")
Back to Journals » Journal of Inflammation Research » Volume 17
A Targeted Proteomics Approach Reveals a Serum Protein Signature as a Diagnostic Biomarker for Colorectal Cancer
Authors Wan Y, Luo W, Song X, Zhao Y, Han Z, Shen J, Xie F, Li Y, He J
Received 20 August 2024
Accepted for publication 12 November 2024
Published 10 December 2024 Volume 2024:17 Pages 10755—10768
DOI https://doi.org/10.2147/JIR.S492356
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ning Quan
Yu Wan,1,* Wenfeng Luo,2,* Xiaoyu Song,2,* Ying Zhao,2 Zeping Han,2 Jian Shen,2 Fangmei Xie,2 Yuguang Li,3 Jinhua He2,4
1Gastroenterology Department, The Affiliated Panyu Central Hospital, Guangzhou Medical University, Guangzhou, Guangdong, 511400, People’s Republic of China; 2Central Laboratory, The Affiliated Panyu Central Hospital, Guangzhou Medical University, Guangzhou, Guangdong, 511400, People’s Republic of China; 3Panyu Maternal and Children Healthcare Hospital (Hexian Memorial Medical Hospital of Panyu District), Guangzhou, Guangdong, 511400, People’s Republic of China; 4Rehabilitation Medicine Institute, The Affiliated Panyu Central Hospital, Guangzhou Medical University, Guangzhou, Guangdong, 511400, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinhua He, Central Laboratory, The Affiliated Panyu Central Hospital, Guangzhou Medical University, FuYu Dong Road Number 8, Guangzhou, 511400, People’s Republic of China, Email [email protected] Yuguang Li, Panyu Maternal and Children Healthcare Hospital (Hexian Memorial Medical Hospital of Panyu District), Guangzhou, Guangdong, 511400, People’s Republic of China, Email [email protected]
Background: Circulating proteins secreted by tumors are an important source of cancer biomarkers. This study aims to investigate the changes in the content of tumor immune-related circulating proteins in peripheral blood from patients with colorectal cancer (CRC).
Methods: Olink’s proximity extension assay was used to detect the levels of 92 tumor immune-related circulating proteins in peripheral blood from CRC patients. An enzyme-linked immunosorbent assay was performed to detect the levels of six proteins. Elastic network regression was used to establish the model, and the performance of the model was verified by multiple iterations of cross-validation.
Results: The best serum protein signature that was composed of six proteins (IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3) was selected. The area under the curve value of this signature was 0.9924 in the training set and 0.8992 in the total set. IL7 and IL15 levels were significantly higher in the ≥ 4 cm tumor volume group than in the < 4 cm tumor volume group (P = 0.0113 and P = 0.004, respectively). MCP-3 levels were significantly higher in the distant metastasis group than in the non-distant metastasis group (P =0.0465). There was a significant difference in MCP-3 levels among different tumor, node, metastasis stages (P = 0.0496). CXCL1 levels were positively correlated with the absolute count of basophils (R = 0.3220, P = 0.0273), and IL10 levels were positively correlated with the absolute count of neutrophils (R = 0.38737, P = 0.0078). CXCL1, IL7, and IL15 were independent prognostic factors of CRC (hazard ratio [HR] = 0.62, P = 0.006; HR = 0.57, P = 0.006; and HR = 0.64, P = 0.011, respectively).
Conclusion: The best serum protein signature model (IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3) was able to distinguish CRC patients from healthy controls. These proteins were also involved in the occurrence and development of CRC.
Keywords: immunology-oncology, colorectal cancer, circulating protein
Introduction
The incidence and mortality of colorectal cancer (CRC) in China are increasing. According to the China Cancer Statistics Report, the incidence and mortality of CRC in China ranked second and fifth among all malignant tumors, respectively, with 555,000 new cases and 286,000 deaths in 2020.1 The incidence of colorectal cancer is much higher in urban areas than in rural areas, and its incidence has increased significantly. Most patients are in the middle and advanced stages when diagnosed. Survival in CRC can be improved by its early detection or use of targeted anticancer therapy.2,3 There is an urgent need to explore non-invasive biomarkers for the early diagnosis and identification of new therapeutic targets for CRC.
Circulating proteins, blood components, and proteins secreted by tumors are an important source of cancer biomarkers.4 Changes in plasma protein levels can be used to track disease progression.5 Circulating proteins enable cancer cells to acquire a variety of abilities to promote angiogenesis and metastasis, such as manipulating immune responses, stimulating growth, or inducing angiogenesis and invasion.6 Proteins from tumors or circulating proteins produced by the immune system in response to cancer play an important role in the development and progression of cancer.7 Circulating proteins can serve as major biological vectors for tumor metastasis.8 Cancer-secreted proteins, eg, enzymes, cytokines, and growth factors, are involved in various biological and physiological processes, such as immune responses and cell-cell communication.
