")
Back to Journals » Journal of Inflammation Research » Volume 17
A Population-Based Study of the Mediating Role of WBC, NEUT and PLT in the Relationship Between Triglyceride-Glucose Index and Urinary Albumin Excretion
Authors Sun X, Zhu J, Qian Z, Chen X, Zhang J, Ji C, Zhao L
Received 15 August 2024
Accepted for publication 26 November 2024
Published 7 December 2024 Volume 2024:17 Pages 10613—10626
DOI https://doi.org/10.2147/JIR.S491694
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Xu Sun,1– 3 Jun Zhu,2,3 Zhuyin Qian,4 Xiaowei Chen,5 Jie Zhang,6 Cheng Ji,7,* Li Zhao1,*
1China Pharmaceutical University, Nanjing, 211198, People’s Republic of China; 2Department of Pharmacy, Nanjing Luhe People’s Hospital, Nanjing, 211500, People’s Republic of China; 3Department of Pharmacy, Nanjing Luhe People’s Hospital, Yangzhou University, Nanjing, 211500, People’s Republic of China; 4Department of General Surgery, Nanjing Luhe People’s Hospital, Yangzhou University, Nanjing, 211500, People’s Republic of China; 5Department of Central Laboratory, Nanjing Luhe People’s Hospital, Yangzhou University, Nanjing, 211500, People’s Republic of China; 6Department of Endocrinology, Nanjing Luhe People’s Hospital, Yangzhou University, Nanjing, 211500, People’s Republic of China; 7Department of Pharmacy, Drum Tower Hospital Affiliated to Nanjing University Medical School, Nanjing, Jiangsu, 210000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Cheng Ji; Li Zhao, Email [email protected]; [email protected]
Aim: To assess the potential association between the TyG index and the risk of abnormal UACR. Additionally, we aimed to determine the role and degree of influence of inflammatory biomarkers between the TyG index and abnormal UACR.
Materials and Methods: A cross-sectional study recruited 1021 participants from a health management center between 2021 and 2022. Logistic or linear regression models, as well as mediation analysis, were employed to investigate the associations between the TyG index, inflammatory biomarkers (total and differential white blood cell counts, platelet, mean platelet volume(MPV), C-reactive protein(CRP)), and the risk of abnormal UACR.
Results: The study included 1021 participants, of whom 55.0% were men. The median age (interquartile range [IQR]) was 61.0 (53, 70) years. In multivariable-adjusted logistic regression models, both with and without the inclusion of smoking, alcohol drinking, BMI, Lipid-lowering drugs using, TC, SUA, ALT, and AST as potential covariates, the TyG index was associated with the risk of UACR, both with the odds ratios (ORs) per 1-standard deviation (SD) increase were 1.32 (95% CI, 1.08– 1.62) and 1.27 (95% CI, 1.05– 1.52), respectively. This study also demonstrated a significant indirect effect of the TyG index on the risk of abnormal UACR through total white blood cell counts, neutrophil counts and platelet (P values < 0.05); The proportions mediated was 11.2%, 3.5% and 29.6% for each respective variable.
Conclusion: Insulin resistance and inflammation are associated with an increased risk of kidney insufficiency. And indicators of inflammation weakly mediate insulin resistance and risk of kidney insufficiency.
Keywords: TyG index, urinary albumin-to-creatinine ratio, UACR, white blood cell counts, systemic inflammation, neutrophil counts, platelet
Introduction
Chronic kidney disease (CKD) is a progressive condition that affects more than 10% of the global population.1 It is particularly prevalent in patients with diabetes mellitus (DM), making early prevention and treatment of CKD essential. Urinary albumin excretion is widely recognized as an early clinical sign of diabetic nephropathy and is considered the most sensitive and reliable diagnostic indicator of early diabetic nephropathy,2 as well as an independent predictor of cardiovascular risk.3 The urinary albumin-to-creatinine ratio (UACR) is widely used in clinical practice as a crucial screening test for diabetic kidney disease (DKD) and diabetic cardiovascular events4 with UACR levels above 30 mg/g (3.4 mg/mmol) considered abnormal. Albuminuria is highly prevalent in hypertensive, diabetic, and obese populations, contributing to adverse clinical outcomes and presenting a significant public health challenge.
Studies have indicated a close association between insulin resistance (IR) and proteinuria and CKD.5–8 However, assessing insulin sensitivity based on the gold standard hyperinsulin-glucose clamp test is cumbersome, and the triglyceride-glucose (TyG) index has been found to be a simpler, easier, and more reliable assessment of IR, calculated as the logarithmic product of fasting triglyceride (TG, mg/dL) and fasting plasma glucose (FPG, mg/dL) levels.9 While several studies have explored the relationship between TyG index and proteinuria and CKD in diabetic populations,1,8,10,11 the correlation between the TyG index and proteinuria in the general healthy population and the mechanisms behind both TyG and proteinuria occurrence remain unclear.
Insulin resistance is itself a chronic, low-grade inflammatory state,7 thought to play a causative role in several other inflammatory diseases, including acute pancreatitis (AP).12 Numerous studies have demonstrated the association of inflammation with kidney damage, with inflammation contributing to the decline of renal function. For example, C-reactive protein (CRP) has been found to accelerate the decline of glomerular filtration rate (eGFR) and the development of CKD. Additionally, CRP, TNF-αR2, leukocyte counts, and IL-6 have been associated with the prognosis of CKD, indicating that chronic inflammation plays a key role in CKD progression.13,14 While inflammation levels have been linked to both insulin resistance and renal damage, the involvement of inflammation in the correlation between insulin resistance and proteinuria, as well as the mechanisms contributing to CKD development, remain unclear.
To our knowledge, limited research has been conducted on the link between the TyG index and the risk of urinary protein, particularly among the general healthy population. Furthermore, the mechanism by which insulin resistance contributes to the occurrence of urinary protein remains unclear. Therefore, the objective of this study was to examine the association between the TyG index and the risk of urinary protein in Chinese adults using a retrospective cohort study involving the general population. Additionally, we aimed to investigate whether this association is influenced by inflammatory biomarkers, thus offering crucial insights into the biological mechanisms connecting the TyG index to chronic kidney disease (CKD). Furthermore, we aimed to quantify these associations and calculate the proportions mediated through the TyG index to elucidate the precise role of inflammation in the development of the TyG index and the risk of urinary protein.
