")
Back to Journals » Clinical Ophthalmology » Volume 18
A Randomized Controlled Trial Comparing STREAMLINE Canaloplasty to Trabecular Micro-Bypass Stent Implantation in Primary Open-Angle Glaucoma
Authors Goldberg DF, Orlich C, Flowers BE, Singh IP, Tyson S, Seibold LK, ElMallah MK, Ison EM, Harbin M , Reynolds H, Kahook MY
Received 8 June 2024
Accepted for publication 2 October 2024
Published 16 October 2024 Volume 2024:18 Pages 2917—2928
DOI https://doi.org/10.2147/OPTH.S481945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Damien F Goldberg,1 Claudio Orlich,2 Brian E Flowers,3 Inder P Singh,4 Sydney Tyson,5 Leonard K Seibold,6 Mohammed K ElMallah,7 Elysia M Ison,8 Med Harbin,8 Heather Reynolds,8 Malik Y Kahook9
1Wolstan & Goldberg Eye Associates, Torrance, CA, USA; 2Clinica 20/20, San Jose, Costa Rica; 3Ophthalmology Associates, Fort Worth, TX, USA; 4The Eye Centers of Racine & Kenosha, Racine, WI, USA; 5Eye Associates & SurgiCenter of Vineland, Vineland, NJ, USA; 6Department of Ophthalmology, University of Colorado Eye Center, Aurora, Colorado, USA; 7Ocala Eye, Ocala, FL, USA; 8New World Medical, Rancho Cucamonga, CA, USA; 9Department of Ophthalmology, University of Colorado Anschutz Medical Campus, Aurora, Colorado, USA
Correspondence: Malik Y Kahook, Department of Ophthalmology, University of Colorado Anschutz Medical Campus, Aurora, Colorado, USA, Tel +1 720 848 2501, Email [email protected]
Purpose: To report interim results of the VENICE study, a multi-center, randomized, controlled trial (RCT) comparing STREAMLINE Surgical System (STREAMLINE) canaloplasty with iStent inject W (iStent W) implantation in patients with mild-to-moderate primary open-angle glaucoma (POAG) undergoing phacoemulsification.
Patients and Methods: Safety and efficacy analyses involving the first 72 randomized eyes are included in this report. Following pre- (Screening) and post-medication washout (Eligibility) visits, one eye per subject was randomized 1:1 to STREAMLINE or iStent W after undergoing uncomplicated phacoemulsification. Subjects were evaluated postoperatively at Day 1, Week 1, Month 1, 3, and 6. Intraocular pressure (IOP) measurements, number of IOP-lowering medications, and adverse events (AEs) were assessed at each follow-up visit.
Results: Seventy-two eyes were randomized; 35 underwent STREAMLINE canaloplasty and 37 were implanted with the iStent W. Seventy eyes completed their 6-month follow-up. Both the mean morning post-washout Baseline IOP between STREAMLINE 24.86± 3.05 mmHg and iStent W 25.16± 3.41 mmHg and the mean IOP at 6 months between STREAMLINE eyes 16.52± 3.63 mmHg and iStent W eyes 16.08± 3.19 mmHg were not statistically significantly different (p=0.691 and 0.596, respectively). At 6 months, more eyes were on zero glaucoma medications in the STREAMLINE group (81.8%) compared to the iStent W group (78.4%). In medication-free eyes, the mean IOP was reduced from 24.80± 2.79 mmHg to 16.00± 3.40 mmHg and 24.60± 3.18 mmHg to 15.80± 2.21 mmHg in the STREAMLINE and iStent W groups, respectively (p=0.752). Both groups showed reduction in IOP-lowering medications at every visit, compared to pre-washout (Screening), with STREAMLINE resulting in numerically fewer medications 0.20± 0.48 compared to iStent W 0.40± 0.79 at 6 months (P=0.384). AEs were mild and self-limited.
Conclusion: To our knowledge, the VENICE trial is the first RCT involving canaloplasty. These interim findings demonstrated comparable IOP and medication reduction between STREAMLINE canaloplasty and iStent W implantation, when combined with phacoemulsification.
Keywords: primary open-angle glaucoma, POAG, STREAMLINE, iStent inject W, canaloplasty, microinvasive glaucoma surgery, MIGS
Introduction
According to a meta-analysis performed by the Vision Loss Expert Group of the Global Burden of Disease Study, glaucoma has remained the leading cause of irreversible blindness globally over the last two decades with 3.61 million people blind and 4.14 million visually impaired in 2020.1 The risk factors and pathophysiology associated with glaucoma have been well-described in previous landmark studies, with intraocular pressure (IOP) being the only modifiable risk factor to slow or prevent visual field deterioration.2,3 Historically, the first line of treatment for IOP control in glaucoma has been the use of topical pressure lowering medication drops followed by laser trabeculoplasty and eventually invasive surgery. The undesirable side effects and lack of compliance with topical drops, along with the adverse events (AEs) and economic burden of more invasive procedures, resulted in a desire for safer, less invasive, and predictably efficacious treatments for glaucoma.4–6
The introduction of micro-invasive glaucoma surgeries (MIGS) addressed the unmet need of safer IOP lowering with less invasive approaches compared to older filtration surgery techniques.7–9 MIGS, as defined by the American Glaucoma Society (AGS), are a broad group of procedures “designed to lower IOP by improving aqueous outflow with minimal disruption to the sclera or conjunctiva with or without an implanted device, or by reducing aqueous production selectively”.10 Since the approval of Trabectome (NeoMedix, Tustin, CA) in 2004 and the first generation iStent in 2012 (Glaukos, Aliso Viejo, CA), MIGS have become a data-driven method of safely and effectively treating patients with various forms of glaucoma, both standalone as well as combined with cataract surgery.11,12 Peer reviewed publications of MIGS treatments have documented safety and efficacy in patients with open-angle glaucoma (OAG), secondary glaucomas including pigmentary and pseudoexfoliative glaucoma,12,13 and across the continuum from early to end-stage disease.9,13–16
MIGS studies have been reported on for over two decades and the data comparing the various procedures in head-to-head randomized clinical trials (RCTs) continues to mount with increasing information that guide treatment algorithms and clinical decision-making.17,18 This report focuses on the RCT findings of the VENICE study which prospectively compares safety and efficacy of STREAMLINE Surgical System (STREAMLINE, New World Medical, Rancho Cucamonga, CA) canaloplasty to iStent inject W when combined with cataract extraction.