Cancer-secreted proteins are also potential biomarkers.9 For example, tumor-associated macrophages and neutrophils promote angiogenesis by secreting various chemokines and pro-angiogenic factors, including CXCR2, CXCR4, CXCR12, CXCL3, CXCR8, CXCR9, CXCR10, CCL2-5, VEGF, TNFa, and IL8.10 The serum levels of GREM1 and CHRDL2 are increased in CRC patients and are associated with an increased risk of CRC. GREM1 and CHRDL2 are expressed mainly by stem cells, epithelial cells, and monocytes in colon tumor tissues. GREM1, CHRDL2, MMP2, and TIMP2 are involved in osteoclast differentiation and CRC development. POLR2F, CSF2RA, CD86, and MMP2 have been used to develop drugs for autoimmune diseases and other cancers and have the potential to be re-explored as therapeutic targets for CRC.11
The proximity extension assay (PEA)-based immuno-oncology panel covers 92 proteins that promote or inhibit tumor immunity, chemotaxis, and vascular and tissue remodeling, and also participate in cell apoptosis, cell damage, cell metabolism, and cell autophagy.12 In this study, we used the PEA to detect differences in immuno-oncology-related plasma proteins circulating in the peripheral blood of CRC patients, and to provide clues for exploring potential plasma protein biomarkers for the early diagnosis of CRC. It might also provide a theoretical basis for revealing the characteristics of the peripheral blood immune environment during the occurrence and development of CRC.
Materials and Methods
Patient Inclusion and Exclusion Criteria
The inclusion criteria for patients with CRC were as follows: preoperative pathological biopsy, postoperative frozen pathology, and immunohistochemistry were all diagnosed as primary colorectal malignant tumor after initially being diagnosed as malignant tumor; no previous history of other malignant tumors; no other systemic diseases except hypertension and diabetes mellitus; and no relevant anti-tumor therapy, such as chemotherapy, radiotherapy, or targeted therapy, was received before surgery.13 The exclusion criteria were as follows: the presence of primarymalignant tumors at other sites or of other types, the existenceof comorbid organ dysfunctions, a history of receiving anti-malignant tumor therapy prior to surgery, and either thepresence of mental illness or an unwillingness to cooperate.
Clinical Samples
Peripheral blood samples were collected from CRC patients at the Affiliated Panyu Central Hospital of Guangzhou Medical University from January 2020 to December 2022 following a pathological diagnosis of CRC. Peripheral blood samples were collected from healthy controls. The acquisition of specimens was approved by the Ethics Committee of The Affiliated Panyu Central Hospital of Guangzhou Medical University (ethics approval number: PYRC-2023-048), and informed consent was obtained before the start of the study. The clinical information of the patients and healthy controls is shown in Supplementary Table 1–2.
PEA
The levels of 92 proteins were measured using an Olink PEA immuno-oncology panel (Supplementary Table 3). The technique is based on the conjugation of a pair of oligonucleotide tags to an antibody against the antigen to be tested. When an antibody binds to a protein, the pair of oligonucleotide markers are located close to each other and form a double chain structure that can be extended by DNA polymerase and hybrid extension after DNA barcoding with microfluidic real-time PCR (Biomark HD, Fluidigm) detection and quantitation. Internal and external quality controls were used for data normalization and quality control. The final results are expressed as the normalized protein expression (NPX) value, which is a Log2 scale unit created by Olink to represent protein expression levels. The PEA technology used in Olink Target 96 incorporates four internal quality control parameters for quality control and data normalization, including two incubation controls for antibody binding. An extension control was used to monitor the elongation reaction, and a detection control, consisting of a piece of synthetic double-stranded DNA, was used to monitor and evaluate potential problems in the final amplification and detection steps. The median difference between the expression of incubation control 2 and detection control in each sample and that of the internal quality control in all samples should not exceed an NPX of 0.3. An external quality control including a sample control was used to evaluate the internal and external accuracy of each protein. Negative controls were used to detect the background noise level of each protein and calculate the limit of detection corresponding to each protein. An inter-plate control or plate control was used to standardize the original Ct value of the lower machine. The final NPX value was obtained by removing the differences in the data, which can also reduce the batch effect between plates. NPX was calculated based on qPCR Ct values, and data were normalized to minimize intra- and inter-assay variability. NPX data allow users to identify changes in the levels of individual proteins in their sample sets, which can then be used to build protein signatures. The specific normalization of NPX, that is, the calculation steps, can be summarized as follows: extension control: CtAnalyte - CtExtension control = dCtAnalyte; inter-plate control: dCtAnalyte-dCtInter - plate control = ddCtAnalyte; adjustment against a correction factor: correction factor- ddCtAnalyte = NPXAnalyte.
Acquisition of Expression Data
The Cancer Genome Atlas (TCGA) database (https://portal.gdc.cancer.gov) was used to download and organize TCGA-COAD and TCGA-READ RNA-seq project data. The data consisted of 698 samples, of which 51 were paracancerous, and 695 samples contained clinical information. According to the data format characteristics, appropriate statistical methods were selected for analysis (stats package and car package). GGplot2 was used to visualize the data.
