")
Back to Journals » Clinical Interventions in Aging » Volume 20
Advancements in the Optimization of Surgical Timing in Elderly Patients with Hip Fractures: A Narrative Review and Future Perspectives
Authors Xu X, Yu H, Wang J, Guo J
Received 17 March 2025
Accepted for publication 14 June 2025
Published 24 June 2025 Volume 2025:20 Pages 881—894
DOI https://doi.org/10.2147/CIA.S526209
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Xin Xu,1,2 Hui Yu,1,2 Junxiang Wang,1,2 Junfei Guo1
1Department of Joint Surgery, Honghui Hospital, Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China; 2Xi’an Key Laboratory of Pathogenesis and Precision Treatment of Arthritis, Xi’an, Shaanxi, People’s Republic of China
Correspondence: Junfei Guo, Department of Joint Surgery, Honghui Hospital, Xi’an Jiaotong University, Xi’an, No. 555, Youyi East Road, Beilin District, Xi’an, Shaanxi, 710054, People’s Republic of China, Email [email protected]
Abstract: The optimal timing for hip fracture surgery in elderly patients remains a topic of intense debate and complexity, with many factors influencing the decision-making process. This review examines the current evidence, exploring the advantages and challenges of early versus delayed intervention. It considers medical stability, preoperative medical stabilization, and patient comorbidities, and logistical challenges such as operating room availability and specialized physician access. While multiple studies have examined early versus delayed surgery, a universally agreed definition of “unacceptable delay” is absent. Some evidence indicates that postponing surgery beyond 24 hours may not significantly impact mortality and complication rates, especially in individuals with complex medical conditions. Conversely, early intervention within 48 hours is often recommended for stable patients. Several contributing factors, such as preoperative medical stabilization, hospital resources, and organizational structures, further complicate the issue. This review highlights the need for a nuanced, individualized, and patient-centered approach, taking into account the unique needs of each patient and the specific circumstances of the healthcare setting. It also emphasizes the importance of further research to provide a more comprehensive understanding of what constitutes an optimal delay, rather than adhering to rigid time frames. By offering a multifaceted examination of this critical subject, the review contributes valuable insights that may guide future clinical practice and policy in orthopedic care.
Keywords: hip fracture, elderly, surgical timing, early surgery, delayed surgery, narrative review
Introduction
Studies conducted in the United States1 and Norway2 have highlighted that although there has been a slight decline in overall hip fracture (HF) rates due to improved osteoporosis treatment, the absolute number of elderly individuals globally suffering from HFs is likely to increase as the older adult population expands. Nowadays, in older populations, HF is a frequent condition that significantly raises the rates of illness, disability, death, and disease, resulting in a large financial burden on society. Despite advancements in surgical methods leading to positive outcomes in functional restoration and alleviation of pain, observational studies demonstrated that excessively early intervention may confer undue risk in a frail fracture patient population, for example, those with American Society of Anesthesiologists (ASA) physical status III–IV, severe cognitive impairment (eg, dementia), significant malnutrition (serum albumin <3.0 g/dL), or sarcopenia (low muscle mass and strength) experience unexpectedly elevated rates of postoperative complications and mortality.3,4
