")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Advanced Practice Respiratory Therapy in the State of California: A Cross-Sectional Needs Assessment Study
Authors Alismail A , Xu Y, Craddock K, Lopez D, Terry M, Tan L
Received 26 March 2025
Accepted for publication 16 June 2025
Published 25 June 2025 Volume 2025:18 Pages 3673—3684
DOI https://doi.org/10.2147/JMDH.S530602
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Abdullah Alismail,1– 3,* Yiqing Xu,1,* Krystal Craddock,4 David Lopez,1 Michael Terry,1,5 Laren Tan1,2
1Department of Cardiopulmonary Sciences, School of Allied Health Professions, Loma Linda University Health, Loma Linda, CA, USA; 2Department of Medicine, Loma Linda University Health, Loma Linda, CA, USA; 3Department of Cardiopulmonary Sciences, College of Health Science, Rush University, Chicago, IL, USA; 4Department of Respiratory Care, University of California Davis Medical Center, Sacramento, CA, USA; 5Department of Respiratory Care, Loma Linda University Medicine Center, Loma Linda, CA, USA
*These authors contributed equally to this work
Correspondence: Abdullah Alismail, Department of Cardiopulmonary Sciences, Loma Linda University, Loma Linda, CA, USA, Email [email protected]
Introduction: As the respiratory therapy (RT) profession in the United States discusses the establishment of the Advanced Practice in Respiratory Therapy (APRT) profession, the purpose of this study was to investigate the perception of the respiratory therapy community in the state of California (CA) on the need to start the APRT profession within the state.
Methods: This was a descriptive pilot cross-sectional anonymous study that was approved by the institutional review board at Loma Linda University. Survey was sent via Email to program directors, faculty, students, bedside RTs, and hospital managers/directors by The Respiratory Care Board of CA, and the California Society in Respiratory Care to be sent out to their constituents.
Results: A total of 1030 responded to the survey. Of the respondents, 50.6% were males and 48.1% females, with mean age of 45.7 ± 13.1 years. Most were practicing RTs (74.2%). Majority of the respondents held at least a bachelor’s degree and worked in a mid-size hospital. An overwhelming majority of the respondents supported the establishment of APRT in CA (91.9%). When asked about APRT educational level, 56% recommended a graduate degree. Nearly 56% of the respondents had knowledge of APRT prior to the survey, with 68.1% of them showing interest in applying for an APRT program once established. The main identified barriers to implementation were acceptance among other advanced practice providers, acceptance among physicians, legislation, scope of practice, and reimbursement. A majority believed that APRT should require a separate license, 71.7%. Chi-Square results showed that those with higher education were more supportive of APRT than those with high school, p = 0.015.
Conclusion: The results of this pilot study show the strong support of the respiratory therapy workforce in California for establishing APRT. In addition, respondents believed that APRT should have its own separate license and those holding higher education were more supportive to establish APRT within the state. Further research is needed by surveying physicians, nurse practitioners, and physician assistants on the need for APRT within the state.
Keywords: APRT, respiratory care, advanced practice respiratory therapy, advanced practice provider, California
Introduction
The Association of American Medical Colleges estimates the United States (US) will be short 124,000 physicians by 2034.1–3 While the physician demand continues to grow, we are simultaneously burdened with increasing amounts of climate-related health conditions and aging population.4,5 Additionally, 3 of the top 6 leading causes of death in the US are cardiopulmonary specific, including heart disease, COVID-19, and COPD.6 Physician shortage is an issue that has been reported and published in several papers in the literature.7–12 This physician shortage leads to poor patient access and higher unnecessary emergency room and urgent care utilization.3,13
To address physician shortages, there has been a growth in Advanced Practice Providers (APPs), which currently include Nurse Practitioners (NPs) and Physician Assistants (PAs). In fact, the US Census Bureau projects job growth for APPs between 2021 and 2031, with a 46% increase for NPs and 28% growth for PAs.14 The respiratory care profession established a new profession that would be the third APP model, called Advanced Practice Respiratory Therapist (APRT).15,16 APRT programs are accredited by the Commission of Accreditation for Respiratory Care (CoARC).17 The APRT would be a credentialed, licensed respiratory care practitioner trained and educated to be a mid-level provider.17 As part of a physician-led team, APRTs would provide diagnostic, therapeutic, critical care and preventive care services with a focus in cardiopulmonary care across multiple settings. They would need to complete a graduate degree program major in APRT that includes both in classroom facilitated learning and clinical rotations. Several studies have shown the need for an APP who is specialized in cardiopulmonary diagnostics. Strickland et al (2020) surveyed physicians in the United States regarding the need for a non-physician APP who is specialized in cardiopulmonary disease, of which 14% (n = 202) were from California. Results showed strong support as well as hiring of these providers when available. Therefore, the key difference an APRT professional add is being a “third” APP, alongside NPs and PAs, who is specialized in cardiopulmonary diseases.