Materials and Methods
Study Participants
A cross-sectional study was conducted at the health management center of Luhe People’s Hospital in Nanjing City, China, from January 2021 to December 2022. The study participants were individuals from the general population in Luhe District of Nanjing City who voluntarily underwent an annual health examination at the study hospital. The exclusion criteria for participants in our analysis were as follows: (1) being under 18 years old, (2) being pregnant, and (3) having incomplete data on UACR, TG, FBG, total and differential WBC counts, platelet, MPV, and CRP. A total of 1806 participants aged above 18 years who underwent urinary microalbumin measurements were eligible for this study. Participants with missing information on UACR (n=197), FBG (n=51), total WBC counts (n=59), basophil counts (n=15), or eosinophil counts (n=9) were excluded. After that, participants were further excluded if they had incomplete data on total cholesterol (TC) (n=83), triglycerides (n=68), alanine transaminase (ALT) (n=25), aspartate transaminase (AST) (n=21), serum creatinine (Scr) (n=27), hypertension (n=123), or body mass index (BMI) (n=117). As a result, 1021 participants aged 18–82 years were included in the final analysis. The present study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and was approved by the ethics committee of Nanjing Luhe People’s Hospital, Yangzhou University Medical College. Informed consent was obtained from all participants prior to their inclusion in the study.
Data Definitions
Assessment of the TyG index: The TyG index was calculated using the formula ln [TG (mg/dL) × FBG (mg/dL) / 2]. Fasting blood glucose (FBG) and triglyceride (TG) levels were measured using the hexokinase / glucose-6-phosphate dehydrogenase method and the enzymatic colorimetric method, respectively. The TG and FBG units were converted from mmol/L to mg/dL before calculation (1 mmol/L = 88.57 mg/dL for TG, 1 mmol/L = 18 mg/dL for FBG).15 TyG index-BMI = TyG index × BMI. The TyG index and TyG index-BMI were divided into quartiles for sensitivity analysis.
Assessment of increased urinary albumin excretion: Urinary albumin-to-creatinine ratio (UACR) was calculated by dividing the urinary albumin concentration in milligrams by the urinary creatinine concentration in grams. Increased urinary albumin excretion (albuminuria) was defined as ACR >30 mg/g16 and was treated as an outcome variable in our analysis. Chronic kidney disease (CKD) was defined as an estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2 and/or microalbuminuria ≥30 mg/g creatinine. eGFR was evaluated using the modification of diet in renal disease (MDRD) equation. The creatinine was determined using the Jaffe technique,17 and albuminuria was determined through turbidimetric immunoassay. Blood and urine samples were collected from participants at a standardized mobile examination center.
Definition of systemic immune-inflammation or low-grade inflammation: The differential WBCs included neutrophils, lymphocytes, monocytes, eosinophils, and basophils in the present study. Total and differential white blood cell (WBC) counts, platelet and mean platelet volume (MPV) were measured using the Coulter DxH 800 analyzer.18 C-reactive protein (CRP) levels were measured using radioimmunoassay kits (Kamiya Biomedical Corp). Total and differential WBC counts, platelet, MPV and CRP were considered exposure variables in our analysis.
Assessment of Covariates
Covariates that may affect the association between the TyG index and albuminuria were also included in the current study were gender (male/female), age (in years), smoking status (yes/no), alcohol drinking (yes/no), body mass index (BMI, in kg/m2), lipid-lowering drugs using(yes/no), waist circumference (in cm), hypertension (yes/no), diabetes (yes/no), non-alcoholic fatty liver disease (NAFLD, yes/no), serum uric acid (SUA, in μmol/L), total cholesterol (in mmol/L), high-density lipoprotein-cholesterol (HDL-C), low-density lipoprotein-cholesterol (LDL-C), alanine transaminase (ALT, in IU/L), aspartate transaminase (AST, in IU/L), and estimated glomerular filtration rate (eGFR, in mL/min/1.73m2). Blood pressures and blood sugar were measured by trained nurses following standard measuring procedures. BMI was calculated as weight in kilograms divided by the square of height in meters. Hypertension was defined as meeting any of the following criteria: systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg, self-reported physician diagnosis of hypertension, or use of antihypertensive medication. The concentrations of biochemical variables, including TC, TG, SUA, Scr, AST and ALT, were measured using an automated analyzer (Cobas 8000; Roche Diagnostics, Basel, Switzerland).
Statistical Analysis
Categorical variables were described as percentages, while continuous variables were reported as mean ± SD for normally distributed data or median (interquartile range) for skewed data. Pearson’s χ2 test was employed to assess the association between two categorical variables. The Kruskal–Wallis rank sum test was used to determine if there were significant differences in the dependent variable across the categories of the independent variable. Fisher’s exact test was utilized when the sample size was small or when the assumptions of the chi-squared test were violated. Odds ratios (ORs) and 95% confidence interval (95% CI) for evaluating the associations of TyG with the risk of abnormal UACR were calculated using multivariate logistic regression model. Model 1 was adjusted for age and sex. Model 2 was adjusted for age, sex, smoking, alcohol drinking, BMI, lipid-lowering drugs using TC, SUA, ALT, and AST. Model 3 was further adjusted for hypertension. A test for linear trend was conducted with the use of quartile of the TyG variable as a continuous variable by assigning the median values of the quartile to the variable. The mediation analyses of low-grade inflammatory biomarkers(total WBC counts, differential WBC counts, platelet, MPV and CRP) in the association between TyG and UACR were performed using an available R package named “mediation”19 and a probit regression model. The mediation analyses estimated the direct effect of the TyG index on UACR risk after controlling confounders, the indirect effect of TyG on UACR risk through low-grade inflammatory biomarkers. We did subgroup analyses by age(<60 and ≥60 years) at cohort entry and BMI(<24 and ≥24Kg/m2), the likelihood ratio test was used for the interaction test. We also did a sensitivity analysis, the derived TyG index-BMI of TyG and UACR, to increase the reliability of our conclusion. The R software (version 4.2.2) was used for the analyses in the current study, and a level of P < 0.05 was considered statistically significant.