Surgery has emerged as the preferred option for addressing HFs in older individuals, as the absence of surgical intervention frequently leads to a more unfavorable prognosis.5,6 According to reports, the likelihood of all-cause mortality in older individuals rises by 5 to 8-fold during the initial 3-month period following a HF compared with age- and sex-matched community controls, which increased risk of death continues for as long as 10 years.7 Moreover, the challenges faced by elderly individuals extend beyond mortality to include post-HF surgery issues, such as loss of mobility and psychological impacts.8 The issue is not limited to a specific area, but rather affects the entire world. Germany witnessed a total of 120,000 surgical interventions for proximal femoral fractures in 2018, with an annual mortality rate of 33,500 individuals due to HFs in the country.9 The problem for seniors after a HF goes beyond mortality, often involving the extra challenge of surgery after the first injury. It is distinguished by the decline in partial mobility, resulting in either partial or complete dependence loss10 and accompanied by unfavorable psychological consequences.11 Consequently, there has been a notable financial impact on patients, their families, healthcare systems, and public resources.12 As human life expectancy is projected to rise over the next decade, the impact of HF and its associated consequences on healthcare systems and society is expected to intensify.13
For more than two decades, global research has explored how the timing of HF surgery influences patient outcomes, yielding at times contradictory conclusions (Figure 1 and 2). While several observational studies indicate that delays beyond 48 hours are associated with higher rates of stress ulcers, postoperative infections, major medical complications, and both in-hospital and one-year mortality,14,15 others report minimal differences or even potential harms of overly early intervention in medically complex or frail patients.16–18 As a result, international guidelines uniformly recommend surgery within 24–48 hours of admission, and many health systems monitor the proportion of cases meeting this benchmark as a quality metric.19,20 Nevertheless, patient comorbidities,21 institutional resources,22 and logistical factors such as inter-facility transfers and preoperative optimization often preclude universal adherence. Surveys from China,6 Japan,22 the United Kingdom,23 and multinational cohorts24 consistently show that only a minority of patients receive surgery within the recommended window.
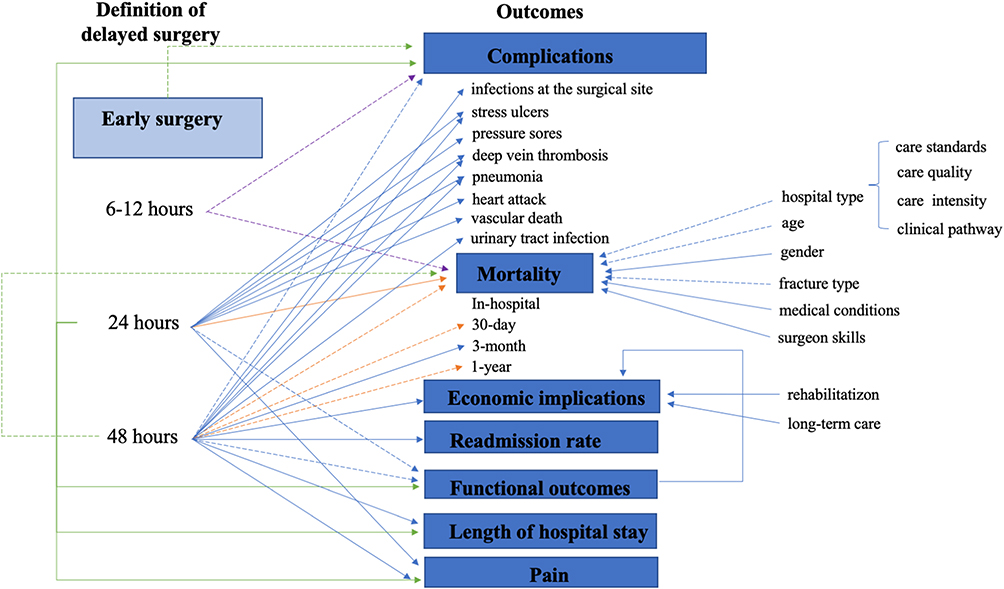 |
Figure 1 Impact of early surgery on outcomes following Hip fracture surgery.Dependencies among factors involved in early surgical timing (defined as within 6–12 hours, 24 hours, and 48 hours) and outcomes including complications, mortality, economic implications, readmission rate, functional outcomes, length of hospital stay, and pain. The arrows represent the relations between variables reported in the reviewed literature, where the solid arrows represent definitively directional dependencies between the variables and the dashed arrow represents the controversial association between the variables. The blue arrows indicate that the level of evidence is from observational studies. The purple arrows indicate that the level of evidence is from interventional studies. The Orange arrows indicate that the level of evidence is from meta-analysis studies. The green arrows indicate that the level of evidence is from guidelines. |
 |
Figure 2 Impact of delayed surgery on outcomes following Hip fracture surgery.Dependencies among factors involved in delayed surgical timing (defined as beyond 72 hours, 96 hours, and 120 hours) and outcomes including complications, mortality, economic implications, readmission rate, functional outcomes, length of hospital stay, and pain. The arrows represent the relations between variables reported in the reviewed literature, where the solid arrows represent definitively directional dependencies between the variables and the dashed arrow represents the controversial association between the variables. The blue arrows indicate that the level of evidence is from observational studies. The purple arrows indicate that the level of evidence is from interventional studies. The Orange arrows indicate that the level of evidence is from meta-analysis studies. The green arrows indicate that the level of evidence is from guidelines. |
