")
Back to Journals » Journal of Inflammation Research » Volume 17
A Prospective Comparative Study on the Clinical Diagnostic Performance of Blood Inflammatory Markers in Acute Appendicitis
Authors Yuan Z , Chen C , Liu K , Chen F
Received 11 July 2024
Accepted for publication 15 October 2024
Published 22 October 2024 Volume 2024:17 Pages 7521—7534
DOI https://doi.org/10.2147/JIR.S486645
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Blood inflammatory markers in acute appendicitis – Video abstract [486645]
Views: 93
Zhenchao Yuan, Changhua Chen, Kefang Liu, Fengying Chen
Department of Clinical Laboratory, People’s Hospital of HuiLi City, Huili, Sichuan Province, 615100, People’s Republic of China
Correspondence: Fengying Chen, Email [email protected]
Objective: Despite the substantial advancements in imaging techniques for the diagnosis and differential diagnosis of acute appendicitis (AA) over recent decades, the specificity and sensitivity of widely utilized laboratory biomarkers in clinical practice remain inadequate.This study aimed to investigate the diagnostic utility of commonly employed blood inflammatory markers for AA.
Methods: A total of 399 participants who either sought medical care or underwent health examinations were enrolled in this prospective study. The cohort comprised 200 patients diagnosed with AA (AA group), 100 patients presenting with abdominal pain but without AA (AP group), and 99 healthy individuals undergoing routine health check-ups (HC group). For all subjects, the following biomarkers were measured: plasma neutrophil gelatinase-associated lipocalin (NGAL), white blood cell count (WBC), neutrophil count (NEU), percentage of neutrophils (NEU%), neutrophil-to-lymphocyte ratio (NLR), and C-reactive protein (CRP). The diagnostic performance of the observed indicators, both individually and in combination, was assessed for the diagnosis of AA using Receiver Operating Characteristic (ROC) curves analysis and Delong’s test.
Results: The laboratory indicators demonstrated a progressive increase from the HC group to the AP group, and further to the AA group (all p< 0.05). Multifactorial logistic regression analysis identified NEU% and plasma NGAL as significant risk factors for the occurrence of AA. ROC curve analysis and Delong’s test indicated that, in distinguishing the AA group from the HC group, the diagnostic performance of plasma NGAL, CRP, and NLR was equally substantial and superior to that of NEU and WBC. Within the AP group, plasma NGAL and CRP exhibited comparable diagnostic efficacy, outperforming NEU, WBC, and NLR. When differentiating AA in the non-appendicitis group (ie HC group + AP group), NGAL and CRP demonstrated comparable diagnostic efficacy, surpassing that of NEU, white WBC, and NLR. While the integration of multiple diagnostic tests can potentially improve overall diagnostic accuracy, the observed enhancement in the AUC is not statistically significant.
Conclusion: NGAL, CRP, WBC, NEU% and NLR were significantly increased in patients with acute abdomen. NGAL and NEU% may function as independent risk factors for predicting the incidence of AA, with NGAL and CRP demonstrating similar and favorable diagnostic performance. While the combined evaluation of these biomarkers may enhance the diagnostic value for AA, the improvement in the area under the curve (AUC) is not substantial.
Keywords: neutrophil gelatinase-associated lipocalin, acute appendicitis, biomarkers, diagnostic value
A Letter to the Editor has been published for this article.
Introduction
Acute appendicitis (AA) represents a common emergency abdominal condition encountered in clinical practice, marked by rapid progression and diverse clinical presentations. These factors frequently contribute to clinical misdiagnosis or oversight, potentially leading to rapid deterioration of the patient’s condition. This deterioration can result in severe complications, such as appendiceal suppuration or perforation, posing a significant threat to the patient’s life if not promptly and appropriately addressed.1 Approximately one-third of AA patients exhibit atypical clinical symptoms,2 further complicating the diagnostic process. When abdominal pain manifests, laboratory tests and/or imaging examinations serve as pivotal tools for diagnostic assistance and differential diagnosis. Presently, laboratory examinations, computed tomography scans, and/or imaging such as ultrasound are commonplace techniques for diagnosing or differentiating AA.3 Although abdominal ultrasound demonstrates a significantly high diagnostic yield,4 its accuracy is contingent upon the proficiency of the examining personnel and their clinical judgment. Recent reports indicate that the diagnosis of AA via ultrasound may involve an estimated misdiagnosis rate of approximately 4% and a delayed diagnosis rate of 63%.5,6 Studies have shown that the misdiagnosis rate of AA in adult ultrasound diagnostics can exceed 50%, while the rate of missed diagnoses approaches 45%.7
In clinical practice, commonly employed inflammatory markers used in clinical laboratories for assisting in the diagnosis of AA mainly include white blood cell (WBC), neutrophil percentage (NEU%), and acute-phase reactants such as C-reactive protein (CRP). However, existing research indicates that these markers demonstrate relatively limited diagnostic efficacy for AA.8–11 Recent research indicates that 5-hydroxyindoleacetic acid, leucine-rich alpha-2-glycoprotein, CA-125, and pentraxin-3 present in urine may serve as potential biomarkers for the diagnosis of AA.12–15 However, their current clinical applications are constrained, necessitating comprehensive prospective studies to validate their diagnostic utility.