Enzyme-Linked Immunosorbent Assay (ELISA)
IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3 levels were assessed using an ELISA kit (Elabscience Company).
Statistical Analysis
The receiver operating characteristic (ROC) index was used to evaluate the performance of the model. The Cox proportional hazard model was used to screen characteristics, and elastic network regression was utilized to establish the model. The performance of the model was verified by multiple iterations of cross-validation. Pearson correlation analysis was used to analyze the correlation between the content of tumor immune-related circulating proteins and the absolute count of immune cells. The Mann–Whitney U-test (Wilcoxon rank sum test) was used for matching sample systems; matching carcinoma and carcinoma samples was generally performed using a paired sample t-test.
Results
Quality Control of Sample Data
We collected peripheral blood samples from 51 patients with CRC and 47 healthy controls. The interquartile range and median distribution of the sample data are presented in the form of a dot plot, and colored by whether the quality control was passed or not. The results showed that only three samples were not suitable, while the rest of the samples passed quality control (Supplementary Figure 1). There was a positive correlation between all tested samples (Supplementary Figure 2).
Screening of Differential Tumor Immune-Related Circulating Proteins in Peripheral Blood from CRC Patients
A total of 49 differentially expressed proteins were screened in this study, consisting of 7 upregulated proteins and 42 downregulated proteins (Figure 1). Gene Ontology (GO) analysis showed that the upregulated genes were enriched in cytoplasmic calcium ion transport and calcium ion membrane transport signaling pathways, while the downregulated genes were enriched mainly in the positive regulation of cell adhesion and lymphocyte proliferation signaling pathways. Kyoto Encyclopedia of Genes and Genomes (KEGG) enrichment analysis showed that the upregulated genes were enriched mainly in the cytokine–cytokine receptor, Toll-like receptor signaling pathway interaction, and other signaling pathways, and the downregulated genes were enriched mainly in the PI3K-AKT, JAK-STAT, and other signaling pathways (Figure 2).
 |
Figure 1 Differences in colorectal cancer (CRC) patients with peripheral blood tumor immune-related circulating protein screening. (A) Boxplot of the NPX values of the screened proteins. (B) Heat map of differentially expressed proteins. (C) Volcano map of differentially expressed proteins. Red indicates proteins with higher expression in healthy controls than in CRC patients, and blue indicates proteins with lower expression in healthy controls than in CRC patients. |
 |
Figure 2 Differences in protein/encoding gene enrichment analysis. (A) Analyze the differences in protein concentrations and display the differences in protein/encoding gene enrichment analysis through a bubble chart: (a) GO enrich for up regulated genes; (b) KEGG enrich for up regulated genes; (c) GO enrich for down regulated genes; (d) KEGG enrich for down regulated genes. (B) Network diagrams in enrichment analysis displaying the connections between the key genes and enriched pathways in the form of a network. The dots in the figure show the enriched pathways or genes, all with their respective identifiers. The size of the dots represents the number of differentially expressed genes enriched under this pathway term, and the larger the dot, the more differentially expressed genes in this pathway: (a) GO enrich for up regulated genes; (b) KEGG enrich for up regulated genes; (c) GO enrich for down regulated genes; (d) KEGG enrich for down regulated genes. |
Predicting the Best Signature Model
To establish a signature model, cross-validation is used for multiple iterations, and a relatively random model is obtained by continuously randomly selecting subsets of the dataset. In the cross-validation method, the model with the highest frequency is considered to have the highest accuracy. At the same time, the elastic network regression method contains some characteristics of lasso regression, so the genes are selected for feature screening in each iteration. After a large number of iterations, the genes with the highest frequency retained by the model represent the most suitable feature selection scheme. According to the above method, a signature composed of six proteins (IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3) was selected as the best signature model. By using the training dataset, testing dataset, and total dataset, we focused on the performance of the evaluation model with ROC curve drawing and area under the curve (AUC) performance assessment. The results showed that the AUC value of this signature model was as high as 0.9924 in the training set and 0.8992 in the total set, with high sensitivity and specificity (Figure 3). The AUCs of IL7, CXCL12, IL10, IL15, and CXCL1 were better than those of CEA and CA-19-9 (Supplementary Table 4). The results showed that the signature model composed of six proteins could clearly distinguish the CRC group from the healthy control group. Therefore, IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3 are potential biomarkers for the differential diagnosis of CRC.
