")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Adjuvant Hepatic Arterial Infusion Chemotherapy Versus Transarterial Chemoembolization for Preventing Early Recurrence After Surgical Resection in Hepatocellular Carcinoma
Authors Xia Y , Wen W, Liao Y, Cai Y, Wan R
Received 27 December 2024
Accepted for publication 8 July 2025
Published 16 July 2025 Volume 2025:12 Pages 1425—1439
DOI https://doi.org/10.2147/JHC.S510814
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ahmed Kaseb
Yangshuo Xia,1,* Wu Wen,1,* Yangyu Liao,2,* Yingxiao Cai,1 Renhua Wan1
1Department of Hepatobiliary Surgery, Nanchang University’s First Affiliated Hospital, Nanchang, Jiangxi, People’s Republic of China; 2Department of Oncology, Nanchang University’s First Affiliated Hospital, Nanchang, Jiangxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Renhua Wan, Department of Hepatobiliary Surgery, Nanchang University’s First Affiliated Hospital, Nanchang, Jiangxi, China, No. 17 Yongwaizheng Street, Donghu District, Nanchang, People’s Republic of China, Email [email protected]
Purpose: HCC exhibits a high postoperative recurrence rate, with early recurrence (≤ 2 years) accounting for 70% of cases, predominantly associated with high-risk recurrence factors. Common adjuvant therapies for HCC include postoperative adjuvant hepatic arterial infusion chemotherapy (PA-HAIC) and postoperative adjuvant transarterial chemoembolization (PA-TACE). This study evaluates the comparative efficacy and safety of PA-HAIC versus PA-TACE in preventing early recurrence among HCC patients with postoperative high-risk recurrence factors.
Patients and Methods: A retrospective analysis included 170 HCC patients with high-risk recurrence factors following surgical resection (2018– 2023), divided into PA-HAIC (n=23) and PA-TACE (n=147) groups. To mitigate potential biases and adjust for baseline characteristics, propensity score matching (PSM) was performed. Survival analyses for two primary endpoints, recurrence-free survival (RFS) and overall survival (OS), were then conducted using the Kaplan-Meier method and Cox proportional hazards regression. Adverse event (AE) rates and severity were compared.
Results: Post-PSM analysis revealed significantly superior RFS rates in the PA-HAIC group versus PA-TACE at 6,12,and 24 months (100%, 95.7%, 95.7% vs 91.3%, 73.9%, 65.2%;p=0.0085). Multivariable Cox regression identified PA-HAIC (HR=0.20, 95% CI:0.02– 0.71;p=0.020) and intact tumor capsule (HR=0.02, 95% CI:0.00– 0.41;p=0.011) as independent protective factors for RFS, while vascular tumor thrombus (HR=28.02, 95% CI:2.07– 378.81;p=0.012) emerged as a risk factor. Subgroup analyses identified age ≥ 50 years, solitary tumors, BCLC-A stage, absence of MVI, intact capsule, and no vascular thrombus as low-risk factors for early recurrence. Safety profiles showed no significant between-group differences in AE incidence or severity.
Conclusion: Among HCC patients with high-risk recurrence factors after surgical resection, PA-HAIC demonstrated significantly prolonged RFS compared to PA-TACE, with a favorable safety profile.
Keywords: hepatocellular carcinoma, adjuvant therapy, hepatic arterial infusion chemotherapy, propensity score-matched, transarterial chemoembolization
Introduction
Hepatocellular carcinoma (HCC) is currently the sixth most common malignancy and the third leading cause of cancer-related death worldwide.1 Curative treatments for HCC include surgical resection, ablation, and liver transplantation, among which hepatic resection remains the preferred treatment option for patients with early-stage disease.2 However, studies have shown that the 5-year postoperative recurrence rate remains as high as 70% following resection.3 Postoperative recurrence can be classified into early recurrence (<2 years) and late recurrence,4 with early recurrence accounting for up to 70% of all cases,5 significantly higher than late recurrence. High-risk factors for early recurrence include vascular invasion, tumor diameter ≥5 cm, multiple tumors, satellite nodules, vascular tumor thrombus, poor tumor differentiation, and the absence of a tumor capsule.6–8 Therefore, early recurrence remains a major obstacle to achieving long-term survival following resection, and reducing early postoperative recurrence has become a critical issue in both clinical research and practice.
Transarterial chemoembolization (TACE) and hepatic arterial infusion chemotherapy (HAIC) have demonstrated favorable efficacy in the treatment of intermediate and advanced-stage HCC and are increasingly being considered as options for adjuvant therapy after hepatic resection. Several studies have shown that postoperative adjuvant TACE (PA-TACE) can improve both OS and RFS in HCC patients. A Phase III randomized clinical trial reported that patients who received PA-TACE after curative resection had significantly longer 3-year RFS than those who did not (56% vs 42.1%). The median RFS was extended by 25.7 months in the PA-TACE group compared to the control group (49.5 vs 23.8 months), and the 3-year OS rate was also higher (85.2% vs 77.4%).9 While PA-TACE confers survival benefits in high-risk HCC patients post-resection, its embolic effects may induce biliary injury or hepatic dysfunction, with ongoing controversy regarding whether clinical benefits originate predominantly from embolization or chemotherapeutic agents.10 Microscopic metastases responsible for early recurrence may lack targetable vasculature for embolization, raising questions about the efficacy of embolization in such cases.
In recent years, HAIC has gained widespread acceptance among clinicians for the treatment of advanced HCC and has also shown promising outcomes in neoadjuvant and adjuvant settings. A large, multicenter, open-label phase III randomized trial demonstrated that in patients with unresectable HCC with tumor diameter >7cm and classified as BCLC stage A or B, HAIC significantly prolonged median OS (23.1 vs 16.1 months, P<0.001) and median PFS (9.6 vs 5.4 months, P<0.001) compared to TACE. Furthermore, the incidence of severe adverse events was lower in the HAIC group, and ORR was more than twice that of the TACE group (46% vs 18%, P<0.001), highlighting the advantages of HAIC in terms of efficacy and safety.11 Other studies have also shown that PA-HAIC after surgical resection improved 5-year RFS (45.2% vs 32.5%) and 5-year OS (35.7% vs 20.9%) compared with surgery alone.12 However, some studies have reported no significant benefit of PA-HAIC in preventing recurrence after surgical HCC resection.13 A network meta-analysis comparing different postoperative adjuvant therapies for HCC found PA-HAIC to be an effective strategy.14
Nonetheless, there remains no consensus on whether PA-HAIC or PA-TACE provides superior survival benefits following curative HCC resection, and direct comparative studies remain limited. This retrospective study utilized propensity score matching (PSM) to compare the efficacy and safety of PA-HAIC versus PA-TACE in preventing early recurrence in patients with high-risk features after surgical resection of HCC, aiming to provide evidence to guide the selection of adjuvant therapy in clinical practice.