Currently, there is only one program that has been producing APRT graduates, the Ohio State University. The program had its first graduates in 2021, seven graduates, as the first in the nation.18 Other states are currently on track to establish APRT programs as well since the profession is fairly new to evaluate the outcome of these graduates and their effect on patient care. A recent paper published in CHEST journal laid out an example APRT curriculum for institutions that are interested in establishing an APRT program.19 Although this profession is new and only one state that currently has graduates, Veterans Affairs in Maryland hired the first APRT graduates from Ohio State University program.20 This support illustrates not just the potential, but the need across VA institutions nationwide. Several papers have been published laying out the expectation of an APRT graduate as well as aid institutions on curriculum design.19,21–23
Therefore, the purpose of this pilot study was to investigate the perceptions of the respiratory therapy community in the state of California to establish an APRT profession in the state.
Methods
This study was a descriptive pilot cross-sectional anonymous survey that was approved by the institutional review board at Loma Linda University Health. Inclusion criteria were practicing respiratory therapist, respiratory therapy faculty, respiratory therapy students, all within the state of California. The survey was designed using Qualtrics platform. The survey was distributed electronically using a convenience sampling approach via Email through California Society in Respiratory Care (CSRC), Respiratory Care Board of California, and Program Directors of accredited programs listed in the CoARC within the state. Each organization sent multiple reminders to take the survey to increase the response rate. The informed consent was embedded in the beginning of the survey where subjects read the consent and chose between “yes” and “no” for participation. If they selected “yes”, they advanced to the survey; while “no” would end the survey. Participation was voluntary.
The authors designed the survey and had it reviewed by a statistician as well as pilot tested it by several healthcare professionals. Content validity was examined by multiple health care providers [respiratory therapist, statistician and methodologist, and a physician]. The survey covered various questions such as demographics, role within the profession, experience, APRT related questions on perception, current understanding, support, barriers and challenges. The APRT definition from the AARC was inserted within the survey to give respondents a background on APRT. In addition, at the end of the survey, the subjects answered two open-ended questions regarding advantages and disadvantages of establishing the APRT profession within the state. The survey was open from April 2023 to May 2024.
Data Analysis
Data was analyzed using SPSS version 29.0. Data was summarized using means and SD values for continuous variables and frequency (%) for categorical variables. Chi-Square test of homogeneity was performed to compare the distribution of APRT support questions with level of education. The level of significance was set at p ≤ 0.05. Comments from the open-ended questions on advantages and barriers were coded and categorized to establish themes.
Results
The survey was sent to all respiratory care practitioners (RCP) in the state of California. A total of 1030 participated in the survey, out of approximately 20,000 RCPs (5.2% response rate). The characteristics of the respondents are displayed in Table 1. Mean age was 45.7 ± 13.0 years with 50.6% males and 48.7% females. Mean years of experience were 18.9 ±13.5 years. Most of the respondents reported to be practicing respiratory therapists (74.2%). In addition, most respondents reported that they hold a minimum of a bachelor’s degree (55.8%), work in medium size hospital of 100–499 beds (63%), and work in a hospital settings (81%). When looking at NBRC credentials, 991 (96%) reported that they hold CRT and RRT credentials. In addition to CRT and RRT. 176 had the Neonatal and Pediatric Specialist (NPS) credential.