Results
Characteristics of the Study Participants
The analyzed cohort of the 1021 participants finally included, 561 (55.0%) were men and 460 (45.0%) were women. The median age (IQR) was 61.0 (53, 70) years. Stratification of participant characteristics by TyG index quartiles showed that the TyG index was associated with younger age, BMI, lipid-lowering drugs using, SUA (serum uric acid), TC, ALT, CRP, WBC counts, and lymphocyte counts (all P < 0.001). Participants with a higher TyG index were more likely to be younger and obese, compared with participants in the lowest quartile. Additionally, significant differences in Biochemical indicators were observed between the groups, with participants in the highest quartile showing significantly higher levels of lipid-lowering drugs using, SUA, TC, ALT, Ca, CRP, WBC counts, Lymphocyte count, NAFLD, compared with those in the first quartile (Table 1).
 |
Table 1 Participant Characteristics |
Association of TyG Index with Abnormal UACR Risk
We constructed three Cox regression models to investigate the association between TyG index levels and abnormal UACR risk presented in Table 2. Higher TyG index levels was associated with a higher risk of abnormal UACR risk when adjusting for age and sex (OR=1.64; 95% CI: 1.00, 2.69; P for trend=0.050). After further adjustment for smoking, alcohol drinking, BMI, lipid-lowering drugs using, TC, SUA, ALT and AST (OR=1.72; 95% CI: 1.02, 2.91; P for trend=0.045) in the highest quartile of TyG index compared with the lowest. However, further adjusting for hypertension attenuated this association to a certain extent (OR=1.74; 95% CI: 1.03, 2.94; P for trend=0.046).
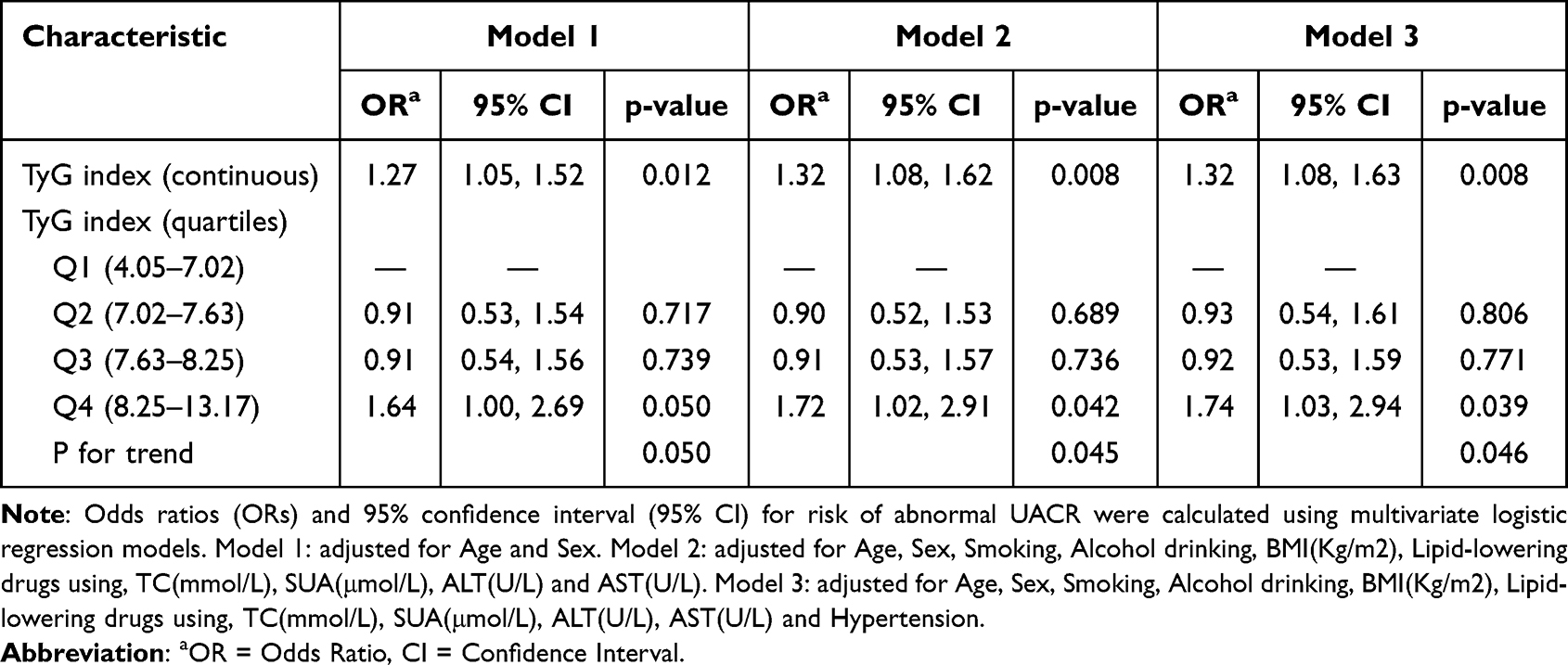 |
Table 2 Risk of Abnormal UACR by TyG Index |
Table 3 presents an indirect effect on abnormal UACR risk through total WBC counts, neutrophil counts and platelet (P values < 0.05). The proportions mediated by these three biomarkers for the TyG index-associated risk of abnormal UACR were 11.2%, 3.5% and 29.6%, respectively.
 |
Table 3 Mediation of Various Factors for the Associations Between TyG Index and Risk of UACR Groups |
Subgroup Analyses and Sensitivity Analyses
The results of subgroup analyses were presented in Figure 1 and Table 4. Age influences the association between TyG index and abnormal UACR risk, within which associations were observed among those younger(< 60 years) (P for interaction=0.024).