Materials and Methods
Patients
From 2018 to 2023, HCC patients who underwent R0 resection at the First Affiliated Hospital of Nanchang University received postoperative adjuvant therapy based on the consensus criteria established by the MDT team. The inclusion criteria were as follows: (1) Presence of high-risk recurrence factors (MVI positivity, tumor diameter ≥5 cm, multiple tumors, satellite nodules, vascular tumor thrombus, poor differentiation, or incomplete capsule).(2) Child-Pugh class A or class B patients corrected to class A before surgery.(3) Eastern Cooperative Oncology Group Performance Status (ECOG PS) score ≤2.Depending on the preferences of the patients and their families, as well as the patients’ physical condition, either PA-HAIC or PA-TACE was selected. Between January 2018 and December 2023, a total of 514 patients with HCC who underwent R0 resection and exhibited high-risk factors for recurrence received postoperative adjuvant TACE or HAIC at the First Affiliated Hospital of Nanchang University and were included in this study. The following criteria served as the basis for inclusion: (1) Eastern Cooperative Oncology Group performance status (ECOG PS) score ≤2; (2) Age between 18 and 75 years; (3) Child-Pugh class A, or class B corrected to class A prior to surgery; (4) Postoperative histopathological confirmation of HCC; (5) No prior history of systemic or locoregional antitumor therapies, including interventional procedures, targeted therapies, or immunotherapies; (6) Radiological evaluation performed 3–5 weeks postoperatively showing no evidence of residual disease or early recurrence; (7) Receipt of only postoperative adjuvant TACE or HAIC therapy; (8) Presence of high-risk factors for recurrence following hepatic resection, including positive MVI, tumor diameter ≥5 cm, multiple tumors, satellite nodules, macrovascular tumor thrombus, poor differentiation, or incomplete tumor capsule; (9) Complete clinical and follow-up data available. The following criteria served as the basis for exclusion: (1) Histologically positive surgical margins; (2) Presence of tumor staining on angiography; (3) Coexistence of other types of malignancies; (4) Inability to tolerate TACE or HAIC treatment; (5) Known hypersensitivity to relevant therapeutic agents.
Criteria for Curative Hepatectomy in HCC
In accordance with the standards for curative surgical resection outlined in the “Guidelines for Diagnosis and Treatment of Primary Liver Cancer (2022)”15(1) Intraoperative Evaluation Criteria: No macroscopic tumor thrombus found in the hepatic veins, bile ducts, portal vein, or inferior vena cava; No invasion of adjacent organs, and no evidence of hilar lymph node metastasis or distant metastasis; The hepatic resection margin must be at least 1 cm from the tumor boundary; if the margin is less than 1 cm, intraoperative histological examination of the liver margin should confirm the absence of tumor cell residuals, thus ensuring a negative margin.(2) Postoperative Evaluation Criteria: Ultrasound, CT, or MRI (at least two modalities) should be performed 1–2 months postoperatively, with no evidence of residual tumor; For patients with preoperative elevated levels of tumor markers, such as serum AFP, DCP, and a combination of seven microRNAs, postoperative tumor marker quantification should be performed 2–3 months after surgery, with results returning to normal levels. The rate of postoperative AFP reduction can be used for early prediction of the completeness of surgical resection.16
Haic
After disinfection of the surgical area and local anesthesia, a vascular access is established in the right femoral artery using the Seldinger technique. Under the guidance of digital subtraction angiography (DSA), a catheter is inserted into the common hepatic artery for hepatic arteriography, allowing for evaluation of the hepatic vascular territory.Based on the specific details of the hepatic resection and the patient’s hepatic artery anatomy, superselective catheterization is performed into the target vessel.17(1) If the patient did not undergo cholecystectomy during the liver cancer resection, the catheter is placed in the hepatic proper artery above the cystic artery. If the patient has undergone cholecystectomy, the catheter is placed in the hepatic proper artery.(2) Based on the pre-established chemotherapy regimen, the prepared antitumor drugs are connected through the catheter for continuous infusion.
The chemotherapy infusion regimen was selected from one of two predefined protocols. The choice of regimen was determined based on a thorough discussion with the patient and their family prior to treatment, taking into consideration both their preferences and the patient’s overall physical condition. FOLFOX modified regimen: Oxaliplatin (85–130 mg/m²) is infused via the artery for 2–3 hours, simultaneously with calcium leucovorin (200 mg/m²) via arterial infusion for 1–2 hours. After an initial dose of 5-fluorouracil (400 mg/m²) by injection, it is followed by continuous infusion of 5-fluorouracil (2400 mg/m²) via the artery for 23 or 46 hours (specific parameters are in accordance with the “2022 Guidelines for the Diagnosis and Treatment of Primary Liver Cancer”). Leucovorin combined regimen: Oxaliplatin (100 mg/m²) combined with Leucovorin (3 mg/m²) is infused sequentially via the artery, with oxaliplatin (100 mg/m²) infused continuously for 4 hours and Leucovorin (3 mg/m²) infused continuously for 1 hour.18
Tace
After completing the preoperative preparation, a vascular access is established in the right femoral artery using the Seldinger technique. Under the guidance of digital subtraction angiography (DSA), a catheter is inserted into the common hepatic artery for hepatic arteriography, allowing for evaluation of the hepatic vascular territory. Under real-time guidance with digital subtraction angiography, the catheter position is adjusted according to whether the gallbladder is resected during the surgery. Subsequently, a mixture of chemotherapeutic agents and embolic agents was administered through the catheter. Commonly used chemotherapy agents include doxorubicin, epirubicin, idarubicin, mitomycin C, fluorouracil, or platinum-based agents.19,20 The embolic agents consisted of a combination of iodized oil and gelatin sponge particles, with the volume of iodized oil ranging from 2 to 5 mL. The drug dosage is dynamically adjusted by the operating physician based on the patient’s body surface area, overall condition, liver function, and response to the TACE procedure.