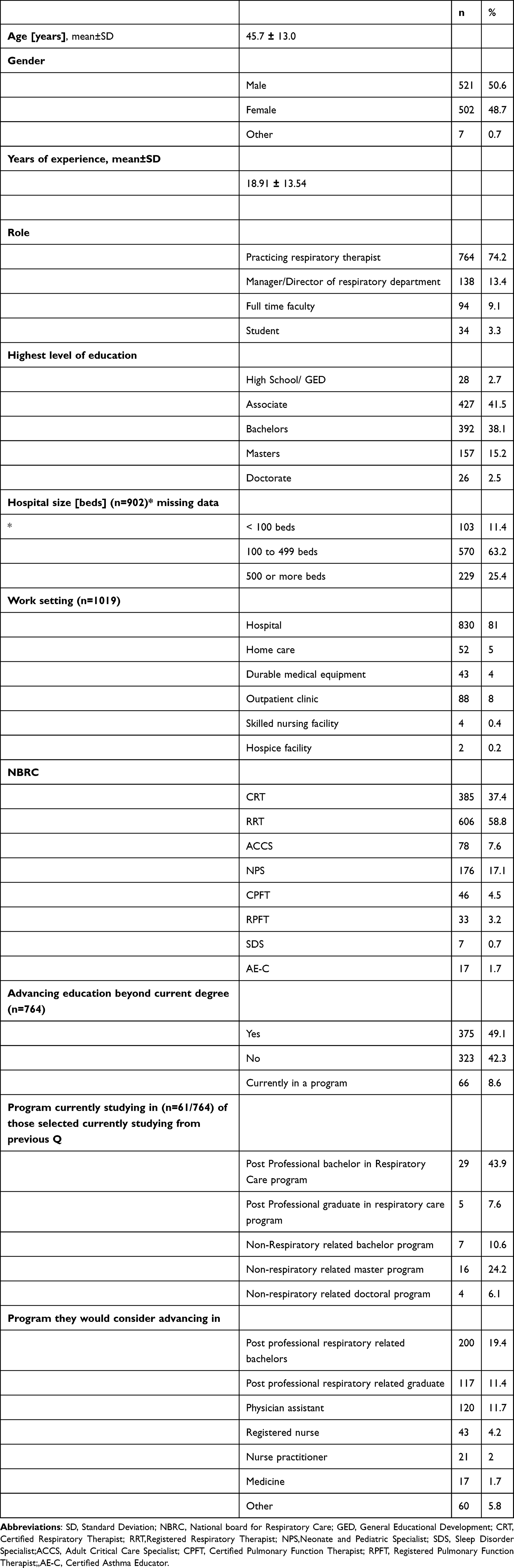 |
Table 1 Characteristics of the Respondents (N = 1030) |
Interestingly, 58% are currently or are considering advancing their education beyond their present degree. Those who are currently in a program advancing their education, 51% are in a respiratory related program. Moreover, for those who would consider advancing beyond current degree, only 30% would consider choosing a respiratory related program. Table 1
APRT: Descriptive Analysis
Table 2 represents questions related to APRT. More than half of the respondents (56.2%) already have knowledge of APRT. The majority (91.1%) support the establishment of the APRT profession in the state of California, with 58% recommending the profession to be at a graduate level degree. When asked if there was a potential employment opportunity for an APRT at their facility, 67.1% responded with yes. Moreover, 71% reported that APRT should have its own separate license other than the current RCP license within the state. Table 3 shows APRT related questions in terms of which areas an APRT should work at where intensive care units, emergency room and outpatient clinics were selected the most.
