")
Back to Journals » Patient Preference and Adherence » Volume 19
A Pilot Study of Virtual Reality in Hemodialysis for Mitigating Pain and Anxiety: User Experiences and Perceptions
Authors Rodríguez de Galvis S, Guerrero Rodríguez E, Audije-Gil J , Hernández SH , Argilés-Huguet M, Botella A , Burgos Villulas M , Casaux-Huertas A, González Sánchez I, Marín López MT , Manso P , Hernán D, Dapena F, Arenas Jiménez MD
Received 5 February 2025
Accepted for publication 28 June 2025
Published 17 July 2025 Volume 2025:19 Pages 2069—2079
DOI https://doi.org/10.2147/PPA.S517622
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Virtual reality in haemodialysis for mitigating pain and anxiety – Video abstract [517622]
Views: 40
Solmar Rodríguez de Galvis,1 Elena Guerrero Rodríguez,1 Julia Audije-Gil,1 Sandra Hernández Hernández,1 Marta Argilés-Huguet,2 Ana Botella,1 Marina Burgos Villulas,1 Ana Casaux-Huertas,1 Isabel González Sánchez,1 María Teresa Marín López,1 Paula Manso,1 David Hernán,1 Fabiola Dapena,1 María Dolores Arenas Jiménez1
1Unidad de Investigación, Fundación Renal Española, Madrid, 28003, Spain; 2CSMIJ Pirineu Sant Joan de Deu Terres, Lleida, Spain
Correspondence: Julia Audije-Gil, Unidad de Investigación, Fundación Renal Española, Calle de José Abascal, 42, 1°, Izq, Madrid, 28003, Spain, Tel +34 659613453, Email [email protected]
Background: Virtual reality (VR) helps control symptoms during procedures in chronic patients. This study analyzes VR’s effect on pain and anxiety in hemodialysis (HD) patients at two points: the vascular access puncture and disconnection.
Methods: A prospective, non-randomized, crossover, multicenter pilot study assessing pre- and post-intervention outcomes with VR headsets. The intervention group used VR for up to 13 sessions, around the puncture, and at the end of the session. Pain was measured with the Faces Pain Scale - Revised (FPS-R) and anxiety with the Visual Analogue Scale for Anxiety (VAS-A). Usability and patient satisfaction with VR were also evaluated.
Results: A total of 73 patients (66.2 ± 13.3 years, 67% men) were included. At the start, 8.2% declined to wear the VR headset. The average number of sessions with the headset was 6.5 ± 4.8, with 23.3% completing all 13 sessions. Pain during punctures significantly improved with VR (1.26 vs 0.97; p = 0.039), while anxiety improved non-significantly. Anxiety during disconnection slightly increased, but also not significantly. Patients with higher initial pain and anxiety levels during puncture and disconnection showed significant improvement, while those with lower initial levels worsened (p < 0.05 in all cases). The HD population showed varying levels of acceptance of VR.
Conclusion: VR headsets help reduce pain during punctures, especially in patients with more intense pain. The effect on anxiety reduction during punctures or at the end of the session is inconclusive, with better results in those with higher anxiety levels. VR acceptance in the HD population is variable.
Keywords: chronic kidney disease, dialysis, virtual reality immersion therapy, pain management, anxiety, psychological anticipation
Introduction
Patients with chronic kidney disease (CKD) undergoing hemodialysis (HD) treatment commonly experience pain and anxiety during sessions.1 Pain is a frequent physical symptom among HD patients,2 which the International Association for the Study of Pain (IASP) defines as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage”.3
According to the World Health Organization (WHO), pain is the most common reason for seeking medical attention.3 Alongside pain, the prevalence of anxiety among HD patients is high, around 40%, although one-third of those affected report mild symptoms.4,5 Nevertheless, it is a concerning health issue, as it impacts the social well-being of patients and negatively affects their perception of their quality of life. In addition, anxiety is a symptom associated with a higher rate of mortality and hospital admissions.6
The high prevalence of these symptoms of pain and anxiety is largely due to the fistula puncture and disconnection during the session. Most patients receiving HD treatment do so through an arteriovenous fistula (AVF). This is considered the safest vascular access, but it presents challenges, as it requires a double venous puncture that can be painful. The success of cannulation is crucial for the appropriate treatment execution.7,8 The importance of proper puncture performance is essential, as it not only determines the quality of dialysis but also represents a traumatic experience for patients, involving pain experienced repeatedly over time.9 Evidence of the significance of this symptom for HD patients is found in the study by Carrasco et al, published in 2019, which assessed overall patient satisfaction and highlighted pain control as the most decisive factor.4
In light of the above, improving the experience of pain and anxiety during AVF punctures is crucial. Technological advances, including virtual reality (VR), have led to significant improvements in healthcare. VR immerses users in a realistic digital environment10 and is increasingly used in medical settings to manage pain and psychological phobias during procedures.11–13 It is considered one of the most effective techniques for reducing pain and emotional distress.14,15
Recent studies have demonstrated in patients undergoing HD treatment that the use of VR headsets during AVF puncture can significantly reduce perceived pain, anxiety, and physiological stress markers, highlighting its potential as a safe, simple, and cost-effective non-pharmacological tool in hemodialysis care.16–18 However, further research is needed to deepen our understanding of patients’ pain and anxiety perceptions across multiple sessions, as well as adherence to VR use, their satisfaction over time, and the technique’s usability.