Materials and Methods
Study Design
The VENICE study was designed to evaluate the safety and efficacy of STREAMLINE canaloplasty compared to iStent inject W implantation at the time of cataract extraction. Both procedures were performed after successful uncomplicated cataract surgery with planned 24-Month follow-up. This study is currently enrolling with subjects recruited from approximately 20 sites in the United States and Latin America. The study protocol was reviewed and approved by a central Institutional Review Board in the US (Sterling IRB), and study was approved by the ethics committee in Costa Rica (Instituto Costarricense de Investigaciones Clinical Comite Etico Cientifico). The study conduct follows the tenets of the Declaration of Helsinki with written informed consent of subjects. The study is registered with the National Library of Medicine database (clinicaltrials.gov, NCT05280366).
The iStent inject W was approved by the FDA in 2018 and contains two preloaded trabecular meshwork (TM) bypass stents that are manufactured from titanium and are coated with heparin. The iStent inject W’s two-stent system creates a patent pathway through the TM and into the canal of Schlemm (CS).19 The STREAMLINE Surgical System (Figure 1A) received FDA clearance in 2021. This single-use disposable device consists of a surgical grade stainless-steel dispensing inner cannula with a retractable outer sleeve and a hand-held body that houses a pump for dispensing ophthalmic viscoelastic fluid. The STREAMLINE device is designed to perform up to 8 applications of viscoelastic fluid into the CS. Each application delivers approximately 7 µL of viscoelastic for a total volume of 56 µL.20
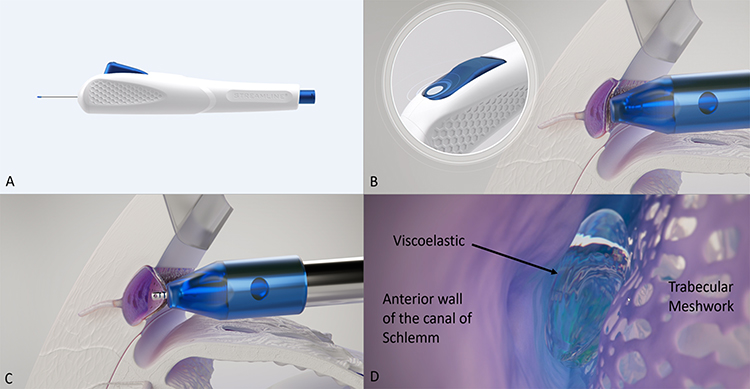 |
Figure 1 The STREAMLINE® Surgical System (A) is designed with a retractable sleeve that indents the trabecular meshwork (B) followed by actuation of the button leading to the inner cannula catheterizing the canal of Schlemm (C) and delivering ~7ul of viscoelastic across several clock hours of the canal through two outlets on either side of the cannula (D). |
Inclusion and Exclusion Criteria
Only one eye per subject was randomized for this study. Patients were eligible to participate in the study if they met the following criteria: were able to understand a written informed consent and able and willing to comply with the protocol, were 22 years or older, had visually significant cataract scheduled for phacoemulsification surgery, diagnosed with mild-to-moderate primary open-angle glaucoma with angles that were non-occludable per Shafer grading, were on 1 to 3 topical glaucoma medications at Screening, and potential for improvement in best corrected visual acuity (BCVA) after cataract surgery.
Eyes that had prior glaucoma surgery (CyPass, Xen, iStent, Express, Hydrus, glaucoma drainage device, canaloplasty, goniotomy, deep sclerotomy, trabeculotomy, trabeculectomy, endoscopic cyclophotocoagulation or cyclophotocoagulation), filtering or implantable glaucoma devices, previous laser peripheral iridotomy or Argon Laser Trabeculoplasty (ALT) were excluded from the study. Selective Laser Trabeculoplasty (SLT) was permitted if performed >3 months prior. Eyes with central corneal thickness less than 480µm or more than 620µm, previous intraocular surgery within the last 6 months, use of any medication that would be contraindicated for a glaucoma surgical procedure, use of oral hypotensive medication treatment for glaucoma, participation (≤30 days prior to Baseline) in an interventional trial which could have a potential effect on the study outcome or any condition, in the investigator’s judgement, that would predispose the subject to significant risk of complications or significant vision loss at medication washout and throughout the study were also excluded. Additional exclusion criteria included eyes with severe or advanced glaucoma in the study eye characterized by: cup/disc ratio (C/D) greater than 0.80 (horizontal or vertical measurement); severe central visual field loss defined as a sensitivity ≤10 dB in at least 2 of the 4 visual field test points closest to the point of fixation; and anyone who could not safely undergo a washout of previously used IOP-lowering medication. Lastly, the non-study eye could not have a BCVA worse than 20/80.
