")
Back to Journals » Clinical Ophthalmology » Volume 18
A Randomized, Multicenter Phase 3 Clinical Trial Evaluating Intracanalicular Dexamethasone Insert for the Treatment of Allergic Conjunctivitis
Authors Kenyon K, McLaurin EB , Silverstein SM , Meyer JC, Anderson E, Patel RH, Gomes PJ, Reilly E, Vantipalli S, Cheung MW, Goldstein MH
Received 1 May 2024
Accepted for publication 27 August 2024
Published 21 September 2024 Volume 2024:18 Pages 2671—2684
DOI https://doi.org/10.2147/OPTH.S476419
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kenneth Kenyon,1 Eugene B McLaurin,2 Steven M Silverstein,3 John C Meyer,4 Erik Anderson,5 Ravi H Patel,6 Paul J Gomes,7 Erin Reilly,8 Srilatha Vantipalli,8 Matthew W Cheung,8 Michael H Goldstein8
1Andover Eye Associates, Andover, MA, USA; 2Total Eye Care, P.A., Memphis, TN, USA; 3Silverstein Eye Centers, Kansas City, MO, USA; 4The Eye Care Institute, Louisville, KY, USA; 5Vision Institute, Colorado Springs, CO, USA; 6Eye Associates of Texas, Round Rock, TX, USA; 7Ora, Inc., Andover, MA, USA; 8Ocular Therapeutix, Inc., Bedford, MA, USA
Correspondence: Matthew W Cheung, Ocular Therapeutix, Inc., 15 Crosby Drive, Bedford, MA, 01730, USA, Tel +1 516-287-7678, Email [email protected]
Purpose: To evaluate the efficacy and safety of a dexamethasone intracanalicular insert (DEX) for treatment of allergic conjunctivitis (AC).
Patients and Methods: In this multicenter, randomized, double-masked, placebo-controlled phase 3 study, adults (≥ 18 years) with AC were randomized 1:1 to DEX or placebo insert (PBO) placed bilaterally. Subjects underwent repetitive conjunctival allergen challenges (CAC) across 30 days and were assessed for changes in AC signs and symptoms. The primary endpoint was ocular itching score at 3, 5, and 7 minutes post-CAC at Day 8 (7 days post-insertion). This trial is registered on ClinicalTrials.gov (NCT04050865).
Results: Ninety-six subjects were randomized (n=48 DEX, n=48 PBO). Compared to PBO, there were statistically significant treatment differences favoring DEX for the primary endpoint of mean ocular itching score at Day 8 (− 0.86, − 0.98, − 0.96 at 3, 5, and 7 minutes post-CAC respectively; P< 0.0001 for all). Treatment differences favored DEX for all 24 time points across 6 visits and were statistically significant (P< 0.05) except for the first post-insertion (Day 7, 3 minutes). For the 18 time points at which conjunctival redness was assessed, DEX had lower scores than PBO (P< 0.05 for all). The most common ocular adverse events (AEs) in DEX subjects were eye discharge and irritation. No serious AEs, elevated intraocular pressure, dacryocanaliculitis, or use of rescue medications were reported.
Conclusion: Results of this study support the potential use of dexamethasone insert as a physician-administered, preservative-free treatment for AC, with significant improvements in ocular itching and conjunctival redness compared with placebo. The dexamethasone insert was generally safe with a favorable safety profile.
Keywords: allergy, conjunctivitis, dexamethasone, insert, intracanalicular
Introduction
Allergic conjunctivitis is an inflammatory-mediated disorder induced by seasonal or perennial allergens and affects up to approximately 40% of the general United States (US) population.1 However, it is often underdiagnosed and undertreated due to its association with other disorders such as dry eye disease and allergic rhinitis.2,3 Two of the most common symptoms of allergic conjunctivitis are itching and redness.3 For patients with moderate to severe symptoms, there is a detrimental impact on quality of life.4 Several studies have examined the impact of allergic conjunctivitis on patients’ quality of life.5–7 In a study of 220 patients with ocular allergy, nearly half rated their disease severity of at least 6 on a scale of 1 to 10; moreover, patient-reported quality of life significantly declined during allergic conjunctivitis episodes (P<0.001).5 A study of more than 1000 patients with allergic rhinoconjunctivitis found that allergic conjunctivitis was associated with a decrease in productivity, illustrated by an impairment while working and an increase in hours of work missed.7
Current treatment options for allergic conjunctivitis include topical antihistamines, which have a rapid onset and short duration of action, and topical mast-cell stabilizers, which require a long loading period.2,8–10 Topical corticosteroids are effective in both the early and late phases of the allergic response but are generally limited to a short course (1–2 weeks) for patients with more severe or persistent symptoms due to the potential for misuse or abuse of steroids, which can lead to complications associated with long-term use.8–10 All topical corticosteroid eye drops commercially available in the US contain preservatives,11–13 which can cause patient discomfort and corneal toxicity.14 Topical corticosteroids also have a complex dosing regimen,11–13 which can result in poor patient compliance and difficulty with self-administration.15,16 An additional limitation with the application of topical drops includes frequent touching of the face, which potentially increases the risk for infection.17,18