 |
Figure 3 Best signature model predictions. (A) The box plot shows how often the different models were selected in multiple iterations, with the abscissa representing different models and the ordinate representing how often that model appeared in the iterations, ranked from left to right according to frequency. (B) ROC of the training dataset. (C) ROC of the testing dataset. (D) ROC of the total dataset. (E) ROC of all datasets overlaid. |
Relationship Between IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3 Levels and the Absolute Count of Immune Cells and Clinicopathological Features of CRC
We used ELISA to verify the relative levels of IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3 in the CRC and healthy control groups. The results showed that IL7, CXCL12, IL10, and CXCL1 levels were higher in the CRC group than in the control group, while IL15 levels were lower in the CRC group than in the control group (Supplementary Figure 3). The absolute counts of peripheral blood immune cells (lymphocytes, monocytes, neutrophils, eosinophils, and basophils) in CRC patients were detected by electrical impedance analysis. The results showed that the absolute number of lymphocytes was lower in the CRC group than in the control group, while the absolute number of monocytes was significantly higher in CRC patients than in healthy controls (Figure 4). CXCL1 levels were positively correlated with the absolute number of basophils, and IL10 levels were positively correlated with the absolute number of neutrophils (Figure 5).
 |
Figure 4 Comparison of the absolute counts of immune cells in peripheral blood between CRC patients and healthy controls. (A) Comparison of absolute neutrophil counts. (B) Comparison of absolute eosinophil counts. (C) Comparison of absolute basophil counts. (D) Comparison of absolute lymphocyte counts. (E) Comparison of absolute monocyte counts. (F) Comparison of absolute lymphocyte counts/absolute monocyte counts. |
 |
Figure 5 Correlation analysis between CXCL1 and IL10 levels and the absolute counts of immune cells. (A) Correlation analysis between IL10 levels and absolute neutrophil count. (B) Correlation analysis between CXCL1 levels and absolute basophil count. |
The relationship between IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3 levels and the clinicopathological features of CRC was further analyzed. The results showed that IL7 and IL15 levels were significantly higher in the ≥4 cm tumor volume group than in the <4 cm tumor volume group, and MCP-3 levels were significantly higher in the distant metastasis group than in the non-distant metastasis group. MCP-3 levels were significantly different among the tumor, node, metastasis (TNM) stages of CRC (Supplementary Tables 5–10). These results showed that IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3 were involved in the occurrence and development of CRC.
IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3 Expression in CRC Tissues
By using the database of TCGA, we analyzed the expression levels of IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3 (CCL7) and their relationship with prognosis using samples from 698 CRC patients (including 51 paracancerous samples). The results showed that CXCL1 expression was significantly higher in CRC tissue than in paracancerous samples. CXCL12, IL10, and IL15 expression was reduced in CRC tissue compared with tumor-adjacent tissues (Figure 6). Survival prognosis analysis showed that high IL7, CXCL1, and IL15 expression was positively correlated with the prognosis of CRC patients, while CXCL12, IL10, and MCP-3 expression was not significantly correlated with prognosis (Figure 7A-F). TCGA database analysis validated the diagnostic performance of the six protein combination in CRC. The ROC curve showed an AUC value of 0.996, which was extremely close to the AUC value of this combination as a signature model, suggesting the higher predictive accuracy of this model (Figure 7G). The above results show that the CXCL12, IL10, and IL15 are involved in the development of CRC, while the expression of IL7, CXCL1, and IL15 is closely related to the prognosis of patients with CRC.
