")
Back to Journals » Journal of Pain Research » Volume 17
A Randomized Controlled Non-Inferiority Trial Evaluating Opioid-Free versus Opioid-Sparing Analgesia for Orbital Fracture Reconstruction Under General Anesthesia
Authors Zhang R, Mai Y, Ye H, Lian X, Yang H, Zhu Y, Gan X
Received 17 August 2024
Accepted for publication 6 November 2024
Published 11 November 2024 Volume 2024:17 Pages 3707—3717
DOI https://doi.org/10.2147/JPR.S491994
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Rui Zhang,1,* Yongjian Mai,1,* Huijing Ye,2,* Xiufen Lian,2 Huasheng Yang,2 Yanling Zhu,1 Xiaoliang Gan1
1Department of Anesthesiology, State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-sen University, Guangdong Provincial Key Laboratory of Ophthalmology Visual Science, Guangdong Provincial Clinical Research Center for Ocular Diseases, Guangzhou, 510060, People’s Republic of China; 2Department of Orbital Diseases and Ocular Oncology, State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-sen University, Guangdong Provincial Key Laboratory of Ophthalmology Visual Science, Guangdong Provincial Clinical Research Center for Ocular Diseases, Guangzhou, 510060, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoliang Gan; Yanling Zhu, Email [email protected]; [email protected]
Background and Objectives: Opioid-minimizing strategies are making their appearance in enhanced recovery after surgery. This study is aimed to explore the potential advantages of opioid-free analgesia (OFA) compared to opioid-sparing analgesia (OSA) in patients undergoing orbital fracture reconstruction.
Methods: In this prospective, single-center, randomized controlled study, we randomly recruited 122 patients undergoing orbital fracture reconstruction under general anesthesia. Patients received total intravenous anesthesia with a flexible laryngeal mask airway, and multimodal analgesia with either OSA or OFA methods. The OSA group (n = 61) received low doses of fentanyl and nonsteroidal anti-inflammatory drugs (NSAIDs), and the OFA group (n = 61) received medial canthus peribulbar block (MCPB) combined with NSAIDs. The primary outcomes consisted of area-under-the-curve (AUC) of the numerical rating scale (NRS) pain score, and the incidence of postoperative nausea and vomiting (PONV) through the first 24h.
Results: Compared to the OSA group, the OFA group demonstrated non-inferiority in postoperative analgesia through the first 24 postoperative hours (difference of the medians, − 6; 95% confidence interval [CI], − 12 to 6), but failed to meet the non-inferiority criterion in the incidence of PONV (difference ratio, 3%; 95% CI, − 7% to 14%). The Quality of Recovery-40 questionnaire (QoR-40) scores on postoperative day 1 was significantly higher in group OFA compared to group OSA (188 [178 to 196] vs 181 [169 to 191], respectively; P = 0.005).
Conclusion: In orbital fracture reconstruction, both OFA and OSA strategies provide effective postoperative pain relief, but OFA using MCPB combined NSAIDs enhances the quality of early postoperative recovery.
Registered: Chinese Clinical Trial Registry ChiCTR1900028088.
Keywords: peribulbar block, opioid-free, opioid-sparing, analgesia, orbital fracture reconstruction
Introduction
Over the past decades, the field of orbital surgery has greatly evolved with the aim of restoring and improving the structural integrity and function of the orbit. Surgical trauma following orbital procedures, such as orbital fracture reconstruction, is a complex issue involving both the soft tissue and bony injuries.1 Our previous research has revealed that 62.5% of these patients experience significant postoperative pain, even when non-opioid analgesics such as acetaminophen and and nonsteroidal anti-inflammatory drugs (NSAIDs) are used.2 Given that the majority of orbital reconstructions are now performed under general anesthesia on an enhanced recovery after surgery pathway, it is imperative to establish an effective and safe analgesic strategy to manage postoperative pain and enhance quality of recovery.
