")
Back to Journals » Clinical Ophthalmology » Volume 19
A Prospective, Crossover, Randomized, Double-Blind Clinical Study Comparing the Effectiveness and Ocular Comfort of 0.1% Hyaluronic Acid and 0.3% Hyaluronic Acid in Patients With Dry Eye Disease
Authors Kim SJ, Yoo WS , Kwon LH, Kim RB , Yoon HJ, Yoon KC
Received 7 October 2024
Accepted for publication 10 January 2025
Published 6 February 2025 Volume 2025:19 Pages 407—416
DOI https://doi.org/10.2147/OPTH.S489669
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Seong-Jae Kim,1,* Woong-Sun Yoo,1,* Lee-Ha Kwon,1 Rock Bum Kim,2,3 Hyeon-Jeong Yoon,4 Kyung Chul Yoon4
1Department of Ophthalmology, Institute of Medical Science, Gyeongsang National University Hospital, Gyeongsang National University College of Medicine, Jinju, South Korea; 2Regional Cardiocerebrovascular Disease Center, Gyeongsang National University Hospital, Jinju, South Korea; 3Department of Preventive Medicine, Institute of Medical Science, Gyeongsang National University College of Medicine, Jinju, South Korea; 4Department of Ophthalmology, Chonnam National University Medical School, Gwangju, South Korea
*These authors contributed equally to this work
Correspondence: Kyung Chul Yoon, Department of Ophthalmology, Chonnam National University Medical School, #42 Jebong-ro, Dong-gu, Gwangju, 61469, South Korea, Tel +82-62-220-6753, Fax +82-62-227-1642, Email [email protected]
Purpose: Report the clinical effects and discomfort of using 0.1% hyaluronic acid (HA [Kynex 1®, Alcon, Seoul, S. Korea]) and 0.3% HA (Kynex 3®, Alcon, Seoul, S. Korea) to treat dry eye disease (DED).
Methods: This study was designed as a prospective, crossover, randomized, and double-blind study. Patients aged > 19 years with DED level 2 or higher, corneal staining score > 1, and tear break-up time (TBUT) < 10s were included. Sixty patients were randomly assigned to two groups. Patients in group 1 were instilled with 0.1% HA for four weeks and then 0.3% HA for the next four weeks. Group 2 patients were instilled with the eye drops in the reverse order of group 1. Patients were evaluated using a corneal staining score, TBUT, and the Standardized Patient Evaluation of Eye Dryness (SPEED) questionnaire at baseline, four weeks, and eight weeks.
Results: In both groups, 0.3% HA showed an increasing trend in TBUT, although the difference was not statistically significant. Changes in the Schirmer test were greater in group 2, but this difference was also not statistically significant. The corneal staining score improved in both groups, with no statistically significant difference. While 0.3% HA was more effective than 0.1% HA according to the absolute value, this difference was not statistically significant. There was no difference between the two groups in the SPEED questionnaire evaluation that assessed aspects of discomfort, such as blurred vision, foreign body sensation, and burning sensation.
Conclusion: 0.3% HA was more effective for treating DED, although the difference was not statistically significant. In terms of discomfort, 0.3% HA showed no difference compared to 0.1% HA. Using both 0.1% HA and 0.3% HA in a tailored treatment approach can improve patient comfort and treatment outcomes.
Plain Language Summary: Dry eye disease (DED) is a common condition that causes discomfort and vision problems. This study aimed to find out how well two eye drops, using 0.1% hyaluronic acid (HA [Kynex 1®, Alcon, Seoul, S. Korea]) and 0.3% HA (Kynex 3®, Alcon, Seoul, S. Korea), work in treating DED and how comfortable they are for patients to use. We included 60 adults with moderate to severe DED and divided them into two groups. One group used 0.1% HA for four weeks and then switched to 0.3% HA for another four weeks, while the other group used the drops in the opposite order. We evaluated their symptoms and signs at the beginning, after four weeks, and after eight weeks using ophthalmologic examinations and a questionnaire. Both eye drops helped improve the symptoms of DED, with 0.3% HA being slightly more effective overall, although the difference was not significant. Both eye drops were similarly comfortable for the patients. The study shows that both 0.1% HA and 0.3% HA are effective treatments for DED. While 0.3% HA might have a slight edge in effectiveness, both drops can be used to improve patient comfort and outcomes. Using these eye drops in a personalized treatment plan can help people with DED manage their symptoms better and lead more comfortable lives.