Recent studies have revealed that neutrophil gelatinase-associated lipocalin (NGAL), a 25 kDa protein from the lipocalin family, is secreted by neutrophils upon activation and exhibits antimicrobial properties. Elevated NGAL levels serve as an inflammatory biomarker in kidney and liver diseases, tumors, and inflammatory bowel diseases. Notably, during appendiceal inflammation, NGAL levels in appendiceal tissue also rise. For instance, a report by Swedish authors highlights NGAL’s sensitivity(Se) and specificity(Sp) of >90% in diagnosing the majority of infectious diseases, showcasing significant superiority over NEU, CRP, procalcitonin, and the expression of CD64 on the surface of neutrophils.16 Recent investigations indicate that NGAL, as an inflammatory marker, aids in the diagnosis of pediatric AA,17 although it is not effective in differentiating between uncomplicated and complicated pediatric AA. Furthermore, while NGAL provides definitive diagnostic information in pediatric AA, it struggles to discern the severity of AA.18 This study focuses on adult subjects, establishes a comparable control group, measures NGAL and common inflammatory markers used in clinical laboratories in the participants, and analyzes their predictive diagnostic performance for adult AA.
Methods
Study Object
AA Group (AA): A total of 200 patients diagnosed with AA at the People’s Hospital of Huili City (Sichuan, China) from April 2021 to April 2023 were selected as the disease group. This group was categorized based on pathological types as follows: 160 cases of uncomplicated AA (congestive, phlegmonous or suppurative appendicitis) and 40 cases of complicated AA (gangrenous or perforated appendicitis). Inclusion criteria: 1) underwent appendectomy and received a final pathological diagnosis of AA; 2) did not receive any treatment before admission; 3) complete clinical case data; 4) age >18 years. 5) patients who have not received any prior treatment before seeking medical attention. Exclusion criteria: 1) various connective tissue diseases; 2) acute or chronic kidney disease; 3) cancer and immunodeficiency; 4) incomplete clinical data; 5) previous appendectomy due to AA. 6) patients who have taken any medication prior to seeking medical attention. This prospective comparative study was approved by the Ethics Committee of the People’s Hospital of Huili (Approval No: 2022–001-lwsc-1).
Abdominal Pain Group (AP): A total of 100 patients with abdominal pain during the same period were included as the disease control group. Diagnoses included 30 cases of acute gastroenteritis, 12 cases of ureteral calculi, and 58 cases of nonspecific abdominal pain. The inclusion and exclusion criteria are consistent with those established for the AA group, with the exception of the AA diagnostic criteria.
Healthy Control Group (HC): Ninety-nine individuals who underwent health examinations at our hospital’s health examination center during the same period were included as the healthy control group. Inclusion criteria: 1) Participants aged 18 years or older; 2) Healthy volunteers with normal examination indicators; 3) Individuals who have not consumed health supplements. Exclusion criteria: 1) Participants experiencing difficulty or failure in venipuncture during blood collection; 2) Pregnant or lactating women; 3) Individuals who have consumed health supplements within the past month.
Operation Steps
Blood samples were obtained from the patient prior to the administration of any treatment upon admission. Healthy subjects underwent an overnight fasting period, after which blood samples were collected in a fasting state between 8:00 and 10:00 the following morning. Blood samples were collected using vacuum blood collection tubes (Kangweishi Medical, Hebei). Two tubes of EDTA-K3 anticoagulant (approximately 2mL per tube) and one tube of additive-free non-anticoagulant blood (approximately 5mL) were drawn to the indicated marks. The tubes were gently inverted eight times as per the instructions to ensure thorough mixing. One tube of anticoagulated blood was used for complete blood cell analysis, while the other tube was centrifuged at approximately 2,300g for 10 minutes to separate plasma for NGAL determination. The additive-free non-anticoagulant blood was allowed to stand for about 30 minutes post-collection to clot. After clotting, serum was separated by centrifugation at 2,300g for 10 minutes for CRP measurement. To screen for patients with impaired renal function, serum urea (Urea) and creatinine (Cr) levels were also measured.
Primary Measurement Index
Within 2 hours of sample collection, complete blood cell count and CRP analyses were performed using the BF-6900 automated hematology analyzer (Dirui, Changchun). This yielded the WBC, NEU, NEU%, and absolute lymphocyte count for each study subject. Additionally, using the absolute counts of NEU and lymphocytes, the NLR (Neutrophil-to-Lymphocyte Ratio) was calculated as NLR = absolute neutrophil count / absolute lymphocyte count.
Within 4 hours of sample collection, measurements were conducted using the AU5800 fully automated biochemical analyzer (Beckman Coulter, USA). The NGAL assay employed latex-enhanced turbidimetric immunoassay methodology, with reagents provided by Zhejiang Quark Biotechnology Co., Ltd. Serum CRP levels were determined using latex-enhanced turbidimetric immunoassay, while Urea levels were measured using the urease-glutamate dehydrogenase method and Cr levels were assessed using the creatininase-creatinase method, with reagents provided by Ningbo Ruiyuan Biotechnology Co., Ltd.