A sustained-release intracanalicular dexamethasone insert (DEXTENZA [dexamethasone ophthalmic insert, 0.4 mg], Ocular Therapeutix, Inc.). has been designed to obviate the need for corticosteroid drops.19 It contains 0.4 mg dexamethasone and is administered through the lacrimal punctum into the canaliculus.19 A single insert provides tapered steroid therapy up to 30 days onto the surface of the eye.19,20 The insert, which is fluorescein-conjugated for visualization, does not contain preservatives and is fully biodegradable.19 The dexamethasone insert had a favorable efficacy and safety profile in studies in subjects undergoing cataract surgery and was approved by the Food and Drug Administration (FDA) for the treatment of postoperative ocular pain and inflammation after ophthalmic surgery in 2018 and 2019, respectively.21,22 The insert was then FDA-approved for the treatment of ocular itching associated with allergic conjunctivitis in 2021.19
For the evaluation of potential therapies for the treatment of allergic conjunctivitis, the Ora-CAC® conjunctival allergen challenge (CAC) model has been designed as an alternative to environmental studies, which can introduce bias due to variability both in the allergens causing allergic conjunctivitis and in subjects’ exposure to the allergens. The CAC model allows for the evaluation of the effect of potential therapies on the early phase of the allergic response by reproducibly inducing an acute moderate-to-severe ocular allergic reaction.23 This model has been used for the approval of antihistamines and mast cell stabilizers including alcaftadine 0.25% (Lastacaft®), cetirizine 0.24% (Zerviate™), ketotifen 0.035% (Alaway® Preservative Free), and bepotastine besilate 1.5% (Bepreve®).24–27 For the evaluation of the effect of potential therapies such as corticosteroids on the late-phase inflammatory response, a modified CAC model using repeated allergen challenges has been developed.28–30
This was a confirmatory study performed to satisfy regulatory requirements. Three prior studies have evaluated the dexamethasone insert for the treatment of allergic conjunctivitis using this repeat CAC model, including a phase 2 study (N=68), a phase 3A study (N=73), and a phase 3B study (N=86).30,31 The primary endpoints were evaluated at 2 weeks after insertion in the phase 2 study and 1 week after insertion in the phase 3A study.30,31 Both studies showed a significant reduction in ocular itching with the dexamethasone insert at the primary endpoint. There was also a significant reduction in conjunctival redness at all 3 post-challenge time points (7, 15, and 20 minutes) in the phase 2 study and in 2 of the 3 post-challenge time points in the phase 3 study (15 and 20 minutes but not 7 minutes). The phase 3B study did not show a statistically significant reduction in the primary endpoint of ocular itching at 1 week after insertion, although subjects treated with the dexamethasone insert had numerically lower itching scores than those treated with the vehicle insert at all 36 time points evaluated in this study (unpublished data).32 Although the phase 3 trials differed somewhat with respect to study visit schedule, the primary endpoint evaluating ocular itching was the same.
The objective of this phase 3 study was to provide further evaluation of the efficacy and safety of a dexamethasone intracanalicular insert for the treatment of the signs and symptoms of allergic conjunctivitis. The repeated CAC model in this study was informed by prior clinical trials utilizing 3 challenges conducted over a 2-day interval to evaluate the effectiveness of a test agent to: 1) prevent an acute ocular allergic reaction (the initial CAC), and 2) evaluate the test agent’s ability to prevent an acute ocular allergic reaction in the presence of late phase-inflammation (the latter re-challenge CACs).
Materials and Methods
Study Design
This was a multicenter, randomized, double-masked, placebo-controlled phase 3 study performed at 6 geographically diverse sites in the United States from August 5, 2019 (when the first subject was screened) to February 28, 2020 (when the last subject underwent the last follow-up visit and the trial was completed). The study consisted of 13 office visits over approximately 5 to 11 weeks (Figure 1), including a screening period of 6 to 45 days, insertion of the ophthalmic insert bilaterally on Day 1, and 2 series of CAC and re-challenge CACs (Days 7–8 and Days 14–15). For each post-insertion CAC, the subject received 1 drop of seasonal or perennial allergen solution bilaterally at the same dose that elicited a positive reaction at the titration visit. The study exit was on Day 30 with final safety evaluations.
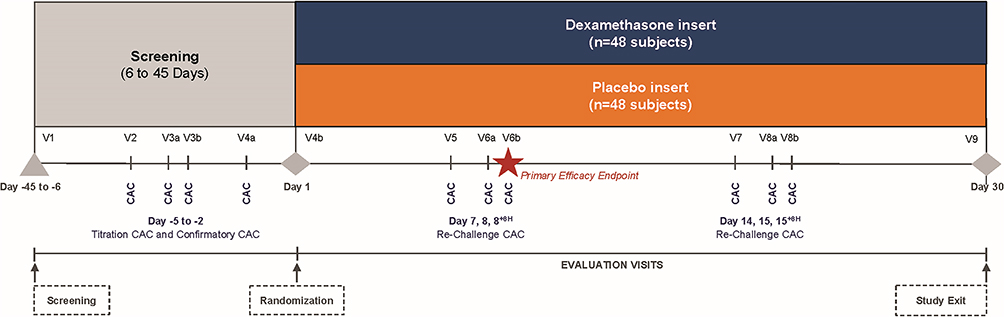 |
Figure 1 Study design. Abbreviation: CAC, conjunctival allergen challenge. |
The study was conducted in compliance with the protocol and International Council for Harmonization (ICH) Good Clinical Practice (GCP) Guidelines and was consistent with the 1996 version of the Declaration of Helsinki. Institutional Review Board (IRB)/Ethics Committee approval was obtained from Alpha IRB. An informed consent form, signed and dated by both the subject and the delegated study staff presenting the consent, was required from each subject prior to enrollment into the study, and before any study specific procedures were initiated. This trial is registered on ClinicalTrials.gov (NCT04050865).