Keywords: dry eye disease, 0.1% hyaluronic acid, 0.3% hyaluronic acid
Introduction
Dry eye disease (DED) is a representative ocular disease with a high prevalence.1 DED has various clinical features, from irritating symptoms such as foreign body sensation or eye discomfort to severe diseases that can cause vision loss due to complications such as corneal infection.2 In 2017, the International Dry Eye Workshop (DEWS II) defined DED as a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film with accompanying ocular symptoms. Tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play etiological roles.3
The treatment of DED focuses on alleviating symptoms, improving tear film stability, and addressing underlying inflammation. First-line therapy typically includes artificial tears to provide immediate symptomatic relief by supplementing the tear film. For patients with persistent symptoms or inflammation, anti-inflammatory medications such as cyclosporine A, or short-term corticosteroids may be prescribed. Recently, the treatment of and research on DED have focused on the instability of the tear film accompanied by ocular surface inflammation. In addition, eye drops designed to increase the stability of the tear film have been widely used in treatment.3,4
Hyaluronic acid (HA) eye drops help regenerate corneal epithelial cells and maintain moisture on the surface of the cornea.5 They are widely used in the clinic to mimic the effect of tears that lubricate the surface of the cornea. In Korea, HA is also used in various concentrations (from 0.1% to 0.3%) to treat dry eyes. The physical viscosity and residual time on the corneal surface vary with HA concentration, so the clinical effects vary. Further, varying HA concentrations have different effects on foreign body sensation and ocular pain.6 Generally, in clinical practice, low concentrations of HA are recommended for patients with mild DED and high concentrations are recommended for patients with severe DED.6
HA eye drops with low concentrations of 0.1–0.15% have low viscosity and are commonly used by patients.7 Lower concentration HA cause relatively less blurring of vision or stickiness, affording less discomfort in the eye after use than higher concentration HA.7 However, since the residual time of low concentration HA on the corneal surface is very short, the protective effect on the expected corneal surface is significantly reduced in patients with severe DED.8 On the contrary, HA eye drops with a high concentration of 0.3% have a relatively high viscosity, which increases their residual time on the corneal surface. Therefore, the protective effect for the corneal surface is prolonged without increasing the frequency of eye drop use.8 However, after using eye drops, some patients report stickiness due to high concentrations, discomfort with the drug, and blurred vision.
This study aimed to compare the clinical effects and discomfort when using 0.1% HA (Kynex 1®, Alcon, Seoul, S. Korea) and low-viscosity 0.3% HA (Kynex 3®, Alcon, Seoul, S. Korea), which is a high concentration of HA that suggests maintaining the clinical effect as well as the comfort of use.
Materials and Methods
Study Design
This study was a prospective, multi-center (Gyeongsang National University Hospital, Chonnam National University Hospital), randomized, double-blind crossover study with a duration of eight weeks. This study was registered in the Clinical Trial Registry of Korea (https://cris.nih.go.kr: KCT 0004912). In this double-blind study, the investigational drug was distributed by a designated investigational nurse who was unblinded and had access to the drug allocation, ensuring that the investigators and participants remained blinded to the treatment assignments throughout the study. Subjects eligible to participate in the study were assigned subject numbers at the first screening visit. The administration of a drop of 0.3% HA or 0.1% HA corresponding to each group was started every six hours (4 times a day). Subjects were evaluated at week 4, and crossover medication was initiated, administering a drop of 0.1% HA or 0.3% HA every six hours (4 times a day). Subjects were re-evaluated four weeks later. Thus, the subjects had a total study and treatment period of eight weeks. Sixty suitable subjects were enrolled and divided into two groups. In group 1, 0.1% HA was administered for four weeks, and 0.3% HA was administered in a dose of a drop four times a day for four weeks. In group 2, 0.3% HA was applied for four weeks, and 0.1% HA was applied in a dose of a drop four times a day for four weeks.