 |
Table 2 Key Advanced Practice in Respiratory Care Related Questions |
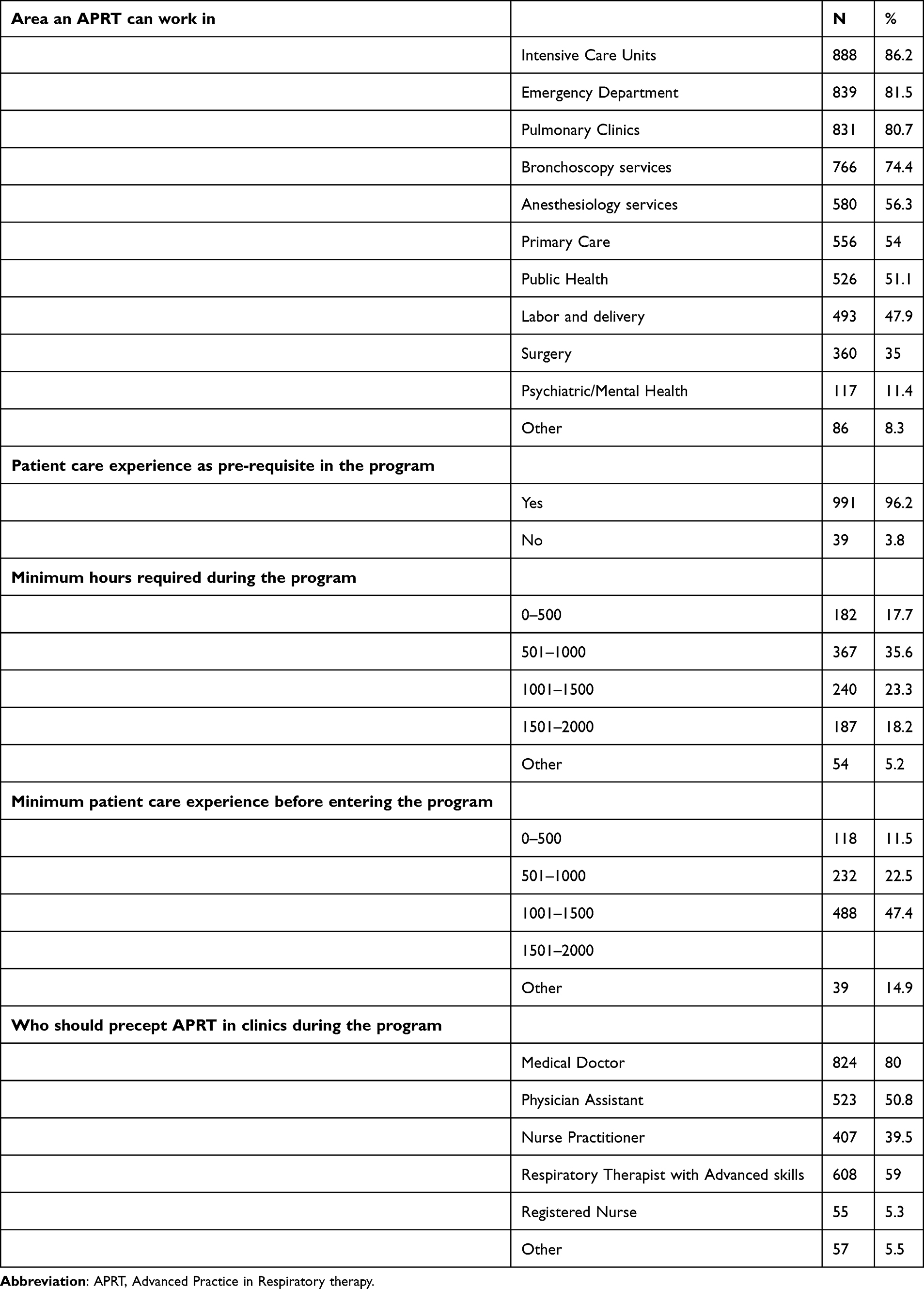 |
Table 3 Respondents’ Description of Which Areas an APRT Would Work at as Well as Educational Program Related Questions |
Chi-Square results showed that the higher the education the higher the support (85.7%) for high school versus 88.1% for those with associate degree versus 92.6% for those with bachelor’s degree versus 94.9% for master’s degree versus 100% among those with doctorate degrees (χ2= 12.3, p = 0.015, η = 0.1). In addition, those with knowledge of APRT were more supportive of establishing the APRT (χ2 = 9.1, p=0.003, η= 0.1).