Subjects
Subjects were ≥18 years of age and had a positive history of ocular allergies, a positive skin test reaction to a perennial allergen (cat dander, dog dander, dust mites, cockroaches) and a seasonal allergen (trees, grasses, and/or ragweed), a positive bilateral CAC reaction (defined as itching score ≥2 on the Ora Calibra itching scale [0–4 scale, where 0 = none and 4 = severe] and conjunctival redness score ≥2 on the Ora Calibra ocular hyperemia scale [0–4 scale, where 0 = none and 4 = severe) within 10±2 minutes of instillation of the last titration of allergen, and average scores of ≥3 for itching and ≥2.5 for conjunctival redness for both eyes after the first 3 post-CAC assessment time points. Subjects were also required to have best-corrected visual acuity (BCVA) ≥50 Early Treatment Diabetic Retinopathy Study (ETDRS) letters (20/100 Snellen equivalent or better) in each eye.
Subjects were excluded if they had a history of refractive surgery in the last 2 years; retinal detachment, diabetic retinopathy, or active retinal disease; presence of an active ocular infection, current diagnosis or history of herpes simplex keratitis; narrow-angle glaucoma, clinically significant blepharitis, follicular conjunctivitis, iritis, pterygium or a diagnosis of dry eye; a score of >0 for ocular itching and/or >1 for conjunctival redness prior to the challenge in either eye; intraocular pressure (IOP) <5 mmHg or >22 mmHg or any type of glaucoma; or history of an IOP increase as a result of steroid treatment.
Treatment
Once subjects met all qualification criteria, they were randomly assigned in a 1:1 ratio to treatment with dexamethasone insert or placebo vehicle (control). The treatment was masked to subjects and investigators via an identical appearance and packaging of the dexamethasone and placebo inserts. The dexamethasone insert contains 0.4 mg dexamethasone and a polyethylene glycol (PEG)-based hydrogel conjugated with fluorescein. The fluorescent PEG allows the insert to be visualized utilizing a blue light source and yellow filter. The placebo vehicle is the same fluorescent PEG hydrogel insert without dexamethasone. Therefore, the placebo will not influence the disease or CAC results. The hydrogel intracanalicular insert is designed to be placed in the canaliculus and swells on contact with moisture to occlude the lumen, securing it in place. Following punctal dilation, it is placed into the punctum by the investigator using forceps in a clinical setting (at the slit lamp, for example). After insertion, the insert continuously releases a tapered dose of dexamethasone over approximately 30 days onto the surface of the eye. Following elution of drug over 30 days, the hydrogel insert undergoes gradual hydrolysis, eventually liquefying, and then clearing the nasolacrimal system by flushing through the nasolacrimal duct.
The randomization schedule was computer-generated, controlled by 4 blocks and stratified by study site. Subjects were randomized on Day 1 by assignment of the lowest 4-digit randomization number available at the investigative site. No product numbers were skipped or omitted. Randomization was performed by a biostatistician independent of the study conduct or project team. The study sponsor, investigator, and subjects were masked to the treatment assignment throughout the study.
Study Endpoints
The primary endpoint was subject-evaluated ocular itching on Day 8 (Visit 6b) at 3±1, 5±1, and 7±1 minutes post-CAC (0–4 scale, allowing half unit increments). Key secondary efficacy endpoints were ocular itching at 3±1, 5±1, and 7±1 minutes post-CAC at the following visits: Days 7, 8, 14, 15, and 15 (Visit 8b). Other secondary efficacy endpoints were ocular itching at 10±1 minutes post-CAC at Days 7, 8, 8 (Visit 6b), 14, 15, and 15 (Visit 8b); and the following assessments at 7±1, 15±1, and 20±3 minutes post-CAC at Days 7, 8, 8 (Visit 6b), 14, 15, and 15 (Visit 8b): investigator-evaluated conjunctival redness; investigator-evaluated ciliary and episcleral redness; investigator-evaluated chemosis; subject-evaluated eyelid swelling; subject-evaluated tearing/watery eyes; and subject-evaluated rhinorrhea, nasal pruritus, ear or palate pruritus, and nasal congestion. The Ora Calibra® scales were used to grade all efficacy endpoints (all 0–4 scales except for eyelid swelling which used a 0–3 scale).
Safety evaluations included adverse events (AEs) (reported, elicited, and observed); BCVA using an ETDRS chart; slit-lamp biomicroscopy, including punctum exam; IOP; and dilated fundoscopy examination.
Statistical Analysis
Efficacy analyses were conducted on the intent-to-treat (ITT) population (all randomized subjects) with Markov Chain Monte Carlo (MCMC) multiple imputation for missing and incomplete efficacy data. Safety analyses were conducted on the safety population (all randomized subjects who received an insert) and were analyzed as treated. The average of each subject’s eyes at each timepoint within each visit were used for efficacy analyses.
Analysis of covariance (ANCOVA) models were run at each post-CAC timepoint of a given visit to estimate least squares (LS) means. These models include the time appropriate post-CAC scores at screening as a baseline covariate for adjustment and treatment group as the sole factor. LS means were used to make treatment comparisons. Statistical significance of treatment differences was determined using a 2-sided significance level of α=0.05.
A sample size of 40 subjects per group was determined to provide 97.0%, 99.8% and 99.9% power to demonstrate a statistically significant difference in ocular itching at 3-, 5-, and 7-minute post-CAC time points at Day 8 (Visit 6b), respectively assuming a treatment difference of 0.87 units at 3 minutes, 1.08 units at 5 minutes, and 1.13 units at 7 minutes post-CAC between subjects in the dexamethasone insert group and subjects in the placebo insert group.