Research into the effects of surgical timing on elderly HF patients has provided an extensive overview of current knowledge in surgical timing of elderly HF. This narrative review encompasses studies published between 1987 and 2025, thereby clarifying the temporal scope of the evidence considered. Against this background of mixed evidence and implementation challenges, our narrative review aims to (1) synthesize and critically appraise the literature on surgical timing and key clinical outcomes, (2) clarify why certain subgroups may benefit from tailored timing strategies, and (3) propose a conceptual framework for individualized decision-making that balances early intervention with patient safety. We believe this approach will help resolve prevailing uncertainties and guide future research toward more personalized perioperative care.
Current Controversy Regarding the Optimal Timing for Surgery in Elderly HF Patients
When is the optimal timing for surgery in a patient population that could most beneficial for patient outcomes? Numerous academics have looked into how the timing of surgery correlates with outcomes in medical studies, yet significant debate persists regarding the findings.16–18,25–28
According to British guidelines in 1989, early surgery within 24 hours of HF was recommended for improved functional outcomes, reduced complications, and shorter length of hospital stays (LOS) and pain duration.29 Initial study supported these recommendations,17 even though data showed no significant impact on mortality from delays exceeding 24 hours. This policy persisted due to the vulnerability of elderly patients to complications and the humanitarian need for prompt intervention. Over the years, the global consensus has shifted towards performing surgery within 24–48 hours after admission, with some nations even incentivizing prompt surgical treatment.30,31 While certain research, particularly regarding immediate results, has indicated advantages,32–34 concerns persist that rushed procedures may compromise preoperative preparation and increase the risk of perioperative complications.17,35
Proponents of early surgical intervention highlight its potential to reduce complications associated with beds, like pressure ulcers and deep vein thrombosis (DVT), and enhance functional outcomes, decrease LOS, and minimize postoperative complications.16,17,25,36 Critics, however, argue that delaying surgery allows time for medical stabilization, thereby reducing operative complications, without affecting mortality rates; conversely, expedited surgical procedures elevate the likelihood of perioperative complications.37–39 The lack of consensus on the definition of “unacceptable delay” in HF surgery (ranging from 6 to 72 hours or more) complicates the issue. A dearth of extensive RCTs further hampers the ability to provide definitive evidence on the timing of surgery. Ethical considerations have limited the use of experimental designs, leaving cohort studies as the most reliable source of information on this matter. According to two recent reviews addressing this issue, the relationship between delayed surgery and postoperative outcomes remains controversial.40,41 It is generally accepted that delayed surgery extends the LOS and increases the risk of pressure sores, pressure ulcers, and pneumonia, while also contributing positively to pain relief and rapid functional recovery. However, further research is necessary to elucidate the correlation between surgical timing, particularly in cases of unacceptable delay, and mortality.
Factors Contributing to Surgical Delay
Several factors contribute to the postponement of HF surgery that can be grouped into three principal domains
Administrative and Logistical Constraints
Operating room availability: limited operating room block time and competing emergency caseloads often lead to scheduling bottlenecks.42,43
Workforce shortages: insufficient numbers of orthopedic surgeons, anesthesiologists, and specialized nursing staff can further impede timely surgery.44
Diagnostic and laboratory delays: dependence on central laboratory workflows and imaging services may prolong preoperative clearance.44
Clinical Optimization Requirements
Medical stabilization: acute comorbidities such as uncontrolled heart failure, electrolyte imbalances, or advanced chronic kidney disease require necessitate preoperative management to mitigate perioperative risk.45
Anticoagulation reversal: protocols for vitamin K administration or FFP infusion introduce deliberate delays to achieve safe coagulation profiles.