This study aims to examine the effect of VR on pain and anxiety perception during AVF punctures and on anxiety at the end of HD sessions. Using a crossover design in which each patient serves as their own control, this study reduces inter-individual variability. Additionally, it evaluates the techniques’ adherence, usability, and patient satisfaction in the medium term.
Methods
Study Design
This multicenter pilot study, conducted from April to December 2023, is a prospective, non-randomized, crossover study designed to assess pre- and post-intervention outcomes using VR headsets.
Study Population
All patients with AVF from three outpatient dialysis centers of Fundación Renal Española were invited to participate. Recruitment, conducted by the nursing staff and psychologists from the support care team, began in April 2023 and continued throughout the study, depending on the availability of VR headsets, as each intervention lasted about one month. Participation was offered to all patients willing to try VR, and those who signed informed consent were included. The inclusion criteria were: 1) more than 3 months on a chronic HD program; 2) patients who are dialyzed through an arteriovenous AVF that is not newly punctured (at least one month after the first puncture); 3) no psychiatric disorders, visual impairment, or history of epilepsy, vertigo, or dizziness.
Virtual Reality Headset and Intervention
The VR headset used included four Pico 4K VR headset (Pico Interactive, San Antonio, Texas, USA) and the WakeUp and Smile software (WakeUp and Smile, Alcobendas, Spain). The device included a built-in audio system, using tracking systems and physical movement, such as eye or head movements, to navigate a digitally created virtual world. It is a head-mounted static VR display that allows participants to change the content. Various realistic scenarios were presented, including random 360° videos: a classical music concert, the city of Paris, a beach, and other different contents, bringing the total to 20 different scenarios.
Methods
VR was used at two points during the HD session:
1) At the start of the session, 10 minutes before the AVF puncture, and continued for 10 minutes after.
2) At the end of the session, starting 30 minutes before the conclusion, and removed during disconnection.
Each patient participated in both the intervention and control conditions, serving as their own control. Four patients began with VR and the other four without; after 13 sessions, the groups switched conditions for another 13 sessions, totaling 26 sessions per patient. This allowed for approximately one month of treatment under each condition, as patients typically undergo hemodialysis three times per week. The impact of VR on pain perception and anxiety during puncture was evaluated using validated scales, as well as its effect on pre-disconnection anxiety at the end of the HD session.
Scales
Adherence to VR treatment was assessed by calculating the number of sessions completed with the VR headsets relative to the total of 13 sessions that could have been completed. The pain and anxiety measures consisted of patients’ subjective ratings on scales administered after the AVF puncture and at the end of the HD session. Pain was measured with the Faces Pain Scale - Revised (FPS-R),19 and anxiety with the validated visual analogue scale for anxiety (VAS-A).20
The first measure, the FPS-R (Faces Pain Scale–Revised), presents six faces ranging from “no pain” to “very much pain”, allowing patients to indicate their pain intensity. This scale is scored from 0 (no pain) to 10 (very much pain). Pain scores were recorded immediately after the punctures, with VR users reporting their ratings after removing the headset. The second measure, the VAS-A (Visual Analogue Scale for Anxiety), uses a 0 to 10 scale, where 0 indicates no perceived anxiety and 10 represents extreme anxiety. Anxiety levels were recorded immediately after the dialysis session, with patients using VR providing their scores after headset removal.
Usability and satisfaction were measured through patients’ subjective ratings at the end of the study after 13 sessions, or earlier if they dropped out. Usability was measured with the System Usability Scale (SUS)21. This scale consists of 10 items with responses on a 1-to-5 scale, where 1 indicates “strongly disagree” and 5 indicates “strongly agree”. It provides an overall usability score, is easy to administer, and is widely used for user interfaces and applications. For greater clarity in the presentation of the results, the SUS responses were grouped into three categories: disagree (1–2), intermediate (3), and agree (4–5).
Satisfaction was measured with the Client Satisfaction Questionnaire (CSQ-8) 22.This scale consists of 8 items that assess overall satisfaction, with responses scored from 1 to 4, where 1 represents the lowest rating and 4 represents the highest. For greater clarity in the presentation of the results, the CSQ-8 responses were grouped into two categories from worst rated (1–2) to best rated (3–4) (Figure 3B).