Study participants were consented and examined at a Screening visit to determine if they met inclusion and exclusion criteria before washing out of medications. Table 1 shows the required minimum washout period for each IOP-lowering medication classification. After appropriate washout, subjects returned for an Eligibility visit where diurnal IOP, Goldmann applanation tonometry measurements taken 4 ± 1 hours apart between 8AM and 4PM, was measured. Subjects that reached an IOP of 22–34 mmHg (inclusive) were randomized 1:1 to either the STREAMLINE or iStent inject W group combined with cataract surgery. Subjects who did not meet the inclusion and exclusion criteria were categorized as screen failure.
 |
Table 1 IOP-Lowering Medication Washout Schedule |
Randomization
All eligible subjects were given a randomization number which dictated the treatment group and randomization numbers could not be reused. On the day of surgery, after successful uncomplicated cataract extraction, subjects were randomized to either STREAMLINE canaloplasty or iStent inject W implantation based on their randomization number. STREAMLINE canaloplasty and iStent inject W implantation were performed per the instructions for use (IFU) as described below. All surgical procedures were performed by trained ophthalmologists with experience in angle-based surgical procedures.
Procedures
For the iStent inject W implantation, the microscope was tilted 35–45 degrees towards the surgeon and the patient’s head was turned approximately 35–45 degrees away from the surgeon. After proper positioning, a gonioprism was used to visualize the TM. The injector was inserted through the same temporal corneal incision used to perform cataract surgery and centered on the nasal TM. Light pressure was applied and the delivery button was held down to penetrate the tissue with the trocar and deploy the implant. A second implant was inserted at least two clock hours away from the first stent implant in all iStent cases.19
For the STREAMLINE Surgical System (Figure 1A) canaloplasty, viscoelastic was loaded into the handpiece and the microscope was tilted 35–45 degrees towards the surgeon and the patient’s head was turned approximately 35–45 degrees away from the surgeon. The handpiece was introduced through the cataract surgery incision and advanced across the anterior chamber to the nasal angle. The outer sleeve was positioned against the TM under direct gonioscopic visualization to indent the tissue (Figure 1B). The actuator button was then fully depressed, retracting the outer sleeve and allowing the inner cannula to enter the CS (Figure 1C). The button was held in the depressed position for 2 seconds to allow the viscoelastic to be delivered (Figure 1C and D). The tip was then withdrawn from the TM and the actuator button released. The procedure was repeated, spacing each application approximately one clock hour away from prior applications with 3–8 applications performed in each eye.20 While STREAMLINE is a multiple function device and allows for incisions in the TM to be performed in addition to the canaloplasty, the VENICE trial was done exclusively with canaloplasty without additional incisions made in the TM.
Visit Assessments
The study was designed to include follow-up visits on Day 1, Week 1, Months 1, 3, 6, 9, 12, 18 and 24. Additional study exam procedures included BCVA, slit lamp, gonioscopy, dilated fundus exam, automated perimetry, pachymetry and endothelial cell density (ECD). All serious non-ocular and all study eye AEs were collected. Any changes in medical or ocular history from Screening and all concomitant systemic and ocular medications were recorded. This manuscript will report findings from Screening, Eligibility, Surgery Day, Day 1, Week 1, and Months 1 through 6 for the first 72 randomized subjects that are eligible for analysis.
Intraocular Pressure & Masking
IOP measurements were performed in both eyes using a calibrated Goldmann applanation tonometer at all visits. To minimize bias, a 2-person method that involved an operator and a reader was used to measure IOP. The operator was responsible for measuring IOP, while the reader recorded the results and was masked to the subject’s treatment group for the entire study. An alternate IOP reader was required for each site should the main IOP reader become unmasked. Two consecutive IOP measurements were taken for each eye, and the applanation probe was withdrawn from the eye between the two measurements. If the difference between the 2 measurements differed by ≤4 mmHg, the average of the measurements was determined to be the mean IOP for that eye. If the two measurements for the same eye differed by >4 mmHg, a third measurement was taken. The two IOP measurements closest to each other were averaged. If the three measurements differed by equal amounts, all 3 measurements were averaged. Mean IOP values were rounded up to the next whole number if the value was equal to or greater than 0.5 mmHg and rounded down if less than 0.5 mmHg.
Statistical Analysis
In this interim report, data were analyzed as part of the planned safety monitoring after at least 60 subjects completed the Month 6 visit. IOP and number of ocular hypotensive medications were summarized by visit. Safety outcomes included intraoperative and postoperative AEs, as well as assessments of BCVA, slit-lamp exam, and ECD data. Subject demographics and Baseline characteristics were compared between the two treatment groups. Continuous variables (e.g., age) were summarized as the mean and standard deviation. The t-test was used to compare the means of two treatment groups for each continuous variable to see if there was a significant difference (t-test p-value less than 0.05). Categorical variables (e.g., sex) were summarized as counts and percentages. The chi-square test was used to examine the association or discrepancy between two treatment groups and the testing p-value was reported.