Postoperative Follow-up
Comprehensive physical examinations, laboratory tests, and dynamic CT or MRI evaluations were performed for all patients at 3 to 5 weeks following surgery and 4 to 6 weeks subsequent to the procedure of initial TACE. Two senior physicians evaluated tumor recurrence based on examination findings, applying the EASL non-invasive diagnostic standards for HCC and the RECIST v1.1 criteria21 to assess extrahepatic recurrence. AEs were classified and evaluated in accordance with version 5.0 of the CTCAE, established by the National Cancer Institute. Radiological monitoring took place a month following the final TACE or HAIC, with subsequent follow-ups scheduled every 3 months, including detailed physical exams, laboratory tests, and imaging, until either the tumor recurs or the observation phase concludes. The study’s monitoring cutoff date was March 1, 2025. RFS served as the primary endpoint, described as the duration between the date of surgery and the first radiological detection of tumor recurrence. The secondary endpoints were OS and safety, with the former defined as the period starting from the surgery date to death due to any reason.
Statistical Analysis
Quantitative variables underwent normality assessment, with data following a normal distribution expressed as mean ± standard deviation and assessed through the Student’s t-test, while data not following a normal distribution were reported as medians with interquartile ranges and evaluated through the Mann–Whitney U-test. Depending on the distribution pattern, categorical data were examined using either the Chi-square test or Fisher’s exact test. RFS was evaluated using Kaplan–Meier survival curves and Log rank tests. Cox proportional hazards regression was employed for multivariate analysis, ensuring that every variable satisfied the proportional hazards assumption. Variables with a p-value less than 0.05 were selected for inclusion in the multivariate framework following the univariate analysis. To reduce the impact of confounding factors, PSM was utilized. The analysis included a multivariate logistic regression model incorporating the following covariates: gender, age, AFP levels, tumor number, presence of liver cirrhosis, hepatitis B status, tumor capsule integrity, anatomical resection, laparoscopic resection, intraoperative blood transfusion, tumor differentiation, MVI, presence of satellite nodules, vascular invasion, maximum tumor diameter, CNLC staging, BCLC staging, and ALBI grade. The propensity score for each patient was calculated, and 1:1 nearest-neighbor matching was performed with a caliper value set at 0.2. After matching, the balance of covariates between the groups was assessed using the standardized mean difference (SMD), with a threshold of SMD < 0.2. Statistical analyses were performed using SPSS version 27.0 and R software version 4.4.1, and a two-tailed p-value below 0.05 was deemed statistically significant.
Results
Patient Characteristics
A total of 514 patients completed adjuvant treatment following liver cancer resection. Based on the inclusion and exclusion criteria, 170 patients ultimately met the study requirements, and the specific screening process is shown in Figure 1. Among them, 198 patients received other types of adjuvant therapy. 119 patients had tumor staining detected in DSA, 10 patients had concomitant major vascular invasion, 5 patients died from other causes, 4 patients had incomplete hospitalization records, and 8 patients were lost to follow-up, resulting in the exclusion of 344 patients. Among the remaining patients, 147 received PA-TACE therapy and 23 received PA-HAIC therapy. Among patients who received PA-TACE, all underwent one cycle of PA-TACE treatment. In the PA-HAIC group, all 23 patients received at least one cycle of PA-HAIC. The majority of patients completed two cycles of PA-HAIC, with only two patients declining the second cycle due to personal reasons. PSM was performed for 170 patients, resulting in 46 matched patients, with 23 in the PA-TACE group and 23 in the PA-HAIC group.
 |
Figure 1 The study flow diagram is presented below. Abbreviations: PA-HAIC, Postoperative adjuvant hepatic artery infusion chemotherapy; DSA, Digital subtraction angiography; PA-TACE, Postoperative adjuvant transcatheter arterial chemoembolization; PSM, Propensity score matching. Notes: Unadjusted Sample corresponds to the SMD prior to PSM, while adjusted Sample represents the SMD following PSM implementation. Treatment 0 corresponds to PA-HAIC, while Treatment 1 is assigned to PA-TACE. |
Table 1 provides a detailed description of the baseline data of patients before propensity score matching. There were no statistically significant differences between the two groups in baseline characteristics, including sex, age, whether anatomical resection was performed, surgical method, transfusion status, presence of satellite nodules, presence of nodular cirrhosis, presence of vascular invasion, number of liver cancer lesions, tumor capsule integrity, degree of differentiation, BCLC stage, hepatitis B history, ALBI grade, and Child-Pugh grade. Among these patients, 19.4% (33/170) underwent open surgery, 13.5% (23/170) were female, and 11.1% (19/170) had multiple liver cancer lesions. The vast majority of patients had intact tumor capsules, and most had a positive hepatitis B surface antigen. Notably, only two patients in the TACE group had a Child-Pugh grade of B, while the rest had a Child-Pugh grade of A. In the PA-TACE group compared to the PA-HAIC group, the proportion of MVI-positive patients (55.1% vs 17.3%, p<0.001), the proportion of tumors with a maximum diameter >5 cm (55.7% vs 21.7%, p=0.002), and the proportion of patients in CNLC stage Ib (54.4% vs 21.7%, p=0.005) were all higher in the PA-TACE group.
 |
Table 1 Baseline Characteristics of HCC Patients: A Comparison Before and After PSM |
After PSM, 23 patients from the PA-HAIC group and 23 patients from the PA-TACE group were matched. Table 1 provides a detailed description of the baseline data of patients after propensity score matching. A clinical analysis of basic characteristics for the matched patients revealed that all variables had a p-value greater than 0.05, indicating comparable characteristics between the PA-HAIC and PA-TACE groups after matching. Figure 2 shows the probability density of PA-HAIC and PA-TACE groups before and after PSM, and through PSM, the probability densities in both groups were balanced. Figure 3 depicts the standardized mean differences (SMD) of PA-HAIC and PA-TACE groups before and after PSM. After matching, the SMD for both groups was reduced to less than 0.2, indicating that the confounding factors were corrected.
 |
Figure 2 The probability density of PA-HAIC and PA-TACE before and after PSM. Abbreviations: PSM, propensity score matching; PA-HAIC, Postoperative adjuvant hepatic artery infusion chemotherapy; PA-TACE, Postoperative adjuvant transcatheter arterial chemoembolization; SMD, standardized mean difference. Notes: Unadjusted corresponds to the SMD prior to PSM, while adjusted represents the SMD following PSM implementation. |
 |
Figure 3 SMDs of Covariates Before and After PSM. Abbreviations: ALBI, Albumin-Bilirubin; CNLC, China Liver Cancer Staging; NOLC, Number of liver cancers; SMD, standardized mean difference; PSM, propensity score matching. |
An evaluation of the effects of PA-HAIC and PA-TACE on RFS and OS in pre- and post-PSM analyses.