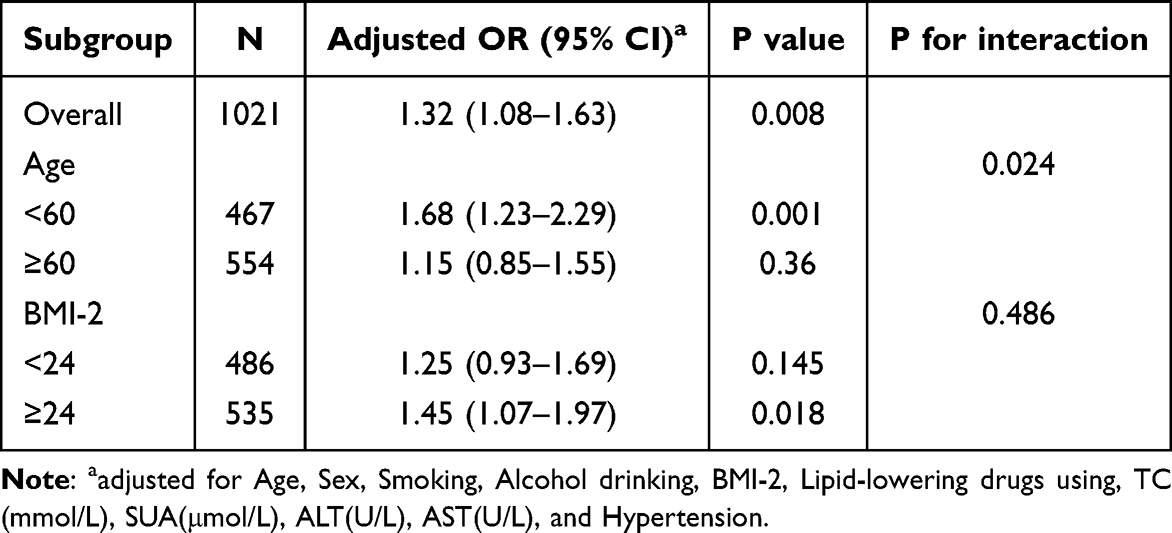 |
Table 4 Association Analysis of TyG Index with Risk of Abnormal UACR in Different Subgroups |
 |
Figure 1 Forest plots of subgroup analyses for the association of TyG with abnormal UACR risk. Note: * adjusted for Age, Sex, Smoking, Alcohol drinking, BMI, Lipid-lowering drugs using, TC(mmol/L), SUA(μmol/L), ALT(U/L), AST(U/L), and Hypertension. |
In sensitivity analyses, results were consistent when using the derived TyG index-BMI of TyG, and had no substantial influence on the primary findings(Table 5 and Table 6).
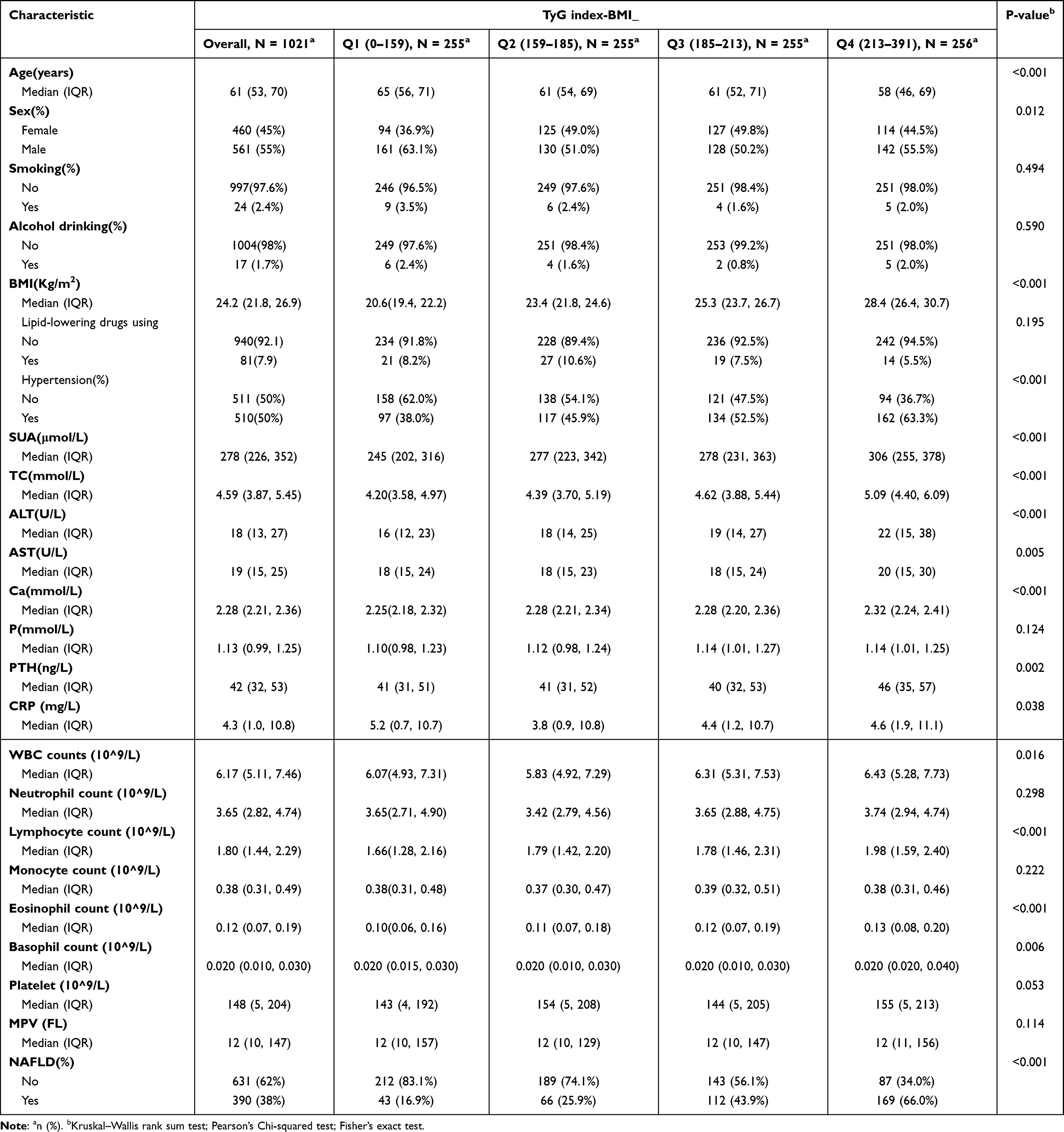 |
Table 5 Patient Demographics and Baseline Characteristics |
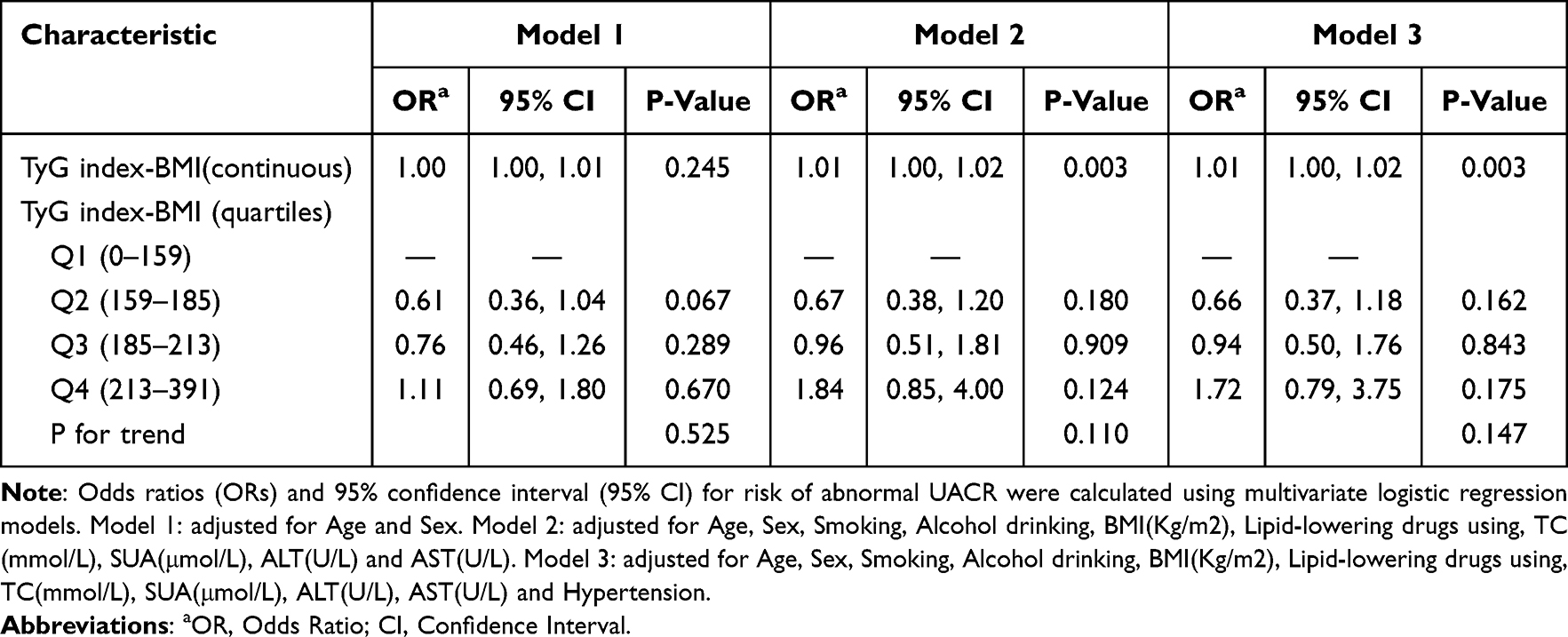 |
Table 6 Association Between TyG Index-BMI and UACR |
Discussion
In this cross-sectional study, we found a significant positive association between the TyG index and the risk of abnormal UACR after adjusting for potential confounders. At the same time, we observed that the inflammatory biomarkers, total WBC counts and neutrophil counts, were independently associated with an increased risk of abnormal UACR. Moreover, WBC counts and neutrophil counts mediate the approximately 10.0% (11.2%) and 3.0% (3.5%), platelet was about 30% of the total association between the TyG index and the risk of abnormal UACR risk, respectively, However, The mediating role of WBC counts and neutrophil counts is weak.
Insulin resistance has been shown to increase urinary albumin excretion,10 which is considered a risk factor for CKD.20 The TyG index, as an alternative to IR, is more convenient and practical for clinical use. Several studies have demonstrated a correlation between the TyG index and urinary protein excretion or CKD.6 Making it a valuable tool for tracking insulin resistance in clinical settings. Research in T2DM populations has further validated the significant association between the TyG index in T2DM patients, urinary protein8 and risk