Results
IOP and IOP-Lowering Medications
At the time of this 6-month analysis, 105 subjects were enrolled (screened), of whom 72 met the inclusion/exclusion criteria. Each of the 72 subjects had one eye randomized, totaling 35 eyes in the STREAMLINE group and 37 eyes in the iStent inject W group. STREAMLINE eyes received an average of 4.43 ± 0.96 applications, each spaced at least one clock hour apart and all iStent inject W eyes successfully received two stent implants. The demographic (Table 2) and preoperative (Table 3) characteristics for both study groups were similar. The mean age was 70.10 ± 7.67 and 70.60 ± 7.07 years in the STREAMLINE and iStent groups, respectively (p = 0.628). The unmedicated diurnal IOP at Eligibility (the Baseline post-washout IOP), calculated as the mean and standard deviation of all IOP measurements taken throughout the entire day, was 24.50 ± 3.02 mmHg in the STREAMLINE group and 25.00 ± 3.23 mmHg in the iStent inject W group, with no statistically significant difference between groups (p = 0.465). Analysis of IOP across study visits (Table 4) compared morning IOP values at Eligibility to morning IOP values at 6 months since full diurnal IOP was not obtained at Month 6 (planned at Month 12). The mean morning Baseline post-washout IOP values were 24.86 ± 3.05 mmHg for STREAMLINE and 25.16 ± 3.41 mmHg for iStent inject W. Overall, the IOP lowering efficacy and reduction in dependence on IOP lowering medications were similar between the two groups throughout the 6-month follow-up period (Table 4 and Figure 2).
 |
Table 2 Subject Demographics |
 |
Table 3 Pre-op Characteristics in Study Eyes at Screening (Visit 1, Before Medication Washout) |
 |
Table 4 Intraocular Pressure Measurements at Each Study Visit |
 |
Figure 2 Mean IOP at pre-washout Screening, post-washout Baseline and postoperative visits. Error bars represent the standard deviation. There was no statistically significant difference between the STREAMLINE and iStent inject W groups across all visits up to postoperative Month 6 follow-up visit. *Subject missed visit. **One subject died and one subject missed visit. Abbreviation: IOP, intraocular pressure. |
The STREAMLINE group required numerically less medications for IOP control at every postoperative follow-up visit (Table 5 and Figure 3). At Week 1, more eyes were on zero medications in the STREAMLINE group (34/35, 97.1%) compared to the iStent inject W group (33/37, 89.2%). At Month 1, 33/35 (94.3%) of the STREAMLINE group eyes were on zero or one medication, compared to 33/37 (89.2%) of the iStent inject W group. At Month 3, 33/34 (97.1%) of the STREAMLINE group eyes were on zero or one medication compared to 34/37 (91.9%) in the iStent inject W group. At Month 6, the STREAMLINE group maintained a higher proportion of eyes on zero or one medication (32/33, 97.0%) compared to in the iStent Inject W group (34/37, 91.9%) and 2/37 (5.4%) eyes were on 3 medications in the iStent inject W group while none of the STREAMLINE eyes required 3 medications for IOP control. Both the STREAMLINE and iStent inject W groups had a statistically significant decrease in number of medications from Screening to Month 6 (p<0.0001 for each group). An analysis of eyes that were off of all IOP-lowering medications at 6 months is shown in Table 6. These data show that 81.8% (27/33) of STREAMLINE eyes and 78.4% (29/37) of iStent inject W eyes were on zero IOP-lowering medications. The mean IOP was reduced from 24.80 ± 2.79 to 16.00 ± 3.40 and from 24.60 ± 3.18 to 15.80 ± 2.21 in the STREAMLINE and iStent inject W groups, respectively (p = 0.752). This equates to a total IOP reduction of 8.8 mmHg for both groups and highlights that eyes remaining off all medications experienced the same level of pressure decrease regardless of the surgical approach.