The criteria for inclusion were:
- An adult male or female over the age of 19,
- A person who met the following two criteria at the first screening visit:
● A person whose tear-film break-up time (TBUT) was 10 seconds or less,● Evaluation of the subject’s dry eye condition was at least “sometimes” to the question “How often do you feel your eyes were dry enough to want to use eye drops?”
The criteria for exclusion were:
- Any history of intraocular surgery on either side of the eye within the past six months,
- Any history of intolerance or hypersensitivity to any ingredient in a research drug,
- Any history or evidence of herpes simplex epithelial keratitis related to vaccination, and active or recent corneal and/or conjunctival varicella zoster virus disease, ocular rosacea, chronic bacterial disease in the cornea and/or conjunctiva and/or lids, ocular mycobacterial infection and/or ocular fungal infection,
- Use of topical ophthalmic drugs during the study period,
- Subjects on systemic medications (ie, treatments for cold and allergic diseases, tricyclic antidepressants, hormone replacement therapy) that may cause dry eyes were not enrolled in the study if they were not administering a stable dose of their medication for at least 30 days prior to visit 0; in addition, the dosage and route of medications were kept stable during the study period,
- Active/acute blepharitis, conjunctival inflammation, or iritis that could make it impossible to ensure safe administration of research products,
- Subjects who had worn contact lenses within 72 hours prior to screening, who needed to use them during the clinical trial period, or who did not agree to refrain from wearing contact lenses,
- Subjects who underwent a punctal closure procedure within 90 days prior to screening (ie, collagen plug, silicon plug),
- Subjects who underwent refractive surgery such as laser-assisted in situ keratomileusis within 12 months prior to screening,
- Subjects with an autoimmune disease (ie, Sjogren’s syndrome),
- Subjects previously diagnosed with a mental illness that may affect the progress of this study,
- Pregnant women, lactating women, women of childbearing age who intended to become pregnant during the study period or were not using appropriate contraceptive methods,
- Subjects with a history of drug or alcohol abuse,
- Researchers, members of the researcher’s family, or individuals residing in such a person’s household,
- Subjects who received other clinical trial drugs or medical devices within 30 days of participation in this study.
To evaluate the effectiveness and safety of eye drops in the treatment of DED, the following were analyzed: score of dry-eye symptoms and signs, corneal staining score, TBUT, score for a change in dry-eye symptoms and signs from the baseline value, change in the corneal staining test value, change of TBUT, treatment compliance, and scores from the Standardized Patient Evaluation of Eye Dryness (SPEED) questionnaire.
Statistical Analysis
The results of categorical variables and continuous variables are presented as the number (%) and mean (standard deviation), respectively. To compare the baseline (first visit) characteristics and parameters of DED between groups, we performed the Mann–Whitney U-test and Fisher’s exact test. To evaluate how the signs of DED, including TBUT, the Schirmer test, and National Eye Institute scores, changed over time (at the first visit, after four weeks, and after eight weeks) between the two groups, we employed a mixed effect model with the subject identifier as a random effect and periods as a fixed effect. To evaluate the changes after using HA isotonic, we calculated the absolute differences of signs of DED and the questionnaire in each of the two groups. Then, we calculated a coefficient of absolute difference based on the mixed effect model, which means the changing of 0.3% HA isotonic groups compared to 0.1% HA isotonic groups. To evaluate the proportions of mild, moderate, and severe compliance Q questionnaire components after dropping the 0.1% and 0.3% HA, we conducted the McNemar test. All statistical analyses were performed using R software (version 4.3; R Core Team, 2023; R: Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria).