Opioids play a crucial role in holistic perioperative analgesia with proven efficacy, reliability, and titratability.3,4 In a study by Charlson et al, postoperative opioids were prescribed at a four times higher rate in oculoplastic and orbital surgeries than for procedures of other ophthalmic subspecialties.5 However, reliance on opioid analgesia has well-documented acute side effects such as nausea and vomiting, and a serious long-term potential of opioid dependence.6,7 The present opioid abuse epidemic has also gained significant attention in ophthalmic association, who is actively seeking alternatives that address postoperative pain in an efficacious manner because opioid-related adverse events can impair short-term recovery and extent hospital stays.8,9
Modern multimodal analgesia protocols emphasise lower perioperative opioid use to avoid opioid-related adverse events and are referred to as opioid-sparing analgesia (OSA).10 This has led to the extreme concept of opioid-free analgesia (OFA). When compared with OSA, OFA is associated with an important reduction in postoperative nausea and vomiting (PONV), thereby enhancing the early recovery.6 Regional blocks have been proposed as an utmost part of the multimodal approach to achieve postoperative non-opioid use, owing to its capacity to directly inhibit the activation of pain pathways triggered by surgical incisions. Peribulbar block (PB) is a common technique of ophthalmic anesthesia; however, it carries a relatively high risk of operation-related complications. A modified approach of PB proposed by Brahma et al, called medial canthus peribulbar block (MCPB), offers a feasible and safer alternative to the traditional peribulbar block.11 Previous research has demonstrated that the MCPB appeared to be as effective as the double-injection percutaneous peribulbar technique and required less local anesthetic.12,13 Currently, there is no good evidence evaluating the benefits of OFA versus OSA in patients undergoing primary reconstruction of orbital fractures under general anesthesia. This study was performed to evaluate the efficacy and safety of OFA with MCPB compared to OSA with low-dose fentanyl, both combined with NSAIDs, for patients undergoing orbital fracture reconstruction.
Methods
This study is a prospective, randomized, controlled, non-inferiority trial with blinded outcome analyses. Study approval was obtained from the Institutional Review Board of Zhongshan Ophthalmic Center, Sun Yat-sen University (approval number: 2019KYPJ154). This study was registered at the Chinese Clinical Trial Registry (Registration No.ChiCTR1900028088). The study adheres to the Consolidated Standards of Reporting Trials (CONSORT) statement. Written informed consent was obtained from all participants or their legal guardians.
Patients aged 16 to 65 years with an American Society of Anesthesiologists (ASA) physical status of 1, 2, or 3, who were scheduled to receive primary reconstructions of extensive orbital floor and medial wall fractures under general anesthesia were included between December 2019 and November 2020. Patients were excluded if they had relevant allergies to any medication included in the study protocol, had contraindications to regional ophthalmic blocks, had current gastrointestinal bleeding or peptic ulcer diseases, had a history of opiate abuse, had chronic pain disorders or cognitive dysfunction that would impede accurate engagement with outcome measurements, or had any other factors present likely to influence the study results.
Study Procedures
The day before surgery, potential participants were identified and screened by staff anesthesiologists in anesthesia preoperative evaluation clinic. Then, an investigator of the research team informed the patients who met the eligibility criteria, and elucidated the study protocol, including the potential risks and benefits to the individual participants or their legal guardians. After obtaining written informed consent, patients were randomly assigned to either group OFA or group OSA in a ratio of 1:1 with a computer-generated random number sequence concealed in opaque envelopes. On the day of surgery, before the performance of the procedure, a nurse working independently of the study opened the envelope to reveal the group allocation. The randomization list was retained by an individual not otherwise involved in the study’s undertaking.
General anesthesia was performed using total intravenous anesthesia according to the conventional hospital protocol for adult patients. Anesthesia was induced with propofol, fentanyl and rocuronium. The airway was established in patients using flexible laryngeal mask airway. For maintenance of anesthesia, propofol and remifentanil were administered in target-controlled infusion mode to achieve a bispectral index value of 40–60 and to keep the blood pressure and heart rate within 20% of preanesthesia values intraoperatively. Intravenous atropine and ephedrine were administered as needed to treat bradycardia and hypotension, respectively. Unless contraindicated, dexamethasone 5 mg and tropisetron 5 mg were given prophylactically for postoperative nausea and vomiting (PONV). At 15 minutes before the end of surgery, flurbiprofen axetil 50 mg (Beijing Taide Pharmaceutical Co., Ltd.) was slowly injected in both groups of patients. Propofol and remifentanil were discontinued when surgery ended. Laryngeal mask airway was removed when the patient resumed spontaneous breathing. Patients were then transferred to the postanesthesia care unit (PACU) for further monitoring.