Before PSM, there was a significant difference in RFS between the PA-HAIC and PA-TACE groups (p=0.0033). The median RFS for the PA-TACE group was 47.38 months (95% CI: 27.70-NA months), while the median RFS for the PA-HAIC group had not yet reached the endpoint of observation (95% CI not available) (Figure 4). After PSM, the analysis showed that RFS was still significantly different between the PA-HAIC and PA-TACE groups (p=0.018), with the PA-HAIC group showing better RFS than the PA-TACE group. The median RFS for the PA-TACE group was 48.00 months (95% CI: 23.62-NA months), and the median RFS for the PA-HAIC group had not reached the observation endpoint (95% CI not available) (Figure 4).
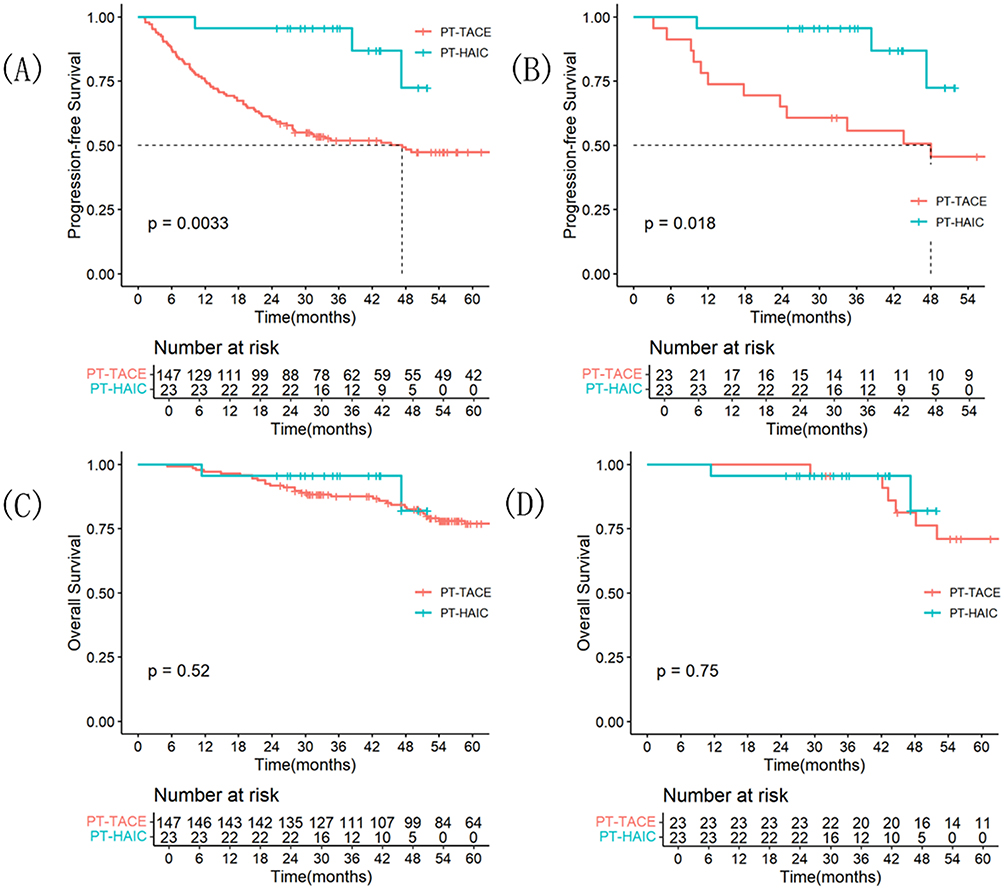 |
Figure 4 Kaplan-Meier survival analysis of RFS in HCC patients: (A) before PSM and (B) after PSM comparing the PA-HAIC and PA-TACE groups; Kaplan-Meier survival analysis of OS in HCC patients: (C) before PSM and (D) after PSM comparing the PA-HAIC and PA-TACE groups. Abbreviations: RFS, recurrence-free survival;OS, overall survival; PSM, propensity score matching; PA-HAIC, Postoperative adjuvant hepatic artery infusion chemotherapy; PA-TACE, Postoperative adjuvant transcatheter arterial chemoembolization. |
Before PSM, there was no significant difference in OS between the PA-HAIC and PA-TACE groups (p=0.52). The 6-month, 12-month, and 24-month survival rates for the PA-TACE group were 99.3% (95% CI: 98.6–100), 97.3% (95% CI: 96.0–98.6), and 91.8% (95% CI: 89.5–94.1), respectively, while the PA-HAIC group had 100%, 95.7% (95% CI: 91.4–100), and 95.7% (95% CI: 91.4–100) survival rates, respectively (Figure 4). After PSM, there was still no significant difference in OS between the two groups (p=0.75). The 12-month and 24-month survival rates for the PA-HAIC group were 95.7% (95% CI: 91.4–100) and 95.7% (95% CI: 91.4–100), respectively, while no deaths were reported in the PA-TACE group during the 2-year follow-up period (Figure 4).
Before PSM, the 6-month, 12-month, and 24-month recurrence-free rates for the PA-TACE group were 87.8% (95% CI: 85.1–90.5), 75.5% (95% CI: 72.0–79.0), and 59.9% (95% CI: 59.5–60.3), respectively, while the PA-HAIC group had 100%, 95.7% (95% CI: 91.4–100), and 95.7% (95% CI: 91.4–100) recurrence-free rates, respectively. After PSM, the 6-month, 12-month, and 24-month recurrence-free rates for the PA-TACE group were 91.3% (95% CI: 85.4–97.2), 73.9% (95% CI: 64.7–83.1), and 65.2% (95% CI: 55.3–75.1), respectively, while the PA-HAIC group had 100%, 95.7% (95% CI: 91.4–100), and 95.7% (95% CI: 91.4–100) recurrence-free rates, respectively.