Patient-Related and Socioeconomic Factors
Demographics and comorbidities: advanced age, frailty (eg, ASA III–IV status), cognitive impairment, and chronic diseases influence readiness for surgery.6,24
Socioeconomic disparities: insurance status, geographic access to specialist centers, and hospital ownership/volume models can differentially affect time-to-operating room.42,44,46,47
The process from fracture occurrence to surgery involves a complex pathway, including patient assessment, clinical stability evaluation, selection of surgical approach, anesthesia determination, and adherence to hospital policies. The primary challenge in addressing surgical delays lies in discerning the disparities between delays due to administrative reasons and those necessary for optimizing acute medical conditions prior to surgery (Figure 3).
 |
Figure 3 Influencing factors for surgical timing.Factors influencing time to Hip fracture surgery. The arrows represent the relations between factors and surgical timing reported in the reviewed literature. The solid arrows represent definitively directional dependencies between the variables. The dashed arrow represents the controversial association between the variables. The blue arrows indicate that the level of evidence is from observational studies. The purple arrows indicate that the level of evidence is from interventional studies. The Orange arrows indicate that the level of evidence is from meta-analysis studies. The green arrows indicate that the level of evidence is from guidelines. |
Analytical Insights
By categorizing delays, we can better tailor solutions as:
- Streamlining administrative delays: implementing dedicated HF operating rooms and automated scheduling algorithms can substantially reduce non-clinical wait times.
- Optimizing clinical pathways: establishing standardized preoperative optimization protocols, such as rapid geriatric co-management, point-of-care testing for coagulation and electrolytes, and multidisciplinary “fast-track” pathways, which can minimize medically necessary delays without compromising safety.
- Addressing socioeconomic barriers: integrating patient navigator programs and telemedicine consultations can improve access and equity, ensuring that vulnerable populations receive timely care.
How Chronic Use of Blood Anticoagulants Affects the Timing of Surgery
Approximately 6.0%-14.7% of HF patients are estimated to use anticoagulants. In clinical practice, anticoagulants are frequently regarded as indicators of the existence of comorbidities like atrial fibrillation, thromboembolism, prosthetic heart valves, and active cardiovascular diseases.48 According to a survey of UK trauma centers, 70% reported having warfarin-reversal guidelines for HF patients.49 Of these, the majority (70%) discontinue warfarin and await natural reversal, whereas a minority employ active strategies using intravenous vitamin K or fresh frozen plasma to expedite INR normalization. Reversal decisions are typically initiated by the orthopaedic or emergency physician and executed under the direction of the anaesthesiologist in collaboration with hematology. Intravenous vitamin K (1–3 mg) is administered per institutional protocols, and intravenous FFP (20 mL/kg) is reserved for cases requiring immediate correction (eg, INR > 2.0 or active bleeding).50–52
Indeed, the act of patiently awaiting natural reversal could lead to an extended period of being under the influence of anticoagulants for patients, thereby heightening the chances of thrombosis development and causing a delay in surgical procedures. This delay is linked to complications during the perioperative period as well as other unfavorable consequences. Typically, it takes around 4–5 days for healthy individuals to naturally revert from an INR of 2–3 to 1.2.53 Furthermore, individuals undergoing antibiotic and alternative medication therapies may also encounter an unplanned rise in INR levels, causing a substantial postponement in the scheduling of the surgical procedure.48 A typical INR threshold of 1.5 is traditionally aimed for surgeries involving neuraxial anesthesia. Nevertheless, the