Results
Subjects
A total of 96 subjects were randomized (48 in the dexamethasone insert arm, 48 in the placebo insert arm) and included in the ITT, which included subjects who received intended treatment and were analyzed for the primary outcome, and safety populations. Subject demographics are shown in Table 1.
 |
Table 1 Subject Demographics |
The mean age was similar across treatment groups (43.8 and 46.0 years in the dexamethasone insert and placebo insert groups, respectively). Slightly more than half of the subjects were female (n=51 [53.1%]). The majority of subjects identified as Caucasian (n=61 [63.5%]) and did not identify as Hispanic or Latino (n=85 [88.5%]). Subjects were allergic to both seasonal and perennial allergens, and the allergens evaluated included a wide variety of both seasonal and perennial allergens (Table 2).
 |
Table 2 Summary of Qualifying Allergens |
A total of 87 subjects completed the study, and 9 subjects withdrew from the study. The reasons for withdrawal included AE of eye irritation (1 subject in the dexamethasone insert arm), consent withdrawn (1 subject in the placebo insert arm), investigator decision (1 subject in the placebo insert arm), only 1 insert placed (5 subjects: 2 in the dexamethasone insert arm and 3 in the placebo insert arm), and other reasons (1 subject in the dexamethasone insert arm). At the Day 30 visit, 95.1% of dexamethasone inserts and 96.5% of placebo inserts were easily visualized by investigators.
Efficacy
The ocular itching primary efficacy measurement was assessed by subjects in each eye using a 0–4 unit scale (half unit increments allowed) at Day 8 (Visit 6b) at 3±1, 5±1, and 7±1 minutes post-CAC and analyzed. Lower scores indicate less ocular itching. There were statistically significant treatment differences (P<0.0001) in favor of the dexamethasone insert group at all 3 post-CAC time points: −0.86 at 3 minutes post-CAC, −0.98 at 5 minutes post-CAC, and −0.96 at 7 minutes post-CAC (Figure 2).
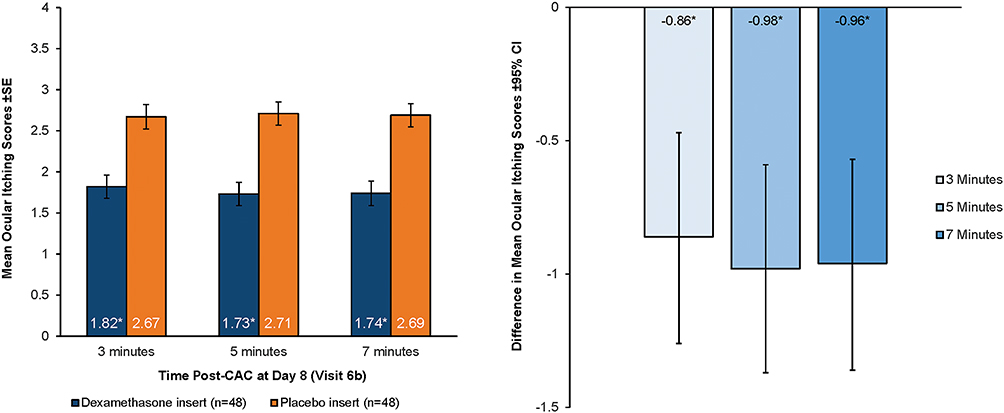 |
Figure 2 Primary endpoint: ocular itching scores on day 8 in the ITT population with MCMC imputation. The left panel shows the primary endpoint of mean subject-evaluated ocular itching scores (scale 0–4) at Day 8 (Visit 6b) with the dexamethasone insert compared with the placebo insert at 3, 5, and 7 minutes post-CAC. The right panel shows the treatment difference (dexamethasone insert minus placebo) at each timepoint post-CAC. Means are least square means estimated by ANCOVA modeling. Error bars represent the 95% CI. Asterisks (*) indicate differences between the dexamethasone insert and the placebo insert with P<0.0001. Abbreviations: ANCOVA, analysis of covariance; CAC, conjunctival allergen challenge; CI, confidence interval; ITT, intent-to-treat; LS, least squares; MCMC, Markov chain Monte Carlo; SE, standard error. |
For all secondary endpoints (24 time points across 6 different visits), the dexamethasone insert group had lower ocular itching scores than the placebo group (Figure 3). Statistically significant treatment differences (P<0.05) favoring the dexamethasone insert group were noted for 23 of the 24 study time points, with the exception of the first post-insertion timepoint (Day 7 at 3 minutes). The treatment differences ranged from −0.75 to −1.24 for all time points at all visits after Day 7. For half of all time points evaluated in the study, the magnitude of the treatment difference between dexamethasone inserts group and the placebo group was >1.00 unit.
 |
Figure 3 Mean ocular itching scores across all time points in the ITT population with MCMC imputation. Mean subject-evaluated ocular itching scores (scale 0–4) at all evaluation visits are shown, comparing the dexamethasone insert with the placebo insert at 3, 5, 7, and 10 minutes post-CAC. Treatment differences (dexamethasone insert minus placebo) are shown on the x-axis. Means are LS means estimated by ANCOVA modeling. Asterisks (*) indicate differences between the dexamethasone insert and the placebo insert with P<0.05. Abbreviations: ANCOVA, analysis of covariance; CAC, conjunctival allergen challenge; ITT, intent-to-treat; LS, least squares; MCMC, Markov chain Monte Carlo; SE, standard error. |
Conjunctival redness was evaluated by the investigator at 7±1, 15±1, and 20±3 minutes post-CAC at Days 7, 8, 8 (Visit 6b), 14, 15, and 15 (Visit 8b) using a 0–4 unit scale (half unit increments allowed). Lower scores indicate less conjunctival redness. Across all 18 time points, there were statistically significant treatment differences in conjunctival redness favoring the dexamethasone insert group, with P values <0.05 at all 18 post-CAC time points and at each overall visit. For all post-CAC time points after Day 7, this treatment difference was ≥0.5 units in favor of the dexamethasone group (P<0.0005) (Figure 4).