of ESRD progression.21 However, most studies on the relationship between the TyG index and urinary protein have been based on diabetic populations, there have been fewer analyses in nondiabetic patients. A prospective cohort study by Josef Fritz and their team on 176,420 Austrian adults over a mean of 22.7 years concluded its potential use in identifying individuals at risk for ESRD.22 The study also suggested that the TyG index plays an important mediating role in the relationship between body mass index (BMI) and ESRD. In a cross-sectional analysis of 982 non-diabetic patients, insulin resistance was found to be significantly associated with microalbuminuria.9 However, a study by Hoorn et al did not find an association between insulin resistance and microalbuminuria in a general elderly population of 622.23 The inconsistency of these findings in the general population makes our study more necessary. Our observation of a significant correlation between the TyG index and urine albumin-to-creatinine ratio (UACR) in the general population provides a theoretical basis for contradictory arguments.
Interestingly, Qing Zhu et al6 found a nonlinear relationship between the TyG index and CKD, as well as estimated glomerular filtration rate (eGFR) abnormalities, with a U-shaped curve. The gradual increase of the TyG level was shown to decrease the risk of CKD and eGFR abnormalities at first, and then increase until the TyG index reached around 8.94, after which it began to rise rapidly. While our study did not show these data, we found a different finding that there is a linear relationship between the TyG index and abnormal UACR levels. Patients with higher TyG levels, especially > 8.25, have an increased risk of abnormal UACR, which provides options for early intervention to prevent proteinuria. Therefore, monitoring the TyG index can be considered to take the necessary preventive measures to slow down the progression of CKD.
