")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Adding Tolvaptan in the Inpatient Treatment for Patients with Heart Failure and Hyponatremia: Budget Impact Analysis in Thailand
Authors Permsuwan U , Leemasawat K, Arunmanakul P
Received 19 November 2024
Accepted for publication 4 July 2025
Published 16 July 2025 Volume 2025:17 Pages 485—494
DOI https://doi.org/10.2147/CEOR.S503735
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Xing Lin Feng
Unchalee Permsuwan,1,2 Krit Leemasawat,3 Poukwan Arunmanakul1,2,4
1Department of Pharmaceutical Care, Faculty of Pharmacy, Chiang Mai University, Chiang Mai, Thailand; 2Center for Medical and Health Technology Assessment (CM-HTA), Department of Pharmaceutical Care, Faculty of Pharmacy, Chiang Mai University, Chiang Mai, Thailand; 3Department of Internal Medicine, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand; 4Pharmaceutical Care Training Center, Department of Pharmaceutical Care, Faculty of Pharmacy, Chiang Mai University, Chiang Mai, Thailand
Correspondence: Poukwan Arunmanakul, Department of Pharmaceutical Care, Faculty of Pharmacy, Chiang Mai University, 239 Suthep Road, Tambon Su Thep, Muang Chiang Mai District, Chiang Mai, 50200, Thailand, Email [email protected]
Objective: Tolvaptan is used as an add-on therapy for heart failure (HF) patients with volume overload, particularly those with hyponatremia (HN), but its cost raises concern. This study aimed to estimate the budget impact of adding 30 mg of tolvaptan to standard treatment compared to standard treatment alone in hospitalized HF patients with HN in Thailand.
Methods: A budget impact analysis (BIA) model was developed in accordance with Thai Health Technology Assessment guidelines from the payer’s perspective. Epidemiological data on HF in Thailand were used to estimate the target population. Clinical effectiveness data were derived from the EVEREST trial. Cost components included tolvaptan acquisition and HF-related hospitalization costs. Cost data were sourced from the National Health Security Office. The net budget impact (NBI) was calculated as the difference in total budget between standard care with tolvaptan and standard care alone. Deterministic sensitivity analysis was performed to explore the impact of key variables.
Results: The total budget without tolvaptan was 201 million THB (5,802,973 USD), increasing to 221 million THB (6,365,607 USD) with tolvaptan, resulting in an NBI of 19.5 million THB (562,634 USD) or 1117 THB (32 USD) per member. Despite higher drug costs, tolvaptan use reduced hospitalization costs (4.2 million USD vs 5.8 million USD) due to fewer HF hospitalization days and length of stay reduction. A lower tolvaptan dose, reduced HN risk, or a daily cost reduction of at least 25.5% could result in a negative NBI.
Conclusion: Although tolvaptan reduced hospital length of stay, its use at 30 mg daily still led to a positive NBI. These findings are relevant for Thailand and similar healthcare systems considering tolvaptan adoption.
Keywords: tolvaptan, budget impact analysis, heart failure, hyponatremia
Introduction
Heart failure (HF) is a major global health concern. Patients with chronic heart failure may experience worsening symptoms known as acute decompensated heart failure (ADHF).1 Common symptoms of ADHF are volume overload and fluid congestion.2 Despite diuretic treatment, 28.7% of the patients with ADHF were found to have congestion on day 7, a clinical outcome associated with HF rehospitalization within 60 days.3 The most common diuretics used to relieve fluid congestion are loop diuretics, which excrete water and sodium. However, use is limited in patients with low blood sodium level or hyponatremia (HN), defined as a serum sodium concentration of < 136 mEq/L, or among patients with diuretic resistance.4,5 HN is related to an increased need for device assistance and longer length of hospital stay.5
Tolvaptan is a vasopressin V2 receptor antagonist diuretic that selectively inhibits the vasopressin V2 receptor in collecting tubules. It prevents the binding of aquaporin-2 and increases the excretion of water in the urine. Unlike other diuretics, tolvaptan excretes only free water. Therefore, this medicine is used in clinical practice as an add-on therapy for patients with volume overload, hypervolemia and/or low blood sodium levels.6 During treatment with tolvaptan, the sodium levels of patients should be monitored to avoid excessive increase in sodium levels.