Statistical Analysis
The Kolmogorov–Smirnov test was employed to evaluate the normality of quantitative variables. Data that did not conform to a normal distribution are presented as the median (P25, P75). Group comparisons were conducted using the Kruskal–Wallis H-test for multiple groups and the Mann–Whitney U-test for pairwise comparisons. Categorical data was presented as frequencies and group comparisons were performed using the chi-square test. A LASSO regression model was constructed using the glmnet function to identify significant variables. A logistic regression analysis with multiple factors was applied to identify the risk factors for AA among the observed indicators. The diagnostic performance of the observed indicators was assessed using Receiver Operating Characteristic (ROC) curve analysis. Statistical analyses were carried out using R for Windows 4.0.3 (R Core Team, Vienna, Austria) and SPSS 26.0 (IBM Corp., Armonk, NY, USA) software. A p<0.05 was considered statistically significant.
Results
Participant Characteristics and Laboratory Test Results
In this study, CRP was measured using two methods that showed high agreement (data not shown). Therefore, only whole blood CRP results were used for statistical analysis. The statistical analysis revealed no significant differences in gender, age, ethnicity, serum Urea, and Cr levels among the three groups (all p>0.05) (Table 1). However, the median values of the other observed laboratory indicators showed a sequential increase across the HC, AP, and AA groups (Figure 1). While these observed indicators displayed statistical differences among the three groups (Table 1), the comparisons between HC and AP for NGAL, CRP, and NEU% did not reach statistical significance (all p>0.05), and there was no statistical difference in WBC levels between AP and AA (p=0.061). However, significant differences were observed between the remaining pairs of groups (all p<0.001). The results show that the chosen participants had similar basic characteristics, validating the selection process. Laboratory indicators varied statistically across groups, indicating their potential use in diagnosing or distinguishing between AP and AA.
 |
Table 1 Participant Basic Characteristics and Observed Laboratory Indicators [M(P25, P75)] |
 |
Figure 1 Distribution of observed laboratory indicators among three groups. (A) NGAL; (B) CRP; (C) NLR; (D) WBC; (E) NEU%. Five laboratory parameters under observation (NGAL, CRP, WBC, NEU%, and NLR) exhibit statistically significant differences among the three groups, with median values increasing sequentially with HC, AP, and AA. NGAL stands for neutrophil gelatinase-associated lipocalin, CRP for C-reactive protein, WBC for white blood cell count, NEU% for percentage of neutrophils, and NLR for neutrophil-to-lymphocyte ratio. HC represents the healthy control group, AP represents the disease control group, and AA represents the disease group. In the graph, the “circle” denotes outside values, while the “asterisk” signifies far-out values. |
Important Predictors for AA Occurrence
In order to identify which observed indicators may serve as important predictors for the occurrence of AA, the two control groups (HC and AP) were classified as non-AA. LASSO regression analysis was employed to explore which of the seven factors, including age, gender, NGAL, CRP, WBC, NEU%, and NLR, might significantly influence the occurrence of AA. The results revealed that as the penalty coefficient (also known as the regularization parameter, λ) increased, the coefficients of the variables included in the model were gradually compressed to zero, thereby preventing overfitting of the model (Figure 2A). Figure 2B illustrates the process of λ selection in LASSO regression, indicating that the degree of variable compression and the number of variables varied with different λ values. The optimal value of λ was chosen where the mean squared error was at its minimum plus one standard error, yielding λ=0.0355, with four corresponding non-zero coefficient variables: NGAL, CRP, WBC, and NEU%. This suggests that NGAL, CRP, WBC, and NEU% may significantly influence the occurrence of AA.
 |
Figure 2 LASSO regression variable selection process. (A) Coefficient curves of LASSO regression for the selection of 7 factors; (B) LASSO regression and parameter λ selection using 10-fold cross-validation. Age, gender, NGAL, CRP, WBC, NEU%, and NLR, a total of 7 factors, show that as λ increases, the variable coefficients are compressed to zero. The optimal λ corresponds to four non-zero coefficient variables, namely NGAL, CRP, WBC, and NEU%. NGAL, Neutrophil Gelatinase-Associated Lipocalin; CRP, C-Reactive Protein; WBC, White Blood Cell count; NEU%, Neutrophil Percentage; NLR, Neutrophil-to-Lymphocyte Ratio. |
Predictive Indicators for AA Occurrence
For the purpose of selecting indicators predicting the occurrence of AA, single-factor logistic regression analysis revealed that when each individual laboratory indicator was included in the analysis, all studied laboratory indicators emerged as risk factors for AA. To establish an influencing factor model with greater precision, the factors NGAL, CRP, WBC, and NEU%, identified through LASSO regression analysis, were introduced as independent variables in a multiple-factor logistic regression analysis (Table 2). The findings demonstrated that only NGAL and NEU% stood out as risk factors for AA, suggesting they can serve as predictive indicators for the occurrence of AA.
 |
Table 2 Univariate and Multivariate Analysis of Risk Factors for Acute Appendicitis |
Diagnostic Performance of Observed Indicators for AA
ROC curve analysis was used to assess the diagnostic performance of each observed indicator for AA. Subsequently, drawing from clinical practices, the accessibility of results, and project costs, four combined testing modes were established and organized in a sequence reflecting increasing complexity. The diagnostic performance of different combinations of indicators for AA detection was analyzed based on the current clinical application status of these observed indicators. These combinations include: 2-Com (WBC + NEU), 3-Com (WBC + NEU + NLR), 4-Com (WBC + NEU + NLR + CRP), and 5-Com (WBC + NEU + NLR + CRP + NGAL). The cutoff value corresponding to the maximum Youden index (= Se + Sp - 1) was selected, and the corresponding sensitivity and specificity were obtained.