Results
The overall age of 60 patients was 36.4 ± 7.8 (mean SD) years, which included 38 women (68.3%). There were no significant differences in age and sex between the two groups. When comparing the average difference in TBUT, the Schirmer test, and corneal staining scores between the two groups using the Mann–Whitney U-test, no statistically significant differences were observed (p = 0.667, 0.622, and 0.760, respectively). Additionally, there were no differences in the results of the SPEED questionnaire (all p > 0.05; Table 1). TBUT values after the first visit, four weeks later, and eight weeks later showed a slight improvement in the second group, based on eyes with low values at the time of the visit. Still, the difference was not statistically significant (p = 0.676, mixed effect model; Figure 1). In the Schirmer test, a comparison between screening and changes at eight weeks showed a slight improvement in group 2, which was not statistically significant (p=0.724, mixed effect model; Figure 2). Even when the corneal staining scores were compared, no significant difference was observed between the two groups (p = 1.0, mixed effect model; Figure 3). To analyze the absolute effect between screening and after the use of eye drops, the effects of 0.1% HA and 0.3% HA were analyzed with mixed effect models based on the eye with worse DED according to screening. In TBUT, 0.1% HA increased by 0.8 ± 1.1 seconds, and 0.3% HA increased by 0.9 ± 1.2 seconds. As a result of checking the coefficient to find out the effect of 0.3% HA compared to 0.1% HA, TBUT increased by 0.11 seconds, and the Schirmer test increased by 0.2 mm. The corneal staining score was measured to be 0.02 points lower, which was a little more effective, but there was no statistical significance (Table 2). Finally, McNemar verification was conducted on the results of the questions asked, dividing the blurring, foreign body sensation, and burning sensation into three stages (mild, modulate, and average) to evaluate compliance with treatment. There was no significant difference in comfort between the two groups (Table 3).
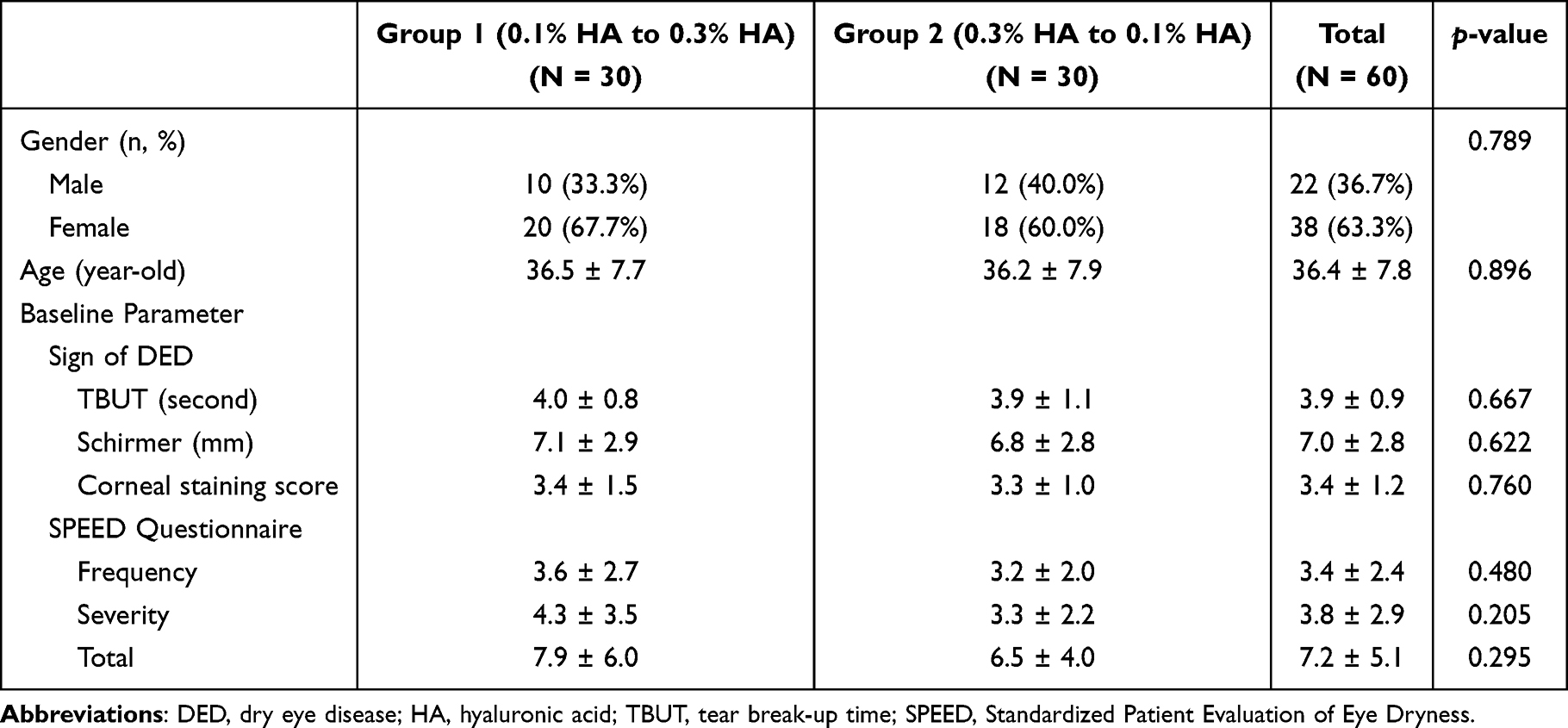 |
Table 1 Baseline Characteristics of the Groups |
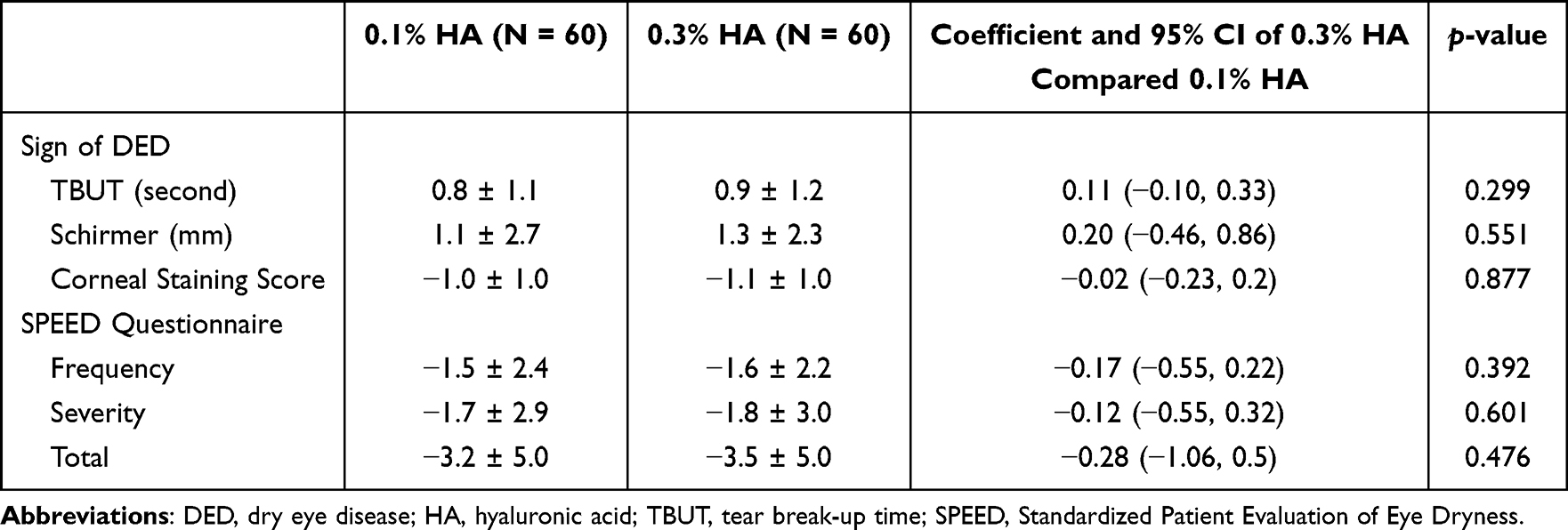 |
Table 2 Absolute Effects Between 0.1% and 0.3% Hyaluronic Acid Using Mixed Effect Models |
 |
Table 3 Comparing Discomforts Between 0.1% and 0.3% Hyaluronic Acid |
 |
Figure 1 TBUT changes from the baseline (mean±SD). There was no significant difference in the increase of TBUT between the two groups at weeks 4 and 8 (p = 0.676). TBUT = Tear-film break-up time. |
 |
Figure 2 Schirmer I score changes from the baseline (mean±SD). There was no significant difference in the increase of Schirmer scores between the two groups at weeks 4 and 8 (p = 0.724). |
 |