The clinical data of tolvaptan was gathered in The EVEREST (Efficacy of vasopressin antagonism in heart Failure: outcome study with tolvaptan) trial, a large multicenter, randomized, double-blind, placebo-controlled study in patients hospitalized with worsening heart failure.7 The trial enrolled over 4000 participants and assessed both short-term symptomatic improvement and long-term cardiovascular outcomes. In this trial, tolvaptan was administered at a dosage of 30 mg once daily. This dosage was selected based on previous studies demonstrating effective aquaretic action and tolerability at this level, with a favorable safety profile.
In Thailand, HF is one of the main cardiovascular health problems and a contributor to the country’s economic burden.8 Data from Thai-ADHERE indicated that the median length of hospitalization was 7.5 days, and that intravenous diuretics (mainly intravenous furosemide) were given in 96.1% of patients with HF during admission.9 Of those receiving furosemide, some patients did not respond well and remained in a volume overload status, requiring additional diuretics. Tolvaptan may be used as an add-on therapy with furosemide to improve symptoms and decrease the length of hospital stay, particularly in patients with HN. Tolvaptan is an expensive medication that has not been included in the National List of Essential Medicine (NLEM) of Thailand. This means that administration of the medication is not covered by Thailand’s health insurance policies, instead shifting the financial burden for tolvaptan treatment to the patients as an out-of-pocket expense. Before tolvaptan can be considered for addition to the NLEM, economic evidence including budget impact analyses are required to assist in decision making.10 In Thailand, there are three main public health insurance schemes: the Civil Servants Medical Benefits Scheme (CSMBS) for government employees and their dependents which accounted for 10% of Thai population, the Social Security Scheme (SSS) for private employees which accounted for 20% of Thai population, and the Universal Health Coverage Scheme (UHCS) for the remaining population which accounted for 70%.11 The government requires all three public health insurance schemes to provide a list of medicines issued by the NLEM at all public health facilities. Therefore, only medicines on the NLEM are reimbursable pharmaceuticals in Thailand.
Tolvaptan was made available in Thailand in 2009, with an ongoing patent. No other generic or competing vasopressin antagonists are currently available. Hence, this study aimed to estimate the budget impact of adding 30 mg tolvaptan to the standard treatment compared to standard treatment alone in hospitalized HF patients with HN in Thailand from the payer’s perspective.
Methods
Methods Overview
This study estimated the budget impact of additional tolvaptan use in the treatment of inpatients with HF and HN. The analytical framework for budget impact analysis (BIA) was based on Thai epidemiologic data and the effects of tolvaptan from the EVEREST trial.5,7 The total budget was the sum of the tolvaptan acquisition and hospitalization costs. The net BIA is the difference in the total budget between the two scenarios (with and without tolvaptan use). The analysis was conducted from the payer’s perspective. In this study, the payer refers to the organization responsible for covering healthcare expenditures. All costs were reported in 2022 in Thai Baht (THB) and converted to US dollars (USD) at an exchange rate of 34.73 THB per USD on December 30, 2022.12
Model Structure and Inputs
A Microsoft Excel-based BIA model was developed following Thai Health Technology Assessment (HTA) guidelines.10 A flow diagram of budget impact analysis is shown in Figure 1. To estimate the budget, several assumptions were made, including 100% patient adherence to tolvaptan treatment and the possibility of HF rehospitalization occurring annually. The first step of the BIA model is identifying the eligible population for this study. Next, the treatment scenarios were identified. All the related costs in the study were identified and included in the model. The final step was to calculate the net budget impact.