Statistical Analysis
The Shapiro–Wilk test was used to assess the normality of the distribution. Descriptive statistics, mean and standard deviation for quantitative variables, and percentages for qualitative variables are presented. Pearson’s chi-squared test was employed for analyzing qualitative data, while the t-test was utilized for quantitative data. Statistical significance was set at p≤0.05. Data were processed using Microsoft® Excel®, Version LTSC Standard 2021 (Redmond, WA: Microsoft Corp), and IBM SPSS Statistics for Windows, Version 29.0.2.0 (Armonk, NY: IBM Corp).
Ethics
The study has been approved by the Ethics Committee of Fundación Jiménez Díaz (EC132-22_FJD-FRIAT), and it complies with the international ethical guidelines of the Helsinki Declaration and its amendments (Fortaleza, Brazil, October 2013), the WHO recommendations, the code of ethics, and relevant Spanish legislation. The processing, communication, and transfer of personal data of all participants have been carried out in accordance with Organic Law 3/2018 of 5 December 2018 on the Protection of Personal Data and the Guarantee of Digital Rights, and Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of personal data.
Results
Recruitment and Adherence
Seventy-three of the 145 eligible HD patients with AVF, representing 50.3% of the eligible population, participated in the study. The mean age was 66.2 ± 13.4 years, 67.1% (49 patients) being male, and 27.4% (n = 20) had a diabetic etiology of CKD. The average number of years participants were on dialysis was 5.0 ± 6.17 (range 0.3–27.3). All patients were dialyzed on a thrice-weekly schedule, in four-hour sessions. All were dialyzed via AVF, and the puncture was performed with 15-gauge needles. There were no modifications to the hemodialysis technique throughout the study.
At the beginning of the study, 6 patients (8.2%) declined the use of VR glasses without completing any session (Figure 1A). The reasons for discontinuation were: 4 patients (5.5%) felt overwhelmed, 1 (1.4%) reported fear, and 1 (1.4%) expressed a lack of interest. Pain was evaluated in 62 patients with and without VR, while anxiety was assessed in 59 patients during connection and 57 during disconnection. All included participants used the VR headset at least during the first session (except for the six patients who declined participation at the beginning). However, some chose not to complete one or both of the pain and anxiety assessments. Additionally, some patients could not be evaluated pre- and post-VR due to discharge from the unit for reasons such as death, transplantation, or transfer. These factors account for the variation in sample size across outcomes.
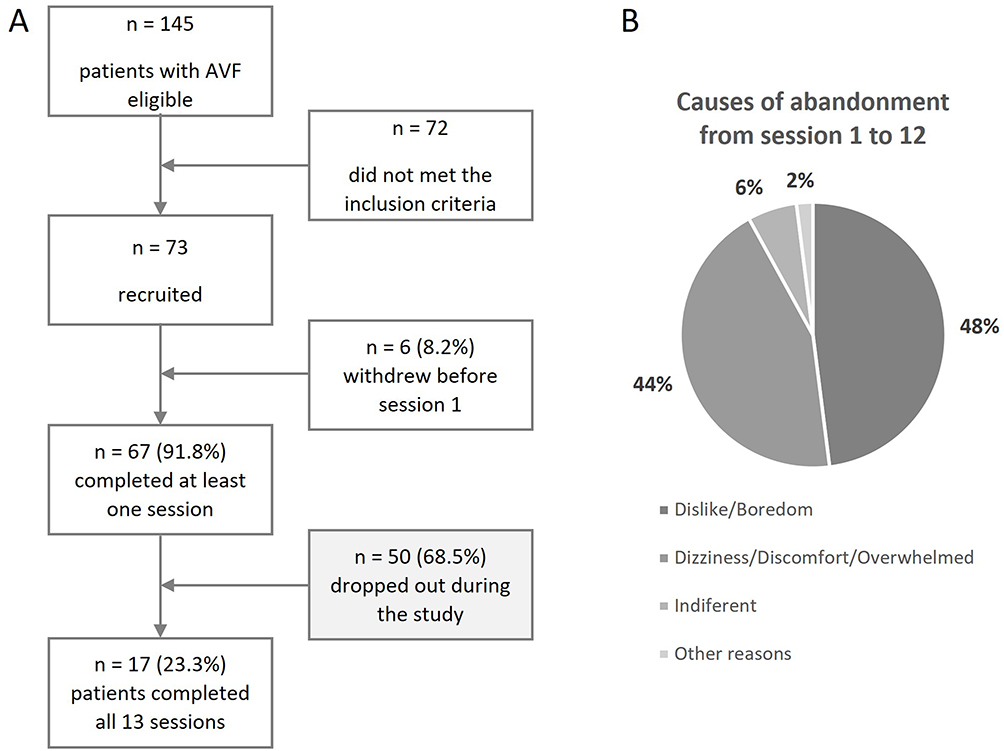 |
Figure 1 Adherence results and causes of abandonment. (A) Flowchart on the recruitment and adherence of the study. (B) Causes of abandonment in the 50 patients that dropped out from session 1 to 12. |
The average number of sessions completed by patients with the VR headset was 6.8 ± 4.8 sessions. Only 17 (23.3%) completed all 13 sessions (Figure 1B). The main reasons for dropout after at least one session up to session 12 were: dislike/boredom (n = 24; 48% of those that participated in at least one session), dizziness/discomfort/feeling overwhelmed (n = 22; 44%), indifference (n = 3; 6%), and others (n = 1; 2%). No significant differences were found in relation to age (p = 0.269), sex (p = 0.397), Charlson Comorbidity Index (p = 0.196), years on dialysis (p = 0.201), or HD session duration (p = 0.169) about discontinuation.