Univariate and Multivariate Analyses of PA-HAIC and PA-TACE After PSM.
For the PSM-matched data, a Cox proportional hazards regression model was used to analyze RFS. Univariate analysis showed that PA-HAIC (hazard ratio [HR] = 0.24, 95% CI: 0.07–0.86, p=0.028) and tumor capsule integrity (HR = 0.09, 95% CI: 0.01–0.83, p=0.034) were independent protective factors for RFS, while vascular invasion (HR = 4.66, 95% CI: 1.03–21.10, p=0.046) and CNLC stage Ib (HR = 3.18, 95% CI: 1.15–8.86, p=0.026) were independent risk factors for RFS. Variables with a p-value less than 0.05 in univariate analysis were included in multivariate analysis. In the multivariate analysis, PA-HAIC (HR = 0.20, 95% CI: 0.02–0.71, p=0.020) and tumor capsule integrity (HR = 0.02, 95% CI: 0.00–0.41, p=0.011) were independent protective factors for RFS, while vascular invasion (HR = 28.02, 95% CI: 2.07–378.81, p=0.012) was an independent risk factor for RFS (Table 2).
 |
Table 2 Univariate and Multivariate Analysis of Prognostic Factors for RFS After PSM |
For the PSM-adjusted data, a univariate analysis of OS was conducted using the Cox proportional hazards model. The results indicated that none of the variables reached statistical significance (P>0.05, Table 3).
 |
Table 3 Univariate Analysis of Prognostic Factors for Overall Survival After Propensity Score Matching |
Subgroup Analysis of PA-HAIC and PA-TACE Post-PSM.
Subgroup analysis of RFS revealed that age ≥50 years, single tumor, BCLC stage A, no MVI, intact capsule, and no vascular invasion were low-risk factors for early recurrence (Figure 5). However, the subgroup analysis of OS did not identify any variables with statistical significance (P>0.05).
 |
Figure 5 Subgroup analysis of RFS risk stratification for PA-HAIC and PA-TACE therapies. Abbreviations: PA-HAIC, Postoperative adjuvant hepatic artery infusion chemotherapy; NOLC, Number of liver cancers; PA-TACE, Postoperative adjuvant transcatheter arterial chemoembolization. |
Safety
The PA-TACE group exhibited markedly higher rates of elevated ALT (47.8% compared to 26.0%), AST (47.8% compared to 30.4%), and bilirubin levels (34.7% compared to 26.0%) than the PA-HAIC group. The analysis showed no significant variation between the two groups regarding grade III or higher adverse events (P=0.571), all of which were effectively managed with medication interventions. Neither group reported any treatment-related fatalities. Further details are provided in Table 4.
 |
Table 4 Treatment-Related Adverse Events |
Discussion
Based on our findings, compared to PA-TACE, the PA-HAIC regimen provided significantly longer RFS in HCC patients with high-risk recurrence factors after resection, suggesting PA-HAIC may be a more effective adjuvant treatment for this population. Multivariable Cox regression analysis following PSM confirmed PA-HAIC as an independent prognostic factor for RFS improvement. Although the OS difference did not achieve statistical significance, Kaplan-Meier analysis revealed a consistent trend toward superior survival outcomes in the PA-HAIC cohort versus the PA-TACE group.
Even after undergoing curative hepatic resection, up to 70% of patients with HCC experience postoperative recurrence.3 Early recurrence typically occurs within two years postoperatively and is believed by most researchers to be associated with intrahepatic micrometastases derived from the primary tumor22 or iatrogenic dissemination resulting from surgical manipulation. Multiple studies have demonstrated that early recurrence is associated with aggressive tumor characteristics such as MVI, tumor diameter >5 cm, elevated AFP levels, multiple tumor nodules, microsatellite lesions, and incomplete or absent tumor capsule formation23–30 According to the Consensus on Tertiary Prevention of Primary Liver Cancer (2022 Edition), risk factors for postoperative recurrence include tumor diameter >5 cm, multiplicity, absence or incompleteness of the tumor capsule, poor tumor differentiation, presence of MVI, and satellite nodules.31 Therefore, how to effectively prevent early recurrence in patients with high-risk recurrence factors such as MVI positivity, tumor diameter>5cm, multiple tumors, satellite nodules, vascular cancer thrombosis, low differentiation, and incomplete capsule after liver cancer surgery resection is an urgent issue.
Currently, locoregional adjuvant therapies commonly used to prevent early recurrence after HCC resection include PA-TACE and PA-HAIC. Previous studies have demonstrated that PA-TACE is an effective adjuvant treatment for primary HCC, capable of significantly improving RFS and OS.32–35 A multicenter study reported that, compared to patients who did not receive PA-TACE, those with intermediate-stage HCC and MVI who received PA-TACE following curative resection had significantly higher RFS rates at 1, 3, and 5 years postoperatively (P < 0.05). Specifically, the RFS rates in the PA-TACE group were 42.0%, 27.2%, and 17.8% at 1, 3, and 5 years, respectively.32 In the present study, patients in the PA-TACE group achieved 6-month, 1-year, and 2-year recurrence-free rates of 91.3%, 73.9%, and 65.2%, respectively, which appear superior to the aforementioned multicenter study. This difference may be attributable to variations in patient populations; in our study, over 90% of patients receiving PA-TACE were classified as BCLC stage A (early-stage HCC), whereas the multicenter study primarily included patients with intermediate-stage disease. A randomized controlled trial led by Professor Jian Zhou similarly demonstrated that, compared with patients who did not receive PA-TACE after surgery, those who did had a 2-year RFS rate of 64.8%,9 which is consistent with the results of the present study.