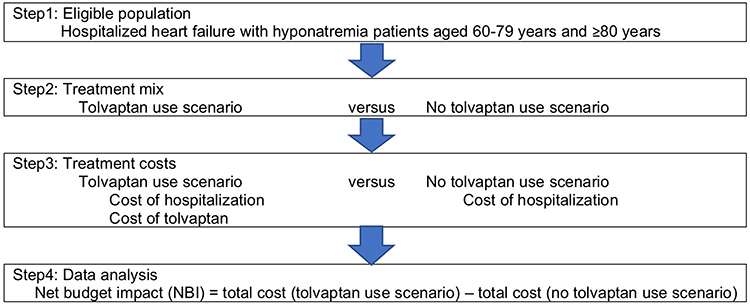 |
Figure 1 Flow diagram of budget impact analysis. |
In this study, the eligible population consisted of patients hospitalized for HF and HN episodes. To accurately estimate the number of eligible patients, we categorized the general population into two subgroups: 1) aged 60–79 years and 2) aged ≥80 years, following the Thai epidemiologic data of HF hospitalization. Janwanishstaporn et al13 reported a national trend in HF hospitalizations under the public health insurance system in Thailand from 2008 to 2013. The average annual rate of HF hospitalization for patients at least 18 years of age is 168 per 100,000 persons. This rate increases with age. Data from this study was used to estimate the rate of HF hospitalization in 2022, which was equal to 520 and 968 per 100,000 persons for populations aged 60–79 and ≥80 years, respectively.
Next, the number of hospitalized HF episodes with HN was estimated, using a cut-off value of serum sodium concentration less than 130 mEq/L. The prevalence of HN in patients admitted for acute HF was obtained from the Thai Acute Decompensated Heart Failure Registry (Thai ADHERE), which reported a prevalence of 9.9%.9
Despite advances in the management of HF, mortality rate remains high in both Western and Asian countries, including Thailand. HF-related mortality during hospital admission ranges from 2 to 6% in Asian populations.14 In this study, we adopted an in-hospital HF mortality rate of 5.5% based on data from Thai ADHERE.9 The age-specific mortality rate of the general Thai population, adjusted for the relative risk of HF, was also applied to the BIA model to estimate the eligible population. In addition, prior HF admission indicated a greater risk of future HF rehospitalization (odds ratio [OR] 3.35, 95% confidence interval, CI 3.29–3.42).13 This indicates a likelihood of rehospitalization for patients with HF in the following year of 41%.13 We assumed that patients with HF surviving after hospital admission would have a 41% chance of rehospitalization in the subsequent year and that rehospitalization would occur only once yearly. Therefore, episodes of rehospitalization in the subsequent year were summarized in a subsequent cohort.
The second step involves identifying the treatment scenario. The budgets of the two scenarios were estimated while making budgetary comparisons in the BIA. 1) Use of tolvaptan for the eligible population and 2) no use of tolvaptan for the eligible population.
The third step was to identify and include all the related costs in the BIA model. Cost inputs included tolvaptan and hospitalization costs. Hospitalization costs were obtained from a cost-effectiveness study of heart failure in Thailand.15 Hospitalization costs including outpatient visits, inpatients stays, laboratory tests, and other related services were obtained from the Central Office for Health Care Information, under the National Health Security Office (NHSO). The NHSO’s electronic database gathers healthcare expenditures for the majority of the Thai population using the Universal Health Care Scheme. Of the 77,163-hospital admission of HF patients, the average hospitalization cost was 1537 THB per day (44.24 USD). The average length of stay (LOS) for HF hospitalization was 7.50 days from Thai ADHERE study.9 These LOS were multiplied by the average daily hospitalization cost to estimate hospitalization costs.
Tolvaptan treatment provided benefits, such as reduced LOS. According to the EVEREST trial,5 all patients with hyponatremia who received tolvaptan had a mean LOS 2.12 days shorter than those received placebo. Therefore, the tolvaptan group would benefit from reduced hospitalization costs. However, this group had to pay for additional tolvaptan treatment, starting on the first day of hospital admission. Acquisition cost of tolvaptan was obtained from the Drug and Medical Supply Information Center (DMSIC), Ministry of Public Health,16 which reported tolvaptan 15 mg of 406.6 THB (11.71 USD) per tablet. The daily dose of tolvaptan used in the base-case analysis was 30 mg, based on the EVEREST trial;5 therefore, the daily acquisition cost of tolvaptan was 813.2 THB (23.41 USD). All inputs of the BIA model are listed in Table 1.
 |
Table 1 Model Inputs |
The last step was to calculate the net budget impact, which is explained in detail in the data analysis.