Pain and Anxiety Perception with VR
The impact of VR on pain intensity (n = 62) and anxiety at the time of the puncture (n = 59) was analyzed. Pain perception during the puncture improved significantly when patients wore the VR headset (pain score of 1.27 in patients without VR vs 0.98 in patients with VR; p=0.039) (Figure 2). For self-perceived anxiety associated with the puncture, a decrease in score was observed, but it was not statistically significant (1.08 vs 1.02; p=0.429).
 |
Figure 2 Change in pain and anxiety average score during puncture, and anxiety in the last half hour of dialysis, with and without virtual reality (VR) headsets. |
No significant differences were found in anxiety perception during disconnection (n = 57), but in this case, an increase in anxiety was observed compared to sessions without the VR headset (0.48 without VR Vs 0.83 with VR; p= 0.077) (Figure 2).
When stratifying patients into those who improved their score, showed no change, or worsened with the use of VR, significant differences were observed in pain and anxiety scores. Patients who improved their scores were those starting with higher levels of pain during connection (2.50 in those who improved vs 1.27 in those who worsened; p < 0.001), anxiety during connection (1.81 vs 0.39, p = 0.002), and anxiety during disconnection (1.54 vs 0.12, p < 0.001) (Table 1).
 |
Table 1 Number and Percentage of Patients Showing Improvement, No Change, or Worsening After VR, Along with Their Respective Sessions Completed and Scores. p-values in Bold Indicate Statistical Significance |
VR Usability and Satisfaction Analysis
System Usability Scale (SUS) responses (n = 58) grouped into three categories are shown in Figure 3A. The usability results for the VR device and software showed that most patients, 45 (77.6%), considered the application easy to use (question 3). Overall, all responses indicated a high level of usability (eg, question 7, where 79.3% of patients believed that most people would learn to use the application very quickly; or question 10, where 96.6% of patients thought that not much training was needed to use the application). However, less than half of the patients felt confident using the application (n = 28; 48.3%).
 |
Figure 3 VR usability and satisfaction analysis. (A) System Usability Scale (SUS) responses grouped in disagree (1–2), intermediate (3), and agree (4–5). (B) Patient Satisfaction Questionnaire (CSQ) responses grouped into two categories from worst rated (1–2) to best rated (3–4). Reproduced from Attkinson CC, Greenfield TK. 2004. The UCSF Client Satisfaction Scales: I. The Client Satisfaction Questionnaire-8. In ME Mauruish (Ed.), The use of phsicological testing for treatment planning and outcomes assessment (3rd Ed) (pp. 799-811). Volume 3. Mahwah, NJ: Lawrence Erlbaum Associates. © This survey uses items and item responses from the Client Satisfaction Questionnaire© by permission of the copyright holder. Copyright©2019. Clifford Attkisson, Ph.D. Use, transfer, copying, reproduction, merger, translation, modification, or enhancement (in any version, format, and/or media including electronic), in whole or in part, is forbidden without written permission by Dr. Attkisson. Contact: [email protected].22 |
Client Satisfaction Questionnaire (CSQ-8) © responses (n = 58) grouped into two categories are shown in Figure 3B. More than half of the patients reported being satisfied with the application (n = 38; 65.5%), would recommend it to a friend (n = 34; 58.6%), and deemed it to be of good quality (n = 30; 51.7%). However, the majority considered that it had not helped improve their well-being (n = 50; 86.2%), had not assisted them in dealing more effectively with their problems (n = 40; 69.0%), and were they satisfied with the amount of content it provided (n = 36; 62.1%).
Discussion
The study demonstrates the effectiveness of VR in reducing pain perception during AVF puncture at the start of the HD session. Although its impact on anticipatory anxiety was less pronounced, while anxiety during the puncture was reduced, there was an increase in anxiety experienced during the final half-hour of dialysis, both changes being statistically non-significant. Notably, patients with initially higher levels of pain and anxiety benefited most from VR, while those starting with lower levels tended to experience worsening symptoms. Especially relevant was the high number of patients who did not complete the 13 sessions with VR.