HC vs AA
The results revealed that the diagnostic performance (represented by AUC) of the observed indicators in distinguishing AA from healthy individuals (HC vs AA) as follows (Figure 3A, Tables 3 and 4): NGAL (0.85) exhibited comparable diagnostic performance with CRP (0.84) and NLR (0.80) (all p>0.05), outperforming both WBC (0.74) and NEU (0.76) (all p<0.05), The diagnostic performance of 5-Com (0.89) and 4-Com (0.88) were comparable (p=0.30), and both outperformed 3-Com (0.79) and 2-Com (0.79)(all p<0.05). The diagnostic performance indicators obtained at the cutoff value selected based on maximum YI, including Se, Sp, and AUC (95% CI), are listed in Table 3. These results suggest that the observed indicators have diagnostic value in distinguishing AA from healthy individuals. The diagnostic performance of 4-Com is comparable to 5-Com, rendering NGAL testing unnecessary while maintaining high diagnostic value. However, the marginal increase in AUC from combined testing suggests that it does not significantly enhance diagnostic performance.
 |
Table 3 Diagnostic Performance Evaluation of Various Indicators for Diagnosing Acute Appendicitis |
 |
Table 4 Pairwise Delong Test Comparison Results for the Area Under the Curve (AUC) of Various Diagnostic Indicators |
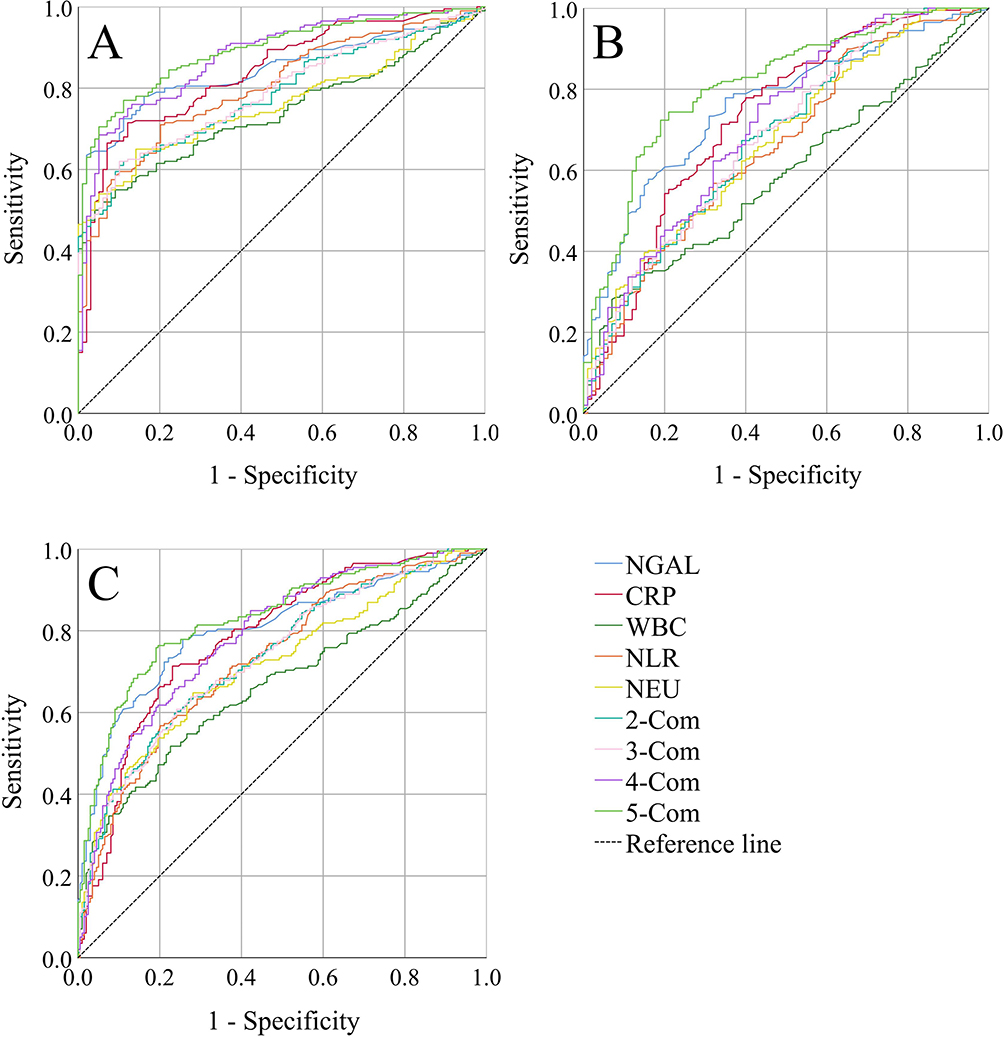 |
Figure 3 ROC curve analysis of each observed indicator. (A) HC vs AA; (B) AP vs AA; (C) (HC+AP) vs AA, where, 2-Com indicates the combination of 2 observed indicators, and so forth. The AUC of each indicator is largest when distinguishing between HC and AA, smallest when distinguishing between AP and AA, and lies between the two when distinguishing between (HC+AP) and AA. Although the AUC for combined detection is larger than that for individual parameters, the increment is marginal. NGAL, Neutrophil Gelatinase-Associated Lipocalin; CRP, C-Reactive Protein; WBC, White Blood Cell count; NEU, Neutrophil count; NLR, Neutrophil-to-Lymphocyte Ratio; HC, Healthy Control Group; AP, Abdominal Pain Group; AA, Acute Appendicitis Group. |
AP vs.AA
ROC analysis of the observed indicators in differentiating AA from individuals with abdominal pain (AP vs AA), the diagnostic performance as follows (Figure 3B, Tables 3 and 4): NGAL (0.76) demonstrated comparable diagnostic performance with CRP (0.73) (p=0.35) and outperformed WBC (0.59), NEU (0.67), and NLR (0.66) (all p<0.05). The diagnostic performances of combined testing were 5-Com (0.81), 4-Com (0.71), 3-Com (0.69), and 2-Com (0.68), and 5-Com surpassed that of other combined diagnostic indicators (all p<0.001). The diagnostic performance indicators obtained at the cutoff value selected based on maximum YI, including Se, Sp, and AUC (95% CI), are listed in Table 3. These results indicate that incorporating NGAL testing can enhance diagnostic value to a certain extent. However, the minimal increase in AUC from combined testing suggests only marginal improvement in diagnostic performance.