Data Analyses
The BIA model was performed from the payer’s perspective in Thailand over a five-year period based on the Thai HTA guidelines.10 In the base-case analysis, the net budget impact (NBI) was calculated from the increment in the total budget required when tolvaptan was routinely used for all eligible populations compared with the total budget without tolvaptan use. Model outcomes were reported as the total NBI and as per member yearly (PMPY), in which members were the average number of inpatients with HF and HN for a five-year period. The calculation was performed by dividing the change in the total costs of the two scenarios by the number of members.
A deterministic sensitivity analysis was performed to assess the impact of the parameter uncertainty on the model results. Key parameters such as tolvaptan cost, LOS, and clinical effect of tolvaptan varied within a prespecified range. For example, the average LOS for HF hospitalization increased by one–six days. In addition, the clinical effect of tolvaptan treatment was tested in the range of 0.5 to 2.0 days in LOS reduction. All analyses were performed using Microsoft Excel version of Microsoft Office 365 Pro Plus.
Results
Base-Case Analysis
Of the 13.6 million Thai elderly aged ≥60 years, 5939 aged 60–79 years and 1049 aged ≥80 years were hospitalized with HF and HN in year 1. Patients who survived hospitalization were readmitted in the following year. The average total number of HF with HN hospitalizations was 17,488 (Table 2).
 |
Table 2 Overall Eligible Population |
Table 3 shows the net budget impacts for the tolvaptan and no-tolvaptan treatment scenarios. Of the total budget for the tolvaptan group, 65% was hospitalization costs, while the remainder was tolvaptan treatment costs. The total cost of no tolvaptan use originates from hospitalization. The total cost of the tolvaptan group was higher than that of the no-tolvaptan group when the total budgets of the two scenarios were compared. The average NBI was 19.5 million THB (562,634 USD) yearly or 1117 THB (32 USD) per member. However, the tolvaptan group incurred lower hospitalization costs than the scenario without tolvaptan (4,162,666 USD vs 5,802,973 USD, respectively).
 |
Table 3 Net Budget Impact of Base-Case Analysis |
Sensitivity Analysis
It is important to show how variations in the most influential parameters cause changes in NBI, as indicated in Table 4. The estimated NBI relies heavily on the clinical effects of the tolvaptan treatment. With fewer LOS reductions from tolvaptan treatment, NBI could become more substantial. When the LOS decreased from 2.12 days in base-case analysis to 0.5 days, the average NBI increased 341%. The NBI increased from year 1 onward, with all changes in LOS reduction after tolvaptan treatment (Figure 2A). Similarly, a longer LOS for HF hospitalization resulted in a greater NBI. On average, one additional day of hospitalization led to an additional NBI of 14.2 million THB (409,469 USD). NBI gradually increased from years 1 to 5 (Figure 2B). When the risk of hyponatremia declined from baseline, the NBI decreased. During the 5-year period, the NBI of year 1 was the lowest, including all risks of hyponatremia (Figure 3A).
 |
Table 4 Net Budget Impact of Varying Influential Parameters in the Budget Impact Model |
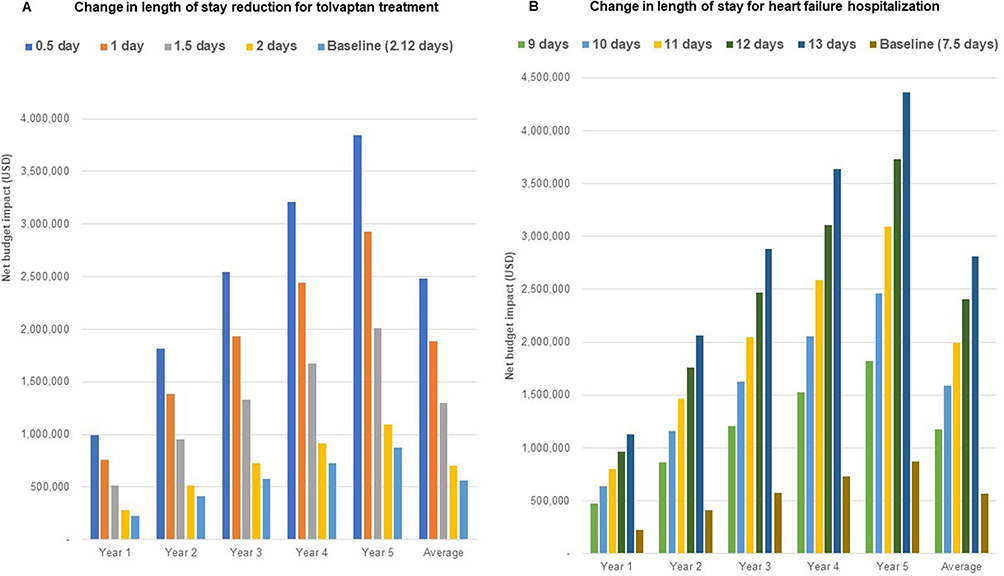 |
Figure 2 Result of deterministic sensitivity analysis ((A) length of stay reduction for tolvaptan treatment, (B) length of stay for heart failure hospitalization). |
 |
Figure 3 Result of deterministic sensitivity analysis ((A) risk of hyponatremia, (B) daily cost of tolvaptan). |