HAIC delivers anti-tumor agents directly into the hepatic artery via a catheter, enabling sustained local drug exposure at the tumor site. Multiple multicenter phase III randomized clinical trials36 and meta-analyses37,38 have demonstrated that PA-HAIC significantly improves RFS compared to conventional therapies. Additionally, a randomized, open-label, multicenter phase III clinical trial found that, for patients with postoperative MVI, those treated with PA-HAIC using the FOLFOX regimen achieved significantly longer DFS compared to those who received routine follow-up only (20.3 months vs 10.0 months, P = 0.01). One-, two-, and three-year survival rates in the PA-HAIC group reached 93.8%, 86.4%, and 80.4%, respectively.39 In our present study, patients in the PA-HAIC group achieved recurrence-free survival rates of 100%, 95.7%, and 95.7% at 6, 12, and 24 months, respectively, with corresponding overall survival rates also reaching 100%, 95.7%, and 95.7%, indicating similarly favorable outcomes.
In this study, PSM was used to minimize confounding bias. Covariate balance was assessed by SMD, and after matching, all key covariates (such as CNLC stage, maximum tumor diameter, and surgical approach) had SMD values <0.2, indicating an adequate balance. Following PSM, the PA-HAIC group achieved 6-, 12-, and 24-month RFS rates of 100%, 95.7%, and 95.7%, respectively, all of which were higher than those in the PA-TACE group (91.3%, 73.9%, and 65.2%, respectively). Multivariate analysis confirmed that receiving PA-HAIC was an independent protective factor for RFS after HCC resection. These findings suggest that PA-HAIC is more effective than PA-TACE in preventing early recurrence following curative resection of HCC. Several potential advantages of PA-HAIC over PA-TACE may explain these outcomes: First, PA-HAIC allows for sustained high intrahepatic concentrations of chemotherapeutic agents. In contrast, PA-TACE achieves peak drug levels over a short period, with systemic release occurring within one hour.40 PA-HAIC extends infusion time and stabilizes local drug concentrations, enhancing efficacy. Second, unlike PA-TACE, PA-HAIC does not involve embolization, preserving hepatic arterial patency and ensuring uninterrupted drug delivery.11 Third, PA-TACE may cause ischemic injury, triggering hypoxia-inducible factor-1α (HIF-1α) activation and promoting liver fibrosis and deterioration of liver function.41 Other studies have shown that PA-TACE can increase circulating tumor cells (CTCs), induce hypoxic stress, upregulate N-cadherin, HIF-1α, and vimentin, and downregulate E-cadherin—changes that collectively promote HCC metastasis and raise the risk of tumor recurrence.42 Additionally, our study found that PA-HAIC appeared to outperform PA-TACE in improving OS, although no statistically significant differences were observed in 1- and 2-year OS rates or in overall survival analysis. This finding warrants further investigation and long-term follow-up.
In the multivariate Cox regression analysis following PSM, we identified PA-HAIC and intact tumor capsule as independent protective factors for RFS, whereas vascular tumor thrombus was an independent risk factor. Previous studies have demonstrated that incomplete tumor capsule is associated with poorer prognosis in patients with HCC.43,44 A predictive model for early recurrence following R0 resection in HCC revealed that the risk of postoperative recurrence was 2.06 times higher in patients with capsule infiltration compared to those with an intact capsule.30 Tumors with intact capsules are generally less invasive and more confined to the primary site, thereby exhibiting a lower risk of recurrence. Moreover, the presence of a complete capsule may facilitate R0 resection, reducing microscopic residual disease and consequently lowering the risk of postoperative recurrence. Adjuvant therapy has been shown to improve the prognosis of patients with vascular tumor thrombus. However, vascular invasion includes portal vein tumor thrombus, hepatic vein tumor thrombus, and bile duct thrombus, all of which reflect tumor cell invasion into the vascular system and indicate a higher risk of distant micrometastases or intrahepatic dissemination. Even with surgical resection or PA-HAIC treatment, some microscopic tumor emboli may have already spread into the distal microvasculature, increasing the likelihood of recurrence. In this study, although the presence of vascular tumor thrombus was confirmed by postoperative pathology, the specific type of thrombus was not clearly identified, and its relationship with RFS requires further investigation.
Subgroup analysis of RFS after PSM revealed that age ≥50 years, solitary tumor, BCLC stage A, absence of microvascular invasion (MVI), intact capsule, and absence of vascular tumor thrombus were associated with a lower risk of early recurrence. Patients with solitary tumors, early-stage disease (BCLC A), no MVI, intact capsule, or no vascular invasion demonstrated a relatively low probability of early recurrence following hepatic resection for HCC.
The occurrence rate of adverse serves as an essential metric for assessing therapeutic protocols. Our study showed that the incidence of adverse events was higher in the PA-TACE group compared to the PA-HAIC group. Specifically, elevated ALT, AST, and hyperbilirubinemia occurred in 45.3% vs 24.0%, 48.0% vs 28.0%, and 36.0% vs 24.0% of patients, respectively. This difference may be attributed to embolic agents used in TACE, which compromise hepatic blood flow and result in damage to normal hepatocytes. Furthermore, permanent arterial embolization may lead to severe biliary complications. In contrast, the PA-HAIC group experienced fewer adverse events, all of which were tolerable, and no new or unexpected adverse events were observed.
Despite the use of PSM to reduce confounding bias, this study has several limitations as a retrospective analysis: Firstly, this study was conducted at a single center with a relatively limited sample size, which may lead to selection bias and information bias inherent to retrospective data. The generalizability of our findings to other institutions remains to be validated. Future large-scale, multicenter, prospective randomized controlled trials are warranted to further substantiate our conclusions. Secondly, the relatively short follow-up duration precluded comprehensive assessment of OS in the patient cohort. Due to the relatively short follow-up period, more than half of the patients in the PA-HAIC group had not yet reached the OS endpoint by the last follow-up date, and the same applied to the PA-TACE group. As a result, only differences in the 2-year cumulative survival rates could be observed between the two groups. Long-term survival benefits require further validation through extended follow-up.
Conclusion
In patients with high-risk factors for recurrence following curative resection of HCC, PA-HAIC significantly prolonged RFS compared to PA-TACE. In terms of safety, the associated adverse events were within manageable limits.
