")
Back to Journals » Journal of Inflammation Research » Volume 17
A Role for Systemic Inflammation in Stroke-Associated Infection and the Long-Term Prognosis of Acute Ischemic Stroke: A Mediation Analysis
Authors Huang S, Xie W, Gao Y, Jin Y, Chen Y, Zhou G, Chen F, Jin Q, Wu Z, Wang L, Chen C, Weng Y , Chen G
Received 25 June 2024
Accepted for publication 7 September 2024
Published 19 September 2024 Volume 2024:17 Pages 6533—6545
DOI https://doi.org/10.2147/JIR.S474344
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Suwen Huang,1,* Wei Xie,1,2,* Yufan Gao,1,3,* Yining Jin,1,3 Yilin Chen,1,2 Guoliang Zhou,1,2 Feng Chen,1,2 Qiaoqiao Jin,1,2 Zihao Wu,1,2 Lingsheng Wang,1,2 Chao Chen,4 Yiyun Weng,1 Guangyong Chen5
1Department of Neurology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China; 2The First School of Medicine, School of Information and Engineering, Wenzhou Medical University, Wenzhou, People’s Republic of China; 3The Second School of Medicine, Wenzhou Medical University, Wenzhou, People’s Republic of China; 4Department of Nutriology, The Third Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China; 5Department of Neurology, The Third Affiliated Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guangyong Chen, Department of Neurology, The Third Affiliated Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China, Email [email protected] Yiyun Weng, Department of Neurology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China, Email [email protected]
Background and Purpose: The dynamic systemic inflammation level and stroke-associated infection (SAI) are related to the prognosis of acute ischemic stroke (AIS). We aimed to explore whether the systemic inflammatory response index (SIRI), systemic immune inflammation index (SII), and their dynamic changes possess predictability for SAI and long-term prognosis.
Methods: A total of 1804 AIS patients without intravenous thrombolysis in two hospitals were included. We explored the relationship between SIRI, SII, and their dynamic changes and outcomes by constructing clusters. The mediating effects of SAI between prognosis and systemic inflammation were further evaluated.
Results: Each SD increase in the concentration of SIRI exhibited a significant correlation with the risk of poor functional outcome, mortality, and functional dependency. Through K-means clustering analysis, patients with dramatically elevated or decreased systemic inflammation levels of SIRI (OR: 2.293, 95% CI: 1.279– 4.109) and SII (OR: 3.165, 95% CI: 1.627– 6.156) within 7 days had a higher risk of functional outcome. Through mediation analysis, SAI mediated the association between systemic inflammation and poor prognosis (SIRI: 33.73%, SII: 16.01%).
Conclusion: Dramatically changing dynamics of SIRI and SII were significantly associated with a higher risk of poor prognosis in AIS patients. SAI mediated the association between systemic inflammation and prognosis at 1 year.
Keywords: AIS, inflammation, SAI, mediation analysis, clustering analysis
Introduction
Acute ischemic stroke (AIS) is a significant type of stroke and is the leading cause of disability and death globally.1 Although endovascular therapies and intravenous thrombolysis (IVT) have been used extensively, they only benefit a small proportion of patients.2 So far, the overall IVT rate in China is still below 10%, rendering the population without IVT considerable.3 Hence, finding valuable biomarkers to improve risk stratification and prevent adverse outcomes in AIS patients is essential.
Inflammatory cascade has been identified as a crucial pathogenic process in AIS and a potential starting point for predicting stroke recovery.4,5 Therefore, inflammatory biomarkers are expected to help predict the functional prognosis of AIS patients. As relatively new markers of systemic inflammation, systemic inflammatory response index (SIRI) and systemic immune inflammation index (SII) can be assessed using biochemical or hematological markers routinely measured in standard blood tests or as ratios derived from these measurements: SIRI was defined as (neutrophil count × monocyte count)/lymphocyte count, and SII was defined as (neutrophil count × platelet count)/lymphocyte count.6 Compared to other commonly used inflammatory markers, SIRI and SII demonstrate superior efficacy in assessing the balance between the inflammatory response and immune status. They have been widely linked to the prediction of cancer and autoimmune diseases in several studies.7–9 To the best of our knowledge, there remains a dearth of research investigating the dynamic fluctuations in systemic inflammation levels among patients with AIS during hospitalization.
Ischemic stroke has complex pathophysiological mechanisms, and the inflammatory response starts quickly after brain injury and lasts for days, weeks, or even months.5 Therefore, when it comes to AIS patient prognosis, the assessment of patients’ dynamic systemic inflammation levels will be more comprehensive. To the best of our knowledge, there remains a dearth of research investigating the dynamic fluctuations in systemic inflammation levels among patients with AIS during hospitalization.
Meanwhile, stroke-associated infection (SAI) is a common stroke-associated complication, which is defined as an infection diagnosed during the hospitalization period.10 SAI occurs in up to 30% of patients with stroke, and the most common infections are urinary tract infections (UTIs) and stroke-associated pneumonia (SAP).11 Previous studies have demonstrated that SAI could lead to negative consequences and even death for stroke patients.10,12 Some studies have determined the application potential of SIRI and SII in the early identification of the severity of SAP.13,14 Still, few studies have linked systemic inflammatory levels to SAI and prognosis in the AIS population. A better understanding of the associations between dynamic systemic inflammatory markers and the long-term outcomes for AIS is necessary to assess systemic inflammatory markers’ potential as biomarkers for earlier identification of the disease prognosis. The objective of this study was to investigate the association between systemic inflammatory markers and their dynamic changes, as well as their impact on long-term prognosis in patients with AIS while also examining the potential mediating role of SAI.
Methods
Study Population
In this retrospective cohort study, a total of 3099 AIS participants without IVT from January to December 2020 hospitalized in the First Affiliated Hospital of Wenzhou Medical University (derivation study) and the Third Affiliated Hospital of Wenzhou Medical University (validation study) were retrospectively recruited. They were diagnosed with AIS according to the World Health Organization criteria and had complete baseline and follow-up data. The exclusion criteria were as follows:15–17 (1) patients with severe diseases such as kidney failure, severe hepatic insufficiency, or cancer; (2) patients with autoimmune diseases; (3) patients using immunosuppressive drugs or use of antibiotics; (5) patients with pre-hospital infection or with infections within 48h after admission. Finally, 1804 patients in these two hospitals were enrolled in this study (Supplementary Figure 1). On this basis, we conducted a comprehensive analysis of the dynamic levels of systemic inflammation in patients with hospitalization duration ≥7 days. The study was approved by the Institutional Ethics Committee review board of the First Affiliated Hospital of Wenzhou Medical University and the Third Affiliated Hospital of Wenzhou Medical University, which was performed following the Declaration of Helsinki.