The tolvaptan dose had an impact on NBI. When the daily dose of treatment was 15 mg, NBI was negative, indicating that tolvaptan treatment incurred a lower total cost than no tolvaptan treatment (Table 4). With a tolvaptan dose of 30 mg daily, a 25.5% reduction in the daily cost of tolvaptan resulted in a negative NBI. This implied that the total cost of tolvaptan group would become lower than that of no tolvaptan group when the daily cost of tolvaptan was below 605.5 THB or 17.4 USD (Figure 3B).
Discussion
HF is a major health problem in many countries, including Thailand.13 It is a common hospitalized condition in aging populations, with a high readmission rate and long-term mortality risk.20 According to the Thai ADHERE study,9 9.9% of HF hospitalizations involved HN. In Thailand, the management of HN in HF patients aligns with international guidelines and adaptations within the Thai healthcare context, including recommendations by the Heart Association of Thailand (HAT).21 The first-line approach is typically fluid restriction, especially for patients with mild to moderate, asymptomatic HN. The dose of loop diuretic can be adjusted or switched to medications with less potential for worsening sodium imbalance. Tolvaptan may be considered for severe or resistant cases if initial management is ineffective. In some cases, pre-authorization or clinical justification is required due to cost and coverage limitations.
Normally, tolvaptan use is restricted to patients with HF and HN admitted to the hospital. The starting dose of tolvaptan was 15 mg daily and was titrated up to 30–60 mg daily according to the patients’ fluid accumulation status and serum sodium level. The cost management of ADHF imposes a substantial health budget on both direct and indirect costs.13 Therefore, third-party payers and government agencies increasingly require evidence of NBI to support the adoption of novel treatments and innovative technologies. This study developed a BIA model to estimate the budget for providing tolvaptan as an add-on therapy for patients with HF and HN compared with the scenario without tolvaptan treatment. The current model is specific to the Thai context, but the framework retains its strengths of flexibility and adaptability to other payer systems to assess the financial impact of tolvaptan use in other countries.
Our study findings suggest that adding tolvaptan to standard treatment in ADHF patients with HN incurred an average NBI of 19.5 million THB (562,634 USD) yearly or 1117 THB (32 USD) per member. Although the overall cost increased, tolvaptan treatment led to lower hospitalization costs compared to standard treatment alone. This reduction is attributed to the clinical benefit of tolvaptan in shortening the LOS, which subsequently lowers hospitalization costs.
These findings highlight an important consideration for healthcare decision makers regarding the potential for pricing negotiations to enhance the affordability of tolvaptan. Our sensitivity analysis indicates that a daily cost reduction of at least 25.5% could offset the additional budget burden, potentially resulting in cost savings. This support the use of value-based pricing strategies to enable broader access to tolvaptan within existing budget constraints, ensuring that patients receive clinically appropriate treatment.
Additionally, the findings underscore the value of dose optimization strategies. A lower dose of tolvaptan or a reduced risk of hyponatremia resulted in a negative NBI. In Thailand, tolvaptan is commonly used at a dose of 15 mg per day with a typical dosage range between 7.5 and 15 mg daily. Similarly, a study in Japan, reported an average dose of 9.4 ± 3.8 mg/day.22 These findings suggest that the usual dose of tolvaptan for Asian populations tends to be lower than that used in European settings, which may contribute to a more favorable budget impact profile in Asian healthcare systems.