Figure 3 National Eye Institute (NEI) score changes from the baseline (mean±SD). The decrease in the NEI score showed no significant difference between the two groups at weeks 4 and 8 (p = 1.000). NEI=National Eye Institute. |
Discussion
HA eye drops with a high concentration of HA (0.3%) generally have a greater protective effect on the surface of the cornea than lower concentration HA (0.1, 0.15%); however, the patients’ compliance is known to be poor due to temporarily blurred vision and foreign body or burning sensations after application.8 0.3% HA used in this study designed with low viscosity technology (Huons Co. Ltd., Seongnam, S. Korea), which helps mitigate the disadvantages of these high-concentration HA eye drops, improving comfort and maintaining the clinical effect. Herein, 0.3% HA was relatively more effective for treating DED, although the difference in effectiveness between 0.3% HA and 0.1% HA was not statistically significant, with a similar level of comfort compared to 0.1% HA.
Most artificial tears have similar core ingredients, but the osmolality, viscosity, and pH differ. Artificial tears are usually based on moisture and contain various types of viscous substances that increase viscosity to promote lubrication and residual time on the corneal surface.6 Viscous substances, such as HA, contained in artificial tears protect the corneal surface via various mechanisms and relieve dry-eye symptoms by increasing the tear film thickness, protecting from dry stimulation, increasing tear residual time, offering a coating effect, and maintaining corneal thickness and goblet cell density.6 HA is a non-sulfated glycosaminoglycan with negative charges and hydrophilicity and is a component of connective tissue, the epithelium, and nerve tissue.8 The viscosity of HA varies with the shear rate; as the shear rate increases, the viscosity decreases, which occurs while blinking.9 The higher the viscosity of HA eye drops, the longer the residual time, but this causes blurred vision or debris to remain on the eyelids or eyelashes, which in turn may decrease patient compliance.9 In the case of clinically severe DED, high-concentration, high-viscosity HA is used to assist patients with corneal epithelial regeneration, risking discomfort such as blurred vision.10 The ideal HA should reduce the discomfort of patients by lowering the viscosity while maintaining a high concentration of HA.10 Therefore, 0.3% HA was developed, which with this aim, maintains a low viscosity while maintaining a high concentration of 0.3% HA. In this study, we showed that that the comfort of patients using 0.3% HA remains similar to that of patients using 0.1% HA.