Control Group (HC+AP) vs AA
ROC analysis of the observed indicators in distinguishing AA within all control groups (Figure 3C, Tables 3 and 4) revealed that the diagnostic performance (represented by AUC) as follows: NGAL (0.80) exhibited comparable diagnostic performance with CRP (0.78) (p=0.47) and outperformed WBC (0.67), NEU (0.72), and NLR (0.73) (all p<0.05). The diagnostic performance of 5-Com (0.83) surpassed that of 4-Com (0.79), 3-Com (0.74), and 2-Com (0.74) (all p<0.05). The diagnostic performance indicators obtained at the cutoff value selected based on maximum YI, including Se, Sp, and AUC (95% CI), are listed in Table 3. These results suggest that the observed indicators have diagnostic value in distinguishing AA within all control groups, with their diagnostic performance falling between the healthy and abdominal pain groups. At the same time incorporating NGAL testing can enhance diagnostic value to a certain extent. Nevertheless, the modest increase in AUC from combined testing suggests only marginal enhancement in diagnostic performance.
Discussion
Acute abdomen refers to a range of urgent abdominal conditions predominantly marked by severe abdominal pain. Among these conditions, AA is recognized as the fourth most prevalent cause of acute abdominal pain, representing approximately 4.0% of cases within this classification.19 The clinical manifestations of AA frequently intersect with those of numerous other acute abdominal conditions, resulting in a high incidence of misdiagnosis or oversight. Timely and precise diagnosis, along with effective differential diagnosis, is essential for delivering appropriate treatment to patients. Research indicates that AA elicits a systemic inflammatory response, with inflammatory markers often employed as diagnostic indicators for this condition.20 Despite this, these markers lack adequate predictive value for the occurrence of AA.21 Consequently, the investigation of novel biomarkers specifically designed for the diagnosis and differential diagnosis of AA is of paramount importance for enhancing diagnostic accuracy and improving patient outcomes. Currently, WBC, NEU%, NLR, and CRP are widely used in clinical practice for diagnosing infections and evaluating their severity. The NLR indicates the balance between neutrophils and lymphocytes. In acute inflammation, neutrophils rise sharply while lymphocytes decrease, leading to elevated NLR values up to 7.0. Thus, NLR effectively reflects the body’s inflammatory status.22 CRP, an acute-phase reactant, is recognized as a highly sensitive biomarker for systemic inflammation and tissue injury.23 A variety of clinical laboratory techniques are employed for the analysis of CRP, utilizing sample sources such as whole blood, serum, and plasma. In numerous clinical laboratories across China, CRP testing is frequently performed in conjunction with complete blood cell counts to evaluate the potential presence of infection in patients, thereby assisting outpatient physicians in making informed decisions regarding the appropriateness of antimicrobial therapy. Therefore, CRP can be effectively integrated with WBC, NEU%, and NLR to monitor the inflammatory infection status of subjects. This study utilized two distinct methods for CRP analysis to assess the consistency of the results. According to literature reports, the diagnostic performance of CRP or NLR in AA exceeds that of WBC.24,25 This study confirms that CRP and NLR outperform WBC counts in diagnostic accuracy. It is noteworthy that in clinical practice, when CRP is utilized as a marker for infection, the upper limit of the reference value for this detection method is 6.0 mg/L. This threshold is approximately equivalent to the cut-off values distinguishing HC group from AA group (HC vs AA) and is closely aligned with the cut-off values differentiating HC+AP group from AA group ([HC+AP] vs AA). These findings underscore the reliability of our research results. However, in the pursuit of optimal diagnostic performance (maximum AUC), the threshold for differentiating between AP group and AA group was found to decrease to 4.44 mg/L. If a cut-off value of 6.0 mg/L is employed, the diagnostic performance (indicated by YI) for HC vs AA, AP vs AA, and (HC+AP) vs AA are 0.59, 0.33, and 0.46, respectively, which do not significantly deviate from their maximum diagnostic performance. Similar trends are observed in NLR, where the differences are statistically significant but do not impact their clinical applicability. However, the combined use of WBC, NEU%, NLR, and CRP for diagnosing AA is underexplored. Many labs do not include CRP in blood tests, and NLR reports are rare. Regrettably, certain clinical laboratories continue to omit the simultaneous detection of CRP in peripheral blood analysis reports, and only a limited number of laboratories include the NLR in their assessments. This oversight may result in the underestimation of the diagnostic efficacy of comprehensive blood test results for inflammatory reactions. It is imperative that clinical practitioners and laboratory personnel address this issue with due seriousness. The addition of detection items is unlikely to significantly enhance diagnostic performance, which may be attributable to the collinearity among white WBC, NEU%, NLR, and CRP levels.