 |
Figure 6 IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3 expression levels in CRC and paracancerous tissues. (A) CXCL1 expression in CRC and paracancerous tissues. (B) CXCL12 expression in CRC and paracancerous tissues. (C) MCP-3 (CCL7) expression in CRC and paracancerous tissues. (D) IL7 expression in CRC and paracancerous tissues. (E) IL10 expression in CRC and paracancerous tissues. (F) IL15 expression in CRC and paracancerous tissues.***P<0.05. |
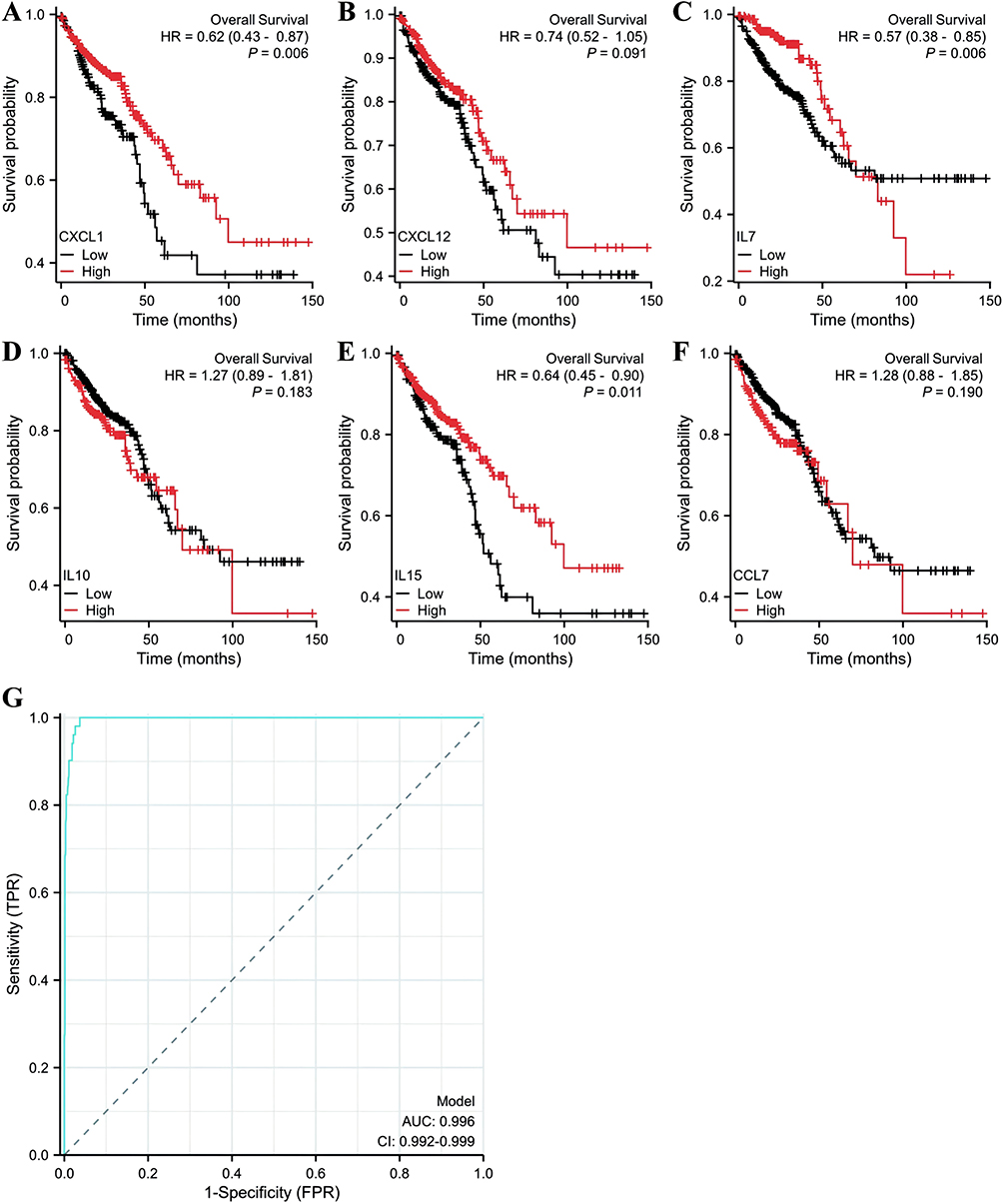 |
Figure 7 Association of IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3 expression with the prognosis of CRC patients. (A) Relationship between CXCL1 expression and the prognosis of CRC patients. (B) Relationship between CXCL12 expression and the prognosis of CRC patients. (C) Relationship between IL7 expression and the prognosis of CRC patients. (D) Relationship between IL10 expression and the prognosis of CRC patients. (E) Relationship between IL15 expression and the prognosis of CRC patients. (F) Relationship between MCP-3 (CCL7) expression and the prognosis of CRC patients. (G) TCGA database analysis validates the diagnostic performance of the six protein panel for CRC. |
Discussion
Recent studies have found that average age of patients with CRC in China is declining. Previously, CRC was diagnosed mainly in individuals aged over 50 years, but now CRC is being diagnosed in an increasing number of young people between 30 and 40 years of age. Early CRC usually has no obvious symptoms, while the appearance of symptoms often indicates that the cancer has progressed to a later stage and may have spread to nearby lymph nodes or organs, causing some physical effects.14 Therefore, the early screening and diagnosis of CRC are particularly important to improve the effect of treatment, reduce mortality, and improve the national health level.
The occurrence and development of CRC are a complex process, involving different molecular changes and regulation. Therefore, the use of omics analysis can more comprehensively reveal the pathogenesis of CRC and improve the accuracy and sensitivity of early diagnosis. Compared with other omics technologies, proteomics analysis of the blood circulation is the most clinically informative.15 The circulatory system contains a large number of proteins and inflammatory factors released from tissues and organs.16 These proteins are significantly different between cancer patients and healthy individuals. Some proteins play a variety of roles in promoting tumor cell proliferation, invasion, metastasis, and regulating the tumor microenvironment, so they can be used as diagnostic biomarkers for CRC.17
In the present study, PEA based on an immuno-oncology panel was used to screen 49 differentially expressed proteins in the peripheral blood of CRC patients, consisting of 7 upregulated proteins and 42 downregulated proteins. Six proteins (IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3) were selected as the best signature. The AUCs of IL7, CXCL12, IL10, IL15, and CXCL1 were better than those of CEA and CA-19-9. These results showed that circulating IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3 proteins have potential value in the early diagnosis of CRC.