Data Collection
All patients’ baseline data, including demographic characteristics (sex, age), personal history data (smoking, drinking), medical history data (previous stroke, hypertension, diabetes, coronary artery disease [CAD], and atrial fibrillation [AF]), clinical features (National Institutes of Health Stroke Scale [NIHSS], modified Rankin Scale [mRS], Barthel Index [BI]), and SAI were obtained through electronic medical records. Patients were diagnosed with hypertension if they had evidence of systolic blood pressure ≥140 mmHg and diastolic blood pressure ≥90 mmHg or had received any antihypertensive medication. Diabetes was defined as a fasting serum glucose level ≥126 mg/dL, a serum glucose level ≥200 mg/dL on 2 random measurements, a glycated hemoglobin level ≥6.5%, or having received antidiabetic therapy (oral hypoglycemic agents or insulin). CAD was defined by a previous history of CAD. AF was defined by a previous history of AF or a diagnosis of AF by electrocardiography. Smoking and drinking status were defined based on current use. SAI was defined as any infection diagnosed during the hospitalization period of AIS patients. Two experienced physicians who were blinded to the clinical and laboratory results of the patients independently diagnosed.
The etiology classification was large-artery atherosclerosis (LAA), cardio embolism (CE), small-artery occlusion (SAO), stroke of other determined etiology (SOE), or stroke of undetermined etiology (SUE) according to the Trial of Org 10172 in acute stroke treatment (TOAST) classification, and other determined cause and undetermined cause are defined as others.18 Laboratory examinations, including blood routine examinations, were performed within 24 hours of admission. The value of the SIRI was defined as (neutrophil count × monocyte count)/lymphocyte count, and SII was defined as (neutrophil count × platelet count)/lymphocyte count.7,19
Clinical Outcomes
The primary outcome was poor functional outcome which was assessed with the mRS score (3–6) 1 year after the stroke onset. The secondary outcomes were mortality (mRS = 6) and functional dependency 1 year after the stroke onset. The mRS score ranges from 0 to 6, with 0 indicating no disability and higher scores indicating more severe disability. The mRS score of 0 to 2 was defined as a favorable functional outcome, and the score of 3 to 6 was defined as a poor functional outcome.20 The functional dependency was assessed with the BI score which ranges from 0 to 100. A higher score indicates better daily self-care ability. The patients with BI < 60 were indicated to have functional dependency.21
Statistical Analysis
Data were first analyzed for normality of distribution by using the Kolmogorov–Smirnov test. Continuous variables were presented as medians and interquartile range (median, IQR), and categorical variables were presented as numbers and percentages (%). For more detailed information on systemic inflammatory markers and long-term prognosis, mRS grouping was used to classify and compare baseline characteristics. The Mann–Whitney U-test was used to compare the groups involving continuous variables, and the chi-square test or Fisher’s exact test was used to compare the groups involving categorical variables. Based on logistic and Cox regression models, associations between SIRI, SII, and long-term prognosis outcomes were measured by odds ratios (ORs), hazard ratios (HRs), and 95% confidence intervals (CIs). Factors known to be associated with stroke prognosis outcomes were included in the analyses as confounders, which included demographics (age, sex), NIHSS at admission, smoking, drinking, medical history (hypertension, diabetes, previous stroke, CAD, AF), and TOAST subtype. In multivariate regression analysis, we adjusted for covariates with p-values <0.05 in univariate regression analysis (Supplementary Table 1): age, sex, NIHSS at admission, smoking, drinking, hypertension, diabetes, previous stroke, CAD, AF, SAI, and TOAST subtype. Moreover, SIRI and SII were standardized, with increments of 1 standard deviation (SD), to facilitate determining its effect. Restricted cubic splines with 5 knots (at the 5th, 27.5th, 50th, 72.5th, and 95th percentiles) were also plotted to demonstrate the correlation between systemic inflammatory markers and functional outcomes.
In addition to this, propensity score matching (PSM) analysis was further applied to address the potential residual confounding effect of covariates to examine the robustness of our results. We utilized the MatchIt package in R to match the mRS 0–2 group and the mRS 3–6 group at a 1:1 ratio (maximum caliper width, 0.2), nearest neighbor matching without replacement, and a conditional logistic regression model for estimating propensity scores.
During 24 hours and the seventh day of admission, the data set of transition of the SIRI and SII was analyzed and classified into 3 clusters using k-means clustering analysis (Figure 1): for SIRI cluster 1 (n = 894), the SIRI ranged from 1.43 in 24h to 1.53 in 7 days, representing a stable SIRI; for SIRI cluster 2 (n = 61), the SIRI ranged from 7.16 in 24h to 3.00 in 7 days, representing a moderate SIRI with a dramatically downward trend; for SIRI cluster 3 (n = 67), the SIRI ranged from 3.23 in 24h to 7.34 in 7 days, representing a moderate SIRI with a dramatically rising trend. For SII cluster 1 (n = 912), the SII ranged from 578.99 in 24h to 611.43 in 7 days, representing a stable or slow-rising SII; for SII cluster 2 (n = 63), the SII ranged from 2236.84 in 24h to 1345.28 in 7 days, representing a high level of SII with the dramatically downward trend; for SII cluster 3 (n = 50), the SII ranged from 1028.67 in 24h to 2430.06 in 7 days, representing a high level of SII with the dramatically rising trend. Upon establishing clusters of the change in SIRI and SII, we examined the association between different clusters with changes in SIRI and SII and long-term outcomes by binary logistic models and Cox regression models.
 |
Figure 1 Clustering of the change in the systemic inflammation markers from 24h to 7 days after admission. Dynamic SIRI and SII scatter plots of different clusters after K-means clustering (A and C). Line chart of dynamic SIRI and SII after K-means clustering (B and D). Abbreviations: SIRI, systemic inflammation response index; SII, systemic immune inflammation index. |
To explicate the association between systemic inflammatory markers at baseline and prognosis outcomes, indirect associations acting through SAI as a mediating variable and direct associations not mediated by SAI were quantified by using the R mediation package (Figure 2). The total effect can be divided into two components: the natural direct effect (NDE) and the natural indirect effect (NIE). The NDE represented the effect of systemic inflammation on poor prognosis that was independent of SAI. An NIE represented the effect of systemic inflammation on poor prognosis that could be explained by changes in the status of SAI. The mediation effect is measured by the percentage mediated, which is the percentage of the total effect that is mediated by the mediator. To test the robustness of our analysis, subgroup analyses were performed. We performed a mediation analysis stratified by age (age ≥ 65, age < 65), sex (male, female), hypertension (Yes, NO), and diabetes (Yes, NO). A double-sided p < 0.05 was regarded as statistically significant. All statistical analysis was performed using SPSS Statistics 26.0 software (SPSS Inc., Chicago, IL) and R version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria).