NGAL is a member of the lipid transport protein family, predominantly expressed by neutrophils and to a lesser extent by epithelial cells in the kidney, prostate, respiratory tract, digestive tract, and appendix.26 Clinically, NGAL is primarily utilized as a biomarker for acute kidney injury.27 Additionally, research has demonstrated its potential as a predictive indicator for sepsis,28 suggesting that NGAL possesses anti-inflammatory properties.29 This study observed a significant elevation of NGAL in peripheral blood of patients with AA, demonstrating superior diagnostic performance compared to commonly used inflammatory markers. This indicates that NGAL may serve as a predictive biomarker for AA. However, NGAL detection requires plasma or serum samples rather than whole blood, which may prolong testing times in clinical laboratories. Fortunately, combined testing revealed that incorporating NGAL into whole blood indices did not significantly enhance the diagnostic accuracy for AA. Therefore, even if clinicians test plasma NGAL in patients suspected of AA, its independent diagnostic performance should be carefully evaluated. In addition to blood testing, NGAL is frequently assessed in urine samples within clinical practice, with results typically adjusted for creatinine levels. Consequently, when kidney dysfunction is ruled out and NGAL levels are elevated, it is imperative to consider the possibility of inflammation occurring in a specific organ or tissue within the patient’s body.
The present study rising trends in various lab indicators for AP and AA, suggesting these parameters could help diagnose or signal the potential occurrence of AA or AP. The ROC curve assessed the diagnostic performance of individual and combined indices for AA, demonstrating that these indices are most effective in distinguishing between healthy controls (HC) and AA, less so in distinguishing between combined (HC+AP) and AA, and least effective in distinguishing between AP and AA. Combining the HC and AP groups could result in an overdiagnosis of the analyzed markers. Nonetheless, differentiating the diagnosis of acute abdomen based on clinical signs and physician expertise remains challenging. Even with ultrasound examination, the misdiagnosis and missed diagnosis rate for AA in adults is approximately 50%. This study amalgamated the HC and AP groups into a control group for evaluation, with the objective of gaining a deeper understanding of the clinical significance of the observed biomarkers for AA. These findings suggest that in the clinical setting, physicians should prioritize the use of inflammatory markers for distinguishing between AA-related and non-AA-related abdominal pain. Our research confirms that in differentiating AP from AA, the diagnostic performance of NGAL is comparable to CRP and superior to other inflammatory markers. Several existing studies indicate that while NGAL offers quantifiable and valuable insights for the diagnosis of AA, its utility is limited in assessing the severity of the condition. Consequently, NGAL cannot serve as an effective biomarker for differentiating between uncomplicated and complex cases of appendicitis,18,30,31 broadly aligning with the results of our study. However, in our study, the cutoff value of NGAL for differentiating non-appendicitis abdominal pain from AA was determined to be 58.15 ng/mL, In contrast Javier et al reported an NGAL cutoff value of only 40.97 ng/mL, highlighting a significant difference between the findings of the two studies. Analysis indicates that these disparities may arise from various factors like different samples (plasma vs serum), varied study populations (adults vs children), detection methods difference, and subject differences (ethnicity and sampling), among others. As there are no specific diagnostic markers for AA, when patients with acute abdominal pain are admitted, clinical laboratory tests rarely involve a single parameter. Particularly in peripheral blood analyses, more than 20 or even more parameters can be obtained from a single test. Therefore, combined observations could theoretically to enhance the diagnostic performance for detecting AA. However, studies show no significant enhancement in performance. In the differentiation of HC vs AA, the diagnostic performance of the 4-com model is comparable to the 5-com model, suggesting that NGAL testing is unnecessary. In distinguishing AP from AA, the diagnostic performance of the 4-com model is lower than that of the 5-com model. Inclusion of NGAL in the combined testing shows some improvement in diagnostic performance, yet the increase in the AUC is not substantial. The limitations of this study include: 1) failure to consider variations in the duration from disease onset to hospital admission, as well as differences in clinical presentation, including symptoms such as fever, vomiting, and other clinical characteristics; 2) failure to distinguish between uncomplicated appendicitis and complicated appendicitis; 3) the study focused only on common inflammation or infection and did not evaluate procalcitonin, despite the growing number of clinical markers available; 4) the study being limited to a single-center small sample, raising questions regarding the representativeness and transferability of its results. 5) the experimental results were not evaluated after adjustment for body surface area. Future research initiatives will encompass multi-center collaborations to evaluate the clinical value of commonly employed inflammatory markers in the prediction and diagnosis of AA. These efforts will aim to replicate findings to confirm their significance.