Similar to our study, a related study from Lee et al23 indicated that tolvaptan was found to have lower cost compared with placebo over the one-month time frame with 34.15 USD in cost saving per member and 0.00347 QALY gain per patient. A more substantial benefit was found among patients with a serum sodium concentration of < 130 mEq/L for tolvaptan treatment with a fixed regimen of 15 mg for the initial four days then increased to 30 mg and 60 mg with 24 h between dose changes.
A BIA study by Amin et al24 using US data indicated that 30.46% of the patients receiving tolvaptan treatment were admitted to intensive care facilities.7 Using tolvaptan for HF and HN inpatients resulted in a budget impact of 52.42 USD per person. The study concluded that tolvaptan had a marginal impact on the hospital budget and should be available as an additional option for sodium correction.
Our study adds valuable new evidence to the literature by demonstrating that a lower fixed dose of tolvaptan may be more cost-effective and accessible, especially in resource-limited settings in Thailand and countries in Southeast Asia.
This study had some limitations; hence, the results must be interpreted with caution. First, we did not include other drug costs for HF treatment; therefore, the budget in each scenario may be lower than that in real-life practice. This was because we assumed that patients in both scenarios would receive the same drugs for HF treatment, except for tolvaptan. Therefore, other drug costs are canceled out for the NBI calculation. Second, the comparators used in this study were not treated with tolvaptan alone. We did not include fluid restriction for HN correction because of limitations in the clinical outcomes, especially in Thai patients. Finally, the issue of generalizability should be cautiously considered. This is because the context of treatment, prevalence of hospitalization for HF, mortality rate during hospitalization for HF, and rate of re-hospitalization vary in different countries. However, the current framework using the BIA model can be adapted to assess the financial impact of tolvaptan use in other countries.
BIA was performed based on Thai epidemiologic data and the effects of tolvaptan from the EVEREST trial. However, in that study (initially published in 2007), tolvaptan initiated for acute treatment of patients hospitalized with heart failure had no effect on long-term mortality or heart failure–related morbidity. Only secondary endpoints such as serum sodium concentration were effective.
Conclusion
Although tolvaptan showed benefits in reducing LOS, the NBI of using tolvaptan 30 mg daily among patients with ADHF and HN remained positive, averaging 19.5 million THB (562,634 USD) per year, or 1117 THB (32 USD) per member. A daily cost reduction of at least 25.5% in the price of tolvaptan would be required to achieve a negative NBI. Targeting specific subgroups of HF patients such as those with fewer day of hospitalization or lower risk of HN may help reduce the overall NBI.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Njoroge JN, Teerlink JR. Pathophysiology and therapeutic approaches to acute decompensated heart failure. Circ Res. 2021;128(10):1468–1486. doi:10.1161/CIRCRESAHA.121.318186
2. Miller WL. Fluid volume overload and congestion in heart failure: time to reconsider pathophysiology and how volume is assessed. Circ Heart Fail. 2016;9(8):e002922. doi:10.1161/CIRCHEARTFAILURE.115.002922
3. Rubio-Gracia J, Demissei BG, Ter Maaten JM, et al. Prevalence, predictors and clinical outcome of residual congestion in acute decompensated heart failure. J Cardiol. 2018;1(258):185–191.