Postoperative Care
Upon completion of wound closure, group OFA received a single shot of MCPB by a consultant ophthalmologist with experience in completing PBs for postoperative analgesia. The block manipulation was performed as a previously described approach by Oliveira.14 A 26-gauge, 13-mm short needle was fully advanced in the semilunaris fold, just above the caruncular and perpendicular to the face (Figure 1). After a lightly negative aspiration, 4 mL of ropivacaine 1% was slowly injected into the hub. Then, compression using Chandler’s manoeuvre was applied for three minutes to facilitate diffusion of the solutions and to prevent elevated ocular hypertonia.15 Group OSA received patient-controlled intravenous analgesia (PCIA) with a regimen of fentanyl (250 μg) and tropisetron (10 mg) diluted with 0.9% normal saline in a total volume of 50 mL. Then, the patient-controlled analgesia (PCA) devices were programmed to deliver 2 mL/h as the basal infusion with a 0.5 mL bolus with 15-min lockout interval, which continued for the first 24 postoperative hours. Patients with a PCA pump were instructed to push the button for administration of a bolus dose if they suffered unbearable pain. The researcher who managed the PCAs decided whether to stop the devices based on the severity of signs and symptoms, and we excluded such cases from the final analysis.
 |
Figure 1 Block Manipulation. Notes: A 26-gauge, 13 mm needle is punctured into the semilunaris fold (white spot), just above the caruncular and perpendicular to the face. The white dashed line delineates the position of the equator of the globe. |
In the PACU, pain was evaluated by an 11-point numeric rating scale (NRS) where 0 is no pain and 10 is the worst pain imaginable. Subjects with NRS >3/10 received an additional dose of flurbiprofen axetil 50 mg as rescue. Subjects were discharged from the PACU once they attained the discharge criteria and had pain scores≤3/10. The analgesic rescue regimen on the surgical ward and at home included scheduled doses of acetaminophen 1 g orally if NRS >3/10. In addition, oral metoclopramide 10mg orally was prescribed as needed for the treatment of PONV unless contraindicated.
Outcomes Measures
The primary outcomes consisted of area-under-the-curve (AUC) of the NRS pain scores, and the incidence of postoperative nausea and vomiting (PONV) through 24h. Pain scores were assessed using NRS pain scores at 2, 6, 12, 24, and 48 hours after surgery, which finally illustrated by calculating the area under the curve (AUC) of NRS points (AUCNRS) for the initial 24h. The incidence of PONV, which encompassed nausea, retching, and vomiting in combination, was analyzed as the primary outcome, and the individual incidence of each symptom was also collected.16
Secondary outcomes, including time to first analgesic request (defined as the time elapsed between the completion of surgery and the first paracetamol intake) and the number of patients requiring analgesics rescue during in-hospital stay, were collected. Each patient was asked to finish the Self-rating Anxiety Scale (SAS) to assess the degree of anxiety prior to surgery. Additionally, patient baseline characteristics, including age, sex, weight, height, ASA classification, history of general anesthesia and ophthalmic surgery, history of smoking and alcoholism, presence of preoperative morbidity, and preoperative pain score were documented. We also calculated the length of surgery (defined as the duration from surgical incision to the completion of wound suturing) as well as cumulative fentanyl and remifentanil consumption during surgery (fentanyl was converted to an equivalent dose of remifentanil by a potency ratio of 1:1.2).
We measured time to out-of-bed (defined as the time interval between the completion of surgery and the first off-bed activity on the ward). Each patient would be asked to complete a QoR-40 questionnaire on postoperative day 1 to determine their recovery status after surgery.17
We also evaluated safety outcomes, including block-related complications (eg, chemosis, periorbital hematoma, globe perforation, visual impairment, and cranial nerve palsy) after performance of the block. Chemosis was assessed on the number of quadrants affected (no quadrants affected scores 0 and all four quadrants affected scores 4).18 Other postoperative complications that were derived from study case report forms were also collected.