Patients with advanced CRC (stage III + IV) had increased concentrations of monocyte/macrophage chemoattraction-related proteins (CCL7, CCL8, CCL15, CCL2, and MIF), M2 polarization-related factors (IL1β and IL4), neutrophil chemoattraction-related proteins and N2 polarization-related cytokines (CXCL2, CXCL5, CXCL6, and IL8), dendritic cell chemoattraction-related proteins (CCL19, CCL20, and CCL21), and natural killer cell-related cytokines (CXCL9 and CXCL10). The concentrations of cell-associated cytokines (CCL1, CCL11, CCL26, CXCL12, IL2, CCL25, and CCL27) were increased, whereas the concentrations of IFN-γ and CX3CL1 were decreased.18 Further comprehensive analysis showed that the absolute number of lymphocytes was lower in CRC patients than in healthy controls, while the absolute number of monocytes was significantly higher in CRC patients than in healthy controls. CXCL1 levels were positively correlated with the absolute number of basophils, and IL10 levels were positively correlated with the absolute number of neutrophils. IL7 and IL15 levels were significantly higher in the >4 cm tumor volume group than in the <4 cm tumor volume group. MCP-3 levels were significantly higher in the distant metastasis group than in the without distant metastasis group, and there were significant differences in MCP-3 levels between the CRC TNM staging groups. CXCL1 degradation mediated by autophagy promotes CRC immune escape, indicating that CXCL1 may be a CRC immunotherapy target.19 IL15 inhibits colitis-associated colon carcinogenesis by modulating antitumor cytotoxicity and modulating the inflammatory tumor microenvironment.20,21 Transfection of the gene encoding the chemokine MCP-3 promotes the induction of anti-CRC immunity.22 There is a significant correlation between high serum IL10 levels and poor CRC survival, and the −1082A/G polymorphism of IL10 has an important impact on CRC progression.23 IL10 is increased in the serum of patients with CRC, and lower levels of IL10 are associated with a lower cancer recurrence rate, a better prognosis, and longer overall survival.24 IL7 levels are lower in CRC patients than in those with active and inactive inflammatory bowel disease.25 The plasma levels of CXCL12 are lower in CRC patients than in controls, and CXCL12 levels are lower in patients with Dukes B and C CRC than in patients with Dukes A CRC.26 In conclusion, circulating plasma proteins have potential application to the diagnosis of CRC and the evaluation of treatment effects and prognosis.
PEA-based proteomics technology has the advantages of ultra-microquantity, precision, stable and reliable results, and high sensitivity and specificity.27 It has been widely used in mining plasma circulating protein markers for the early diagnosis of tumors (eg, epithelial ovarian cancer, cervical cancer, esophageal cancer, glioma, non-small cell lungcancer, gastric cancer, and hepatocellular carcinoma).28–35,36 We utilized PEA proteomics technology to mine six proteins (IL 7, CXCL12, IL10 IL15, CXCL1, and MCP-3) to generate the best signature model representing the differences between CRC patients and healthy controls with high sensitivity and specificity that play a role in the development and progression of CRC. Further verification is needed using a larger sample size. In addition, the expression levels of IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3 in CRC tissues were identified by TCGA-COADREAD dataset analysis. IL7, IL10, and CXCL1 are independent factors for evaluating the prognosis of CRC patients, but they have not been verified using CRC tissue samples. We hypothesize that IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3 expressed in CRC tissues are secreted into the blood circulation and may play an important role in the occurrence and development of CRC.
In conclusion, our study confirmed that the best serum protein signature model (IL7, CXCL12, IL10, IL15, CXCL1, and MCP-3) was able to distinguish CRC patients from healthy controls. These proteins were also involved in the occurrence and development of CRC. Our study provide a theoretical basis for the involvement of peripheral immune environment features in the occurrence and development of CRC.
Abbreviations
CA-19-9, carbohydrate antigen 19-9; CEA, carcinoembryonic antigen; CCL2-5, C-C motif chemokine 2-5; CD86, CD86 antigen; CHRDL2, chordin-like 2; CRC, colorectal cancer; CSF2RA, colony-stimulating factor 2 receptor alpha; CXCL1, C-X-C motif chemokine 1; CXCL3, C-X-C motif chemokine 3; CXCL9, C-X-C motif chemokine 9; CXCL10, C-X-C motif chemokine 10; CXCL11, C-X-C motif chemokine 11; CXCL12, stromal cell-derived factor 1; CXCR2, CXC chemokine receptor 2; CXCR3, CXC chemokine receptor 3; CXCR4, CXC chemokine receptor 4; CXCR8, CXC chemokine receptor 8; CXCR9, CXC chemokine receptor 9; CXCR10, CXC chemokine receptor 10; CXCR12, CXC chemokine receptor 12; ELISA, enzyme-linked immunosorbent assay; FGF2, fibroblast growth factor 2; GO, Gene Ontology; GREM1, gremlin 1; HR, hazard ratio; IFN-γ, interferon-gamma; IL2, interleukin-2; IL7, interleukin-7; IL8, interleukin-8; IL10, interleukin-10; IL15, interleukin-15; KEGG, Kyoto Encyclopedia of Genes and Genomes; MCP-3, C-C motif chemokine 7; MMP2, matrix metalloproteinase 2; NPX, normalized protein expression; PEA, Proximity Extension Assay; PI3K-AKT, phosphatidylinositol 3 kinase-protein kinase B; POLR2F, polymerase (RNA) II (DNA directed) polypeptide F; ROC, receiver operating characteristic; TCGA, The Cancer Genome Atlas; TIE2, angiopoietin-1 receptor; TIMP2, tissue inhibitor of metalloproteinase 2; TNFa, tumor necrosis factor alpha; TNFRSF9, tumor necrosis factor receptor superfamily member 9; TNM, tumor, node, metastasis; TRAIL, TNF-related apoptosis-inducing ligand; VEGF, vascular endothelial growth factor.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials.