 |
Figure 4 Mean conjunctival redness scores across all time points in the ITT population with observed data. Mean investigator-evaluated conjunctival redness scores (scale 0–4) at all evaluation visits are shown, comparing the dexamethasone insert with the placebo insert at 7, 15, and 20 minutes post-CAC. Treatment differences are shown on the x-axis. Means are LS means estimated by ANCOVA modeling. Asterisks (*) indicate differences between dexamethasone insert and placebo insert with P<0.05. Abbreviations: ANCOVA, analysis of covariance; CAC, conjunctival allergen challenge; ITT, intent-to-treat; LS, least squares; SD, standard deviation. |
Additional secondary endpoints for 6 study visits on Days 7–8 and Days 14–15 at 7, 15, and 20 minutes post-CAC are shown in Table 3. For both ciliary and episcleral redness, treatment differences favored the dexamethasone insert group with P<0.05 at all visits; for visits after Day 7 (except Day 8 at 7 minutes for episcleral redness), the treatment difference was >0.5 units in favor of the dexamethasone insert group. The results for most additional secondary endpoints, including eyelid swelling, tearing/watery eyes, rhinorrhea, nasal pruritus, ear or palate pruritus, and nasal congestion, favored the dexamethasone insert group.
 |
Table 3 Key Secondary Efficacy Endpoints Across All Timepoints in the ITT Population. The Difference in Mean Scores (Dexamethasone Insert Minus Placebo Insert) is Presented |
Safety
Of the 96 subjects in the safety population, 23 subjects reported a total of 30 AEs: 9 subjects in the dexamethasone insert group and 14 subjects in the placebo group. No ocular or non-ocular serious AEs (SAEs) were reported. All AEs were mild or moderate in severity. Of the 30 AEs, 22 were non-ocular AEs, and none were considered related to study treatment. The remaining 8 AEs were ocular, of which 7 were mild and 1 was moderate in severity (in the placebo group – swelling of eyelid). All of the AEs are known reactions to allergy challenge. The overall safety summary is shown in Table 4.
 |
Table 4 Overall Safety Summary: Safety Population |
Of the 8 subjects with ocular AEs, 2 were in the dexamethasone insert group and 6 in the placebo group. The 2 ocular AEs in the dexamethasone insert group were eye discharge and eye irritation (Table 5). Both were considered to be related to study treatment, and the AE of eye irritation led to withdrawal of treatment 3 days after insertion in 1 subject. No subjects required rescue medication. No subjects had an AE of elevated IOP (IOP ≥30 mmHg or IOP increases of 10 mmHg). In addition, mean IOP change from baseline at all time points tested ranged from −1.6 to −0.5 mmHg in the dexamethasone insert group and from −2.3 to −1.6 mmHg in the placebo group (Table 6). Further, no subjects reported dacryocanaliculitis or an AE related to a worsening of visual acuity.
 |
Table 5 Ocular Treatment-Emergent Adverse Events: Safety Population |
 |
Table 6 Intraocular Pressure in the Safety Population |
Discussion
The primary objective of this study was to evaluate the efficacy and safety of a dexamethasone insert when placed in the canaliculus of the eyelid for the treatment of the signs and symptoms of allergic conjunctivitis using a modified version of the CAC model. The primary efficacy endpoint of lower mean ocular itching scores at Day 8 was met. The dexamethasone insert group had a statistically significant treatment difference over the placebo group at the 1 week post-insertion series of challenges, demonstrating an early onset of action. Additionally, the dexamethasone insert group showed significant treatment differences compared to the placebo group at 23 of 24 time points evaluated, demonstrating duration of action for at least 2 weeks in this study. Together these findings support the use of the dexamethasone insert to reduce ocular itching quickly (within the first 7 days following insertion) and to maintain this benefit for at least 2 weeks after insertion. The dexamethasone insert also showed efficacy in reducing conjunctival redness, with significant improvements in conjunctival redness scores at all 18 post-CAC time points. The results of this study are consistent with previously reported phase 2 and phase 3 studies of the dexamethasone insert in subjects with allergic conjunctivitis using a similar repeat CAC model, despite differing slightly in study visit schedule.30,31
In addition to showing a benefit in itching and redness, which are 2 of the most common patient complaints related to allergic conjunctivitis, the dexamethasone insert showed a directional benefit in eyelid swelling, tearing/watery eyes, and nasal symptoms (rhinorrhea, nasal pruritus, and nasal congestion).3 Nasal congestion may be the primary complaint in individuals with rhinoconjunctivitis, followed by ocular symptoms.3
The dexamethasone insert was generally safe and well tolerated with no serious or severe ocular or non-ocular AEs observed. In the dexamethasone insert arm, 2 subjects experienced ocular AEs that were considered related to treatment: eye discharge and eye irritation. This safety profile is in line with prior phase 2 and 3 studies in allergic conjunctivitis and clinical studies with the same insert following cataract surgery.21,22,30,31 Moreover, there have been few treatment-related AEs with the dexamethasone insert: 2 in the current study and 14 in prior phase 2 and 3 allergic conjunctivitis and cataract surgery studies (N=632).21,22,30,31,33
Dexamethasone and other corticosteroids are known to be associated with a number of complications associated with long-term topical use, including elevated IOP/induction or exacerbation of glaucoma, cataract formation, delayed wound healing, and increased susceptibility to infection.8–10,34 In individuals who are considered “steroid responders” and have greater IOP increases in response to topical corticosteroid eye drops, glaucoma may occur through a proposed mechanism of reduced aqueous outflow due to possible effects on the trabecular meshwork.9,34 In the current study, no subjects reported an AE of elevated IOP, IOP ≥30 mmHg, or IOP increases of 10 mmHg, nor did subjects report any other AEs known to be complications of steroid use. In the previous phase 2 and 3 studies, there were a total of 3 subjects with IOP increases in the dexamethasone arms.30,31 Together, safety data from the current study and previous dexamethasone insert studies provide evidence for the safety of a corticosteroid applied to the ocular surface.