To clarify the influence of MCPB on vision acuity (VA) and periocular pressure in orbital surgical patients, we calculated the changes in uncorrected vision acuity (UCVA), intraocular pressure (IOP) and orbital pressure (Porb) before and 1 day after surgery. UCVA test results were determined using decimal acuity based on the number of letters read correctly and according to the test distance. The decimal acuity was then converted into a logarithm of the minimum angle of resolution (logMAR) scale value, which was calculated by -log (decimal acuity). VA tests do not cover the whole range of the VA scale, and accurate quantitative measurements of “light perception” and “no light perception” were not possible; however, based on a previous study, “counting fingers” could be replaced by a decimal acuity of 0.014 (20/1500), while “hand motion” would correspond to 0.005 (20/4000).19 IOP was measured using a Tono-Pen.20 We also evaluated the Porb after each peribulbar injection with Bowman’s method using digital tonometry as follows: Tn indicates normal pressure, T+1 indicates mildly elevated pressure, T+2 indicates moderately elevated pressure, T+3 indicates extremely high pressure, with the periorbital tissue being considered as hard as stone; conversely, T-1, T-2, T-3 represent slightly low, moderately low, and extremely low intraocular pressure, respectively.
Sample Size Considerations
The minimum difference required to detect non-inferiority on the two primary outcomes are 24 (point·h) referred to AUCNRS, and 13% referred to the incidence of PONV.21,22 To achieve a power of 0.8 with a one-sided α-value of 0.025, 19 patients per group was needed for AUCNRS under the assumption of a non-inferiority margin (NIM) of 24 (point·h) and a common SD value of 24.3 (unpublished preliminary data, October 2019; n = 16) with considering a non-parametric adjustment, while 52 patients per group was required for the incidence of PONV with assuming a NIM of 13% and a reference incidence of PONV in the PCIA group of 6%. Thus, a total sample size of 104 subjects was chosen. The sample sizes were calculated using PASS version 15.0 (NCSS, LLC).
Statistical Analysis
In this intention-to-treat analysis, descriptive statistics were used to present baseline characteristics for the two groups. Data were inspected and assessed for distribution according to the Kolmogorov–Smirnov test and histogram analysis. We expressed data as mean ± standard deviation (SD) for normally distributed variables, median (interquartile range [IQR]) values for non-normally distributed variables, and frequencies with percentages for categorical variables. Normally distributed data were compared between two groups using the independent t test, whereas non-normally distributed data were compared using the Mann–Whitney U-test. Categorical variables were analyzed using the chi-squared test or Fisher exact test as appropriate. In the primary outcome analysis, we assessed non-inferiority of group OFA to group OSA on AUCNRS and incidence of PONV through the first 24 postoperative hours with 1-tailed non-inferiority t tests. Non-inferiority would be claimed if the upper limit of the two-sided 95% confidence interval (CI) for the differences between two groups lied below the predefined NIM. A two-tailed P<0.05 was considered statistically significant. Statistical analysis was performed using SPSS version 23.0 (IBM, Chicago, Illinois, USA).
Results
We included 122 of 130 eligible patients for randomization and analysis (Figure 2). Six were withdrawn from the study based on the predetermined criteria, and two declined to provide informed consent. In addition, the VA assessments of 14 patients who displayed presurgical “light perception” or “no light perception” were inappropriate for analysis, and their visual outcomes were omitted from the study. The patient and surgical characteristics are presented in Table 1.
 |
Table 1 Patient and Surgical Characteristics |
 |
Figure 2 Consolidated Standards of Reporting Trials Statement Flow Diagram. |
Postoperative Analgesic Effects
Overall, postoperative pain control was sufficient in both OFA and OSA groups since the median pain scores were low (<3 points) and comparable at any examined time point (Table 2). NRS pain scores through 24h after surgery were converted over time to examine the AUC as a primary outcome; however, no significant difference in the AUCNRS was noted between the groups. The median difference and 95% CI between OFA and OSA groups was −6 (95% CI, −12 to 6; P = 0.65), and the upper limit was below the predetermined NIM of 24 (point·h). Consequently, OFA was found to be non-inferior to OSA (Figure 3). On discharge to the surgical ward, only 4 patients in the OFA group and 3 patients in the OSA group required additional analgesic rescue. Time to first postoperative analgesic requirement was similar in both groups (Table 2).