uncertainties and advantages of this objective remain unclear.54,55 Most consensus guidelines56 recommend deferring neuraxial blocks until the INR is below 1.5 to minimize the risk of spinal epidural hematoma. Retrospective cohort studies have demonstrated bleeding complications becomes evident with a preoperative INR in the 1.1–1.25 range, and those patients with INR≥1.5 are at significantly increased risk of mortality.57,58 On the contrary, according to a number of recent studies, it has been demonstrated that individuals with INR levels ranging from 1.5 to 2, which exceed the typical range, are able to proceed with surgical procedures compared with those with normal coagulation profiles. Notably, when compared to the control group having an INR value of 1.2, there was no noteworthy rise in hemorrhage or additional transfusion requirements, ICU admissions, or mortality rates at 30 days and 1 year postoperatively, which can typically be managed with standard measures.53,59
Algorithms for making decisions regarding anticoagulant treatment offer various choices for selecting warfarin, direct oral anticoagulants, and alternative anticoagulants for patients who require anticoagulation. These algorithms help identify patients who may benefit from a transition period or those who need active management.60 The growing body of literature indicates that these algorithms for active management decision-making have the potential to cut the time between patient hospital admission and surgery in half, lower the incidence of surgical cancellations, and potentially improve perioperative complication and mortality rates to different extents.53,60,61
Effect of Surgical Timing on Mortality Rates in Older Individuals with HFs
The surgical timing in HF patients and its correlation with mortality rates remains a widely debated topic within the orthopedic research community.
Evidence Supporting Early Surgery
Uzoigwe et al examined 2056 patients, categorizing them into groups based on surgery within 12, 24, or after 36 hours. Mortality rates decreased gradually for surgeries within 24 and 12 hours, but increased after 36 hours.25 Similar findings by Hapuarachchi et al indicated higher mortality in patients operated on more than 24 hours later.26 Recently, the study by Danford et al,62 involving 27,058 elderly patients with HFs and using the national trauma data bank, suggested that postponing surgery for over 48 hours could be associated with increased short-term morbidity and mortality. In Canada, a large retrospective study identified a crucial 24-hour period for mortality, associating early surgery with decreased mortality and postoperative complications like heart attack, lung infection, and DVT.63 In 2018, Chang et al carried out a systematic review and meta-analysis, examining 25,349 patients across 16 studies, to determine preventable risk factors for mortality post-HF surgery. Their results further identified that time to surgery over 2 days significantly increased mortality risk.64 In 2020, research from a multicenter clinical trial65 explored whether patients with HFs benefited more from surgery conducted within 6 hours or 24 hours of being admitted. The HIP ATTACK study concluded that the accelerated surgery group did not experience any advantageous outcome in relation to mortality or other significant complications when compared with the standard care group. This study’s objective was to explore extremely early versus early surgical procedures, but its applicability across varying global medical resource scenarios remains limited. More recently, the study by Yaacobi et al66 demonstrated that postponing surgery was significantly associated with elevated mortality rates at 3 and 12 months following surgery. Systematic reviews and meta-analyses have consistently found that surgery performed within 24 to 72 hours reduces mortality rates.19,21 Klestil et al67 evaluated data from more than 30,000 patients involved in 28 prospective trials and found that surgery within 48 hours resulted in notably less perioperative issues (8% compared to 17%) and a decrease of 20% in overall mortality rates.