Acknowledgments
The study adhered to the Declaration of Helsinki, with approval obtained from the Ethics and Academic Committees of Nanchang University’s First Affiliated Hospital (Academic Approval No.: ISL2024778; Ethics Approval No.: IIT(2024) Clinical Review No. 686).Given that the study was retrospective and relied solely on pre-existing medical data without direct intervention or new participant data collection, informed consent requirements were exempt. The original data can be inquired anonymously via [email protected] or [email protected]. This study received no financial support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tadokoro T, Tani J, Morishita A, Fujita K, Masaki T, Kobara H. the treatment of hepatocellular carcinoma with major vascular invasion. Cancers. 2024;16(14). doi:10.3390/cancers16142534
2. Brown ZJ, Tsilimigras DI, Ruff SM, et al. Management of hepatocellular carcinoma: a review. JAMA Surgery. 158(4):410–420. doi:10.1001/jamasurg.2022.7989
3. Llovet JM, Pinyol R, Yarchoan M, et al. Adjuvant and neoadjuvant immunotherapies in hepatocellular carcinoma. Nat Rev Clin Oncol. 2024;21(4):294–311. doi:10.1038/s41571-024-00868-0
4. Wang MD, Li C, Liang L, et al. Early and late recurrence of hepatitis b virus-associated hepatocellular carcinoma. oncologist. 2020;25(10):e1541–e1551. doi:10.1634/theoncologist.2019-0944
5. Zhao L, Song J, Sun Y, et al. Tumor-derived proliferative CTCs and CTC clusters predict aggressiveness and early recurrence in hepatocellular carcinoma patients. Cancer Med. 2023;12(13):13912–13927. doi:10.1002/cam4.5946
6. Li J, Liu Y, Qiu Y, Qu C, Li J. Comparison of adjuvant treatment regimens for high-risk hepatocellular carcinoma: a Bayesian network meta analysis and systematic review. Front Immunol. 2024;15:1487353. doi:10.3389/fimmu.2024.1487353
7. Nevola R, Ruocco R, Criscuolo L, et al. Predictors of early and late hepatocellular carcinoma recurrence. World J Gastroenterol. 2023;29(8):1243–1260. doi:10.3748/wjg.v29.i8.1243
8. Xu XF, Xing H, Han J, et al. Risk factors, patterns, and outcomes of late recurrence after liver resection for hepatocellular carcinoma: a multicenter study from china. JAMA Surg. 2019;154(3):209–217. doi:10.1001/jamasurg.2018.4334
9. Wang Z, Ren Z, Chen Y, et al. adjuvant transarterial chemoembolization for HBV-related hepatocellular carcinoma after resection: a randomized controlled study. Clin Cancer Res. 2018;24(9):2074–2081. doi:10.1158/1078-0432.Ccr-17-2899
10. Chan SL, Hui EP, Yu S, Yeo W. Re: roles played by chemolipiodolization and embolization in chemoembolization for hepatocellular carcinoma: single-blind, randomized trial. J National Cancer Inst. 2013;105(8):580. doi:10.1093/jnci/djt047
11. Li QJ, He MK, Chen HW, et al. Hepatic arterial infusion of oxaliplatin, fluorouracil, and leucovorin versus transarterial chemoembolization for large hepatocellular carcinoma: a randomized phase iii trial. J Clin Oncol. 40(2):150–160. doi:10.1200/jco.21.00608
12. Feng M, Tang C, Feng W, Bao Y, Zheng Y, Shen J. Hepatic artery-infusion chemotherapy improved survival of hepatocellular carcinoma after radical hepatectomy. Onco Targets Ther. 2017;10:3001–3005. doi:10.2147/ott.S136806
13. Kim DY, Ahn SH, Kim SU, et al. Adjuvant hepatic arterial infusional chemotherapy with 5-fluorouracil and cisplatin after curative resection of hepatocellular carcinoma. Oncology. 2011;81(3–4):184–191. doi:10.1159/000333827
14. Liu Y, Wang Y, Guo X, et al. Comparative effectiveness of adjuvant treatment for resected hepatocellular carcinoma: a systematic review and network meta-analysis. Front Oncol. 2021;11:709278. doi:10.3389/fonc.2021.709278
15. Zhou J, Sun H, Wang Z, et al. Guidelines for the diagnosis and treatment of primary liver cancer (2022 edition). Liver Cancer. 2023;12(5):405–444. doi:10.1159/000530495
16. Li XL, Zhu XD, Cai H, et al. Postoperative α-fetoprotein response predicts tumor recurrence and survival after hepatectomy for hepatocellular carcinoma: a propensity score matching analysis. Surgery. 2019;165(6):1161–1167. doi:10.1016/j.surg.2019.01.009
17. Iwamoto H, Shimose S, Shirono T, Niizeki T, Kawaguchi T. Hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma in the era of chemo-diversity. Clin Mol Hepatol. 2023;29(3):593–604. doi:10.3350/cmh.2022.0391
18. Chen S, Zhang K, Liu W, Yu W. Hepatic arterial infusion of oxaliplatin plus raltitrexed in patients with intermediate and advanced stage hepatocellular carcinoma: a Phase II, single-arm, prospective study. Eur. J. Cancer. 2020;134:90–98. doi:10.1016/j.ejca.2020.03.032
19. Raoul JL, Forner A, Bolondi L, Cheung TT, Kloeckner R, de Baere T. Updated use of TACE for hepatocellular carcinoma treatment: how and when to use it based on clinical evidence. Cancer Treat Rev. 2019;72:28–36. doi:10.1016/j.ctrv.2018.11.002
20. Hamaya S, Oura K, Morishita A, Masaki T. Cisplatin in liver cancer therapy. Int J Mol Sci. 24(13):10858. doi:10.3390/ijms241310858
21. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
22. Wang J, He XD, Yao N, Liang WJ, Zhang YC. A meta-analysis of adjuvant therapy after potentially curative treatment for hepatocellular carcinoma. Canadian J Gastroenterol. 2013;27(6):351–363. doi:10.1155/2013/417894
23. Poon RT, Fan ST, Ng IO, Lo CM, Liu CL, Wong J. Different risk factors and prognosis for early and late intrahepatic recurrence after resection of hepatocellular carcinoma. Cancer. 2000;89(3):500–507. doi:10.1002/1097-0142(20000801)89:3<500::AID-CNCR4>3.0.CO;2-O