 |
Table 2 Comparison of Primary and Secondary Outcomes Between the Groups |
 |
Figure 3 Treatment Differences for AUCNRS (A) and the Incidence of PONV (B) during the First 24 hours after Surgery. Abbreviations: AUC, area-under-The-curve; NRS, numerical rating scale; PONV, postoperative nausea and vomiting; NIM, non-inferiority margin; CI, confidence interval; OSA, opioid-sparing analgesia; OFA, opioid-free analgesia. Notes: The dashed line designates the NIM (∆). The spot shows the median and ratio difference between the two groups for the AUCNRS of pain scores and the incidence of PONV, respectively. The error bars designate the two-sided 95% CI of the differences between the OFA and OSA groups. |
Postoperative Complication and Recovery
PONV is a common complication that is highly associated with opioid use and elevated IOP. With respect to the incidence of PONV during the first 24 postoperative hours, group OFA failed to demonstrate non-inferiority compared to group OSA. In the OFA group, 6.6% of patients experienced PONV compared to 9.8% in the OSA group (ratio difference, 3%; 95% CI, −7% to 14%; P = 0.51), noting that the upper limit exceeded the predefined NIM of 13% (Figure 3). The incidences of nausea (1.6% vs 3.3%, respectively) and vomiting (4.9% vs 6.6%, respectively) were comparable between the groups (Table 2).
No significant differences in other postoperative in-hospital complications, including dizziness, headache, and urinary retention, were found, but we observed that 18% of patients in the OSA group felt dizziness, while just 6.6% in the OFA group did. No patients in either group required unanticipated medical treatment or readmission for any complication after discharge. In terms of recovery quality, time to ambulation was similar between the groups. A statistical difference in QoR-40 scores was observed between the OFA and OSA groups on postoperative day 1 (188 [178–196] vs 181 [169–191], respectively; median difference, 6; 95% CI, 2 to 10; P = 0.005). Among the five dimensions of QoR-40, scores of emotional status, physical comfort, and physical independence were significantly higher in the OFA group than in the OSA group (P = 0.004, P = 0.03 and P = 0.001, respectively) (Figure 4).
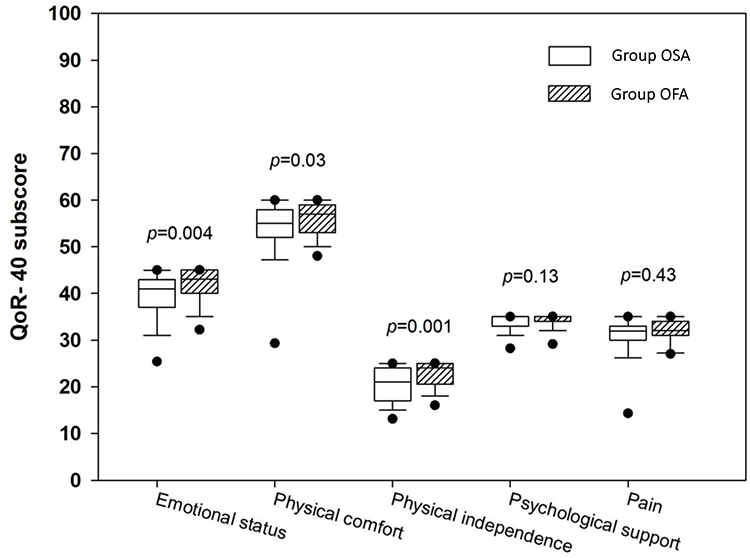 |
Figure 4 Box Plots of QoR-40 Scores at 24 hours after Surgery. Abbreviations: OSA, opioid-sparing analgesia; OFA, opioid-free analgesia; QoR, quality of recovery; IQR, interquartile range. Notes: Box plots represent median (solid lines) and IQR (boxes, 25th and 75th percentiles) values, with the whiskers representing 10th and 90th percentiles and dark spots designating fifth and 95th percentiles, respectively. P < 0.05 was considered statistically significant. |
The Influence on Ocular Features on the Eye to Be Operated
There were no sight-threatening adverse events happen related to the blocks. The difference in UCVA as well as the IOP before and after surgery was comparable among the two groups (Table 2). We also compared the Porb after each peribulbar injection in group OFA to those in group OSA without blockade implementation, and found no significant increases. However, in the group OFA, we observed that 19.7% of patients displayed chemosis after injection, which was possibly attributed to the local anesthetic spreading beneath the conjunctiva.