 |
Figure 2 Illustration of mediation effect. Abbreviations: NDE, natural direct effect; NIE, natural indirect effect. |
Results
Baseline Characteristics
In this study, a total of 1804 patients with AIS were enrolled. In the derivation study, the median age of the included patients was 67 (59–76) years, and 835 (65.85%) were men. The most common disease was hypertension (n = 828 [65.30%]), followed by diabetes (n = 369 [29.10%]) and previous stroke (n = 165 [13.01%]). Over half of the patients had LAA (n = 750 [59.15%]), and one in five had SAO (n = 275 [21.69%]). The median SIRI for all included participants was 1.23 (0.82–2.01), and the median SII for all included participants was 531.28 (368.99–772.43) (Table 1). The baseline characteristics of patients with AIS divided according to mRS were shown in Table 1. Enrolled individuals were divided into two groups according to the mRS at 1 year (mRS: 0–2, mRS: 3–6). Patients with poor functional outcomes tended to be older (66 [57–73] vs 76 [69–82], p < 0.001), had higher NIHSS on admission (4 [2–6] vs 8, [5–12] p < 0.001), and had a higher proportion of hypertension (656 [63.44%] vs 172 [73.50%], p = 0.004), diabetes (287 [27.76%] vs 82 [35.04%], p = 0.027), previous stroke (118 [11.41%] vs 47 [20.09%], p < 0.001), CAD (16 [1.55%] vs 13 [5.56%], p < 0.001), AF (47 [4.55%] vs 24 [10.26%], p < 0.001), and SAI (68 [6.58%] vs 24 [26.50%], p < 0.001). The elevated SIRI levels (1.15 [0.79–1.77] vs 1.98 [1.14–3.45], p < 0.001) and elevated SII (503.66 [348.04–721.10] vs 705.41 [433.77–1245.71], p < 0.001) levels were observed in patients with poor functional outcomes at 1 year. The baseline characteristics of the validation study were shown in Supplementary Table 1. The differences between groups in baseline characteristics were similar to those in the derivation cohort.
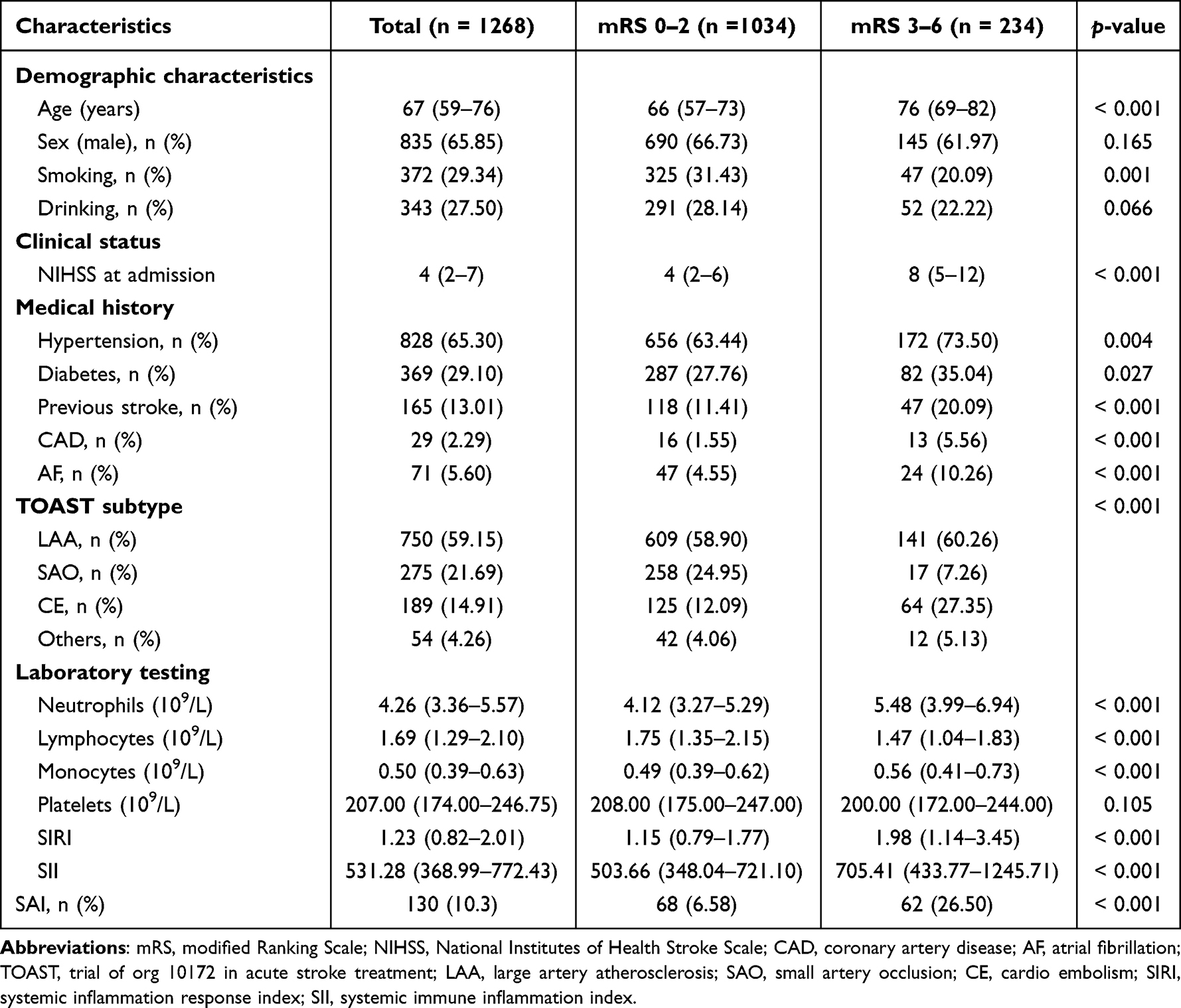 |
Table 1 Baseline Characteristics of Subjects Divided by mRS at 1 Year in the Derivation Study |
Association Between Systemic Inflammatory Markers and Long-Term Prognosis
The univariate binary logistic regression and Cox regression results for the risk of poor functional outcome in AIS patients and variables with analysis that may influence prognosis were obtained from clinicians’ suggestions and clinical experience (Supplementary Table 2). Table 2 shows the prognosis outcomes after 1 year across quartiles of systemic inflammatory markers in the derivation study. After adjusting for age, sex, smoking, drinking, hypertension, diabetes, previous stroke, CAD, AF, TOAST subtype, NIHSS at admission, and SAI, we found that compared with the first quartile of SIRI and SII, the highest quartile of SIRI and SII were associated with an increased risk of poor functional outcome (OR: 2.198, 95% CI: 1.264–3.822; OR: 2.638, 95% CI: 1.501–4.637), mortality (HR: 5.154, 95% CI: 1.185–22.408; HR: 2.994, 95% CI: 1.135–7.898). The highest quartile of SII was associated with an increased risk of functional dependency at 1 year (OR: 2.894, 95% CI: 1.093–7.659). However, SIRI was not statistically significant in functional dependency. Each SD increase in the concentration of SIRI exhibited the most significant correlation with the risk of poor functional outcome (OR: 1.333, 95% CI: 1.105–1.609), and mortality (HR: 1.563, 95% CI: 1.121–2.179). Each SD increase in the concentration of SII exhibited the most significant correlation with the risk of functional dependency (OR: 1.224, 95% CI: 1.040–1.441). In addition, we found that higher SIRI and SII were associated with the risk of SAI (OR: 3.088, 95% CI: 1.659–5.749; OR: 2.655, 95% CI: 1.490–4.731).