4. Ellison DH, Felker GM. Diuretic treatment in heart failure. N Engl J Med. 2017;377(20):1964–1975. doi:10.1056/NEJMra1703100
5. Cyr PL, Slawsky KA, Olchanski N, et al. Effect of serum sodium concentration and tolvaptan treatment on length of hospitalization in patients with heart failure. AJHP. 2011;68(4):328–333. doi:10.2146/ajhp100217
6. Dubois EA, Rissmann R, Cohen AF. Tolvaptan. Br J Clin Pharmacol. 2012;73(1):9–11. doi:10.1111/j.1365-2125.2011.04029.x
7. Konstam MA, Gheorghiade M, Burnett JC, et al. Effects of oral tolvaptan in patients hospitalized for worsening heart failure, the EVEREST outcome trial. JAMA. 2007;297(12):1319–1331. doi:10.1001/jama.297.12.1319
8. Leelahavarong P, Doungthipsirikul S, Kumluang S, et al. Health technology assessment in Thailand: institutionalization and contribution to healthcare decision making: review of literature. Int J Technol Assess Health Care. 2019;35(6):467–473. doi:10.1017/S0266462319000321
9. Laothavorn P, Hengrussamee K, Kanjanavanit R, et al. Thai acute decompensated heart failure registry (Thai ADHERE). CVD Prev Control. 2010;5(3):89–95.
10. Leelahavarong P. Budget impact analysis. J Med Assoc Thai. 2014;97 Suppl 5:S65–S71.
11. Teerawattananon Y, Tritasavit N, Suchonwanich N, et al. The use of economic evaluation for guiding the pharmaceutical reimbursement list in Thailand. ZEFQ. 2014;108(7):397–404.
12. Bank of Thailand. Foreign exchange rates 2023. 2023. Available from: https://www.bot.or.th/thai/_layouts/application/exchangerate/exchangerate.aspx.
13. Janwanishstaporn S, Karaketklang K, Krittayaphong R. National trend in heart failure hospitalization and outcome under public health insurance system in Thailand 2008-2013. BMC Cardiovasc Disord. 2022;22(1):203. doi:10.1186/s12872-022-02629-2
14. Krittayaphong R, Laothavorn P, Hengrussamee K, et al. Ten-year survival and factors associated with increased mortality in patients admitted for acute decompensated heart failure in Thailand. Singapore Med J. 2020;61(6):320–326. doi:10.11622/smedj.2019108
15. Krittayaphong R, Permsuwan U. Cost-utility analysis of add-on dapagliflozin treatment in heart failure with reduced ejection fraction. Int J Cardiol. 2021;322:183–190. doi:10.1016/j.ijcard.2020.08.017
16. Drug and medical supply information center, ministry of public health 2023. 2023. Available from: http://dmsic.moph.go.th.
17. Office statistics registration systems, The bureau of registration administration, Ministry of Interior. Population statistics 2023. 2023. Available from: https://stat.bora.dopa.go.th/stat/statnew/statMenu/newStat/stat/.
18. Strategy and Planning Division, Ministry of Public Health. Public Health Statistics A.D.2021. Ministry of Public Health; 2023.
19. Corrao G, Ghirardi A, Ibrahim B, et al. Burden of new hospitalization for heart failure: a population-based investigation from Italy. Eur J Heart Fail. 2014;16(7):729–736. doi:10.1002/ejhf.105
20. Krittayaphong R, Karaketklang K, Yindeengam A, et al. Heart failure mortality compared between elderly and non-elderly Thai patients. J Geriatr Cardiol. 2018;15(12):718–724. doi:10.11909/j.issn.1671-5411.2018.12.006
21. Ariyachaipanich ABA, Phrommintikul A, Chirakarnjanakorn S, et al. 2022 HFCT focused update of the 2019 HFCT heart failure guidelines: part 1 - heart failure classification and pharmacological treatment for heart failure with reduced ejection fraction (HFrEF). J Med Assoc Thai. 2022;105:1153–1159.
22. Kinugawa K, Sato N, Inomata T, et al. Real world effectiveness and tolerability of tolvaptan in patients with heart failure- final results of the Samsca post-marketing surveillance in heart failure (SMILE) study. Circ J. 2019;83(7):1520–1527. doi:10.1253/circj.CJ-19-0158
23. Lee MY, Kang HJ, Park SY, et al. Cost-effectiveness of tolvaptan for euvolemic or hypervolemic hyponatremia. Clin Ther. 2014;36(9):1183–1194. doi:10.1016/j.clinthera.2014.07.010
24. Amin AN, Ortendahl JD, Harmon AL, et al. Utilization and budget impact of tolvaptan in the inpatient setting among patients with heart failure and hyponatremia. Curr Med Res Opin. 2018;34(3):559–566. doi:10.1080/03007995.2018.1423958
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.