Discussion
This randomized controlled trial compared the impact of low-dose postoperative opioid use with OFA on short-term outcomes after primary orbital fracture reconstruction. Although our results cannot rule out with certainty the non-inferiority of OFA compared with OSA for the prevention of PONV, the data show that OFA using the MCPB provides adequate postoperative pain relief and early recovery. These findings suggest an opioid-free analgesic regimen with MCPB and NSAIDs can optimize short-term outcomes in primary reconstructions of extensive orbital floor and medial wall fractures, which enhances early postoperative recovery.
Effective regional blocks and multimodal non-opioid analgesic strategies are major components of enhanced recovery after surgery pathways that reduce opioid utilization and improve recovery outcomes.23 Ophthalmic regional blocks have a long tradition of utility in orbital surgery, frequently used for pain control during the surgical procedures. Medial canthus block is an extension of PB, Deruddre and Benhamou first applied this technique as an effective alternative regional block for cataract surgery. It is reported that a single injection of MCPB is as effective as a double-injection percutaneous peribulbar technique and requires less local anesthetic.12 Therefore, we developed a multimodal non-opioid analgesic regimen that includes the combination of MCPB and non-opioid analgesics. This regimen has the potential to provide more comprehensive pain relief by targeting both inflammation and pain signaling pathways. To achieve prolonged analgesia, we employed a single-injection MCPB using 1% ropivacaine (a long-lasting local anesthetic with a mean duration of anesthesia of 21.5 h [range, 19 to 23 h]), which resulted in sustained analgesic effect comparable to the continuous intravenous analgesia of the OSA protocol.24
Of note, we observed a better quality of recovery in patients receiving OFA than OSA, given by higher scores in emotional status, physical comfort, and physical independence of QoR-40.25 It is conceivable that patients with non-opioid multimodal analgesic regimen may avoid side effects of opioids, as demonstrated by a lower incidence rate of dizziness in OFA compared to OSA with opioids. The dizziness may make patients feel distress and uncomfortable, and often impede faster return to independent activities after surgery.
Previous study has demonstrated that PONV is highly associated with the use of opioids.26 Many patients have their first opioid exposure in the perioperative setting and can be expected to benefit from OFA techniques. It has been hypothesized that MCPB with non-opioid analgesics may effectively prevent PONV.27 However, regarding the short-term incidence of PONV, we failed to demonstrate non-inferiority of the OFA group compared to the OSA group in this study, but the incidence of PONV in two groups was both low. This can probably be attributed to multimodal prophylactic drugs including propofol anesthesia and antiemetic prophylaxis (dexamethasone combined with 5-hydroxytryptamine-3 receptor antagonists) given in all participants.28
With unspecific symptoms such as headache, nausea and vomiting, the possibility of acute rise in IOP and Porb caused by the injection of local anesthetic must be considered. In the present study, it was observed that the use of MCPB did not result in a dramatic elevation of IOP or Porb.
This study has several limitations. Firstly, we could not evaluate the real effects of the MCPB by checking the akinesia and pain perception because we performed blocks under general anesthesia. However, we chose to perform blocks at the end of surgery, rather than the beginning, to avoid disrupting the orbital anatomy. Secondly, injecting 3 to 5 mL of local anesthetic into the orbit may cause a dramatic increase in periorbital pressure, requiring operators to pay attention to the changes of IOP and Prob during the injection process.29 Thirdly, using fentanyl may not be a standard protocol to prevent postoperative pain after orbital fracture reconstruction; however, to our knowledge, no optimal multimodal analgesia methods have been presented orsearched in the web of science.
In conclusion, both the OFA and OSA strategies offer effective and safe postoperative pain management following orbital fracture reconstruction. However, the opioid-free multimodal analgesia strategy, which incorporates MCPB and NSAIDs, can improve the quality of early recovery to a greater extent.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Study approval was obtained from the Institutional Review Board of Zhongshan Ophthalmic Center, Sun Yat-sen University (approval number: 2019KYPJ154). Informed consent was obtained from all individual participants or their legal guardians prior to their participation.