As in this study, other research has also demonstrated a reduction in pain associated with the use of VR in patients undergoing HD, as well as the recent study by Namazinia et al (2024)23 who demonstrated that the use of VR is effective in reducing pain during AVF puncture when compared with a control group. VR is a non-pharmacological pain relief method that helps reduce pain perception by diverting the patient’s attention. For example, in pediatric patients, its effectiveness has been proven in needle-related procedures, including venipuncture and catheter placement.24–26 In adults, VR distraction has also been demonstrated as an effective strategy for managing pain and/or anxiety in various procedures and treatments, including surgical or burn wounds,27,28 chemotherapy,29 emergency interventions,30 preoperative procedures,31 and other chronic or acute pain problems.32,33
In the case of patients undergoing HD, there is limited evidence regarding the efficacy, safety, and acceptability of VR in alleviating the symptoms associated with the dialysis session.34,35 In our study, VR was beneficial for pain management, particularly in patients who initially had higher levels of pain, as they benefited most from VR. However, those starting with lower pain levels tended to experience worsening symptoms. These findings suggest that VR should be adopted as a standard practice in HD, specifically for patients who experience higher levels of pain during puncture. Despite this, it is noteworthy that 77% of the patients in this study were unable to complete all 13 sessions with the VR headsets, the reasons for which will be discussed later in this section. However, the use of VR for other HD utilities such as implementing exercise programs during HD sessions, improving patients’ physical condition, and reducing fatigue, as well as symptoms of anxiety and depression36–38 has demonstrated its usefulness and its acceptability.
In the case of anxiety, the results are less conclusive. In our study, only those patients who had high levels of anxiety at the beginning of the puncture and half an hour before its completion showed benefits from the use of VR. This contrasts with other studies in HD patients, such as the one conducted by Hosseini et al (2024),35 where the VR intervention significantly reduced both state and trait anxiety compared to the control group.
The lack of knowledge about the procedure and poorly managed pain are often the main causes of peri-procedural anxiety.39 According to our results, at the time of puncture, VR appears to act as a distraction from both pain and anxiety, promoting relaxation, entertainment, and/or cognitive stimulation for patients. However, during disconnection, VR may not effectively distract from impatience or fatigue related to the anticipation of disconnection, especially in patients who initially have lower levels of anticipatory anxiety. In any case, given the high prevalence of anxiety in HD patients (with up to 30–60% of patients experiencing it35) and its impact on treatment adherence40 further research is needed to unravel whether VR should be applied at the end of the session or, conversely, only at the HD session beginning. In any case, high levels of pain or anxiety appear to be necessary for the benefits of the technique to outweigh the discomfort associated with using VR headsets.
Another key aspect to be explored is which type of VR and which content are most beneficial and best accepted by patients.41 In this study, the VR used displayed images of everyday life but did not require any action from the patients. It is likely that this type of content, combined with the lack of active participation, contributed to the high dropout rate (77%) and the absence of results in reducing anxiety at the time of disconnection, and even led to an increase in anxiety. Other studies have shown that the level of immersion in VR is important for the effectiveness in managing HD session symptoms.42 The more immersive the VR, the greater the analgesic effect.25,27,29,43,44 When the patient is fully immersed in the situation and feels as if they are part of the virtual world, it makes the experience more engaging. There are four types of VR commonly recognized:24 desktop VR (like computer video games), augmented VR (like road navigation systems), mixed VR (which combines real and virtual objects), and immersive VR. The latter can be passive (like in our study) or active (allowing the user to participate).
Thus, it is not simply a matter of whether or not to use VR, but also of making an appropriate choice regarding the type of VR employed. Ideally, active immersive VR, which requires greater user involvement, would enhance the potential for distraction, symptom improvement, and adherence. Notably, 48% of patients who dropped out after one session cited boredom or dissatisfaction with the videos as their reason for discontinuing.
In this regard, despite most patients reporting high usability of the VR (96.6% of patients thought that not much training was needed to use the application and 77.6% considered the application easy to use), the majority were not fully satisfied, as they did not find it beneficial for pain and anxiety management during routine HD sessions. It has been suggested that low digital literacy, possibly due to an average age (over 65) or lower educational levels, could contribute to this dissatisfaction.45 However, no significant age differences were found in our study, consistent with other research.46 In fact, 65.5% of patients reported a positive experience with the VR headsets, suggesting that age may not be a key factor. Thus, it seems that the unsatisfactory experience could be linked to the type of VR used. So that, further studies are needed to determine the optimal levels of immersion and interactivity required to achieve favorable outcomes.
Among the study limitations, one notable aspect was the large number of patients who failed to complete all 13 VR sessions, which needs to be further explored in future interventions. Also, the novelty effect may have contributed to the initial reduction in pain and anxiety, highlighting the need for longer follow-up and a larger sample size. Another factor was the aforementioned limited interactivity and content of the videos, which, along with discomfort, were key reasons for dropout. These issues may have affected the effectiveness of VR, particularly concerning anxiety symptoms. It should also be noted that symptoms such as dizziness or headaches are commonly experienced by HD patients, so future analysis should consider whether the source of this discomfort was the side effects of VR (known as cyberemesis) or those of dialysis.34
Despite those limitations, the results of this study are promising, emphasizing the need for further research into non-pharmacological, non-invasive, and cost-effective strategies to reduce pain and anxiety during HD AVF puncture and disconnection. VR could help improve psychological comfort, make the procedure less unpleasant, or even aid in training for fistula creation itself. Considering this, it should be examined whether the level of interaction with active immersive VR using more advanced special controllers improves the results.