 |
Table 2 Multivariate Regression Analysis for Systemic Inflammation Markers with Outcomes at 1 Year in Derivation Study |
Furthermore, the restricted cubic splines regression model was used to reveal that the risk of poor functional outcome, mortality, and functional dependency at 1 year increased linearly with SIRI levels (p for nonlinearity = 0.114, p for nonlinearity = 0.404 and p for nonlinearity = 0.078, respectively) (Supplementary Figure 2). The risk of mortality at 1 year increased linearly with SII levels (p for nonlinearity = 0.226). Still, the risk of poor functional outcome and functional dependency at 1 year increased nonlinearly with SII levels (p for nonlinearity = 0.008, p for nonlinearity = 0.043).
In the validation study, by multivariable logistics and Cox regression using these predictors, the SIRI remained the significant predictor of poor functional outcome (OR: 1.307, 95% CI: 1.007–1.698, per 1 SD), mortality (HR: 1.335, 95% CI: 1.040–1.712, per 1 SD) (Supplementary Table 3). The SII remained the significant predictor of mortality (HR: 1.560, 95% CI: 1.158–2.103, per 1 SD).
PSM Analysis of Systemic Inflammatory Markers and Long-Term Prognosis
To eliminate bias between the two groups, PSM was performed between derivation and validation study, and 650 patients were successfully matched in a 1:1 ratio in Supplementary Table 4. No significant differences were observed in age, sex, smoking, drinking, NIHSS at admission, medical history, and SAI between the two groups after PSM (p-value > 0.05). The conditional logistic regression analysis for outcomes after 1:1 PSM was shown in Supplementary Table 5. Regardless of whether PSM is performed or not, both SIRI and SII were associated with the outcomes at 1 year (Supplementary Table 5).
Dynamic Analysis of Systemic Inflammation and Long-Term Prognosis
To expand the sample size of dynamic analysis, we combine derivation and validation study for dynamic analysis derivation and validation study by K-means clustering analysis. Figure 1 shows the dynamic changes and density distribution of SIRI and SII based on the constructed clusters. Table 3 shows the associations between the change in systemic inflammation and prognosis outcomes after 1 year. After adjusting for potential confounders, compared with SIRI cluster 1 (patients with stable SIRI), SIRI cluster 2 (patients with dramatically downward trend SIRI) was associated with an increased risk of poor functional outcome (OR: 2.293, 95% CI: 1.279–4.109), mortality (HR: 3.113, 95% CI: 1.160–8.351), and functional dependency (OR: 2.103, 95% CI: 1.070–4.134). Compared with SIRI cluster 1 (patients with stable SIRI), SIRI cluster 3 (patients with dramatically rising SIRI) was associated with an increased risk of mortality (HR: 2.691, 95% CI: 1.077–6.722). After adjusting for potential confounders, compared with SII cluster 1 (patients with stable SII), SII cluster 2 (patients with dramatically downward trend SII), and SII cluster 3 (patients with dramatically downward trend SII) were associated with an increased risk of poor functional outcome (OR: 3.165, 95% CI: 1.627–6.156; OR: 2.085, 95% CI: 1.007–4.318), and functional dependency (OR: 5.134, 95% CI: 2.255–11.690; OR: 2.619, 95% CI: 1.150–5.967), while the others were not statistically significant. In the sensitivity analysis of the dynamic data, we repeated the logistic regression separately in the patients in clusters 1 and 2 (stable or downward trend), and associations of systemic inflammation markers with outcomes remained significant (Supplementary Table 6).