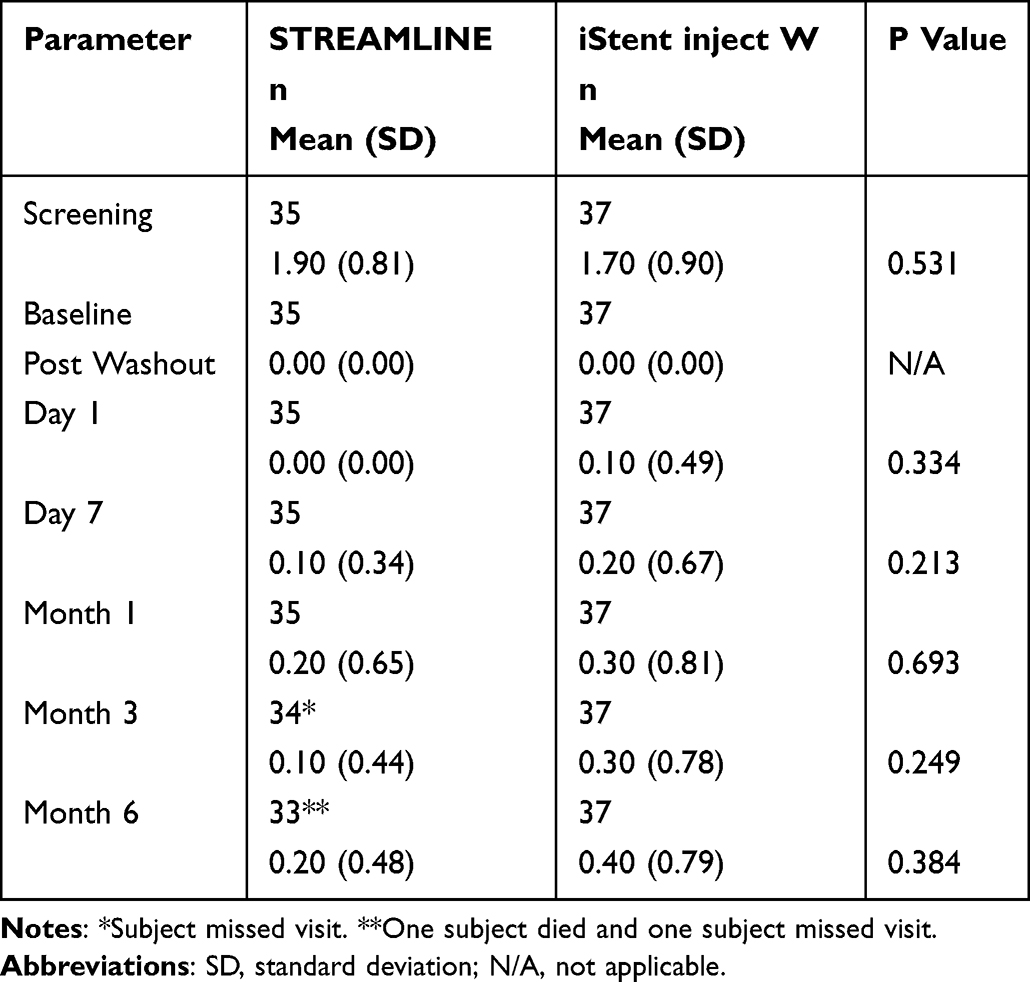 |
Table 5 Medication Use at Each Study Visit |
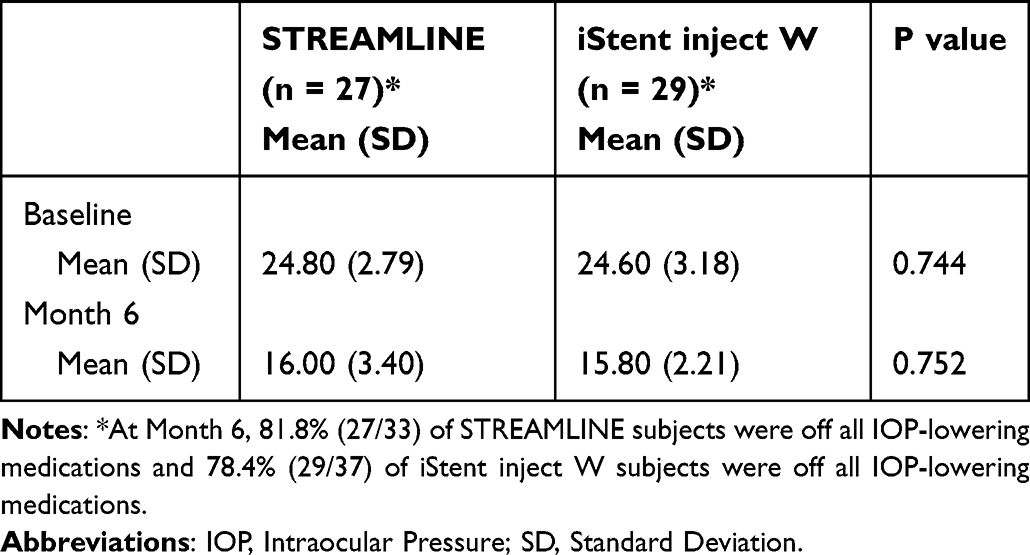 |
Table 6 Analysis of IOP for Subjects off of All IOP-Lowering Medications |
 |
Figure 3 Mean number of IOP-lowering medications at pre-washout Screening and each postoperative visit. Error bars represent standard deviation. There was no statistically significant difference between the STREAMLINE and iStent inject W groups in mean glaucoma medication reduction from pre-washout Screening to postoperative Month 6 follow-up visit. *Subject missed visit. **One subject died and one subject missed visit. Abbreviation: IOP, intraocular pressure. |
Safety
LogMAR BCVA at Screening for STREAMLINE was 0.60 ± 0.24 and iStent was 0.60 ± 0.22, (p = 0.762). All subjects underwent uncomplicated cataract surgery before the randomization and BCVA improved to 0.90 ± 0.21 for STREAMLINE and 0.90 ± 0.19 for iStent inject W. ECD measurements were completed at a subset of sites using an Automated Non-contact Specular Microscope. There were 21 subjects in the STREAMLINE group and 25 subjects in the iStent inject W group that were able to have ECD measured at Screening. For STREAMLINE, the mean ECD was 2642.20 ± 218.98 cells per square millimeter (cells/mm2) at Screening and decreased to 2158.10 ± 537.18 cells/mm2 by Month 6. Three eyes in the STREAMLINE group did not have ECD measurements at Month 6. For iStent inject W, 25 eyes had ECD measurements, with a mean of 2570.00 ± 264.65 cells/mm2 at Screening decreasing to 2181.90 ± 499.77 cells/mm2 at Month 6. These findings are consistent with ECD changes after cataract surgery alone and also in line with past MIGS studies.21
AEs were generally mild and self-limited. Two eyes (one in the STREAMLINE group and one in the iStent inject W group) had early mild corneal edema with transiently elevated IOP and resolved with short-term use of topical therapeutics. One eye in the STREAMLINE group had late corneal edema with elevated eye pressure that occurred 30 days postoperatively and also resolved with short-term use of topical therapeutics. Two eyes (one in the STREAMLINE goup and one in the iStent inject W group) had early elevated IOP which resolved without sequelae after paracentesis tap and topical medication. Four study eyes in the STREAMLINE group were noted to have cell and flare 4 to 9 weeks after surgery. The inflammation was unrelated to the STREAMLINE device or canaloplasty procedure per the investigator; 3 eyes responded to topical therapy and AE was resolved. One eye experienced recurrent iritis post-surgery with continued close follow-up and work-up with rheumatology for etiology. One eye in the STREAMLINE group was noted to have blood in the angle at postoperative Day 1, but this resolved without sequela. Another eye in the STREAMLINE group was noted to have a vitreous floater postoperatively that was unrelated to the device or procedure. Lastly, one subject in the STREAMLINE group died for reasons unrelated to the study (cancer-related) after their Month 3 visit. One eye in the iStent inject W group had mild cystoid macular edema which resolved with topical treatment. A second eye in the iStent inject W group was diagnosed with a branch retinal vein occlusion, epiretinal membrane, and moderate cystoid macular edema occurring 3 months postoperatively (deemed by the investigator to be unrelated to the procedure).