The dexamethasone insert has a number of advantages compared with eye drops. Because it is placed by the clinician, the dexamethasone insert is not associated with patient compliance or overuse concerns. Reasons associated with poor compliance in patients taking eye drops typically include medication-related factors, such as difficulty in administration, side effects, and medication schedule difficulties.16 While proper administration of eye drops is an important component of compliance, a study of patients following cataract surgery (N=54) found that the majority (92%) lacked proper administration technique.15
Steroid eye drops in particular are problematic because overuse due to symptomatic relief can lead to complications.35 The dexamethasone insert cannot be abused by patients. It is physician administered, which eliminates the role of the patient in delivering the medication. The insert biodegrades on its own without the need for removal. In rare cases, it can be easily removed if necessary.19 Physician administration of the dexamethasone insert also removes the risk of infection associated with the frequent hand-face contact required for eye drop administration.17,18
The dexamethasone insert is a preservative-free steroid treatment. Exposure to preservatives in topical ocular therapies may be associated with a compromised ocular surface due to dry eye disease and inflammatory irritation.36 The most common ophthalmic antimicrobial preservative utilized is benzalkonium chloride (BAK), which is associated with discomfort and pain following instillation as well as ocular surface toxicity, conjunctival hyperemia, decreased tear production, tear film instability, and superficial punctate keratitis.36–38 There are currently no other commercially available preservative-free ophthalmic steroid therapy options for the treatment of allergic conjunctivitis.
Untreated allergic conjunctivitis can result in ocular complications, underscoring the need for safe, effective treatments for allergic conjunctivitis. Eye rubbing due to ocular itching is associated with corneal ectasia, including keratoconus, which can lead to acute corneal hydrops, corneal perforation, corneal scarring, and vision loss.39–42 Potential complications associated with untreated allergic conjunctivitis are detrimental to quality of life, especially for individuals who have concomitant dry eye disease.43,44 Concomitant dry eye disease is common in individuals with allergic conjunctivitis,45 and future studies in this population are needed. The 2 conditions interact with each other,46 and the symptoms of dry eye disease may exacerbate the itching, redness, and chemosis experienced during allergen challenge in subjects with allergic conjunctivitis.47
The population in this study exhibited a moderate to severe ocular reaction across various concentrations of allergens and types of allergens, evaluating subjects with both seasonal and perennial allergens. The wide variety of allergens used in the study support the use of the dexamethasone insert as a possible treatment for all allergen-induced allergic conjunctivitis and further support the insert’s mechanism of action.
Although there are several advantages to using the CAC model, the controlled allergen exposure in the model reduces variability and does not replicate the real-world environmental conditions in which an allergen would be encountered by patients and therefore is a potential limitation of this study. Another limitation is the comparator selected for the control arm. The use of placebo vehicle inserts aligns with regulatory requirements for clinical trial design, but additional studies should be performed using an active control, such as topical corticosteroids, to compare efficacy and safety with a currently available treatment option. Furthermore, allergic conjunctivitis can burden patients by adversely impacting sleep, activities of daily living and work productivity. Future study designs might consider including patient-reported outcome questionnaires to assess potential treatment effects on quality of life.
Conclusion
In summary, the results of this phase 3 study support the potential use of dexamethasone as a sustained-release, physician-administered therapy to treat allergic conjunctivitis, with significant improvements in both ocular itching and conjunctival redness compared with placebo. The primary endpoint was met, and the safety profile was favorable.
Data Sharing Statement
Requests should be directed to [email protected]. To obtain access, data requestors will be required to sign a data access agreement. When requested individual participant data that underlie the results reported in this article (text, tables, and figures) will be shared after deidentification.
Acknowledgments
This study and preparation of this manuscript was sponsored by Ocular Therapeutix, Inc., Bedford, MA. The authors acknowledge the editorial assistance of Lisa Cimakasky, PhD, and Cecelia Wall, MPH during the preparation of this manuscript.
Funding
Funding/support provided by Ocular Therapeutix, Inc.
Disclosure
Kenneth Kenyon, Eugene McLaurin, Steven Silverstein, John Meyer, Erik Anderson, and Ravi Patel were study investigators and have no conflicts of interest to disclose for this work. Paul Gomes is an employee of Ora, Inc. Erin Reilly, Srilatha Vantipalli, and Matthew Cheung are employees of Ocular Therapeutix, Inc. Michael H. Goldstein is a former employee of Ocular Therapeutix, Inc. The authors report no other conflicts of interest in this work.
References
1. Leonardi A, Castegnaro A, Valerio AL, Lazzarini D. Epidemiology of allergic conjunctivitis: clinical appearance and treatment patterns in a population-based study. Curr Opin Allergy Clin Immunol. 2015;15(5):482–488. doi:10.1097/ACI.0000000000000204
2. Carr W, Schaeffer J, Donnenfeld E. Treating allergic conjunctivitis: a once-daily medication that provides 24-hour symptom relief. All Rhinol. 2016;7(2):107–114.
