10.1016/j.cbi.2023.110817
20. Kim DJ, Oh JY, Rhee CK, Park SJ, Shim JJ, Cho JY. Metabolic fingerprinting uncovers the distinction between the phenotypes of tuberculosis associated COPD and smoking-induced COPD. Front Med. 2021;8:619077. doi:10.3389/fmed.2021.619077
21. Ong CWM, Elkington PT, Friedland JS. Tuberculosis, pulmonary cavitation, and matrix metalloproteinases. Am J Respir Crit Care Med. 2014;190(1):9–18. doi:10.1164/rccm.201311-2106PP
22. Tian ZX. Progress in tuberculosis associated obstructive pulmonary disease. Mod J Integr Trad Chin Western Med. 2021. doi:10.3969/j.issn.1008-8849.2021.29.024
23. Ugarte-Gil CA, Elkington P, Gilman RH, et al. Induced Sputum MMP-1, −3 & −8 Concentrations during Treatment of Tuberculosis. PLoS One. 2013;8(4):e61333. doi:10.1371/journal.pone.0061333
24. Malherbe ST, Shenai S, Ronacher K, et al. Persisting PET-CT lesion activity and M. tuberculosis mRNA after pulmonary tuberculosis cure. Nat Med. 2016;22(10):1094–1100. doi:10.1038/nm.4177
25. Radovic M, Ristic L, Ciric Z, et al. Changes in respiratory function impairment following the treatment of severe pulmonary tuberculosis – limitations for the underlying COPD detection. Int J Chron Obstruct Pulmon Dis. 2016;11:1307–1316. doi:10.2147/COPD.S106875
26. van Eeden SF, Tan WC, Suwa T, et al. Cytokines involved in the systemic inflammatory response induced by exposure to particulate matter air pollutants (PM(10)). Am J Respir Crit Care Med. 2001;164(5):826–830. doi:10.1164/ajrccm.164.5.2010160
27. Thomas MR, Storey RF. The role of platelets in inflammation. Thromb Haemost. 2015;114(3):449–458. doi:10.1160/TH14-12-1067
28. Navab M, Anantharamaiah GM, Fogelman AM. The role of high-density lipoprotein in inflammation. Trends Cardiovasc Med. 2005;15(4):158–161. doi:10.1016/j.tcm.2005.05.008
29. Sheinenzon A, Shehadeh M, Michelis R, Shaoul E, Ronen O. Serum albumin levels and inflammation. Int J Biol Macromol. 2021;184:857–862. doi:10.1016/j.ijbiomac.2021.06.140
30. Islam MM, Satici MO, Eroglu SE. Unraveling the clinical significance and prognostic value of the neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, systemic immune-inflammation index, systemic inflammation response index, and delta neutrophil index: an extensive literature review. Turk J Emerg Med. 2024;24(1):8–19. doi:10.4103/tjem.tjem_198_23
31. Tiucă OM, Morariu SH, Mariean CR, Tiucă RA, Nicolescu AC, Cotoi OS. Impact of blood-count-derived inflammatory markers in psoriatic disease progression. Life. 2024;14(1):114. doi:10.3390/life14010114
32. Wei XU, Li-jua WU, Ning S, Wen—li. CAO. Progress in diagnosis and treatment in tuberculosis patients associated chronic obstructive pulmonary disease. J Tuberculosis Lung Health. 2017;6(3):5. doi:10.3969/j.issn.2095-3755.2017.03.017
33. Lee CH, Lee MC, Lin HH, et al. Pulmonary tuberculosis and delay in anti-tuberculous treatment are important risk factors for chronic obstructive pulmonary disease. PLoS One. 2012;7(5):e37978. doi:10.1371/journal.pone.0037978
34. Butler A, Walton GM, Sapey E. Neutrophilic inflammation in the pathogenesis of chronic obstructive pulmonary disease. COPD. 2018;15(4):392–404. doi:10.1080/15412555.2018.1476475
35. Dai S, Xiang Y, Pang Z, Pan H, Su Y, Zheng F. Correlation between neutrophil to lymphocyte ratio in peripheral blood and immune function in COPD patients. J Mod Clin Med. 2023;49(5):324–327. doi:10.11851/j.issn.1673-1557.2023.05.002
36. Nurwidya F, Damayanti T, Yunus F. The role of innate and adaptive immune cells in the immunopathogenesis of chronic obstructive pulmonary disease. Tuberc Respir Dis. 2016;79(1):5–13. doi:10.4046/trd.2016.79.1.5
37. Chen X, Bai M, Zhang Z, Wang X. Clinical significance of lymphocyte function determination in common lung diseases. J Pra Med. 2019;35(20):3204–3207. doi:10.3969/j.issn.1006-5725.2019.20.018
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.