In DED, an increase in osmotic pressure in the tear increases inflammation of the surface of the cornea, damages the corneal epithelium, and eventually causes a vicious cycle that worsens DED.3 In previous studies, increased osmotic pressure in tears has been found to increase the concentration of inflammatory cytokines such as tumor necrosis factor-alpha, interferon-gamma, interleukin-1, IL-6, and IL-8.3 In order to decrease osmotic pressure in tears, it was confirmed that hypotonic 0.3% HA produced less corneal damage, fewer inflammatory cytokines occurred in the DED model, and the goblet cell of the conjunctiva remained high compared to isotonic 0.3% HA.11 A number of studies compared hypotonic and isotonic HA, but there have been no studies comparing the improvement effect in DED and comfort of use according to the HA content. In addition, no significant differences have been reported in a comparison between HA eye drops and other eye lubricants or by the concentration, molecular weight, and frequency of HA eye drops.9 This is thought to be caused by an insufficient number of study subjects due to the diversity of comparison subjects. A study that compared 0.1%, 0.18%, and 0.3% HA with 0.05% cyclosporine ophthalmic solutions reported that the corneal staining score evaluated at 12 weeks after starting eye drops decreased in 0.1% HA by −3.77 ± 1.97 and 0.3% HA by −3.52 ± 2.15, compared to baseline.12 After 12 weeks of treatment, TBUT increased with 0.1% HA by 2.18 ± 2.63 and with 0.3% HA by 2.24 ± 2.30, and Schirmer change was 1.31 ± 6.04 for 0.1% HA and 2.54 ± 6.46 for 0.3% HA, which was similar to our study.12 Still, statistical significance was not found, and adverse reactions were also not significantly different with 0.1% HA (13.33%) and 0.3% HA (12.77%).12 In a study comparing tear film thickness using anterior segment optical coherence tomography between the saline group and the groups of 0.1%, 0.2%, and 0.3% HA, the depth, height, and turbidity of the tear film immediately after application increased in all concentrations compared to baseline, and the duration was longer in proportion to the concentration of HA.13 This is thought to be due to higher concentrations resulting in longer residual times. In our study, TBUT results showed a slight improvement in the group that first used 0.3% HA and then switched to 0.1% HA. Still, there was no statistically significant difference between the groups. In the analysis of TBUT at screening and at four weeks, the slope was steeper in the group using 0.3% HA at baseline than in the group using 0.1% HA at baseline, and the slope increased again in the group using 0.3% HA after four weeks switching from 0.1% HA. Although there was no statistically significant increase in TBUT, it can be seen that, consistent with previous studies, a 0.3% HA is more effective.12 In the Schirmer test, comparing the changes at screening and at week 8, the group using 0.3% HA at baseline showed a slight improvement, although it was not statistically significant. In order to analyze the absolute effect of eye drops, the effect of 0.1% HA and 0.3% HA was examined with a mixed effect model. The TBUT increased in 0.3% HA by 0.9 ± 1.2 seconds and increased in 0.1% HA by 0.8 ± 1.1 seconds. Eventually, 0.3% HA was more effective than 0.1% HA in TBUT improvement, corneal staining score, and the Schirmer test, especially by rapidly increasing TBUT. In severe DED, 0.3% HA can be used first to recover ocular surface homeostasis.