Discussion
In this analysis, we evaluated the short-term, 6-month, safety and IOP-lowering efficacy of the STREAMLINE Surgical System versus iStent inject W when combined with cataract surgery in patients with mild to moderate, primary open-angle glaucoma (POAG). The IOP-lowering efficacy and reduction of IOP-lowering medications were similar between groups. AEs were also similar between groups and generally categorized as minor and unrelated to the devices used. These findings are similar to data reported on other MIGS devices with 6 months of follow-up and indicate that both STREAMLINE canaloplasty and iStent inject W are effective options for treating mild-to-moderate POAG when combined with cataract extraction (Table 7).15,22–28
 |
Table 7 Comparison of Month 6 IOP & Glaucoma Medication Reduction in Other MIGS Studies |
The American Academy of Ophthalmology (AAO) describes canaloplasty as “Cannulation of Schlemm’s canal (SC) with a catheter or stent with either an internal or external approach for at least three clock hours with an injection of viscoelastic while removing the stent to dilate the canal would be a canaloplasty. Alternatively, viscoelastic injections made via three or more punctures of the TM spanning at least three clock hours (90 degrees) to dilate SC should also qualify as canaloplasty.”29 The STREAMLINE Surgical System administers approximately 7 µl of ophthalmic viscoelastic device (OVD) per application, with 3–8 applications spaced about one clock hour apart, resulting in a total OVD volume of 21 to 56 µl.20 This volume is comparable to or exceeds that used by other canaloplasty devices.30,31 The goal of using the STREAMLINE Surgical System for canaloplasty is to lower IOP and reduce reliance on IOP-lowering medications by addressing the main blockage points in the TM, SC, and the distal collector channels. The canaloplasty procedure has been found to be safe and effective, and similar to other MIGS procedures, both standalone and combined with cataract extraction, in multiple studies and in various forms of glaucoma.15,22–28
Table 7 contains information about various MIGS procedures including both IOP-lowering efficacy and efficiency at decreasing dependence on IOP-lowering medications. One example is from the GEMINI study, reporting prospective safety and efficacy outcomes of 360° canaloplasty and 180° trabeculotomy using the OMNI surgical system with concomitant phacoemulsification in 137 patients with OAG. Results at 6 months revealed 78% of patients were medication-free with IOP of 14.5 mmHg and a mean reduction of 9 mmHg from Baseline. They reported non-serious AEs such as hyphema in 7 (4.6%) patients, IOP elevation in 3 (2.0%), blepharitis in 2 (1.3%), cystoid macular edema in 1 (0.7%) and vitreous hemorrhage in 1 (0.7%) patient.22 Hirsch and colleagues reported similar findings with a retrospective review of the OMNI system, in which case both canaloplasty and trabeculotomy were completed, showing effective IOP reduction and meaningful medication reduction for up to 12 months postoperatively.23 They included two groups (overall n=81) in the study: Group 1 (Baseline IOP over 18mmHg) and Group 2 (Baseline IOP equal to or under 18mmHg). The mean IOP was reduced in Group 1 from 21.9 to 15.1 mmHg (P < 0.0001) and in Group 2 from 14.1 to 13.4 mmHg (p = 0.318). Mean medication use decreased from 2.0 ± 1.3 to 1.1 ± 1.1 and from 1.6 ± 1.3 to 0.9 ± 1.2 in Groups 1 and 2, respectively. AEs were typical for cataract or angle surgery: mild inflammation (11%), IOP spikes (IOP >10 mmHg above Baseline at >1 month, 5%), and hyphema (4%). It is noteworthy that both the ROMEO and GEMINI studies combined canaloplasty with trabeculotomy;22,23 whereas, the prospective RCT data from this report (VENICE) only involved canaloplasty using the STREAMLINE device while achieving similar IOP-lowering effect and medication reduction across all three studies at the 6-month timepoint.
Limitations of this report include the relatively shorter follow-up period, while its strengths include the RCT design, comparison of two commonly used canal-based MIGS approaches and the use of surgeons from across various regions of the world and a diverse patient population. This study is ongoing and 12-month results for this cohort will be reported in the future to help better understand the long-term efficacy and safety for both STREAMLINE canaloplasty and iStent inject W implantation to treat glaucoma when combined with cataract surgery.
Conclusion
The 6-month results of the first 72 subjects randomized in the VENICE prospective RCT comparing STREAMLINE canaloplasty to iStent inject W implantation when combined with cataract extraction show similar safety and IOP lowering efficacy. Overall reduction in dependence on IOP-lowering medications was comparable with a numerically larger reduction in the STREAMLINE group. To our knowledge, this study is the first to directly compare the safety and efficacy of STREAMLINE canaloplasty to iStent inject W implantation at the time of cataract extraction.