Acknowledgments
We would like to give special thanks to Prof. Ling Jin (senior statistician of Zhongshan Ophthalmic Center) for assistance with statistical analysis of this study. This study was supported by the Natural Science Foundation of Guangdong Province, China (2021A1515010553), and the clinical research project of Zhongshan Ophthalmic Center of Sun Yat-sen University (3030901011175). The sponsors had no role in the study design, survey process, data analysis, or manuscript preparation. Rui Zhang, Yongjian Mai, and Huijing Ye are co-first authors for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hsieh TY, Vong S, Strong EB. Orbital reconstruction. Curr Opin Otolaryngol Head Neck Surg. 2015;23(5):388–392. doi:10.1097/MOO.0000000000000190
2. Ye H, Chen R, Lian X, et al. Risk factors associated with postoperative pain and discomfort in oculoplastic surgery with general anesthesia: a prospective study. J Pain Res. 2018;11:407–415. doi:10.2147/JPR.S156104
3. Shanthanna H, Ladha KS, Kehlet H, Joshi GP. Perioperative Opioid Administration. Anesthesiology. 2021;134(4):645–659. doi:10.1097/ALN.0000000000003572
4. Dumbarton TC. Anesthésie régionale pour les cas pédiatriques complexes: progrès dans l’analgésie avec épargne opioïde [Regional anesthesia in complex pediatric patients: advances in opioid-sparing analgesia]. Can J Anaesth. 2024;71(6):727–730. doi:10.1007/s12630-023-02616-x
5. Charlson ES, Feng PW, Bui A, Grob S, Tao JP. Opioid prescribing patterns among American society of ophthalmic plastic and reconstructive surgery members in the medicare part D database. Ophthalmic Plast Reconstr Surg. 2019;35(4):360–364. doi:10.1097/IOP.0000000000001266
6. Mauermann E, Clamer D, Ruppen W, Bandschapp O. Association between intra-operative fentanyl dosing and postoperative nausea/vomiting and pain: a prospective cohort study. Eur J Anaesthesiol. 2019;36(11):871–880. doi:10.1097/EJA.0000000000001081
7. Brummett CM, Waljee JF, Goesling J, et al. New persistent opioid use after minor and major surgical procedures in US adults [published correction appears in JAMA Surg. 2019 Mar 1;154(3):272. doi: 10.1001/jamasurg.2018.5476]. JAMA Surg. 2017;152(6):e170504. doi:10.1001/jamasurg.2017.0504
8. Patel S, Sternberg P Jr. Association between opioid prescribing patterns and abuse in ophthalmology. JAMA Ophthalmol. 2017;135(11):1216–1220. doi:10.1001/jamaophthalmol.2017.4055
9. Kolomeyer AM, Yu Y, VanderBeek BL. Association of opioids with incisional ocular surgery. JAMA Ophthalmol. 2019;137(11):1283–1291. doi:10.1001/jamaophthalmol.2019.3694
10. Alexander JC, Patel B, Joshi GP. Perioperative use of opioids: current controversies and concerns. Best Pract Res Clin Anaesthesiol. 2019;33(3):341–351. doi:10.1016/j.bpa.2019.07.009
11. Brahma AK, Pemberton CJ, Ayeko M, Morgan LH. Single medial injection peribulbar anaesthesia using prilocaine. Anaesthesia. 1994;49(11):1003–1005. doi:10.1111/j.1365-2044.1994.tb04324.x
12. Deruddre S, Benhamou D. Medial canthus single-injection peribulbar anesthesia: a prospective randomized comparison with classic double-injection peribulbar anesthesia. Reg Anesth Pain Med. 2005;30(3):255–259. doi:10.1016/j.rapm.2005.01.008
13. Guerrier G, Rothschild PR, Lehmann M, Azan F, Baillard C. Impact of video technology for improving success of medial canthus episcleral anesthesia in ophthalmology. Reg Anesth Pain Med. 2017;42(6):757–759. doi:10.1097/AAP.0000000000000658
14. Oliveira AR, Oliveira JBR, Kronbauer A, Severo N, Picetti E. Medial canthus single injection Peribulbar anesthesia using 13x0,45mm needle: technique presentation. Int J Anes & Rel. 2017;1:23–27.