Managers and Directors of RT Department in Hospitals (n=138)
Among this group, 2 had GED, 31 associate degree; 52 bachelor’s degree, 47 master’s degree, and 7 doctoral degree. The majority worked in a medium size hospital of 100 to 499 beds (n = 81) with an average of 26.0 ± 11.5 years of experience. They also reported that they oversee a median of 40.5 (1, 250) full time RT staff within their department. When asked about hosting students, 110 reported that their hospital is a clinical site for RT students.
APRT Related Questions
When asked about support of APRT, 43 reported they do not support the establishment of APRT, while the majority supported establishing the profession (69%). At the same time, 110 see potential employment for APRT at their hospital once established.
Challenges and Barriers of APRT
Figure 1 shows barriers that respondents believe will face the establishment of APRT. The most common barriers were in order: acceptance of APRT among other advanced practice providers, acceptance among physicians, legislation, scope of practice, and reimbursement.
 |
Figure 1 Barriers to establishing the Advanced Practice in Respiratory Therapy [APRT] profession in the state of California. |
Open Ended Questions
Following an analysis of the qualitative open-ended questions, three major themes emerged, below are the themes along with examples for each theme:
Acceptance and Resistance From Other Professions
Respondents shared concern regarding support and acceptance from other professions (MD, APPs). They cited competition, professional recognition, and scope of practice as concerns.
Very slow acceptance - Unions will be an issue - RCB may be a barrier - has still not accepted BS as minimum. Not enough RTs who have masters to teach - Limited instructors in general.
Support from physicians and hospital administrators.
Resistance from other disciplines such as RN’s, MD’s, and PA/NP.
Legislation, Licensing, and Educational Infrastructure
Respondents reported that legislation approval is a major barrier citing other potential oppositions from other professions. In addition, they reported the need to have a clear scope of practice that defines APRT role to avoid overlap with existing professions. They also reported worries about shortage of qualified instructors and programs on top of program development and availability in educational institutions within the state.
The initial barriers would include details such as specific curriculum, determinants of mastery of curriculum, and recruiting trainers.
Scope of practice, and of course proving the profession as “valuable” and Capable amongst other health care providers perceptions.
Legislation supporting the development of a license for APRT. Possible barriers from NP/PA with license overlap.
Financial and Structural Challenges
Many respondents expressed concerns overcompensation, reimbursement, and the cost of education and licensing. Expressing that without adequate financial incentives, respiratory therapists may be reluctant to pursue APRT. There are also concerns regarding hospitals and healthcare institutions creating job openings for APRTs and ensuring that the advanced role aligns with organizational budgets, particularly in light of increasing labor costs in California.
They need to pay more if people attain this certification or else it just won’t be worth it.
Payment/wages.
Nursing unions, anesthesia, and health care entities desire to keep RT as a lower cost allied health modality in order to produce profits.
Discussion
The main objective of this study was to investigate the perception of APRT among the respiratory therapy community in the state of California.
The majority of the participants were bedside or manager RTs working in a hospital setting, more than 80%. Interestingly, while California is the largest state that has CoARC programs in the nation, with only 1 entry level bachelor’s program, more than half of the sample hold at least a bachelor’s degree. Furthermore, almost 60% are interested in advancing their education beyond their current degree. This shows the passion for advancing education, learning, and growth. It can be attributed to current changes within the state by allowing community colleges to start a post-professional bachelor’s program in respiratory care. In other words, graduates of the associate degree entry level programs have continued their education by applying for a post professional bachelors degree program [AS to BS/BA degree]. From a nationwide perspective, these findings were also seen in North Carolina where a majority of RT’s expressed interest in advancing their education.24 Moreover, this shows that it is trying to meet the AARC 2030 position statements on minimum of bachelor’s degree.25 Interestingly, in our study, 30% would advance their education in a program related to respiratory care, compared to Physician Assistant 11%, which is similar to Keene et al.26 This can be interpreted that there is some sort of loyalty within the profession by practicing RTs.