Evidence Indicating Limited or No Impact of Delay
In contrast, some studies suggest that postponing surgery has limited or no impact on mortality.68,69 Al-Ani et al16 compared results of surgery within 24, 36, and 48 hours, finding no disparity in mortality rates. Moran et al39 reported stability in outcomes with delays up to four days, noting an increase only after that period. Vidán et al43 corroborated these findings, showing no effect on postoperative mortality for delays up to 120 hours, even after adjusting for age and comorbidities. Kavak et al,27 further suggested that a three-day delay may be acceptable for medical optimization and team consensus. According to a prospective cohort study of 1,234 patients, authors70 suggested that a delay of more than two days for HF surgery did not correlate with increased complications or mortality if the delay was to stabilize patients with active comorbidities at admission. Recently, Vitiello et al revealed that in the case of acute and reversible conditions, waiting about 24 h to stabilize the patient with preoperative stabilization protocols, such as managing anticoagulation, optimizing hemodynamics, or addressing acute medical conditions including infection prevention, guarantees better results.71 De Luca et al also demonstrated that in HF patients with age over 85, the early surgery threshold may be extended to 72 hours to provide time for pre-operative stabilization and medical optimization, as intra-hospital and 30-day mortality rates are still considerably lower.72
Nuanced Findings in Specific Subgroups and Methodological Constraints
Seckel et al28 found that performing surgery on isolated HFs in people in their nineties within 24 hours is linked to reduced mortality compared to postponing the surgery while Schermann et al73 showed that for patients aged 80–94, surgery on the initial day might be more favorable than on the following day, while for those aged 95 and above, the timing of surgery did not affect mortality. In 1987, certain research indicates that even medically poor individuals can benefit from surgery within a day or two.74 In 1992, Bredahl and their et.al discovered that conducting surgery within 12 hours led to a significant decrease in mortality between 5 months and 1 year.75 However, the impact might diminish when considering influencing variables such as chronic illnesses and mental well-being.43,45 Other studies, like Zuckerman et al, found that delays over 72 hours increased mortality rates, even after adjusting for confounding factors.76 A systematic analysis21 examined 16 studies (both prospective and retrospective) involving more than 250,000 patients, analyzed the relationship between surgery timing and mortality in individuals with HF. The review revealed that surgical delay >48 hours was linked to higher mortality rates. However, the researchers acknowledged that observational studies may have confounding variables that restrict making definitive conclusions on this matter.
Contextual Considerations and Future Directions
Systematic reviews by Khan et al and retrospective analysis by Kenzora et al also found that survival outcomes were not enhanced by early surgery, and in some cases, patients who underwent immediate surgery had higher 1-year mortality.77,78 It was noted that numerous patients who were not appropriate for immediate surgery underwent the procedure and had a higher likelihood of benefiting from postponing the surgery to enhance their medical condition. Incorporating these patients into the early surgery group would lessen the true impact of postponing the surgery. The guidelines of the British Orthopaedic Association and the Association of Anaesthetists of Great Britain and Ireland79 outline several factors that are considered acceptable delays, which include low hemoglobin levels (<8g/dL), imbalanced electrolytes, unmanaged diabetes, heart failure, irregular heart rhythm, respiratory infection, and manageable blood clotting issues. For safety reasons, it is recommended that patients with these coexisting conditions should be adequately stabilized prior to undergoing surgery (Table 1).
 |
Table 1 Reasons for Delaying Surgery for Hip Fracture That the Working Party Considers Acceptable and Unacceptable |
The lack of consistent results across studies is often attributed to methodological constraints, such as insufficient statistical power and inadequate adjustment for potential confounding factors. Weller et al approximated that at least 5,000 participants would be required to identify a significant odds ratio of 1.2 with a power of 80% and α = 0.05 in favor of early surgery, and even more when adjusting for multiple confounding factors.80 Small-scale studies may lead to unreliable outcomes due to a limited range of prognostic factors and an insufficient patient population. In 2017, Sheehan et al created a dependency chart to illustrate the complex interactions among different factors. The findings highlighted the interdependence among multiple factors and strengthened the causal inference linking mortality outcomes to changes in surgical timing.33
Influence of Timing of Surgery on Occurrence of Postoperative Complications