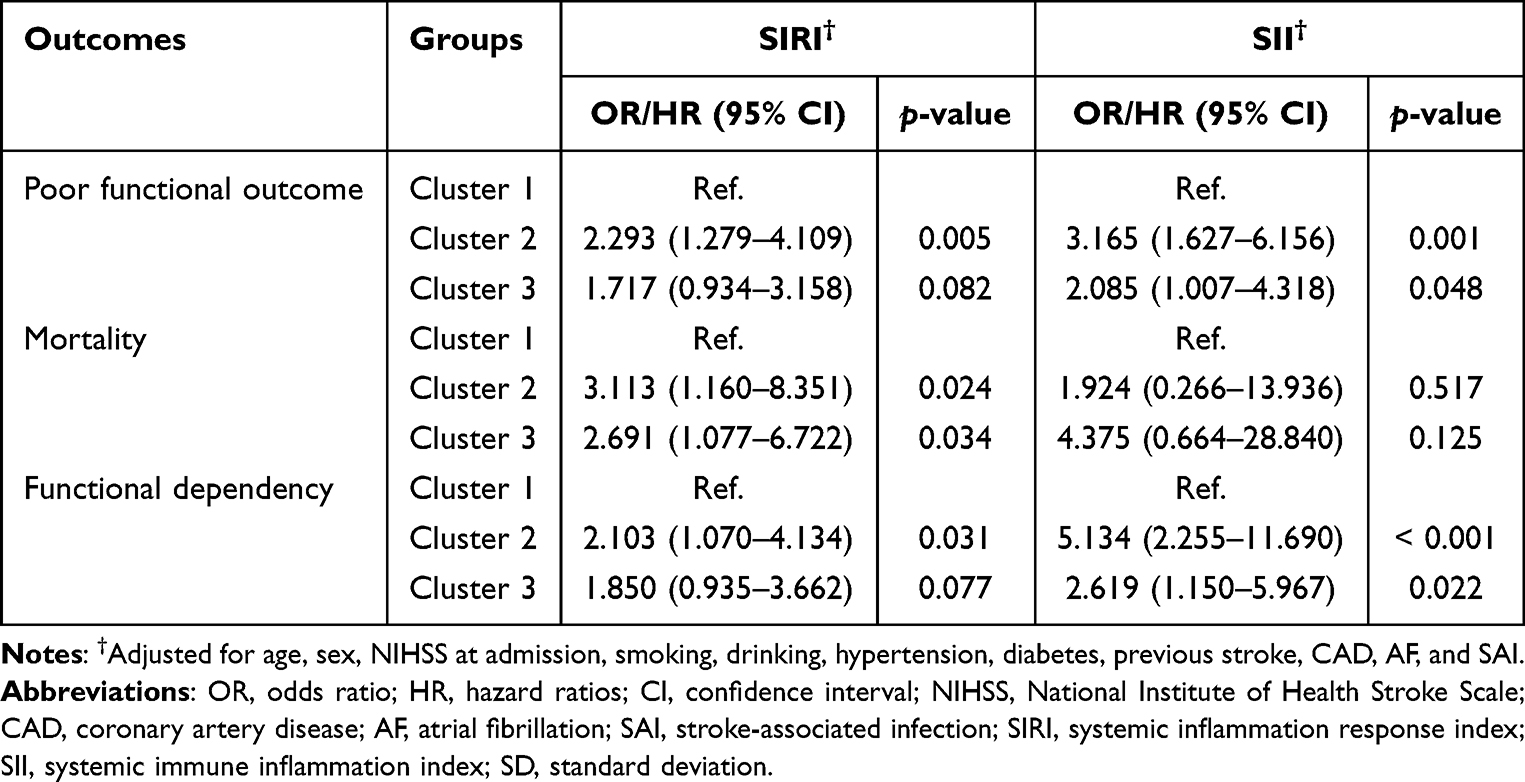 |
Table 3 Multivariate Regression Analysis for Different Dynamic Change Classes of Systemic Inflammation Markers with Outcomes at 1 Year |
Mediation Analysis of Systemic Inflammation, SAI, and Prognosis
The boxplots showed that the SIRI (1.19 [0.81–1.85] vs 2.47 [1.13–4.27], p < 0.001) and SII (510.87 [359.33–731.10] vs 823.39 [482.11–1313.49], p < 0.001) of AIS patients with SAI were much higher than patients without SAI in the derivation study (Supplementary Figure 3A and B). The accumulative bar diagram showed that the proportion of AIS patients who were complicit in SAI with poor functional outcomes was much higher than patients without SAI (15.11% vs 47.70%, p < 0.001) (Supplementary Figure 3C). Therefore, SAI may affect patients’ long-term outcomes to some extent. Based on this conjecture, we conducted further research.
The results of the mediation analysis of SAI in systemic inflammation markers on poor prognosis at 1 year were presented in Figure 3. After adjusting for potential confounders, the percentage of SAI-mediated association in the association between SIRI and poor functional outcome was 33.73% (95% CI: 16.48–77.56%), mortality was 20.62% (95% CI: 7.64–75.11%), and functional dependency was 16.03% (95% CI: 7.73–29.07%). The mediated percentage between SII and poor functional outcomes was 16.01% (95% CI: 6.23–43.55%), mortality was 15.12% (95% CI: 6.67–52.26%), and functional dependency was 9.96% (95% CI: 4.17–19.27%).
 |
Figure 3 Mediation analysis of systemic inflammation markers (A) SIRI, (B) SII for outcomes through SAI at 1 year. Adjusted for age, sex, NIHSS on admission, smoking, drinking, hypertension, diabetes, previous stroke, CAD, and AF. Abbreviations: CI, confidence interval; SIRI, systemic inflammation response index; SII, systemic immune inflammation index; NIHSS, National Institute of Health Stroke Scale; CAD, coronary artery disease; AF, atrial fibrillation; SAI, stroke-associated infection.. |
Furthermore, the mediation analysis was stratified by age (age ≥ 65, age < 65), sex (male, female), hypertension (Yes, NO), and diabetes (Yes, NO). The mediated effects of SAI were found to be contingent upon specific factors such as sex, and age. SAI more powerfully mediated the association between SIRI and poor prognosis at 1 year in older (28.09%), male (20.78%) patients with hypertension (24.92%), and without diabetes (36.07%). Similar results were found in the association between SII and poor prognosis at 1-year older (9.35%), male (10.06%), patients with hypertension (12.39%), and without diabetes (12.17%) (Figure 4). At the same time, the mediating effects in younger female patients without hypertension and with diabetes were not statistically significant. In the outcomes of mortality and functional dependence, the above conclusions remained stable (Supplementary Tables 7 and 8).
Discussion
In this retrospective cohort study, we observed that the severity of systemic inflammation during hospitalization was associated with a higher risk of long-term poor prognosis in AIS patients. In particular, both sharply elevated or declined systemic inflammation markers in the hospital may predict a poor long-term prognosis and a higher risk of mortality. In addition, we found that SAI mediated the association between systemic inflammation and poor prognosis at 1 year among patients with AIS, especially in older male patients with hypertension and without diabetes. This finding may support the hypothesis that systemic inflammation state at admission may increase the risk of SAI during hospitalization, which, in turn, increases the risk of prognostic impairment. These results can provide additional prognostic information for physicians to help formulate rehabilitation treatment for patients with ischemic stroke.