24. Poon RT. Differentiating early and late recurrences after resection of HCC in cirrhotic patients: implications on surveillance, prevention, and treatment strategies. Ann Surg Oncol. 2009;16(4):792–794. doi:10.1245/s10434-009-0330-y
25. Jung SM, Kim JM, Choi GS, et al. Characteristics of early recurrence after curative liver resection for solitary hepatocellular carcinoma. J Gastrointestinal Surg. 2019;23(2):304–311. doi:10.1007/s11605-018-3927-2
26. Huang Y, Su Y, Chen Y, et al. Risk factors and nomogram predictive models for postsurgical progression/hyperprogression recurrence in hepatocellular carcinoma with macroscopic vascular invasion. World Journal of Surgical oncology. 2024;22(1):305. doi:10.1186/s12957-024-03572-6
27. Yao LQ, Chen ZL, Feng ZH, et al. Clinical features of recurrence after hepatic resection for early-stage hepatocellular carcinoma and long-term survival outcomes of patients with recurrence: a multi-institutional analysis. Ann Surg Oncol. 2022. doi:10.1245/s10434-022-11454-y
28. Liang BY, Gu J, Xiong M, et al. Tumor size may influence the prognosis of solitary hepatocellular carcinoma patients with cirrhosis and without macrovascular invasion after hepatectomy. Sci Rep. 2021;11(1):16343. doi:10.1038/s41598-021-95835-5
29. Shinkawa H, Tanaka S, Takemura S, et al. Nomograms predicting extra- and early intrahepatic recurrence after hepatic resection of hepatocellular carcinoma. Surgery. 2021;169(4):922–928. doi:10.1016/j.surg.2020.10.012
30. Zhang K, Tao C, Siqin T, Wu J, Rong W. Establishment, validation and evaluation of predictive model for early relapse after R0 resection in hepatocellular carcinoma patients with microvascular invasion. J Transl Med. 19(1):293. doi:10.1186/s12967-021-02940-0
31. The consensus on tertiary prevention of primary liver cancer (2022 version)]. Zhonghua gan zang bing za zhi = Zhonghua ganzangbing zazhi =. Chin J Hepatol. 2022;30(8):832–845. doi:10.3760/cma.j.cn501113-20220616-00330
32. Xiang C, Shen X, Zeng X, et al. Effect of transarterial chemoembolization as postoperative adjuvant therapy for intermediate-stage hepatocellular carcinoma with microvascular invasion: a multicenter cohort study. Int J Surg. 2024;110(1):315–323. doi:10.1097/js9.0000000000000805
33. Sun JJ, Wang K, Zhang CZ, et al. postoperative adjuvant transcatheter arterial chemoembolization after r0 hepatectomy improves outcomes of patients who have hepatocellular carcinoma with microvascular invasion. Ann Surg Oncol. 2016;23(4):1344–1351. doi:10.1245/s10434-015-5008-z
34. Qi YP, Zhong JH, Liang ZY, et al. Adjuvant transarterial chemoembolization for patients with hepatocellular carcinoma involving microvascular invasion. Am J Surg. 2019;217(4):739–744. doi:10.1016/j.amjsurg.2018.07.054
35. Zhu XD, Li KS, Sun HC. Adjuvant therapies after curative treatments for hepatocellular carcinoma: current status and prospects. Genes Dis. 2020;7(3):359–369. doi:10.1016/j.gendis.2020.02.002
36. Li L, Zz L, Pan LX, et al. Adjuvant therapy for hepatocellular carcinoma after curative treatment: several unanswered questions. J clin Translational Hepatol. 2024;12(5):525–533. doi:10.14218/jcth.2024.00030
37. Ke Q, Wang L, Wu W, et al. Meta-analysis of postoperative adjuvant hepatic artery infusion chemotherapy versus surgical resection alone for hepatocellular carcinoma. Front Oncol. 2021;11:720079. doi:10.3389/fonc.2021.720079
38. Hu L, Zheng Y, Lin J, Shi X, Wang A. Does adjuvant hepatic artery infusion chemotherapy improve patient outcomes for hepatocellular carcinoma following liver resection? A meta-analysis. World Journal of Surgical oncology. 2023;21(1):121. doi:10.1186/s12957-023-03000-1
39. Li SH, Mei J, Cheng Y, et al. Postoperative adjuvant hepatic arterial infusion chemotherapy with folfox in hepatocellular carcinoma with microvascular invasion: a multicenter, phase iii, randomized study. J clin Oncol. 2023;41(10):1898–1908. doi:10.1200/jco.22.01142
40. He MK, Zou RH, Wei W, et al. Comparison of stable and unstable ethiodized oil emulsions for transarterial chemoembolization of hepatocellular carcinoma: results of a single-center double-blind prospective randomized controlled trial. J Vasc Int Radiol JVIR. 2018;29(8):1068–1077.e2. doi:10.1016/j.jvir.2018.03.027
41. Qu K, Yan Z, Wu Y, et al. Transarterial chemoembolization aggravated peritumoral fibrosis via hypoxia-inducible factor-1α dependent pathway in hepatocellular carcinoma. J Gastroenterol Hepatol. 2015;30(5):925–932. doi:10.1111/jgh.12873
42. Fang ZT, Wang GZ, Zhang W, et al. Transcatheter arterial embolization promotes liver tumor metastasis by increasing the population of circulating tumor cells. Onco Targets Ther. 2013;6:1563–1572. doi:10.2147/ott.S52973
43. Xing H, Zhang WG, Cescon M, et al. Defining and predicting early recurrence after liver resection of hepatocellular carcinoma: a multi-institutional study. HPB. 2020;22(5):677–689. doi:10.1016/j.hpb.2019.09.006
44. Zhang XP, Wang K, Wei XB, et al. An Eastern hepatobiliary surgery hospital microvascular invasion scoring system in predicting prognosis of patients with hepatocellular carcinoma and microvascular invasion after R0 liver resection: a large-scale, multicenter study. oncologist. 2019;24(12):e1476–e1488. doi:10.1634/theoncologist.2018-0868
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Adjuvant Lenvatinib for High-Risk CNLC IIb/IIIa Hepatocellular Carcinoma After Curative Hepatectomy: A Prospective Exploratory Study
Sun HC, Huang ZY, Wen T, Liu L, Zhu XD, Zhang E, Li C, Zhang X, Wang J, Fan J, Zhou J
Journal of Hepatocellular Carcinoma 2025, 12:1043-1056
Published Date: 22 May 2025