Postoperative complications are intricately linked to the timing of HF surgery. Several research suggest that when surgery is performed does not have a major impact on the occurrence of postoperative complications.39,81 However, other researches emphasize a connection between delays exceeding 24 hours and increased occurrences of pressure sores and vascular death.32,38,82 Systematic reviews and cohort studies also linked delayed surgery to pneumonia.19,32,83 The relationship between delayed surgery and venous thromboembolism events is also identified. Shin et al reporting an 11.1% incidence when surgery was delayed over 24 hours84 while Sun et al83 concluded that earlier surgery can reduce the DVT rates, as well as pulmonary infections, urinary tract infection, and readmission rate. Thorough preoperative examination is recommended to mitigate this risk. Al-Ani et al found that early surgery could enhance long-term functional outcomes, increasing the likelihood of achieving self-sufficiency within 4 months.16 Delayed surgery, associated with stress reactions and insulin insensitivity, may hasten muscle decline, impede recovery, and increase delirium risk.85 Surgical delay has been identified as an independent risk factor for postoperative delirium: in a prospective cohort of HF patients, each 24-hour delay increased delirium risk by 11%.86 Early surgery (within 24 hours) has been shown to reduce postoperative delirium by approximately 26% compared with standard pathways.87 Moreover, the reduced LOS conferred by earlier surgery further contributes to delirium prevention by minimizing exposure to immobility, polypharmacy, and hospital environmental stressors.88 A study involving 1,206 patients found that performing surgery within 24 hours greatly decreased the duration of severe pain.17 However, the diverse findings and methodological limitations in many studies, especially the lack of comprehensive prospective RCTs, make it challenging to definitively determine the impact of surgical delay on outcomes. The existing evidence may not sufficiently distinguish whether the delay itself influences outcomes or merely indicates underlying comorbidities that adversely affect complication outcomes.
Impact of Timing of Surgery on Recovery of Functional Outcomes
The influence of surgical timing on patients’ ability to regain independent living status after HF has yielded conflicting results, with variations observed across different studies. While some have identified a significant correlation between early surgical intervention and improved independence,89,90 others have reported non-significant correlations.91 In a prospective multicenter cohort study, Cai et al revealed that delayed surgery, particularly beyond 72 hours from injury, led to poor functional outcomes, with significant impacts on hip function and slower early recovery within the first three months.90 Conversely, Doruk et al found that performing surgery within 5 days of admission could enable early weight-bearing post-operation and facilitate recovery of daily activities.92
Impact of Timing of Surgery on the LOS and Costs
The consensus in the literature underscores the relationship between early surgical intervention for HFs and shorter LOS in the hospital. Numerous studies, both unadjusted18,93 and adjusted16,83 suggest that delaying surgery is related to increased LOS. A 15-year study carried out by Siegmeth et al on 3,628 individuals who had HF surgery, demonstrated that those who had surgery within 48 hours experienced a reduction in average LOS by 10.9 days.18 Similarly, Al-Ani et al concluded that surgery within a day experienced a reduction of 4 days in their median hospital stay.16 Recently, Guo et al94 identified that surgical delay and BMI are associated with longer hospital stays rather than mortality, which agrees with the literature by Kempenaers et al95 and Lizaur et al.70
The primary reason cited for surgical postponement is the lack of operating rooms and essential resources.19,21,43,96–98 Additionally, studies have explored the “weekend effect” whether a deficiency in care quality during weekends has been linked to unfavorable outcomes.99,100 Some researchers identified a link between being admitted on weekends and higher 30-day mortality rates,101 while others, including a rigorous meta-analysis,102 and a more recent study in China,99 found no significant association with HFs. The contrasting findings on the weekend effect may reflect differences in institutional practices, staffing, and resource allocation. These insights highlight the need for optimizing surgical timing and resource management in treating HFs, with potential implications for neutralizing any potential “weekend effect”, reducing LOS, and improving patient outcomes.
The economic implications of HFs in the elderly are substantial, encompassing initial hospitalization, rehabilitation, and long-term care. Study has highlighted that early surgical intervention may reduce medical expenses, as delayed surgery correlates with an extended LOS.103
Strategies for Managing Delayed Surgery in Elderly HFs
In managing elderly HFs, multidisciplinary cooperation is paramount, involving emergency departments, radiology, anesthesia, internal medicine, operating rooms, and rehabilitation departments. The UK’s National Institute for Health and Care Excellence has outlined specific medical conditions and treatments that may necessitate the postponement of HF surgery, including anemia, anticoagulation therapy, electrolyte imbalances, and unregulated heart failure, among others.104 Other studies have proposed expanded lists,18,105 and personal reasons may also influence surgery delay, underscoring the need for expert consensus.