Conclusions
VR has proven effective in reducing pain perception during AVF puncture at the start of HD sessions. However, its impact on anticipatory anxiety was less pronounced and conclusive: anxiety during puncture appeared to decrease, but anxiety experienced during the final half-hour of dialysis showed a clinically relevant, yet statistically non-significant increase. Notably, patients with initially higher levels of pain and anxiety benefited most from VR. Although most patients reported high usability, the majority were not fully satisfied, perceiving VR as not particularly beneficial for pain and anxiety management. Further studies are required to determine the optimal level of presence, immersion, and interactivity needed to achieve positive results, as well as to identify the patient group that benefits most from this technology.
Individual Contribution
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Acknowledgments
This research was funded by social project “Atención integral del paciente renal crónico en tratamiento de hemodiálisis” (MD22-00286) by Fundación la Caixa, and is supported by the Unidad de Investigación de la Fundación Renal Española. The authors wish to thank the supervisors, physicians, and technicians of the Fundación Renal Española for their assistance in data collection and the members of the Fundación Renal Working Group for their valuable collaboration.
Funding
This research was funded by social project “Atención integral del paciente renal crónico en tratamiento de hemodiálisis“ (MD22-00286) by Fundación la Caixa, and is supported by the Unidad de Investigación de la Fundación Renal Española.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Gutiérrez Sánchez D, Leiva-Santos JP, Macías López María J, Cuesta-Vargas AI. Prevalencia de síntomas en enfermedad renal crónica avanzada. Nefrologia. 2018;38(5):459–572. doi:10.1016/j.nefro.2017.11.019
2. Moreno Núñez E, Arenas Jiménez M D, Porta Bellmar E, et al. Study of the prevalence of anxious and depressive disorders in patients under haemodialysis. Rev Soc Esp Enferm Nefrol. 2004;7:1.
3. Raja SN, Carr DB, Cohen M, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982.PMID: 32694387; PMCID: PMC7680716. doi:10.1097/j.pain.0000000000001939
4. Carrasco MP, Edrm A, Palomo SV, Leiva MIL. Pain perception according to manner of arteriovenous fistula cannulation in patients undergoing hemodialysis. In: Systematic Review. Vol. 22. Enfermeria Nefrologica. Sociedad Espanola de Enfermeria Nefrologica; 2019:10–17.
5. Gómez Vilaseca L, Pac Gracia N, Traguany M, Lozano Ramírez S, Leonel J, Montesinos C. Prevalencia de ansiedad y depresión en pacientes de hemodiálisis. Enferm Nefrol. 2015;18:112–117.
6. Merino-Martínez RM, Morillo-Gallego N, Sánchez-Cabezas AM, Gómez-López VE, Crespo-Montero R. Relationship between health-related quality of life and anxiety / depression in patients on chronic hemodialysis. Enfermeria Nefrologica. 2019;22(3):274–283.
7. Blanco Mavillard I, Rodríguez Calero MÁ, Sánchez Rojas C. Evaluación de complicaciones de la fístula arteriovenosa para hemodiálisis según la técnica de canalización. Vol. 20. Enfermeria Nefrologica. Sociedad Espanola de Enfermeria Nefrologica; 2017:167–177.
8. Tovar-Muñoz L, Serrano-Navarro I, Mesa-Abad P, Crespo-Montero R, Ventura-Puertos P. “More than pain”: experiences of dialyzed patients regarding their puncture in hemodialysis. Enfermeria Nefrologica. 2020;23(1):34–43. doi:10.37551/S2254-28842020004
9. Granados Navarrete I, Abril Sabater D, Alcaraz Busqueta F, et al. Una actuación de enfermería. intentar aliviar el dolor en las punciones de hemodiálisis. Enfermería Nefrológica. 2005;8:231–236.
10. LaValle SM. Virtual Reality. Cambridge: Cambridge University Press; 2017:418.
11. Jerdan SW, Grindle M, van Woerden HC, Kamel Boulos MN. Head-mounted virtual reality and mental health: critical review of current research. JMIR Serious Games. 2018;6:e14. doi:10.2196/games.92267
12. Indovina P, Barone D, Gallo L, Chirico A, De Pietro G, Giordano A. Virtual reality as a distraction intervention to relieve pain and distress during medical procedures: a comprehensive literature review. Clin J Pain. 2018;34(9):858–877. doi:10.1097/AJP.0000000000000599
13. Dascal J, Reid M, IsHak WW, et al. Virtual reality and medical inpatients: a systematic review of randomized, controlled trials. Innov Clin Neurosci. 2017;14:14–21.