Conclusion
Acute appendicitis (AA) is the leading cause of emergency abdominal surgery and necessitates prompt diagnosis.32 A delayed diagnosis of AA can result in severe complications, including appendiceal perforation, peritonitis, and sepsis, thereby increasing both the incidence rate and mortality.33 AA is characterized by an early localized inflammatory response, prompting the evaluation of various inflammation-related biomarkers—such as WBC count, absolute neutrophil count, immature granulocyte count, CRP, procalcitonin, interleukin-6, and NLR—as potential predictive factors for complex AA. Nevertheless, the findings in this domain remain contentious.32,33 This study identified NGAL, CRP, WBC, NEU%, and NLR as potential independent risk factors for predicting the occurrence of AA. Among these, NGAL and CRP demonstrated comparable and robust diagnostic performance. However, the combined assessment of these inflammatory markers did not significantly enhance their diagnostic value for AA.
Data Sharing Statement
The datasets used and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Ethics Approval
This study was approved by the Ethics Committee of the People’s Hospital of Huili (Approval No: 2022-001-lwsc-1) and complied with the Declaration of Helsinki.
Informed Consent
All patients signed an informed consent form.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Science and Technology Research Project of the Liangshan Yi Autonomous Prefecture (Grant No. 21ZDYF0103).
Disclosure
The authors have no relevant financial or nonfinancial interests to disclose.
References
1. Güney C, Coskun A. Can Fetuin-A, CRP, and WBC levels be predictive values in the diagnosis of acute appendicitis in children with abdominal pain? Healthcare. 2019;7:110. doi:10.3390/healthcare7040110
2. Dal F, Cicek Y, Pekmezci S, et al. Role of Alvarado score and biological indicators of C-reactive protein, procalicitonin and neopterin in diagnosis of acute appendicitis. Ulus Travma Acil Cerrahi Derg. 2019;25:229–237. doi:10.5505/tjtes.2018.57362
3. Moris D, Paulson EK, Pappas TN. Diagnosis and management of acute appendicitis in adults: a review. JAMA. 2021;326:2299–2311. doi:10.1001/jama.2021.20502
4. Neal JT, Monuteaux MC, Rangel SJ, Barnewolt CE, Bachur RG. Refining sonographic criteria for paediatric appendicitis: combined effects of age-based appendiceal size and secondary findings. Emerg Med J. 2022;39:924–930. doi:10.1136/emermed-2021-211751
5. Staab S, Black T, Leonard J, Bruny J, Bajaj L, Grubenhoff JA. Diagnostic accuracy of suspected appendicitis: a comparative analysis of misdiagnosed appendicitis in children. Pediatr Emerg Care. 2022;38:690–696. doi:10.1097/PEC.0000000000002323
6. Michelson KA, Reeves SD, Grubenhoff JA, et al. Clinical features and preventability of delayed diagnosis of pediatric appendicitis. JAMA Netw Open. 2021;4:e2122248. doi:10.1001/jamanetworkopen.2021.22248
7. Kam CT, Alsahaf M, Chongbang K, et al. Ultrasound vs. clinical diagnosis-which is better in diagnosing acute appendicitis?: a cohort study. Ann Med Surg. 2023;85:2336–2340. doi:10.1097/MS9.0000000000000730
8. Altali Alhames K, Martín-Sánchez FJ, Ruiz-Artacho P, et al. Diagnostic accuracy of combining C-reactive protein and Alvarado score among 2-to-20-year-old patients with acute appendicitis suspected presenting to emergency departments. Rev Esp Quimioter. 2021;34:220–227. doi:10.37201/req/008.2021
9. Bom WJ, Scheijmans JCG, Salminen P, Boermeester MA. Diagnosis of uncomplicated and complicated appendicitis in adults. Scand J Surg. 2021;110:170–179. doi:10.1177/14574969211008330
10. Peksöz R, Dişçi E, Kaya A, et al. Significance of laboratory parameters in diagnosing acute appendicitis during pregnancy. ANZ J Surg. 2022;92:121–127. doi:10.1111/ans.17443
11. Peksöz R, Bayar B. The role of complete blood count parameters in diagnosing acute appendicitis and measuring the severity of inflammation. Ulus Travma Acil Cerrahi Derg. 2021;27:654–661.