Data Sharing Statement
Study data are available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to thank Theresa Landry, PhD for study design, Adelina Paunescu, PhD and team (Medi Ink Solutions, LLC) for providing data analysis, and the New World Medical clinical research team for their support and dedication.
The VENICE Study Investigators: Damien F Goldberg, Claudio Orlich, Brian E Flowers, Inder P Singh, Sydney Tyson, Leonard K Seibold, Mohammed K ElMallah, William J Flynn, Adam J Jorgensen, Ranjan Malhotra, Kenneth W Olander, Gagan K Sawhney, and Steven D Vold.
Funding
This clinical study was sponsored by New World Medical (Rancho Cucamonga, CA).
Disclosure
EMI, HR, and MH are employees of New World Medical. Inc. and participated in the design and conduct of the study, the collection, management, and analysis of data, and the preparation of the manuscript. DFG has financial interests and/or receives consulting fees with New World Medical, Glaukos, AbbVie, Alcon, Johnson & Johnson and Ocular Science. CO receives consulting fees from New World Medical. BEF receives consulting from New World Medical, Glaukos, Alcon, Sight Sciences, iStar Medical, Iantrek and Sanoculis, and research grants from NiCox; IPS receives consulting, research and/or speaker fees from New World Medical, Glaukos, AVG, Alcon, Allergan, B+L, Elios, IStar Medical, Lumibird, Nova Eye, Ocular Therapeutix, Radius, Rayner, Sight Sciences, Tarsus and Thea. LKS receives consulting fees from New World Medical, Allergan and Oculus Surgical. MKE receives research support from New World Medical and Glaukos. MYK is a consultant to New World Medical and his university receives fees on his behalf for this consultancy. MYK also has a patent (No. 10,729,584) related to the STREAMLINE Surgical System technology and a patent (US 2021/0322218 A1) owned by New World Medical. The authors report no other conflicts of interest in this work.
References
1. Bourne RRA, Jonas JB, Friedman D; Vision Loss Expert Group of the Global Burden of Disease Study; GBD. Blindness and vision impairment collaborators. Global estimates on the number of people blind or visually impaired by glaucoma: a meta-analysis from 2000 to 2020. Eye. 2024;11:2036. Epub ahead of print. PMID: 38565601. doi:10.1038/s41433-024-02995-5
2. The AGIS Investigators. The advanced glaucoma intervention study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration. The AGIS investigators. Am J Ophthalmol, 2000; 130(4):429–440. PMID: 11024415. doi:10.1016/s0002-9394(00)00538-9
3. Heijl A, Leske MC, Bengtsson B, Hyman L, Bengtsson B, Hussein M. early manifest glaucoma trial group. Reduction Intraocular Pres Glaucoma Progres Arch Ophthalmol. 2002;120(10):1268–1279.
4. Sun Y, Chen A, Zou M, et al.. Time trends, associations and prevalence of blindness and vision loss due to glaucoma: an analysis of observational data from the global burden of disease study 2017. BMJ Open. 2022;12(1):e053805. doi:10.1136/bmjopen-2021-053805 PMID: 34992115; PMCID: PMC8739070.
5. Allison K, Patel D, Alabi O. Epidemiology of glaucoma: the past, present, and predictions for the future. Cureus. 2020;12(11):e11686. doi:10.7759/cureus.11686 PMID: 33391921; PMCID: PMC7769798.
6. Weinreb RN, Aung T, Medeiros FA. The pathophysiology and treatment of glaucoma: a review. JAMA. 2014;311(18):1901–1911. doi:10.1001/jama.2014.3192 PMID: 24825645; PMCID: PMC4523637.
7. Balas M, Mathew DJ. Minimally invasive glaucoma surgery: a review of the literature. Vision. 2023;7(3):54. doi:10.3390/vision7030054 PMID: 37606500; PMCID: PMC10443347.
8. Yang SA, Ciociola EC, Mitchell W, et al.. IRIS® registry analytic center consortium. efficacy of microinvasive glaucoma surgery in the United States: intelligent research in sight registry analysis 2013-2019. Ophthalmology. 2023;130(3):242–255. doi:10.1016/j.ophtha.2022.10.021 Epub 2022 Oct 29. PMID: 36522820; PMCID: PMC10321208.
9. Joshi P, Dangwal A, Guleria I, et al.. Glaucoma in adults-diagnosis, management, and prediagnosis to end-stage, categorizing glaucoma’s stages: a review. J Curr Glaucoma Pract. 2022;16(3):170–178. doi:10.5005/jp-journals-10078-1388 PMID: 36793264; PMCID: PMC9905872.
10. Fellman RL, Mattox C, Singh K, et al.. American glaucoma society position paper: microinvasive glaucoma surgery. Ophthalmol Glaucoma. 2020;3(1):1–6. doi:10.1016/j.ogla.2019.12.003 PMID: 32672638; PMCID: PMC7531041.
11. Birnbaum FA, Neeson C, Solá-Del Valle D. Microinvasive glaucoma surgery: an evidence-based review. Semin Ophthalmol. 2021;36(8):772–786. doi:10.1080/08820538.2021.1903513 Epub 2021 Jul 23. PMID: 34297650.
12. Mathew DJ, Buys YM. Minimally invasive glaucoma surgery: a critical appraisal of the literature. Annu Rev Vis Sci. 2020;6:47–89. PMID: 32936738. doi:10.1146/annurev-vision-121219-081737.