14. Windich-Biermeier A, Sjoberg I, Dale JC, Eshelman D, Guzzetta CE. Effects of distraction on pain, fear, and distress during venous port access and venipuncture in children and adolescents with cancer. J Pediatr Oncol Nurs. 2007;24(1):8–19. doi:10.1177/1043454206296018
15. Huguet A. Realidad virtual y manejo del dolor. 2007. Available from: https://www.researchgate.net/publication/28229388.
16. Elzeky ME, Salameh B, Reshia FAA, Sabry AA, Shahine NF, Mohamed EA. The effect of virtual reality distraction on haemodialysis patients’ pain and anxiety during arteriovenous fistula puncture: a randomised controlled trial. J Res Nurs. 2024;29(6):421–434. doi:10.1177/17449871241252005
17. Şen H, Lafcı Bakar D. The effect of virtual reality glasses on pain and patient satisfaction in arteriovenous fistula cannulation procedure. Appl Nurs Res. 2024;79:151841. doi:10.1016/j.apnr.2024.151841
18. Ersoy NA, Kesik G, Dede F. Effect of virtual reality video application on fistula puncture-associated pain in patients undergoing hemodialysis: assessor-blinded randomized trial. J Vasc Access. 2024;1:11297298241295447. doi:10.1177/11297298241295447
19. Thong ISK, Jensen MP, Miró J, Tan G. The validity of pain intensity measures: what do the NRS, VAS, VRS, and FPS-R measure? Scand J Pain. 2018;18(1):99–107.PMID: 29794282. doi:10.1515/sjpain-2018-0012
20. Abend R, Dan O, Maoz K, Raz S, Bar-Haim Y. Reliability, validity and sensitivity of a computerized visual analog scale measuring state anxiety. J Behav Ther Exp Psychiatry. 2014;45(4):447–453.Epub 2014 Jun 18. PMID: 24978117. doi:10.1016/j.jbtep.2014.06.004
21. Brooke J. SUS: a “quick and dirty” usability scale. In: Jordan PW, Thomas B, Weerdmeester B, McClelland IL, editors. Usability Evaluation in Industry. London: Taylor & Francis; 1996:189–194.
22. Attkisson CC, Greenfield TK. The UCSF Client Satisfaction Scales: I. The Client Satisfaction Questionnaire-8. In ME Mauruish (Ed.). The use of phsicological testing for treatment planning and outcomes assessment
23. Namazinia M, Mohajer S, Abbaspour S, Lopez V, Sarboozi-Hoseinabadi T. Effects of virtual reality on pain induced by arteriovenous fistula needle insertion in patients undergoing hemodialysis: a randomized clinical trial. J Vasc Access. 2024;7:11297298231225755. doi:10.1177/11297298231225755
24. Czech O, Wrzeciono A, Guzik A, Rutkowska A, Kiper P, Rutkowski S. Virtual reality interventions for needle-related procedural pain, fear and anxiety-a systematic review and meta-analysis. J Clin Med. 2021;10(15):3248.PMID: 34362032. doi:10.3390/jcm10153248
25. Atzori B, Vagnoli L, Graziani D, et al. An exploratory study on the effectiveness of virtual reality analgesia for children and adolescents with kidney diseases undergoing venipuncture. Int J Environ Res Public Health. 2022;19(4):2291. doi:10.3390/ijerph19042291
26. Gold JI, SooHoo M, Laikin AM, Lane AS, Klein MJ. Effect of an Immersive virtual reality intervention on pain and anxiety associated with peripheral intravenous catheter placement in the pediatric setting: a randomized clinical trial. JAMA Network Open. 2021;4(8):e2122569. doi:10.1001/jamanetworkopen.2021.22569
27. Chuan A, Zhou JJ, Hou RM, Stevens CJ, Bogdanovych A. Virtual reality for acute and chronic pain management in adult patients: a narrative review. Anaesthesia. 2021;76(5):695–704. doi:10.1111/anae.15202
28. Ko SY, Wong EM, Ngan TL, et al. Effects of virtual reality on anxiety and pain in adult patients undergoing wound-closure procedures: a pilot randomized controlled trial. Digit Health. 2024;10:20552076241250157. doi:10.1177/20552076241250157
29. Chow H, Hon J, Chua W, Chuan A. Effect of virtual reality therapy in reducing pain and anxiety for cancer-related medical procedures: a systematic narrative review. J Pain Symptom Manage. 2021;61(2):384–394. doi:10.1016/j.jpainsymman.2020.08.016
30. Birrenbach T, Bühlmann F, Exadaktylos AK, Hautz WE, Müller M, Sauter TC. Virtual reality for pain relief in the emergency room (VIPER) - a prospective, interventional feasibility study. BMC Emerg Med. 2022;22(1):113. doi:10.1186/s12873-022-00671-z