12. Arredondo Montero J, Pérez Riveros BP, Bueso Asfura OE, Rico Jiménez M, López-Andrés N, Martín-Calvo N. Leucine-rich alpha-2-glycoprotein as a non-invasive biomarker for pediatric acute appendicitis: a systematic review and meta-analysis. Eur J Pediatr. 2023;182:3033–3044. doi:10.1007/s00431-023-04978-2
13. Arredondo Montero J, Pérez Riveros BP, Bueso Asfura OE. Diagnostic performance of serum CA-125 for overall and complicated acute appendicitis: a systematic review and meta-analysis. Updates Surg. 2024;76:793–801. doi:10.1007/s13304-024-01842-2
14. Anand S, Pakkasjärvi N, Bajpai M, et al. Utility of Pentraxin-3 as a biomarker for diagnosis of acute appendicitis: a systematic review and meta-analysis. Pediatr Surg Int. 2022;38:1105–1112. doi:10.1007/s00383-022-05149-4
15. Arredondo Montero J, Bueso Asfura OE, Pérez Riveros BP, López Burgos E, Rico Jiménez M. Diagnostic performance of urinary 5-hydroxyindoleacetic acid in acute appendicitis: a systematic review and diagnostic test accuracy meta-analysis. Int J Colorectal Dis. 2023;38:269. doi:10.1007/s00384-023-04556-w
16. Venge P. Human neutrophil lipocalin (HNL) as a biomarker of acute infections. Ups J Med Sci. 2018;123:1–8. doi:10.1080/03009734.2017.1420112
17. Sobczak J, Burzyńska M, Sikora A, Wysocka A, Karawani J, Sikora JP. Post-traumatic stress response and appendicitis in children-clinical usefulness of selected biomarkers. Biomedicines. 2023;11:1880. doi:10.3390/biomedicines11071880
18. Kakar M, Delorme M, Broks R, et al. Determining acute complicated and uncomplicated appendicitis using serum and urine biomarkers: interleukin-6 and neutrophil gelatinase-associated lipocalin. Pediatr Surg Int. 2020;36:629–636. doi:10.1007/s00383-020-04650-y
19. Cervellin G, Mora R, Ticinesi A, et al. Epidemiology and outcomes of acute abdominal pain in a large urban emergency department: retrospective analysis of 5,340 cases. Ann Transl Med. 2016;4:362. doi:10.21037/atm.2016.09.10
20. Bukhari HA, Mirza M. Complicated appendicitis is predicted by the presence of systemic inflammatory response syndrome. Saudi Surg J. 2020;8:32. doi:10.4103/ssj.ssj_6_20
21. Schellekens DH, Hulsewé KW, van Acker BA, et al. Evaluation of the diagnostic accuracy of plasma markers for early diagnosis in patients suspected for acute appendicitis. Acad Emerg Med. 2013;20:703–710. doi:10.1111/acem.12160
22. Zahorec R. Neutrophil-to-lymphocyte ratio, past, present and future perspectives. Bratisl Lek Listy. 2021;122:474–488. doi:10.4149/BLL_2021_078
23. Samuel MS, Latha R, Kavitha K, Sivasubramanian V. A study on biomarkers of sepsis and potential role of procalcitonin and ferritin marker in diagnosis, prognosis and treatment. J Family Med Prim Care. 2022;11:2608–2612. doi:10.4103/jfmpc.jfmpc_1920_21
24. Patmano M, Çetin DA, Gümüş T. Laboratory markers used in the prediction of perforation in acute appendicitis. Ulus Travma Acil Cerrahi Derg. 2022;28:960–966.
25. Duyan M, Vural N. Assessment of the diagnostic value of novel biomarkers in adult patients with acute appendicitis: a cross-sectional study. Cureus. 2022;14:e32307. doi:10.7759/cureus.32307
26. Li N, Zhao WG, Xu FL, Zhang WF, Gu WT. Neutrophil gelatinase-associated lipocalin as an early marker of acute kidney injury in patients with traumatic brain injury. J Nephrol. 2013;26:1083–1088. doi:10.5301/jn.5000282
27. Marakala V. Neutrophil gelatinase-associated lipocalin (NGAL) in kidney injury - A systematic review. Clin Chim Acta. 2022;536:135–141. doi:10.1016/j.cca.2022.08.029
28. Ragán D, Horváth-Szalai Z, Szirmay B, Mühl D. Novel damage biomarkers of sepsis-related acute kidney injury. EJIFCC. 2022;33:11–22.
29. Nasioudis D, Witkin SS. Neutrophil gelatinase-associated lipocalin and innate immune responses to bacterial infections. Med Microbiol Immunol. 2015;204:471–479. doi:10.1007/s00430-015-0394-1
30. Bakal U, Saraç M, Ciftci H, et al. Neutrophil gelatinase-associated lipocal in protein levels as an acute appendicitis biomarker in children. Springerplus. 2016;5:193. doi:10.1186/s40064-016-1853-x
31. Arredondo Montero J, Antona G, Bardají Pascual C, et al. Serum neutrophil gelatinase-associated lipocalin (NGAL) as a diagnostic tool in pediatric acute appendicitis: a prospective validation study. Pediatr Surg Int. 2022;38:1569–1576. doi:10.1007/s00383-022-05197-w
32. Adir A, Braester A, Natalia P, et al. The role of blood inflammatory markers in the preoperative diagnosis of acute appendicitis. Int J Lab Hematol. 2024;46:58–62. doi:10.1111/ijlh.14163
33. Díaz López MI, Crespo Álvarez E, Martínez Manzano Á, et al. Usefulness of extended inflammatory parameters related to neutrophil activation reported by Sysmex XN-1000 hematology analyzer for predicting complicated acute appendicitis. comparison with canonical inflammatory laboratory tests. Cir Esp. 2024;102:300–306. doi:10.1016/j.ciresp.2023.11.014
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.