The mechanisms by which insulin resistance promotes the onset and progression of CKD are still being explored. Current research suggests that insulin resistance affects the viability of podocytes, which is considered to be the first step in the development of proteinuria. Additionally, insulin resistance of the podocytes increases podocyte death and disrupts insulin signaling, leading to a failure to maintain the integrity of the glomerular filtration barrier.24 Furthermore, excess insulinemia increases sodium reabsorption and induces glomerular filtration, affecting renal hemodynamic deterioration, and promoting glomerular tunica dilatosa and tubulointerstitial fibrosis.25,26 Finally, insulin resistance increases the risk of developing metabolic diseases such as hypertension, hyperglycemia, hyperuricemia, and hyperlipidemia.27 While multiple neurohumoral, metabolic, and hemodynamic factors have been associated with renal disease, the exact mechanisms remain incompletely understood. However, our findings show that systemic inflammatory indicators play an important mediating role in insulin resistance and urinary microalbumin, providing innovative theoretical support to elucidate the mechanisms mediating the association of insulin resistance and proteinuria, as well as the progression of CKD.
Insulin resistance is associated with chronic low-grade inflammation, and total white blood cell (WBC) count is often used as a marker of low-grade inflammation in the assessment of inflammatory and metabolic-related diseases.28 People with insulin resistance and impaired glucose metabolism early in life are more likely to have increased total white blood cell counts, leading to a higher risk of inflammation and infection. Additionally, individuals in inflammatory states and infections are more likely to develop insulin resistance, suggesting that immune system activation leads to decreased insulin sensitivity.29 This indicates that insulin resistance and chronic low-grade inflammatory states interact with each other, reflecting potential activation of the immune system, which in turn affects β-cell function, promotes the development of T2DM, and affects renal function. Several previous studies have shown a pathological connection between insulin resistance and inflammation. In the presence of insulin resistance, adipose tissue is induced to produce inflammation, activating and releasing pro-inflammatory cytokines such as IL-6 and TNF-α, which induce renal endothelial dysfunction, leading to microalbuminuria.25,30 Additionally, defective insulin action in muscle and liver tissues in insulin-resistant states leads to a chronic low-grade inflammatory state, activating various pro-inflammatory factors such as interleukin 1, interleukin 6, tumor necrosis factor alpha, monocyte chemotactic proteins, leptin, and resistin, which further promote leukocyte differentiation and maturation, causing a migration of inflammatory factors to the outside of blood vessels, ultimately leading to an increase in circulating leukocytes and inflammatory factors in peripheral blood.31 On the other hand, inflammation itself impairs insulin signaling and promotes β-cell death, accelerating the progression of TDM and CKD.32 The relationship between leukocytes, as markers of inflammation, and IR is bidirectional: IR and lack of insulin sensitivity lead to chronic inflammation and release of inflammatory markers, whereas chronic inflammation promotes IR. Therefore, the results of the study confirming the use of thiazolidinediones to improve insulin sensitivity in reducing proteinuria are significant.33 Improved insulin sensitivity may help prevent early-stage proteinuria, which is a clinically relevant measure for intervening in cardiovascular outcomes in relevant populations.
The impact of inflammation on renal function has been identified in several studies. Shankar et al conducted a cross-sectional study of 4926 patients, where they systematically analyzed multiple inflammatory markers such as WBC count, ultrasensitive CRP, TNF-α, and IL-6 in relation to CKD.13 In patients with end-stage renal disease (ESRD), IL-6 has been shown to be an important predictor of ESRD morbidity and mortality.34 Additionally, population-based, animal, and epidemiological studies have demonstrated the strong association of CRP with a rapid decline in eGFR and the development of CKD. CRP has also been associated with mortality in ESRD patients.35 Rabbit experiments have shown that increasing doses of TNF-α led to a corresponding dose-dependent injury in glomerular endothelial cells.36 Another study by Qin Z et al found that the systemic immune-inflammatory index (SII) was associated with increased urinary albumin excretion compared to traditional inflammatory factors.37 SII combines three inflammatory cells, namely, platelets, neutrophils, and lymphocytes, and is calculated by platelet count x neutrophil count/lymphocyte count. All of these studies support the clear correlation between inflammation and reduced renal function, although the exact mechanism remains unclear. Some researchers believe that inflammatory factors affect glomerular oxidative stress and glomerular monocyte infiltration leading to glomerulosclerosis, injury, and proteinuria, accelerating CKD progression.38 It has also been suggested that inflammation causes glomerular vein stenosis and obstruction of vascular pathways.39
Our present study demonstrated that total leukocyte count and neutrophil count were independently associated with an increased risk of abnormal UACR. However, it is noteworthy that CRP did not significantly increase the risk of abnormal UACR in our preliminary findings. This may be attributed to the relatively small sample size of our study participants or the fact that our study participants were in a non-acute inflammatory state, resulting in a diminished effect of CRP on abnormal UACR. Further studies are needed to validate our findings and identify factors that may influence the relationship between CRP and abnormal UACR. Understanding the mechanisms behind this relationship will help us comprehend the pathophysiology of proteinuria.
To the best of our knowledge, our study is the first to investigate the role of systemic inflammatory markers as mediators between the TyG index and the risk of abnormal proteinuria, thus providing insight into the mechanism by which the TyG index is associated with abnormal proteinuria. Using multivariable-adjusted models, we found that the TyG index was independently associated with an increased risk of abnormal proteinuria. Specifically, 29.6% of the total association between the TyG index and the risk of proteinuria was mediated through platelet, while 11.2% and 3% was mediated through white blood cell (WBC) counts, and neutrophil counts, respectively.
Our study provides epidemiologic support for the biological hypothesis that systemic inflammation plays a crucial role in the pathway between insulin resistance and abnormal proteinuria. It is conceivable that the association between the TyG index and the risk of abnormal proteinuria may be mediated through systemic inflammation, which could be partially explained by the development of diabetes and diabetic nephropathy.
Furthermore, our findings have clinical and public health implications, as the global epidemic of insulin resistance is leading to an increase in the number of patients with diabetes-induced CKD. Insulin resistance and inflammation are modifiable and preventable risk factors, and a substantial number of CKD and diabetes cases can be prevented if the general population maintains a normal body mass index and a healthy lifestyle that reduces levels of insulin resistance and pro-inflammatory markers in the body.