3. Rosario N, Bielory L. Epidemiology of allergic conjunctivitis. Curr Opin Allergy Clin Immunol. 2011;11(5):471–476. doi:10.1097/ACI.0b013e32834a9676
4. Meltzer EO, Farrar JR, Sennett C. Findings from an online survey assessing the burden and management of seasonal allergic rhinoconjunctivitis in us patients. J All Clin Immunol in Practice. 2017;5(3):779–89.e6. doi:10.1016/j.jaip.2016.10.010
5. Palmares J, Delgado L, Cidade M, Quadrado MJ, Filipe HP. Allergic conjunctivitis: a national cross-sectional study of clinical characteristics and quality of life. Europ J Ophthalmol. 2010;20(2):257–264. doi:10.1177/112067211002000201
6. Petersen KD, Kronborg C, Gyrd-Hansen D, Dahl R, Larsen JN, Løwenstein H. Quality of life in rhinoconjunctivitis assessed with generic and disease-specific questionnaires. Allergy. 2008;63(3):284–291. doi:10.1111/j.1398-9995.2007.01583.x
7. Virchow JC, Kay S, Demoly P, Mullol J, Canonica W, Higgins V. Impact of ocular symptoms on quality of life (QoL), work productivity and resource utilisation in allergic rhinitis patients--an observational, cross sectional study in four countries in Europe. J Med Econom. 2011;14(3):305–314. doi:10.3111/13696998.2011.576039
8. Bielory BP, O’Brien TP, Bielory L. Management of seasonal allergic conjunctivitis: guide to therapy. Acta Ophthalmologica. 2012;90(5):399–407. doi:10.1111/j.1755-3768.2011.02272.x
9. Bielory L, Delgado L, Katelaris CH, Leonardi A, Rosario N, Vichyanoud P. ICON: diagnosis and management of allergic conjunctivitis. Anna All Asthm Immunol. 2020;124(2):118–134. doi:10.1016/j.anai.2019.11.014
10. Varu DM, Rhee MK, Akpek EK, et al. Conjunctivitis preferred practice pattern®. Ophthalmology. 2019;126(1):94–169. doi:10.1016/j.ophtha.2018.10.020
11. Allergan. FML (Fluorometholone Ophthalmic Suspension, USP) [Prescribing Information]. Madison, NJ: Allergan; 2018.
12. Bausch + Lomb. LOTEMAX (Loteprednol Etabonate Ophthalmic Suspension) [Prescribing Information]. Bridgewater, NJ: Bausch + Lomb; 2016.
13. Alcon Laboratories, Inc. MAXIDEX (Dexamethasone Ophthalmic Suspension) [Prescribing Information]. Fort Worth, TX: Alcon Laboratories, Inc; 2017.
14. Porela-Tiihonen S. Recovery after cataract surgery. Acta Ophthalmologica. 2016;94(5):523–524. doi:10.1111/aos.13197
15. An JA, Kasner O, Samek DA, Lévesque V. Evaluation of eyedrop administration by inexperienced patients after cataract surgery. J Cataract Refract Surg. 2014;40(11):1857–1861. doi:10.1016/j.jcrs.2014.02.037
16. Newman-Casey PA, Robin AL, Blachley T, et al. The most common barriers to glaucoma medication adherence: a cross-sectional survey. Ophthalmology. 2015;122(7):1308–1316. doi:10.1016/j.ophtha.2015.03.026
17. American Academy of Ophthalmology. COVID-19 and Your Eye Care. 2020; Available from: https://www.aao.org/Assets/6d7c9a1a-9242-4326-a75d-9c6c9a827594/637208545943870000/coronavirus-and-your-eyes-pdf?inline=1.
18. Spencer SKR, Francis IC, Coroneo MT. Spontaneous face- and eye-touching: infection risk versus potential microbiome gain. Ocul Surf. 2021;21:64–65. doi:10.1016/j.jtos.2021.04.008
19. Ocular Therapeutix, Inc. DEXTENZA (Dexamethasone Ophthalmic Insert) [Prescribing Information]. Bedford, MA: Ocular Therapeutix, Inc; 2021.
20. Blizzard C, Desai A, Driscoll A. Pharmacokinetic studies of sustained-release depot of dexamethasone in beagle dogs. J Ocul Pharmacol Ther. 2016;32(9):595–600. doi:10.1089/jop.2016.0025
21. Tyson SL, Bafna S, Gira JP, et al. Multicenter randomized phase 3 study of a sustained-release intracanalicular dexamethasone insert for treatment of ocular inflammation and pain after cataract surgery. J Cataract Refract Surg. 2019;45(2):204–212. doi:10.1016/j.jcrs.2018.09.023
22. Walters TBS, Vold S, Bafna S, et al. Efficacy and safety of sustained release dexamethasone for the treatment of ocular pain and inflammation after cataract surgery: results from two phase 3 studies. J Clin Exp Ophthalmol. 2016;7(4):572. doi:10.4172/2155-9570.1000572
23. Abelson MB, Chambers WA, Smith LM. Conjunctival allergen challenge. A clinical approach to studying allergic conjunctivitis. Arch Ophthalmol. 1990;108(1):84–88. doi:10.1001/archopht.1990.01070030090035
24. Bergmann MT, Williams JI, Gomes PJ. Treatment of allergic conjunctivitis with bepotastine besilate ophthalmic solution 1.5%. Clin Ophthalmol. 2014;8:1495–1505.