A growing number of studies have shown the relevance of neuroinflammation in the pathogenesis of stroke.22–25 On the one side, ischemic stroke results in neuronal cell death and releases factors such as damage-associated molecular patterns (DAMPs), which can strongly and effectively activate immune active cells, such as microglia and astrocytes. On the other side, the release of DAMPs into the blood circulation can promote the inflammatory cells, such as neutrophils and monocytes, to invade the brain and activate the complex immune response of stroke.22,24 In addition, inflammation can induce endothelial cell activation and facilitate the adhesion and migration of those inflammatory cells to the brain parenchyma and microvessels from a systematic perspective.24 By releasing pro-inflammatory factors, proteases, matrix metalloproteinase (MMPs), and other molecules, the recruited neutrophils and monocytes can cause injury.23 It is also now well documented that neuroinflammation and immune mediators play a crucial role in neuronal tissue damage and healing in the distal regions, termed sites of secondary neurodegeneration (SND).25 This represents how inflammation affects nerve damage on a broader scale. Recently, one study reported on the involvement of peripheral infiltrating immune cells, especially lymphocytes, in distal regions of the brain post-stroke.26 Some animal stroke experiments have suggested that increased lymphocytes up-regulate the levels of IL-10 and inhibit inflammatory cytokines such as IL-6 and TNF-α, thus playing a neuroprotective role.27 Contrastingly, a study highlighted that lymphocytes were not neurotoxic.28 As such, it is still uncertain whether lymphocytes have a harmful or protective effect after stroke. Despite ongoing debate about their specific role, it is generally accepted that lymphocytes have a negative impact after an ischemic injury. Platelets play a role in the formation of atherosclerosis and atherothrombosis, which is a critical process during the pathophysiology of stroke. When AIS occurs, blood stagnation flow produces shear stress on endothelial cells and platelets, thus resulting in the deployment of P-selectin of the adhesion molecules to the cell surface. Platelets interact directly with circulating leukocytes by changing the surface expression of P-selectin or CD40, thereby forming platelet-leukocyte aggregates and activating the innate immune response to ischemic, thus exacerbating stroke.29 An experiment conducted on mice demonstrated that necrotic platelets interact with neutrophils, thereby exacerbating brain injury during ischemic stroke through the regulation of cyclophilin D, a mediator of necrosis.30 Therefore, SIRI and SII, integrating the above-mentioned inflammatory cells, may correlate with the stroke prognosis.
SAI is a significant complication of stroke and has attracted increasing attention in recent years since it was reported to be one of the leading causes of mortality after acute stroke. However, the underlying mechanism of SAI remained unclear, posing a challenge for clinicians. An increasing body of preclinical and clinical evidence suggests that persistent infection is emerging as an essential mechanism of prognosis impairment in patients with AIS.31,32 The durative inflammatory process will consume many immune substances in patients’ bodies, significantly reducing systemic immune activity and forming systemic immunosuppression. This increases the susceptibility of patients to infection after stroke and provides a favorable hotbed for the occurrence of SAI. Peripheral infections can further affect the neuroinflammation of the central nervous system, so the neuroinflammatory response in SAI patients will be more intense.32,33 There is evidence that sympathetic activation and the attendant release of stress steroids and catecholamines are involved.34 Our study found that SAI patients had worse outcomes than non-SAI patients (Supplementary Figure 3), which directly confirmed the view of the above study. It is important to note that patients with infections experience a delayed recovery of lymphocytes, which contributes to a high level of systemic inflammation markers and hinders the improvement of neurological function.35 Our research also identified that the mediation effects of SAI had sex-specificity, age-specificity, and etiological-specificity (Table 2, Supplementary Tables 2 and 3). Although the prognosis for female patients with AIS is generally worse, previous studies have found that the changes in the gut microbiota of men can also exacerbate the level of systemic inflammation and stroke prognosis.36 Meanwhile, hypertension can alter cerebrovascular structure and function induced, which may explain why the mediation effects were stronger in AIS with hypertension in our study.37
According to the statistical results in our study, after adjusting for confounders, the highest quartiles of both SIRI and SII were highly associated with long-term poor outcomes (Table 2). In conclusion, when patients’ SIRI > 2.01, or SII > 799.00, physicians should prioritize monitoring the patient’s conditions and proactively administer anti-inflammatory treatment. Further, compared with SII, SIRI had a higher capability for long-term poor prognosis, and its mediated percentages were more significant (Table 2 and Figure 4). This implies that to predict outcomes based on systemic inflammatory levels, physicians could prioritize the use of SIRI over SII. Our analysis revealed that about 20% of long-term poor prognosis variance could be explained by SAI. So, for patients with high levels of systemic inflammation, physicians need to pay special attention to the prevention of SAI: physicians should pay attention to oral hygiene, and timely removal of oral secretions, food debris, vomit, and gastroesophageal reflux for conscious disorders and swallowing disorders patients; physicians also should reduce the use of glucocorticoids, proton pump inhibitors, H2 blockers, sedatives, and muscle relaxants to prevent SAI.38 By timely prevention of SAI, physicians can effectively improve the prognosis of AIS patients. Although 20% of long-term poor prognosis variance could be explained by SAI, 80% of nerve injury results from the pathway between systemic inflammation and poor prognosis without mediation. Therefore, the secondary prevention strategies for preventing SAI are far from sufficient to improve the prognosis, and anti-inflammatory therapy should be given more attention from the perspectives of both acute-phase and later-phase mechanisms. For example, pre-clinical studies have confirmed that natalizumab can reduce infarct volume and leukocyte invasion into the brain after cortical stroke.39 Fingomode, as an immunomodulatory drug, reduces infarct volume in a mouse transient ischemia-reperfusion model by inducing lymphopenia.40 At present, the Phase III clinical trial of edaravone dextrocamphorol injection has demonstrated that it can significantly improve functional outcomes in patients with acute ischemic stroke and is one of the few agents with significant anti-inflammatory effects after stroke.41
 |
Figure 4 Mediation analysis of SIRI and SII for poor functional outcome at 1year through SAI stratified by prespecified subgroups. Adjusted for age, sex, NIHSS on admission, smoking, drinking, hypertension, diabetes, previous stroke, CAD, and AF. The asterisk *Indicates p< 0.05. Abbreviations: SIRI, systemic inflammation response index; SII, systemic immune inflammation index; NIHSS, National Institute of Health Stroke Scale; CAD, coronary artery disease; AF, atrial fibrillation; SAI, stroke-associated infection. |
The role of SIRI and SII in predicting patient outcomes has gained attention lately. However, to date, studies based on patient SIRI and SII levels and poor prognosis of patients with ischemic stroke are still scarce. A few studies demonstrated that SIRI was a significant predictor of poor outcomes at 3 months.42,43 What’s more, a study proved that SII and SIRI can predict the occurrence of stroke-associated pneumonia and poor outcomes at discharge in intracerebral hemorrhage patients.44 Another research also showed that elevated SIRI levels were significantly associated with the risk of stroke and its subtypes in elderly patients with hypertension, which this result fits neatly into our mediation analysis stratified by prespecified subgroups. Compared with other studies of AIS, our study has the following advantages. First, we used SIRI and SII, a convenient and accessible indicator for systemic inflammation, to explore the association between systemic inflammation and prognosis. Second, we have a longer follow-up time of 1 year, which suggests that systemic inflammation markers have a greater predictive ability of functional prognosis in patients with AIS. Third, this study, along with the findings of earlier studies, has led to a more comprehensive analysis: SAI can mediate systemic inflammation and indirectly affect the prognostic level of patients.