Strengths and Limitations
There are several noteworthy points in this study. First, we applied a new analytical tool which allows for a mathematically consistent decomposition of the total association into direct and indirect associations with a clear interpretation, unlike traditional methods of mediation analysis.40 Second, to the best of our knowledge, this study explored for the first time the mediating role of WBC counts in the association between the TyG index and the risk of abnormal UACR. This provides useful clues to further explore the inflammatory mechanisms between insulin resistance and CKD. Finally, this study contributes to expanding the range of reproducible low-cost monitoring tools for assessing and stratifying patients at high risk for CKD.
However, some limitations should also be acknowledged. Firstly, due to the cross-sectional design of this study, it was not possible to determine a causal relationship between the TyG index, WBC count, and the risk of abnormal UACR. Therefore, prospective studies with larger sample sizes are needed to determine causality. Second, although we adjusted for some potential covariates, we could not completely rule out the influence of other possible confounders. Third, our sample size was small, limiting generalization to different age groups and ethnicities. Fourth, we lacked long-term patient follow-up, and we need to further observe the effects of insulin resistance and inflammatory markers on the progression of renal disease in this population.
Conclusions
In summary, the current study revealed a significant directive association between the TyG index and the risk of urinary albumin-to-creatinine ratio (UACR) in a Chinese adult population. Mediation analysis showed that this association was statistically mediated by total white blood cell (WBC) counts, neutrophil counts and platelet, suggesting that systemic inflammation may be one of the biological mechanisms related to this association. Focusing on systemic inflammation in public health efforts may help reduce the kidney complications of insulin resistance and the development of CKD. Efforts should be aimed at reducing the occurrence of these burdens.
Acknowledgments
The authors wish to thank the participants for their contribution to the current study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding for this study were provided by the National Medical Information Network Popular Science Research of Chinese Pharmaceutical Society in 2022 (Grant Number CMEI2022KPYJ00534 to Xu Sun); The Pharmaceutical science research of Changzhou Four-Medicine Hospital of Nanjing Pharmaceutical Society in 2022 (Grant Number 2022YX020 to Xu Sun); The Health Science and Technology Development Project Foundation of Nanjing in 2022 (Grant Number YKK22232 to Xu Sun).
Disclosure
No potential conflicts of interest relevant to this article were reported.
References
1. Wang Z, Qian H, Zhong S, et al. The relationship between triglyceride-glucose index and albuminuria in United States adults. Front Endocrinol. 2023;14:1215055. doi:10.3389/fendo.2023.1215055
2. Iseki K, Kinjo K, Iseki C, et al. Relationship between predicted creatinine clearance and proteinuria and the risk of developing ESRD in Okinawa, Japan. Am J Kidney Dis. 2004;44(5):806–814. doi:10.1016/S0272-6386(04)01080-7
3. Thoenes M, Bramlage P, Khan BV, et al. Albuminuria: pathophysiology, epidemiology and clinical relevance of an emerging marker for cardiovascular disease. Future Cardiol. 2007;3(5):519–524. doi:10.2217/14796678.3.5.519
4. Miller WG, Bruns DE, Hortin GL, et al. Current Issues in Measurement and Reporting of Urinary Albumin Excretion. Clin Chem. 2009;55:24–38. doi:10.1373/clinchem.2008.106567
5. Zhao S, Yu S, Chi C, et al. Association between macro- and microvascular damage and the triglyceride glucose index in community-dwelling elderly individuals: the Northern Shanghai Study. Cardiovasc Diabetol. 2019;18(1):95. doi:10.1186/s12933-019-0898-x
6. Zhu Q, Chen Y, Cai X, et al. The non-linear relationship between triglyceride-glucose index and risk of chronic kidney disease in hypertensive patients with abnormal glucose metabolism: a cohort study. Front Med Lausanne. 2022;9:1018083. doi:10.3389/fmed.2022.1018083
7. Hsu CC, Chang HY, Huang MC, et al. Association between insulin resistance and development of microalbuminuria in type 2 diabetes: a prospective cohort study. Diabetes Care. 2011;34(4):982–987. doi:10.2337/dc10-1718
8. Pilz S, Rutters F, Nijpels G, et al. Insulin sensitivity and albuminuria: the RISC study. Diabetes Care. 2014;37(6):1597–1603. doi:10.2337/dc13-2573
9. Mykkänen L, Zaccaro DJ, Wagenknecht LE, et al. Microalbuminuria is associated with insulin resistance in nondiabetic subjects: the insulin resistance atherosclerosis study. Diabetes. 1998;47(5):793–800. doi:10.2337/diabetes.47.5.793
10. Esteghamati A, Ashraf H, Nakhjavani M, et al. Insulin resistance is an independent correlate of increased urine albumin excretion: a cross-sectional study in Iranian Type 2 diabetic patients. Diabet Med. 2009;26(2):177–181. doi:10.1111/j.1464-5491.2008.02653.x
11. Artunc F, Schleicher E, Weigert C, et al. The impact of insulin resistance on the kidney and vasculature. Nat Rev Nephrol. 2016;12(12):721–737. doi:10.1038/nrneph.2016.145
12. Park JM, Shin SP, Cho SK, et al. Triglyceride and glucose (TyG) index is an effective biomarker to identify severe acute pancreatitis. Pancreatology. 2020;20(8):1587–1591. doi:10.1016/j.pan.2020.09.018