15. Melo MAP, Garcia EA. Chandler maneuver following peribulbar anesthesia for reduction of intraocular pressure in facectomy. Acta Medica Misericordæ. 2001;4:29–31.
16. Kim EJ, Shim JK, Soh S, Song JW, Lee SR, Kwak YL. Patient-controlled analgesia with propacetamol-fentanyl mixture for prevention of postoperative nausea and vomiting in high-risk patients undergoing spine surgery: a randomized controlled trial. J Neurosurg Anesthesiol. 2016;28(4):316–322. doi:10.1097/ANA.0000000000000252
17. Gornall BF, Myles PS, Smith CL, et al. Measurement of quality of recovery using the QoR-40: a quantitative systematic review. Br J Anaesth. 2013;111(2):161–169. doi:10.1093/bja/aet014
18. Gill VS, Presland AH, Lord JA, Bunce C, Xing W, Charteris DG. Two-quadrant high-volume sub-Tenon’s anaesthesia for vitrectomy: a randomised controlled trial. Br J Ophthalmol. 2012;96(2):189–192. doi:10.1136/bjo.2010.198374
19. Schulze-Bonsel K, Feltgen N, Burau H, Hansen L, Bach M. Visual acuities “hand motion” and “counting fingers” can be quantified with the Freiburg Visual Acuity Test. Invest Ophthalmol Vis Sci. 2006;47(3):1236–1240. doi:10.1167/iovs.05-0981
20. Raina UK, Rathie N, Gupta A, Gupta SK, Thakar M. Comparison of Goldmann applanation tonometer, Tono-Pen and noncontact tonometer in children. Oman J Ophthalmol. 2016;9(1):22–26. doi:10.4103/0974-620X.176096
21. Olsen MF, Bjerre E, Hansen MD, et al. Pain relief that matters to patients: systematic review of empirical studies assessing the minimum clinically important difference in acute pain. BMC Med. 2017;15(1):35. doi:10.1186/s12916-016-0775-3
22. Chae D, Kim SY, Song Y, et al. Dynamic predictive model for postoperative nausea and vomiting for intravenous fentanyl patient-controlled analgesia. Anaesthesia. 2020;75(2):218–226. doi:10.1111/anae.14849
23. Wu CL, King AB, Geiger TM, et al. American society for enhanced recovery and perioperative quality initiative joint consensus statement on perioperative opioid minimization in opioid-naïve patients. Anesth Analg. 2019;129(2):567–577. doi:10.1213/ANE.0000000000004194
24. Keramidas EG, Rodopoulou SG. Ropivacaine versus lidocaine in digital nerve blocks: a prospective study. Plast Reconstr Surg. 2007;119(7):2148–2152. doi:10.1097/01.prs.0000260725.33655.88
25. Guimarães-Pereira L, Costa M, Sousa G, Abelha F. Quality of recovery after anaesthesia measured with QoR-40: a prospective observational study. Braz J Anesthesiol. 2016;66(4):369–375. doi:10.1016/j.bjane.2014.11.010
26. Horn CC, Wallisch WJ, Homanics GE, Williams JP. Pathophysiological and neurochemical mechanisms of postoperative nausea and vomiting. Eur J Pharmacol. 2014;722:55–66. doi:10.1016/j.ejphar.2013.10.037
27. Frauenknecht J, Kirkham KR, Jacot-Guillarmod A, Albrecht E. Analgesic impact of intra-operative opioids vs. opioid-free anaesthesia: a systematic review and meta-analysis. Anaesthesia. 2019;74(5):651–662. doi:10.1111/anae.14582
28. Gan TJ, Belani KG, Bergese S, et al. Fourth consensus guidelines for the management of postoperative nausea and vomiting [published correction appears in Anesth Analg. 2020;131(5):e241. doi: 10.1213/ANE.0000000000005245]. Anesth Analg. 2020;131(2):411–448. doi:10.1213/ANE.0000000000004833
29. Theusinger OM, Spahn DR, Chaloupka K. Postoperative pain and vomiting after orbital wall surgery in trauma. Eur J Anaesthesiol. 2008;25(8):695–697. doi:10.1017/S0265021508004122
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.