There are still some limitations in our study. First, the retrospective design of this study limited the ability to validate the causality between systemic inflammation markers and function prognosis or SAI. Second, this was a small sample study conducted in a single center. Third, other potential confounders that have yet to be considered may bias our analysis. Fourth, although we excluded infection events detected before admission, elevated systemic inflammation markers may indicate an underlying, undetected, but already established inflammatory process associated with SAI. Fifth, blood laboratory data displayed a skewed distribution, which may bias the estimation of mediating effects. To mitigate the potential influence, analysis on the per 1 SD effect of the systemic inflammation markers was replenished, revealing consistent and robust results and thus authenticating our conclusions. The results of this study provide new information for long-term prognosis prediction of patients with AIS. However, further investigations are required to explore the relevant mechanisms underlying the findings of this study.
Conclusions
Elevated SIRI and SII levels were associated with an increased risk of long-term poor functional outcomes in patients with AIS. Patients with elevated SII levels in the hospital may predict a poor long-term prognosis and a higher risk of mortality. SAI mediated the association between systemic inflammation and poor prognosis at 1 year among patients with AIS, especially in older male patients with hypertension, and without diabetes.
Data Sharing Statement
The data supporting this study’s findings are available from the corresponding author, Guangyong Chen, upon reasonable request.
Ethics Approval and Consent to Participate
The article did not have specific personal privacy, but we had ethical approval (approval number: YJ2020034) and patient-informed consent.
Consent for Publication
All authors have read the manuscript and approved its publication.
Acknowledgments
We sincerely thank the participating hospital, patients, their families, and colleagues who have provided valuable suggestions for this study.
Author Contributions
Co-first author: Suwen Huang, Wei Xie and Yufan Gao. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Wenzhou Municipal Sci-Tech Bureau Program (No. Y20210585).
Disclosure
The authors declare that they have no competing interests.
References
1. Campbell BCV, Khatri P. Stroke. Lancet. 2020;396:129–142. doi:10.1016/S0140-6736(20)31179-X
2. Macrez R, Ali C, Toutirais O, et al. Stroke and the immune system: From pathophysiology to new therapeutic strategies. Lancet Neurol. 2011;10:471–480. doi:10.1016/S1474-4422(11)70066-7
3. Ye Q, Zhai F, Chao B, et al. Rates of intravenous thrombolysis and endovascular therapy for acute ischaemic stroke in China between 2019 and 2020. Lancet Reg Health West Pac. 2022;21:100406. doi:10.1016/j.lanwpc.2022.100406
4. Anrather J, Iadecola C. Inflammation and stroke: An overview. Neurotherapeu. 2016;13:661–670. doi:10.1007/s13311-016-0483-x
5. Fu Y, Liu Q, Anrather J, Shi FD. Immune interventions in stroke. Nat Rev Neurol. 2015;11:524–535. doi:10.1038/nrneurol.2015.144
6. Zhao Y, Hong X, Xie X, et al. Preoperative systemic inflammatory response index predicts long-term outcomes in type B aortic dissection after endovascular repair. Front Immunol. 2022;13:992463. doi:10.3389/fimmu.2022.992463
7. Cao Y, Zheng X, Hu Y, et al. Levels of systemic inflammation response index are correlated with tumor-associated bacteria in colorectal cancer. Cell Death Dis. 2023;14:69. doi:10.1038/s41419-023-05602-9
8. Jin Z, Hao D, Song Y, Zhuang L, Wang Q, Yu X. Systemic inflammatory response index as an independent risk factor for ischemic stroke in patients with rheumatoid arthritis: a retrospective study based on propensity score matching. Clin Rheumatol. 2021;40:3919–3927. doi:10.1007/s10067-021-05762-z
9. Qi Q, Zhuang L, Shen Y, et al. A novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer. 2016;122:2158–2167. doi:10.1002/cncr.30057
10. Suda S, Aoki J, Shimoyama T, et al. Stroke-associated infection independently predicts 3-month poor functional outcome and mortality. J Neurol. 2018;265:370–375. doi:10.1007/s00415-017-8714-6
11. Westendorp WF, Nederkoorn PJ, Vermeij JD, Dijkgraaf MG, van de Beek D. Post-stroke infection: A systematic review and meta-analysis. BMC Neurol. 2011;11:110. doi:10.1186/1471-2377-11-110
12. Miller CM, Behrouz R. Impact of infection on stroke morbidity and outcomes. Curr Neurol Neurosci Rep. 2016;16:83. doi:10.1007/s11910-016-0679-9
13. Cui Z, Kuang S, Yang X, et al. Predictive value of the systemic immune inflammation (SII) index for stroke-associated pneumonia. Brain Behav. 2023; 13:e3302.