13. Shankar A, Sun L, Klein BE, et al. Markers of inflammation predict the long-term risk of developing chronic kidney disease: a population-based cohort study. Kidney Int. 2011;80(11):1231–1238. doi:10.1038/ki.2011.283
14. Stenvinkel P, Chertow GM, Devarajan P, et al. Chronic Inflammation in Chronic Kidney Disease Progression: role of Nrf2. Kidney Int Rep. 2021;6(7):1775–1787. doi:10.1016/j.ekir.2021.04.023
15. Simental-Mendía LE, Rodríguez-Morán M, Guerrero-Romero F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord. 2008;6(4):299–304. doi:10.1089/met.2008.0034
16. Cho YT, Chen CW, Chen MP, et al. Diagnosis of albuminuria by tryptic digestion and matrix-assisted laser desorption ionization/time-of-flight mass spectrometry. Clin Chim Acta. 2013;420:76–81. doi:10.1016/j.cca.2012.12.016
17. Küme T, Sağlam B, Ergon C, et al. Evaluation and comparison of Abbott Jaffe and enzymatic creatinine methods: could the old method meet the new requirements? J Clin Lab Anal. 2018;32(1):e22168. doi:10.1002/jcla.22168
18. Shamsuzzaman AS, Winnicki M, Wolk R, et al. Independent association between plasma leptin and C-reactive protein in healthy humans. Circulation. 2004;109(18):2181–2185. doi:10.1161/01.CIR.0000127960.28627.75
19. Tingley D, Teppei H, Mit Y, et al. mediation: r Package for Causal Mediation Analysis. J Statil Soft. 2014;59(5). doi:10.18637/jss.v059.i05
20. Yang S, Kwak S, Song YH, et al. Association of Longitudinal Trajectories of Insulin Resistance With Adverse Renal Outcomes. Diabetes Care. 2022;45(5):1268–1275. doi:10.2337/dc21-2521
21. Gao YM, Chen WJ, Deng ZL, et al. Association between triglyceride-glucose index and risk of end-stage renal disease in patients with type 2 diabetes mellitus and chronic kidney disease. Front Endocrinol. 2023;14:1150980. doi:10.3389/fendo.2023.1150980
22. Fritz J, Brozek W, Concin H, et al. The Triglyceride-Glucose Index and Obesity-Related Risk of End-Stage Kidney Disease in Austrian Adults. JAMA Network Open. 2021;4(3):e212612. doi:10.1001/jamanetworkopen.2021.2612
23. Jager A, Kostense PJ, Nijpels G, et al. Microalbuminuria is strongly associated with NIDDM and hypertension, but not with the insulin resistance syndrome: the Hoorn Study. Diabetologia. 1998;41(6):694–700. doi:10.1007/s001250050970
24. Welsh GI, Coward RJ. Podocytes, glucose and insulin. Curr Opin Nephrol Hypertens. 2010;19(4):379–384. doi:10.1097/MNH.0b013e32833ad5e4
25. De Cosmo S, Menzaghi C, Prudente S, et al. Role of insulin resistance in kidney dysfunction: insights into the mechanism and epidemiological evidence. Nephrol Dial Transplant. 2013;28(1):29–36. doi:10.1093/ndt/gfs290
26. Jauregui A, Mintz DH, Mundel P, et al. Role of altered insulin signaling pathways in the pathogenesis of podocyte malfunction and microalbuminuria. Curr Opin Nephrol Hypertens. 2009;18(6):539–545.
27. Su WY, Chen SC, Huang YT, et al. Comparison of the Effects of Fasting Glucose, Hemoglobin A1c, and Triglyceride-Glucose Index on Cardiovascular Events in Type 2 Diabetes Mellitus. Nutrients. 2019;11(11):2838. doi:10.3390/nu11112838
28. Paschou SA, Kothonas F, Lafkas A, et al. Favorable Effect of Anti-TNF Therapy on Insulin Sensitivity in Nonobese, Nondiabetic Patients with Inflammatory Bowel Disease. Int J Endocrinol. 2018;2018:6712901. doi:10.1155/2018/6712901
29. Vozarova B, Weyer C, Lindsay RS, et al. High white blood cell count is associated with a worsening of insulin sensitivity and predicts the development of type 2 diabetes. Diabetes. 2002;51(2):455–461. doi:10.2337/diabetes.51.2.455
30. Shimobayashi M, Albert V, Woelnerhanssen B, et al. Insulin resistance causes inflammation in adipose tissue. J Clin Invest. 2018;128(4):1538–1550. doi:10.1172/JCI96139
31. Fain JA. NHANES. Diabetes Educ. 2017;43(2):151. doi:10.1177/0145721717698651
32. Hotamisligil GS. Inflammation and metabolic disorders. Nature. 2006;444(7121):860. doi:10.1038/nature05485
33. Sarafidis PA, Stafylas PC, Georgianos PI, et al. Effect of thiazolidinediones on albuminuria and proteinuria in diabetes: a meta-analysis. Am J Kidney Dis. 2010;55(5):835–847. doi:10.1053/j.ajkd.2009.11.013
34. Pecoits-Filho R, Lindholm B, Axelsson J, et al. Update on interleukin-6 and its role in chronic renal failure. Nephrol Dial Transplant. 2003;18(6):1042–1045. doi:10.1093/ndt/gfg111
35. Iseki K, Tozawa M, Yoshi S, et al. Serum C-reactive protein (CRP) and risk of death in chronic dialysis patients. Nephrol Dial Transplant. 1999;14(8):1956–1960. doi:10.1093/ndt/14.8.1956
36. Bertani T, Abbate M, Zoja C, et al. Tumor necrosis factor induces glomerular damage in the rabbit. Am J Pathol. 1989;134(2):419–430.
37. Qin Z, Li H, Wang L, et al. Systemic Immune-Inflammation Index Is Associated With Increased Urinary Albumin Excretion: a Population-Based Study. Front Immunol. 2022;13:863640. doi:10.3389/fimmu.2022.863640
38. Wang H, Li J, Gai Z, et al. TNF-α Deficiency Prevents Renal Inflammation and Oxidative Stress in Obese Mice. Kidney Blood Press Res. 2017;42(3):416–427. doi:10.1159/000478869
39. Viecelli AK, Mori TA, Roy-Chaudhury P, et al. The pathogenesis of hemodialysis vascular access failure and systemic therapies for its prevention: optimism unfulfilled. Semin Dial. 2018;31(3):244–257. doi:10.1111/sdi.12658
40. VanderWeele TJ. Mediation Analysis: a Practitioner’s Guide. Annu Rev Public Health. 2016;37:17–32. doi:10.1146/annurev-publhealth-032315-021402
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.