25. Greiner JV, Mundorf T, Dubiner H, et al. Efficacy and safety of ketotifen fumarate 0.025% in the conjunctival antigen challenge model of ocular allergic conjunctivitis. Am J Ophthalmol. 2003;136(6):1097–1105. doi:10.1016/S0002-9394(03)00708-6
26. Meier EJ, Torkildsen GL, Gomes PJ, Jasek MC. Phase III trials examining the efficacy of cetirizine ophthalmic solution 0.24% compared to vehicle for the treatment of allergic conjunctivitis in the conjunctival allergen challenge model. Clin Ophthalmol. 2018;12:2617–2628. doi:10.2147/OPTH.S185835
27. Torkildsen G, Shedden A. The safety and efficacy of alcaftadine 0.25% ophthalmic solution for the prevention of itching associated with allergic conjunctivitis. Curr Med Res Opin. 2011;27(3):623–631. doi:10.1185/03007995.2010.548797
28. Abelson MB, Gomes PJ. Olopatadine 0.2% ophthalmic solution: the first ophthalmic antiallergy agent with once-daily dosing. Expert Opin Drug Metab Toxicol. 2008;4(4):453–461. doi:10.1517/17425255.4.4.453
29. Goldstein MH, Tubridy KL, Agahigian J, et al. A phase 2 exploratory study of a novel interleukin-1 receptor inhibitor (EBI-005) in the treatment of moderate-to-severe allergic conjunctivitis. Eye Contact Lens. 2015;41(3):145–155. doi:10.1097/ICL.0000000000000152
30. Torkildsen G, Abelson MB, Gomes PJ, McLaurin E, Potts SL, Mah FS. Vehicle-controlled, phase 2 clinical trial of a sustained-release dexamethasone intracanalicular insert in a chronic allergen challenge model. J Ocul Pharmacol Ther. 2017;33(2):79–90. doi:10.1089/jop.2016.0154
31. McLaurin EB, Evans D, Repke CS, et al. Phase 3 randomized study of efficacy and safety of a dexamethasone intracanalicular insert in patients with allergic conjunctivitis. Am J Ophthalmol. 2021;229:288–300. doi:10.1016/j.ajo.2021.03.017
32. McLaurin SM, Torkildsen G, Sato M, et al. Evaluating the Safety and Efficacy of DEXTENZA, a Dexamethasone Insert (0.4 mg) for the Treatment of Ocular Itching: results from Three Clinical Trials.
33. Walters T, Endl M, Elmer TR, Levenson J, Majmudar P, Masket S. Sustained-release dexamethasone for the treatment of ocular inflammation and pain after cataract surgery. J Cataract Refract Surg. 2015;41(10):2049–2059. doi:10.1016/j.jcrs.2015.11.005
34. Phulke S, Kaushik S, Kaur S, Pandav SS. Steroid-induced glaucoma: an avoidable irreversible blindness. J Curr Glauc Pract. 2017;11(2):67–72. doi:10.5005/jp-journals-10028-1226
35. Sen P, Jain S, Mohan A, Shah C, Sen A, Jain E. Pattern of steroid misuse in vernal keratoconjunctivitis resulting in steroid induced glaucoma and visual disability in Indian rural population: an important public health problem in pediatric age group. Indian J Ophthalmol. 2019;67(10):1650–1655. doi:10.4103/ijo.IJO_2143_18
36. Rosin LM, Bell NP. Preservative toxicity in glaucoma medication: clinical evaluation of benzalkonium chloride-free 0.5% timolol eye drops. Clin Ophthalmol. 2013;7:2131–2135.
37. Goldstein MH, Silva FQ, Blender N, Tran T, Vantipalli S. Ocular benzalkonium chloride exposure: problems and solutions. Eye. 2022;36(2):361–368. doi:10.1038/s41433-021-01668-x
38. Thygesen J. Glaucoma therapy: preservative-free for all? Clin Ophthalmol. 2018;12:707–717. doi:10.2147/OPTH.S150816
39. Garcia-Ferrer FJ, Akpek EK, Amescua G, et al. Corneal ectasia preferred practice pattern®. Ophthalmology. 2019;126(1):170–215. doi:10.1016/j.ophtha.2018.10.021
40. Léoni-Mesplié S, Mortemousque B, Mesplié N, et al. Epidemiological aspects of keratoconus in children. J Fr Ophtalmol. 2012;35(10):776–785. doi:10.1016/j.jfo.2011.12.012
41. Maharana PK, Sharma N, Vajpayee RB. Acute corneal hydrops in keratoconus. Indian J Ophthalmol. 2013;61(8):461–464. doi:10.4103/0301-4738.116062
42. Najmi H, Mobarki Y, Mania K, et al. The correlation between keratoconus and eye rubbing: a review. Int J Ophthalmol. 2019;12(11):1775–1781. doi:10.18240/ijo.2019.11.17
43. Maspero J, Lee BW, Katelaris CH, et al. Quality of life and control of allergic rhinitis in patients from regions beyond Western Europe and the United States. Clin Exp Allerg. 2012;42(12):1684–1696. doi:10.1111/j.1365-2222.2012.04025.x
44. Morthen MK, Magno MS, Utheim TP, Snieder H, Hammond CJ, Vehof J. The physical and mental burden of dry eye disease: a large population-based study investigating the relationship with health-related quality of life and its determinants. Ocul Surf. 2021;21:107–117. doi:10.1016/j.jtos.2021.05.006
45. Hom MM, Nguyen AL, Bielory L. Allergic conjunctivitis and dry eye syndrome. Ann Allergy Asthma Immunol. 2012;108(3):163–166. doi:10.1016/j.anai.2012.01.006
46. Villani E, Rabbiolo G, Nucci P. Ocular allergy as a risk factor for dry eye in adults and children. Curr Opin Allergy Clin Immunol. 2018;18(5):398–403. doi:10.1097/ACI.0000000000000471
47. Gomes PJ, Ousler GW, Welch DL, Smith LM, Coderre J, Abelson MB. Exacerbation of signs and symptoms of allergic conjunctivitis by a controlled adverse environment challenge in subjects with a history of dry eye and ocular allergy. Clin Ophthalmol. 2013;7:157–165. doi:10.2147/OPTH.S38732
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.