Ethics Approval and Consent
Our study complies with the Declaration of Helsinki.
The Ethics Committee of The Affiliated Panyu Central Hospital of Guangzhou Medical University approved this study. Written informed consent was obtained from all patients.
Acknowledgments
We appreciate the support from the YuceBio technology company for detection and data analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Medical Science and Technology Research Fund Projects of Guangdong Province (Grant Nos. A2024164, A2024270, A2023216, A2022524), Basic and Applied Basic Research Foundation of Guangdong Province (Grant No. 2022A1515220217), Science and Technology Program of Guangzhou (Grant Nos. 202201010810, 202102080532), Science and Technology Project of Panyu, Guangzhou (Grant Nos. 2022-Z04-009, 2022- Z04-090, 2022-Z04-072, 2021-Z04-053), and Scientific Research Project of the Affiliated Panyu Central Hospital of Guangzhou Medical University(Grant Nos. PY-2023-001, PY-2023-002, PY-2023-003, PY-2023-004, PY-2023-005, PY- 2023-030, 2022Y002, 2021Y004, 2021Y002).
Disclosure
No potential conflict of interest was reported by the author(s).
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Guo F, Cui J. Anti-angiogenesis: opening a new window for immunotherapy. Life Sci. 2020;258:118163. doi:10.1016/j.lfs.2020.118163
3. Rahma OE, Hodi FS. The intersection between tumor angiogenesis and immune suppression. Clin Cancer Res. 2019;25(18):5449–5457. doi:10.1158/1078-0432
4. Núñez C. Blood-based protein biomarkers in breast cancer. Clin Chim Acta. 2018;490:113–127. doi:10.1016/j.cca.2018.12.028
5. Hamza GM, Raghunathan R, Ashenden S, et al. Proteomics of prostate cancer serum and plasma using low and high throughput approaches. Clin Proteom. 2024;21(1):21. doi:10.1186/s12014-024-09461-0
6. Munkley J, Elliott DJ. Hallmarks of glycosylation in cancer. Oncotarget. 2016;7(23):35478–35489. doi:10.18632/oncotarget.8155
7. Gonzalez H, Hagerling C, Werb Z. Roles of the immune system in cancer: from tumor initiation to metastatic progression. Gene Dev. 2018;32(19–20):1267–1284. doi:10.1101/gad.314617.118
8. Schaaij-Visser TB, de Wit M, Lam SW, et al. The cancer secretome, current status and opportunities in the lung, breast and colorectal cancer context. Biochim Biophys Acta. 2013;1834(11):2242–2258. doi:10.1016/j.bbapap.2013.01.029
9. Karagiannis GS, Pavlou MP, Diamandis EP. Cancer secretomics reveal pathophysiological pathways in cancer molecular oncology. Mol Oncol. 2010;4(6):496–510. doi:10.1016/j.molonc.2010.09.001
10. Owen JL, Mohamadzadeh M. Macrophages and chemokines as mediators of angiogenesis. Front Physiol. 2013;4:159. doi:10.3389/fphys.2013.00159
11. Sun J, Zhao J, Jiang F, et al. Identification of novel protein biomarkers and drug targets for colorectal cancer by integrating human plasma proteome with genome. Genome Med. 2023;15(1):75. doi:10.1186/s13073-023-01229-9
12. Assarsson E, Lundberg M, Holmquist G, et al. Homogenous 96-plex PEA immunoassay exhibiting high sensitivity, specificity, and excellent scalability. PLoS One. 2014;9(4):e95192. doi:10.1371/journal.pone.0095192
13. Department of Medical Administration, National Health Commission of the People’s Republic of China, Oncology Society of Chinese Medical Association. National Health Commission Chinese guidelines for diagnosis and treatment of colorectal cancer (2023 editions). Chin J Gastrointest Surg. 2023;26:505–528.