To evaluate compliance with the treatment, McNemar verification was performed on the results of the questions divided into mild, moderate, and average regarding blurring, foreign body sensation, and burning sensation. There was no significant difference in comfort of use between the two groups using 0.3% HA and 0.1% HA. Regarding blurring, six patients (10%) and three patients (5%) reported discomfort at a moderate level in 0.3% HA and 0.1% HA, respectively. In terms of foreign body sensation and burning sensation, four (6.9%) and three (5.2%) patients experienced moderate discomfort with 0.3% HA, while eight (13.8%) and nine (15.5%) did with 0.1% HA. At this point, even if 0.3% HA causes a little more blurring, it is manufactured with low viscosity, so the comfort seems to be improved compared to 0.1% HA in terms of foreign body sensation and burning sensation.
This study has the following limitations. First, the number of patients enrolled was relatively small. It is highly possible that this was the reason no statistically significant differences were observed between the two groups. Second, the follow-up period was short at eight weeks. Third, the crossover design requires at least two weeks of rest in the process of changing the two drugs, but the present study did not comply with this requirement. However, this was inevitable because the selection criteria were set for patients who usually used 0.1% HA. Additionally, the study did not account for matching participants by factors such as age, gender, or severity of dryness, which could influence treatment outcomes and reduce variability. Considering these points for the future, large-scale multi-center clinical trials are expected to be necessary.
Conclusions
In conclusion, a low-viscosity 0.3% HA, showed better comfort, such as foreign body and burning sensations, than 0.1% HA. Though the differences were not statistically significant, 0.3% HA showed slightly more effective results in TBUT and the Schirmer test. 0.3% HA could be a good alternative for patients who have severe DED and feel uncomfortable with 0.1% HA. Managing patients with DED using a tailored approach that includes both 0.1% HA and 0.3% HA can enhance patient comfort and treatment efficacy.
Abbreviations
DED, dry eye disease; DEWS, Dry Eye Workshop; HA, hyaluronic acid; NEI, National Eye Institute; SPEED, Standardized Patient Evaluation of Eye Dryness; TBUT, tear break-up time.