When looking at the APRT related questions, a high percentage, 44% of respondents had not heard of APRT or they had limited knowledge about it. This is a concern where it shows there is a need to educate all stakeholders about what APRT is about. Chi-Square analysis clearly shows the higher the degree the person holds and knowledge of APRT, the stronger the support for APRT establishment. Thus, the state society and educational programs should increase efforts to raise awareness of APRT among current and prospective respiratory therapists within the state.
Managers and directors clearly support the establishment of the profession even when they are late in their career. They see potential employment at their hospital and need for APRT as an APP. This is in line with what has been published in the literature about the need of non-MD specialized in cardiopulmonary disease as a solution for physician shortage and employment.27–30
While data from this study reflects the perception and support of APRT within the state, establishment is always going to be an issue. This support is recommended to have a separate license that is different from the current Respiratory Care Practitioner license where it will include extended scope of practice, such as prescriptive capacity at the provider level. As the respondents shared their perspective on barriers to establish the profession within the state, acceptance from MDs and other APPs was the highest, increased education, communication, and discussion with the perspective profession is the solution. This will help shape the scope of practice within the state, which is not yet established. This may also overcome some of the barriers and challenges reported by the respondents in this survey. Data in our study should also help education programs define pre-requisite requirements concerning minimal patient care experience prior to program entry. It also addresses having APPs and MDs as preceptors during the APRT student clinical rotation within the program. Based on this, educational programs and the profession should start thinking about the evaluation and assessment of APRT students by not relying only on competency based medical education model. Instead, they should establish an Entrustable Professional Activity (EPA) framework and model for evaluating and assessing APRT students. Alismail and Lopez (2020) have proposed a layout, model, and steps on the reasons to use EPAs for APRTs.23 Therefore, we believe that APRTs, when established, should be “entrusted” and evaluated at the provider level and not practitioner level. Physicians evaluate their residents and fellows using EPA models which is considered as a higher level compared to competency based framework.31–38
Limitation
This study has several limitations. First, low sample size and the use of convenience sampling approach where it might introduce sampling bias, and may not reflect the larger population. This introduces a bias where generalizability is hard to make considering the number of respiratory care professionals overall. Another limitation is the potential recall bias where respondents’ prior knowledge of APRT might potentially influence the results. Therefore, we recommend that further studies are needed from physicians and other APPs (NPs and PAs) to add their perspectives as it is crucial to the establishment of the APRT profession within the state. This can be achieved by either surveying them or conducting a qualitative methodology study [interviews or focus groups] to answer the following questions:
1. Is there a need to have a third APP, APRT, who is specialized in cardiopulmonary disease?
2. What would the scope of practice of an APRT be?
Lastly, an in-depth qualitative methodology study of various stakeholders [respiratory therapists, nursing, physicians, NPs, PAs, hospital directors, etc.] might also shed further insight on challenges and opportunities of APRT in the state.
Conclusion
The results of this descriptive pilot cross-sectional study show a strong support APRT profession in the state of California. Acceptance from other providers (MDs and APPs) along with legislation and scope of practice definition were the top barriers reported. It was also noted that there is a lack of understanding of what an APRT profession is where it shows a need for more education about the new profession from key stakeholders such as AARC, CSRC, and educational programs.
Acknowledgment
Abdullah Alismail and Yiqing Xu are co-first authors for this study. We would like to thank the California Society for Respiratory Care, the Respiratory Care Board of California, and all individuals who supported and distributed this survey. We also extend our gratitude to the participants who took part in this survey and shared their thoughts and opinions to help shape the APRT profession within the state of California.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Ms Krystal Craddock reports personal fees from Theravance Biopharma, Fisher and Paykel, AirLife, and Electromed, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Zhang X, Lin D, Pforsich H, Lin VW. Physician workforce in the United States of America: forecasting nationwide shortages. Hum Resour Health. 2020;18(1):8. doi:10.1186/s12960-020-0448-3
2. GlobalData P. The complexities of physician supply and demand: projections from 2021 to 2036 [Internet]. AAMC; 2024 [cited November 18, 2024]. Available from: https://www.aamc.org/media/75236/download.