14. Tanaka LF, Figueroa SH, Popova V, et al. The rising incidence of early-onset colorectal cancer. Dtsch Arztebl Int. 2023;120(Forthcoming):59–64. doi:10.3238/arztebl.m2022.0368
15. Geyer PE, Holdt LM, Teupser D, et al. Revisiting biomarker discovery by plasma proteomics. Mol Syst Biol. 2017;13(9):942. doi:10.15252/msb.20156297
16. Surinova S, Radová L, Choi M, et al. Non-invasive prognostic protein biomarker signatures associated with colorectal cancer. Embo Mol Med. 2015;7(9):1153–1165. doi:10.15252/emmm.201404874
17. Surinova S, Choi M, Tao S, et al. Prediction of colorectal cancer diagnosis based on circulating plasma proteins. Embo Mol Med. 2015;7(9):1166–7118. doi:10.15252/emmm.201404873
18. Li W, Chen F, Gao H, et al. Cytokine concentration in peripheral blood of patients with colorectal cancer. Front Immunol. 2023;14:1175513. doi:10.3389/fimmu.2023.117551318
19. Kong J, Xu S, Zhang P, et al. CXCL1 promotes immune escape in colorectalcancer by autophagy-mediated MHC-I degradation. Hum Immunol. 2023;84(12):110716. doi:10.1016/j.humimm.2023.09.002
20. Bahri R, Pateras IS, D’Orlando O, et al. IL-15 suppresses colitis-associated colon carcinogenesis by inducing antitumor immunity. Oncoimmunology. 2015;4(9):e1002721. doi:10.1080/2162402X.2014.1002721
21. Zhang S, Zhao J, Bai X, et al. Biological effects of IL-15 on immune cells and its potential for the treatment of cancer. Int Immunopharmacol. 2021;91:107318. doi:10.1016/j.intimp.2020.107318
22. Hu JY, Li GC, Wang WM. Transfection of colorectal cancer cells with chemokine MCP-3 (monocyte chemotactic protein-3) gene retards tumor growth and inhibits tumor metastasis. World J Gastroenterol. 2002;8(6):1067–72. doi:10.3748/wjg.v8.i6.1067
23. Miteva LD, Stanilov NS, Deliysky TS, et al. Significance of-1082A/G polymorphism of IL10 gene for progression of colorectal cancer and IL-10 expression. Tumor Biol. 2014;35(12):12655–12664. doi:10.1007/s13277-014-2589-2
24. Li B, Wang F, Ma C, et al. Predictive value of IL-18 and IL-10 in the prognosis of patients with colorectal cancer. Oncol Lett. 2019;18(1):713–719. doi:10.3892/ol.2019.10338
25. Krzystek-Korpacka M, Zawadzki M, Neubauer K, et al. Elevated systemic interleukin-7 in patients with colorectal cancer and individuals at high risk of cancer: association with lymph node involvement and tumor location in the right colon. Cancer Immunol Immunother. 2017;66(2):171–179. doi:10.1007/s00262-016-1933-3
26. Bocchi M, de Sousa Pereira N, De Oliveira KB, et al. Involvement of CXCL12/CXCR4 axis in colorectal cancer: a mini-review. Mol Biol Rep. 2023;50(7):6233–6239. doi:10.1007/s11033-023-08479-1
27. Ding Z, Wang N, Ji N, et al. Proteomics technologies for cancer liquid biopsies. Mol Cancer. 2022;21(1):53. doi:10.1186/s12943-022-01526-8
28. Dobilas A, Åkesson A, Leandersson P, et al. A multiplex biomarker assay improves the prediction of survival in epithelial ovarian cancer. Cancer Genom Prote Om. 2023;20(3):273–280. doi:10.21873/cgp.20380
29. Gyllensten U, Hedlund-Lindberg J, Svensson J, et al. Next generation plasma proteomics identifies high-precision biomarker candidates for ovarian cancer. Cancers. 2022;14(7):1757. doi:10.3390/cancers14071757
30. Weaver C, Nam A, Settle C, et al. Serum Proteomic Signatures in Cervical Cancer: Current Status and Future Directions. Cancers (Basel). 2024;16(9):1629. doi:10.3390/cancers16091629
31. Yang X, Suo C, Zhang T, et al. Targeted proteomics-derived biomarker profile develops a multi-protein classifier in liquid biopsies for early detection of esophageal squamous cell carcinoma from a population-based case-control study. Biomark Res. 2021;9(1):12. doi:10.1186/s40364-021-00266-z
32. Ghorbani A, Avery LM, Sohaei D, et al. Discovery of novel glioma serum biomarkers by proximity extension assay. Clin Proteom. 2023;20(1):12. doi:10.1186/s12014-023-09400-5
33. Xu F, Xu H, Wan Z, et al. A linear discriminant analysis model based on the changes of 7 proteins in plasma predicts response to anlotinib therapy in advanced non-small cell lung cancer patients. Front Oncol. 2022;11:756902. doi:10.3389/fonc.2021.756902
34. Davies MPA, Sato T, Ashoor H, et al. Plasma protein biomarkers for early prediction of lung cancer. EBio Med. 2023;93:104686. doi:10.1016/j.ebiom.2023.104686
35. Shen Q, Polom K, Williams C, et al. A targeted proteomics approach reveals a serum protein signature as diagnostic biomarker for resectable gastric cancer. EBio Med. 2019;44:322–333. doi:10.1016/j.ebiom.2019.05.044
36. Xing X, Cai L, Ouyang J, et al. Proteomics-driven noninvasive screening of circulating serum protein panels for the early diagnosis of hepatocellular carcinoma. Nat Commun. 2023;14(1):8392. doi:10.1038/s41467-023-44255-2
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.