13. Lavia C, Dallorto L, Maule M, Ceccarelli M, Fea AM. Minimally-invasive glaucoma surgeries (MIGS) for open angle glaucoma: a systematic review and meta-analysis. PLoS One. 2017;12(8):e0183142. doi:10.1371/journal.pone.0183142 PMID: 28850575; PMCID: PMC5574616.
14. Lazcano-Gomez G, Antzoulatos GL, Kahook MY. Combined phacoemulsification and STREAMLINE surgical system canal of schlemm transluminal dilation in eyes of Hispanic patients with mild to moderate glaucoma. Clin Ophthalmol. 2023;17:1911–1918. PMID: 37425029; PMCID: PMC10329431. doi:10.2147/OPTH.S409164.
15. Lazcano-Gomez G, Garg SJ, Yeu E, Kahook MY. Interim analysis of STREAMLINE® surgical system clinical outcomes in eyes with glaucoma. Clin Ophthalmol. 2022;16:1313–1320. PMID: 35510271; PMCID: PMC9058234. doi:10.2147/OPTH.S358871.
16. Samuelson TW, SR S
17. Ahmed IIK, Fea A, Au L, et al.. COMPARE investigators. A prospective randomized trial comparing Hydrus and istent microinvasive glaucoma surgery implants for standalone treatment of open-angle glaucoma: the COMPARE study. Ophthalmology. 2020;127(1):52–61. doi:10.1016/j.ophtha.2019.04.034 Epub 2019 Apr 26. PMID: 31034856.
18. Falkenberry S, Singh IP, Crane CJ, et al.. Excisional goniotomy vs trabecular microbypass stent implantation: a prospective randomized clinical trial in eyes with mild to moderate open-angle glaucoma. J Cataract Refract Surg. 2020;46(8):1165–1171. doi:10.1097/j.jcrs.0000000000000229 PMID: 32358417.iStent inject W Instructions For Use.
19. iStent inject W Instructions for Use. Glaukols Corp.; 2021. Available from: https://www.glaukos.com/wp-content/uploads/2021/09/45-0244-Rev-1-artwork-IFU-G2-W-iStent-inject-W-Commercial-US.pdf.
20. New World Medical. Streamline Surgical System Instructions for Use. Rev B. Rancho Cucamonga, CA: New World Medical; 2021.
21. Realini T, Gupta PK, Radcliffe NM, et al.. The effects of glaucoma and glaucoma therapies on corneal endothelial cell density. J Glaucoma. 2021;30(3):209–218. doi:10.1097/IJG.0000000000001722
22. Gallardo MJ, SR S Jr, Vold SD, et al.. GEMINI study group. Canaloplasty and trabeculotomy combined with phacoemulsification in open-angle glaucoma: interim results from the GEMINI study. Clin Ophthalmol. 2021;15:481–489. PMID: 33603325; PMCID: PMC7882439. doi:10.2147/OPTH.S296740.
23. Hirsch L, Cotliar J, Vold S, et al.. Canaloplasty and trabeculotomy ab interno with the OMNI system combined with cataract surgery in open-angle glaucoma: 12-month outcomes from the ROMEO study. J Cataract Refract Surg. 2021;47(7):907–915. doi:10.1097/j.jcrs.0000000000000552 PMID: 33315733.
24. Louanchi Y, Brasnu E, Hamard P, Aragno V, Baudouin C, Labbé A. Short-term efficacy and safety of phacoemulsification associated with iStent Inject W in patients with controlled open angle glaucoma. J Glaucoma. 2023;32(12):1052–1057. doi:10.1097/IJG.0000000000002327 Epub 2023 Oct 19. PMID: 37974323.
25. Deneri S, Merté RL, Eter N, Brücher VC. Comparison of the iStent Inject® versus the iStent Inject® W-both in combination with cataract surgery-in open-angle glaucoma. J Clin Med. 2023;12(23):7259. doi:10.3390/jcm12237259 PMID: 38068308; PMCID: PMC10707291.
26. Hirabayashi MT, King JT, Lee D, An JA. Outcome of phacoemulsification combined with excisional goniotomy using the Kahook dual blade in severe glaucoma patients at 6 months. Clin Ophthalmol. 2019;13:715–721. PMID: 31114149; PMCID: PMC6488161. doi:10.2147/OPTH.S196105.
27. Hirabayashi MT, Lee D, King JT, Thomsen S, An JA. Comparison of surgical outcomes of 360° circumferential trabeculotomy versus sectoral excisional goniotomy with the Kahook dual blade at 6 months. Clin Ophthalmol. 2019;13:2017–2024. PMID: 31686776; PMCID: PMC6800543. doi:10.2147/OPTH.S208468.
28. Mechleb N, Tomey K, Cherfan D, et al.. Six months’ follow-up of combined phacoemulsification-kahook dual blade excisional goniotomy. Saudi J Ophthalmol. 2022;36(2):195–200. doi:10.4103/sjopt.sjopt_151_21 PMID: 36211310; PMCID: PMC9535917.
29. American Academy of Ophthalmology. Canaloplasty. Available from: https://www.aao.org/practice-management/news-detail/canaloplasty.
30. OMNI Surgical System Instruction. Available from: https://omnisurgical.com/wp-content/uploads/2023/08/PN-05854-Rev-K-IFU-OMNI-System-2.0-US.pdf.
31. iTrack instructions for use. Available from: https://nova-eye.com/us/healthcare-professionals/itrack/.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.