31. Chiu PL, Li H, Yap KY, Lam KC, Yip PR, Wong CL. Virtual reality-based intervention to reduce preoperative anxiety in adults undergoing elective surgery: a randomized clinical trial. JAMA Network Open. 2023;6(10):e2340588. doi:10.1001/jamanetworkopen.2023.40588
32. Wong KP, Tse MMY, Qin J. Effectiveness of virtual reality-based interventions for managing chronic pain on pain reduction, anxiety, depression and mood: a systematic review. Healthcare. 2022;10(10):2047. doi:10.3390/healthcare10102047
33. Slatman S, Staal JB, van Goor H, Ostelo R, Soer R, Knoop J. Limited use of virtual reality in primary care physiotherapy for patients with chronic pain. BMC Musculoskelet Disord. 2024;25(1):168. doi:10.1186/s12891-024-07285-5
34. Hernandez R, Burrows B, Mhem B, et al. Mindfulness-based virtual reality intervention in hemodialysis patients: a pilot study on end-user perceptions and safety. Kidney360. 2021;2(3):435–444. doi:10.34067/KID.0005522020
35. Hosseini T, Hooshmandja M, Noaparast M, Mojtahedzadeh R, Mohammadi A. Virtual reality exposure therapy to decrease anxiety before surgical invasive procedures in hemodialysis patients: an interventional study. BMC Nephrol. 2024;25(1):30. doi:10.1186/s12882-024-03461-w
36. Omonaiye O, Smyth W, Nagle C. Impact of virtual reality interventions on haemodialysis patients: a scoping review. J Ren Care. 2021;47(3):193–207.Epub 2021 Jan 24. PMID: 33491276. doi:10.1111/jorc.12362
37. Romeu-Perales M, Segura-Ortí E, Cana-Poyatos A, et al. The effect of intradialytic exercise using virtual reality on the body composition of patients with chronic kidney disease. Nutrients. 2024;16(12):1968. doi:10.3390/nu16121968
38. Turoń-Skrzypińska A, Tomska N, Mosiejczuk H, et al. Impact of virtual reality exercises on anxiety and depression in hemodialysis. Sci Rep. 2023;13(1):12435. doi:10.1038/s41598-023-39709-y
39. Bashir Z, Misquith C, Has P, Bukhari S. Effectiveness of virtual reality on anxiety and pain management in patients undergoing cardiac procedures: a protocol for systematic review and meta-analysis. Open Heart. 2023;10(1):e002305. doi:10.1136/openhrt-2023-002305
40. Burrai F, Othman S, Brioni E, et al. Effects of virtual reality in patients undergoing dialysis: study protocol. Holist Nurs Pract. 2019;33(6):327–337. doi:10.1097/HNP.0000000000000330
41. Yamashita Y, Aijima R, Danjo A. Clinical effects of different virtual reality presentation content on anxiety and pain: a randomized controlled trial. Sci Rep. 2023;13(1):20487. doi:10.1038/s41598-023-47764-8
42. Gurz D, Coimbatore Dada K, Naga Nyshita V, et al. The impact of virtual reality (VR) gaming and casual/social gaming on the quality of life, depression, and dialysis tolerance in patients with chronic kidney disease: a narrative review. Cureus. 2023;15(9):e44904. doi:10.7759/cureus.44904
43. Tesarz J, Herpel C, Meischner M, et al. Effects of virtual reality on psychophysical measures of pain: superiority to imagination and nonimmersive conditions. Pain. 2024;165(4):796–810. doi:10.1097/j.pain.0000000000003083
44. Guenther M, Görlich D, Bernhardt F, et al. Virtual reality reduces pain in palliative care-A feasibility trial. BMC Palliat Care. 2022;21(1):169. doi:10.1186/s12904-022-01058-4
45. Dy M, Olazo K, Lisker S, et al. Virtual Reality for Chronic Pain Management Among Historically Marginalized Populations: systematic Review of Usability Studies. J Med Internet Res. 2023;25:e40044. doi:10.2196/40044
46. Teh JJ, Pascoe DJ, Hafeji S, et al. Efficacy of virtual reality for pain relief in medical procedures: a systematic review and meta-analysis. BMC Med. 2024;22(1):64. doi:10.1186/s12916-024-03266-6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Exploring the Agreement Between Self-Reported Medication Adherence and Pharmacy Refill-Based Measures in Patients with Kidney Disease
Murali KM, Mullan J, Roodenrys S, Cheikh Hassan HI, Lonergan MA
Patient Preference and Adherence 2022, 16:3465-3477
Published Date: 30 December 2022
Determinants of Anemia Among Patients with Chronic Kidney Disease: A Systematic Review of Empirical Evidence
Prapaiwong P, Ruksakulpiwat S, Jariyasakulwong P, Kasetkala P, Puwarawuttipanit W, Pongsuwun K
Journal of Multidisciplinary Healthcare 2025, 18:3765-3780
Published Date: 28 June 2025