3. Maganty A, Byrnes ME, Hamm M, et al. Barriers to rural health care from the provider perspective. Rural Remote Health. 2023;23(2):1–11. doi:10.3316/informit.197516774554362
4. Tran HM, Tsai FJ, Lee YL, et al. The impact of air pollution on respiratory diseases in an era of climate change: a review of the current evidence. Sci Total Environ. 2023;898:166340. doi:10.1016/j.scitotenv.2023.166340
5. Boers E, Barrett M, Su JG, et al. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Network Open. 2023;6(12):e2346598. doi:10.1001/jamanetworkopen.2023.46598
6. Center for Disease Control. Leading causes of death [Internet]; 2024 [cited November 18, 2024]. Available from: https://www.cdc.gov/nchs/fastats/leading-causes-of-death.html.
7. Walensky Rochelle P, McCann Nicole C. Challenges to the future of a robust physician workforce in the United States. N Engl J Med. 2025;392(3):286–295. doi:10.1056/NEJMsr2412784
8. Koffi A. Addressing the rural primary care physician shortage: a focused review of policy interventions and their implications [Internet] [masteressay]. University of Pittsburgh; 2024 [cited March 26, 2025]. Available from: https://d-scholarship.pitt.edu/46138/.
9. Adashi EY, O’Mahony DP, Cohen IG. The National physician shortage: the imperative of congressional action. Am J Med. 2024;137(11):1030–1031. doi:10.1016/j.amjmed.2024.05.032
10. Menezes J, Zahalka C. Anesthesiologist shortage in the United States: a call for action. J Med Surg Public Health. 2024;2:100048. doi:10.1016/j.glmedi.2024.100048
11. Leifeld N, Ongoro G, Bright P, Nalin P. Alleviating the physician shortage by increasing medical student and resident physician capacity in the North Midwest (Iowa, Minnesota, North Dakota, South Dakota, Wisconsin). J Reg Med Campuses. 2024;7(4).
12. Varga DW, Lee TH. Resolving physician shortages with new care models. NEJM Catal Innov Care Deliv. 2024. doi:10.1056/CAT.24.0072
13. Gross TK, Lane NE, Timm NL. COMMITTEE ON PEDIATRIC EMERGENCY MEDICINE. Crowding in the Emergency Department: challenges and best practices for the care of children. Pediatrics. 2023;151(3):e2022060972. doi:10.1542/peds.2022-060972
14. Hooker RS, Christian RL. The changing employment of physicians, nurse practitioners, and physician associates/assistants. J Am Assoc Nurse Pract. 2023;35(8):487–493. doi:10.1097/JXX.0000000000000917
15. Varekojis SM, Schweller J, Sergakis G. Introducing the advanced practice respiratory therapist. Chest. 2021;160(2):e157–9. doi:10.1016/j.chest.2021.03.053
16. AARC [Internet]. Advanced Practice Respiratory Therapist. [cited November 18, 2024]. Available from: https://www.aarc.org/your-rt-career/advanced-practice-rt/.
17. Accreditation Standards for Advanced Practice Programs in Respiratory Care [Internet]. Commission on Accreditation for Respiratory Care (CoARC); 2022 [cited November 18, 2024]. Available from: https://coarc.com/wp-content/uploads/2023/01/CoARC-APRT-Standards-6.1.2022.E.pdf.
18. Hanlon P. Advanced practice respiratory therapists expand the scope of practice. RT J Respir Care Pract. 2022;35(1):20–23.
19. Varekojis SM, Schweller J, Sergakis G. Creation of an Advanced Practice Respiratory Therapy (APRT) Education Program. Chest. 2024;167:818–824. doi:10.1016/j.chest.2024.10.024
20. AARC [Internet]. The advanced practice respiratory therapist gets a big boost from the VA in Maryland. [cited November 18, 2024]. Available from: https://www.aarc.org/news/an23-the-advanced-practice-respiratory-therapist-gets-a-big-boost-from-the-va-in-maryland/0.