14. Yu T, Liu H, Liu Y, Jiang J. Inflammatory response biomarkers nomogram for predicting pneumonia in patients with spontaneous intracerebral hemorrhage. Front Neurol. 2022;13:1084616. doi:10.3389/fneur.2022.1084616
15. Dziedzic EA, Gąsior JS, Tuzimek A, et al. Investigation of the associations of novel inflammatory biomarkers-systemic inflammatory index (SII) and systemic inflammatory response index (SIRI)-with the severity of coronary artery disease and acute coronary syndrome occurrence. Int J Mol Sci. 2022;23:9553. doi:10.3390/ijms23179553
16. Guldolf K, Vandervorst F, Gens R, Ourtani A, Scheinok T, De Raedt S. Neutrophil-to-lymphocyte ratio predicts delirium after stroke. Age Ageing. 2021;50:1626–1632. doi:10.1093/ageing/afab133
17. Sivri S, Sokmen E, Celik M, Ozbek SC, Yildirim A, Boduroglu Y. Usefulness of white blood cell count to mean platelet volume ratio in the prediction of SYNTAX score in patients with non-ST elevation myocardial infarction. Pak J Med Sci. 2019;35:824–829. doi:10.12669/pjms.35.3.1017
18. Adams HP Jr, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of org 10172 in acute stroke treatment. Stroke. 1993;24:35–41. doi:10.1161/01.STR.24.1.35
19. Zhong X, Qiang Y, Wang L, et al. Peripheral immunity and risk of incident brain disorders: A prospective cohort study of 161,968 participants. Transl Psych. 2023;13:382. doi:10.1038/s41398-023-02683-0
20. Zhao J, Yuan F, Song C, et al. Safety and efficacy of three enteral feeding strategies in patients with severe stroke in China (OPENS): A multicentre, prospective, randomised, open-label, blinded-endpoint trial. Lancet Neurol. 2022;21:319–328. doi:10.1016/S1474-4422(22)00010-2
21. Quinn TJ, Langhorne P, Stott DJ. Barthel index for stroke trials: Development, properties, and application. Stroke. 2011;42:1146–1151. doi:10.1161/STROKEAHA.110.598540
22. Iadecola C, Buckwalter MS, Anrather J. Immune responses to stroke: Mechanisms, modulation, and therapeutic potential. J Clin Invest. 2020;130:2777–2788. doi:10.1172/JCI135530
23. Jayaraj RL, Azimullah S, Beiram R, Jalal FY, Rosenberg GA. Neuroinflammation: Friend and foe for ischemic stroke. J Neuroinfla. 2019;16:142. doi:10.1186/s12974-019-1516-2
24. Shi K, Tian DC, Li ZG, Ducruet AF, Lawton MT, Shi FD. Global brain inflammation in stroke. Lancet Neurol. 2019;18:1058–1066. doi:10.1016/S1474-4422(19)30078-X
25. Stuckey SM, Ong LK, Collins-Praino LE, Turner RJ. Neuroinflammation as a key driver of secondary neurodegeneration following stroke? Int J Mol Sci. 2021;22:13101. doi:10.3390/ijms222313101
26. Jones KA, Maltby S, Plank MW, et al. Peripheral immune cells infiltrate into sites of secondary neurodegeneration after ischemic stroke. Brain Behav Immun. 2018;67:299–307. doi:10.1016/j.bbi.2017.09.006
27. Kim YS, Jeong HG, Chang JY, et al. Effect of statin therapy on cardiovascular outcome in stroke patients with low baseline low-density lipoprotein cholesterol. Ann Neurol. 2024;95:876–885. doi:10.1002/ana.26895
28. Dinkel K, Dhabhar FS, Sapolsky RM. Neurotoxic effects of polymorphonuclear granulocytes on hippocampal primary cultures. Proc Natl Acad Sci USA. 2004;101:331–336. doi:10.1073/pnas.0303510101
29. Ansari J, Gavins FNE. Neutrophils and platelets: Immune soldiers fighting together in stroke pathophysiology. Biomed. 2021;9:1945. doi:10.3390/biomedicines9121945
30. Denorme F, Manne BK, Portier I, et al. Platelet necrosis mediates ischemic stroke outcome in mice. Blood. 2020;135:429–440. doi:10.1182/blood.2019002124
31. Elkind MSV, Boehme AK, Smith CJ, Meisel A, Buckwalter MS. Infection as a stroke risk factor and determinant of outcome after stroke. Stroke. 2020;51:3156–3168. doi:10.1161/STROKEAHA.120.030429
32. Westendorp WF, Dames C, Nederkoorn PJ, Meisel A. Immunodepression, infections, and functional outcome in ischemic stroke. Stroke. 2022;53:1438–1448. doi:10.1161/STROKEAHA.122.038867
33. Liu DD, Chu SF, Chen C, Yang PF, Chen NH, He X. Research progress in stroke-induced immunodepression syndrome (SIDS) and stroke-associated pneumonia (SAP). Neurochem Int. 2018;114:42–54. doi:10.1016/j.neuint.2018.01.002
34. Meisel C, Schwab JM, Prass K, Meisel A, Dirnagl U. Central nervous system injury-induced immune deficiency syndrome. Nat Rev Neurosci. 2005;6:775–786. doi:10.1038/nrn1765
35. Vogelgesang A, Grunwald U, Langner S, et al. Analysis of lymphocyte subsets in patients with stroke and their influence on infection after stroke. Stroke. 2008;39:237–241. doi:10.1161/STROKEAHA.107.493635
36. Wang J, Zhong Y, Zhu H, et al. Different gender-derived gut microbiota influence stroke outcomes by mitigating inflammation. J Neuroinfla. 2022;19:245. doi:10.1186/s12974-022-02606-8
37. Faraco G, Iadecola C. Hypertension: A harbinger of stroke and dementia. Hypertension. 2013;62:810–817. doi:10.1161/HYPERTENSIONAHA.113.01063
38. Song TJ, Kim J. Risk of post-stroke pneumonia with proton pump inhibitors, H2 receptor antagonists and mucoprotective agents: A retrospective nationwide cohort study. PLoS One. 2019;14:e0216750. doi:10.1371/journal.pone.0216750
39. Llovera G, Hofmann K, Roth S, et al. Results of a preclinical randomized controlled multicenter trial (pRCT): Anti-CD49d treatment for acute brain ischemia. Sci Transl Med. 2015;7:299ra121. doi:10.1126/scitranslmed.aaa9853
40. Brait VH, Tarrasón G, Gavaldà A, Godessart N, Planas AM. Selective sphingosine 1-phosphate receptor 1 agonist is protective against ischemia/reperfusion in mice. Stroke. 2016;47:3053–3056. doi:10.1161/STROKEAHA.116.015371
41. Xu J, Wang A, Meng X, et al. edaravone dexborneol versus edaravone alone for the treatment of acute ischemic stroke: A Phase III, randomized, double-blind, comparative trial. Stroke. 2021;52:772–780. doi:10.1161/STROKEAHA.120.031197
42. Ma X, Yang J, Wang X, Wang X, Chai S. The clinical value of systemic inflammatory response index and inflammatory prognosis index in predicting 3-month outcome in acute ischemic stroke patients with intravenous thrombolysis. Int J Gen Med. 2022;15:7907–7918. doi:10.2147/IJGM.S384706
43. Zhou Y, Zhang Y, Cui M, Zhang Y, Shang X. Prognostic value of the systemic inflammation response index in patients with acute ischemic stroke. Brain Behav. 2022;12:e2619.
44. Wang RH, Wen WX, Jiang ZP, et al. The clinical value of neutrophil-to-lymphocyte ratio (NLR), systemic immune-inflammation index (SII), platelet-to-lymphocyte ratio (PLR) and systemic inflammation response index (SIRI) for predicting the occurrence and severity of pneumonia in patients with intracerebral hemorrhage. Front Immunol. 2023;14:1115031. doi:10.3389/fimmu.2023.1115031
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.