Data Sharing Statement
The data used during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the institutional review board of Gyeongsang National University Hospital and Chonnam National University Hospital. All procedures involving human material were performed in accordance with the current ethical standards of the institutional and national research committees, the Declaration of Helsinki, and its later amendments or comparable ethical standards. Written informed consent was obtained from all participants prior to their inclusion in the study. This study was registered in the Clinical Trial Registry of Korea (https://cris.nih.go.kr: KCT 0004912).
Acknowledgments
This research was supported by Alcon through an Investigator Initiated Trial Research Grant No. 54247305, biomedical research institute fund (GNUHBRIF-2023-0002) from the Gyeongsang National University Hospital, the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. NRF-2023R1A2C1007712, 2021R1A4A3027122, and RS-2023-00219399), and the grant from Institute of Health Science of Gyeongsang National University (2022).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Johnson ME, Murphy PJ. Changes in the tear film and ocular surface from dry eye syndrome. Prog Retin Eye Res. 2004;23(4):449–474. doi:10.1016/j.preteyeres.2004.04.003
2. Sutu C, Fukuoka H, Afshari NA. Mechanisms and management of dry eye in cataract surgery patients. Curr Opin Ophthalmol. 2016;27(1):24–30. doi:10.1097/ICU.0000000000000227
3. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
4. Kusada N, Yokoi N, Kato H, et al. Evaluation of dry eye with videokeratographer using a newly developed indicator. Am J Ophthalmol. 2023;252:135–146. doi:10.1016/j.ajo.2023.03.023
5. Srinivasan S, Garofalo R, Williams R. Safe and effective management of dry eye symptoms with hydroxypropyl guar and hyaluronic acid dual-polymer lubricating eye drops: a review of preclinical and clinical studies. Clin Ophthalmol. 2023;17:3883–3889. doi:10.2147/OPTH.S428725
6. Hynnekleiv L, Magno M, Moschowits E, et al. A comparison between hyaluronic acid and other single ingredient eye drops for dry eye, a review. Acta Ophthalmol. 2023;12. doi:10.1111/aos.15675
7. Chen N, Zhang JS, Zhang TX, Fan BL, Ning Y. The effect of sodium hyaluronate on tear film stability in patients with dry eye syndrome after cataract surgery. Graefes Arch Clin Exp Ophthalmol. 2023;261(4):1011–1017. doi:10.1007/s00417-022-05880-7
8. Calonge M, Sahyoun M, Baillif S, et al. Sodium hyaluronate 0.30% ocular gel versus sodium hyaluronate 0.18% eye drop in the treatment of moderate to severe dry eye disease. Eur J Ophthalmol. 2023;33(1):188–195. doi:10.1177/11206721221096321
9. Hynnekleiv L, Magno M, Vernhardsdottir RR, et al. Hyaluronic acid in the treatment of dry eye disease. Acta Ophthalmol. 2022;100(8):844–860. doi:10.1111/aos.15159
10. Yang YJ, Lee WY, Kim YJ, Hong YP. A meta-analysis of the efficacy of hyaluronic acid eye drops for the treatment of dry eye syndrome. Int J Environ Res Public Health. 2021;18(5):2383. doi:10.3390/ijerph18052383
11. Li Y, Cui L, Lee HS, et al. Comparison of 0.3% hypotonic and isotonic sodium hyaluronate eye drops in the treatment of experimental dry eye. Curr Eye Res. 2017;42(8):1108–1114. doi:10.1080/02713683.2017.1297462
12. Park YL, Song JS, Choi CY, et al. A randomized multicenter study comparing 0.1%, 0.15%, and 0.3% sodium hyaluronate with 0.05% cyclosporine in the treatment of dry eye. J Ocul Pharmacol Ther. 2017;33(2):66–72. doi:10.1089/jop.2016.0086
13. Carracedo G, Pastrana C, Serramito M, Rodriguez-Pomar C. Evaluation of tear meniscus by optical coherence tomography after different sodium hyaluronate eyedrops instillation. Acta Ophthalmol. 2019;97(2):e162–e169. doi:10.1111/aos.13887
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.