21. O’Neil K. Reintroducing the advanced practice respiratory therapist. Chest. 2025;167(3):642–644. doi:10.1016/j.chest.2024.11.005
22. Shaw R, Vines D, Benavente J, Keene S. The foundation supporting future assessments of education program outcomes among providers of advanced practice respiratory therapy. Chest. 2025;167(1):202–210. doi:10.1016/j.chest.2024.09.026
23. Alismail A, López D. Clinical competencies in advanced practice respiratory therapy education: is it time to entrust the learner? Adv Med Educ Pract. 2020;11:83–89. doi:10.2147/AMEP.S239376
24. Krystal B, Jamy C, Kimberly C. Perceptions of pursuing advanced education among respiratory therapists: a pilot study. Respir Care Educ Annu. 2024;33(Fall 2024):3–11.
25. AARC. Entry requirements to respiratory therapy practice: 2030 and thereafter [Internet]. AARC; 2019 [cited November 18, 2024]. Available from: https://www.aarc.org/wp-content/uploads/2019/09/statement-entry-requirements-to-respiratory-therapy-practice-2030-and-therafter.pdf.
26. Keene S, McHenry K, Byington R, Washam M. Respiratory therapists as physician extenders: perceptions of practitioners and educators. ETSU Fac Works [Internet]; 2015. Available from: https://dc.etsu.edu/etsu-works/2548.
27. Joyner RL, Strickland SL, Becker EA, et al. Adequacy of the provider workforce for persons with cardiopulmonary disease. Chest. 2020;157(5):1221–1229. doi:10.1016/j.chest.2019.09.030
28. Physician support for non-physician advanced practice providers for persons with cardiopulmonary disease | respiratory care [Internet]. [cited November 18, 2024]. Available from: https://rc.rcjournal.com/content/65/11/1702.short.
29. Hwang D, Woodrum RR. Inadequacy of current solutions to address provider shortage. Chest. 2020;157(5):1055–1057. doi:10.1016/j.chest.2020.03.025
30. Ireland K, Daher N, Terry M, et al. Perception, Challenges, and Barriers of Point-of-Care Lung Ultrasound Among Respiratory Therapist in the United States. CHEST Pulmonary. 2024;2(1):100029.
31. Ten Cate O. Nuts and bolts of entrustable professional activities. J Grad Med Educ. 2013;5(1):157–158. doi:10.4300/JGME-D-12-00380.1
32. ten Cate O. Entrustability of professional activities and competency-based training. Med Educ. 2005;39(12):1176–1177. doi:10.1111/j.1365-2929.2005.02341.x
33. Bargagliotti LA, Davenport D. Entrustables and entrustment: through the looking glass at the clinical making of a nurse practitioner. J Nurse Pract. 2017;13(8):e367–74. doi:10.1016/j.nurpra.2017.05.018
34. Mulder H, Ten Cate O, Daalder R, Berkvens J. Building a competency-based workplace curriculum around entrustable professional activities: the case of physician assistant training. Med Teach. 2010;32(10):e453–459. doi:10.3109/0142159X.2010.513719
35. Anthamatten A, Pfieffer ML, Richmond A, Glassford M. Exploring the utility of entrustable professional activities as a framework to enhance nurse practitioner education. Nurse Educ. 2020;45(2):83. doi:10.1097/NNE.0000000000000697
36. Jarrett JB, Berenbrok LA, Goliak KL, Meyer SM, Shaughnessy AF. Entrustable professional activities as a novel framework for pharmacy education. Am J Pharm Educ. 2018;82(5):6256. doi:10.5688/ajpe6256
37. Pittenger AL, Chapman SA, Frail CK, Moon JY, Undeberg MR, Orzoff JH. Entrustable professional activities for pharmacy practice. Am J Pharm Educ. 2016;80(4):57. doi:10.5688/ajpe80457
38. Fessler HE, Addrizzo-Harris D, Beck JM, et al. Entrustable professional activities and curricular milestones for fellowship training in pulmonary and critical care medicine: report of a multisociety working group. Chest. 2014;146(3):813–834. doi:10.1378/chest.14-0710
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.