Efficient reduction in surgical delay may be achieved through expedited preoperative assessments, and specialized coordination or dedicated operating rooms for elderly HF patients have been shown to decrease wait times and complications particularly for patients in good health and without significant underlying conditions.106 Yet, contrasting evidence suggests hospital administration may have minimal impact on mortality and complication rates within well-functioning healthcare systems.45 Factors like age, gender, fracture type, and preoperative condition predominantly contribute to mortality, with adjustable factors like surgical timing having less effect.
Given the significance and debate surrounding elderly HF surgery, prioritizing resource allocation is vital. Some healthcare systems have implemented accelerated surgery pathways,96–98 but the unclear relationship between surgical timing and adverse outcomes like patient death necessitates careful consideration to balance urgency and potential benefits.
Exploration of Techniques and Future Outlook for Timing of Surgical Procedures
Determining when to optimally perform HF surgery is a complex issue, largely because it relies on observational studies that are inherently prone to biases and confounding factors. While prospective observational studies can reduce bias by establishing a temporal sequence of events, confounding variables still pose a challenge. Regression analysis has been employed to adjust findings, considering risk factors and forecasting outcomes. In some instances, adjusted results have revealed that the correlation between surgery delay and in-hospital mortality lessens compared to unadjusted findings,37,107 suggesting that delays may be indicative of the need for extended medical stabilization rather than a direct cause of negative outcomes.
Prospective randomized controlled trials (RCTs) stand as the gold standard to mitigate confounding but pose ethical dilemmas, particularly in intentionally delaying surgery.16 Therefore, it can be noted that the majority of current extensive prospective RCTs primarily contrast groups undergoing surgery at an extremely early stage (eg, surgery within 6–12 hours after admission) with groups undergoing routine surgery (ie, surgery within 24–48 hours after admission), and the chosen timing for delaying surgery appears to be rational. Regarding the inquiry about what constitutes an “unacceptable delay” (for instance, surgery conducted after 48–72 hours), the ability to conduct prospective RCT remains restricted. The limitations in current research methodologies underscore the necessity for future multicenter, large-sample “real-world studies” to yield definitive insights into the most suitable timeframe for surgery in elderly HF patients.
Conclusions and Future Prospects
Elderly HFs pose complex clinical, logistical, and socioeconomic challenges that demand coordinated, multidisciplinary management. Although substantial advances have been made in understanding fracture biology and perioperative care, key opportunities remain to optimize preoperative evaluation and mitigate postoperative morbidity and mortality. Future efforts must focus not only on surgical outcomes but also on preserving functional independence, enhancing quality of life, and alleviating the broader societal costs of HFs.
The optimal timing for HF surgery remains a debated issue, with existing evidence primarily observational and potentially biased. Based on the available evidence, it appears that delays beyond 24 hours may not significantly affect mortality and complications, especially in medically compromised patients, while early intervention might adversely affect those with correctable conditions. Ethical considerations further complicate the establishment of ideal surgical timing through RCT.
This review emphasizes the importance of further research to provide a more comprehensive understanding of what constitutes an optimal delay, rather than adhering to rigid time frames. That is, a balanced approach advocates for early surgery in medically stable patients within 48 hours post-injury, with reasonable delays for frail patients requiring medical stabilization. While early surgery may reduce LOS and certain complications, in medically unstable patients undue haste could increase perioperative risk. Emerging evidence suggests that an intermediate operative window between 24 and 48 hours may strike the best balance, allowing sufficient time for optimization of comorbidities without incurring the delays associated with extended waiting periods. Further investigations should aim to define both the urgency of surgery and the most suitable delay, ensuring that limited medical resources and time are effectively utilized, ultimately enabling patients to recover and reintegrate into social life at the earliest opportunity. The anticipated advancement in technology and research methodology will likely provide deeper insights into this complex issue, paving the way for tailored and effective treatment strategies for elderly HFs.
Abbreviations
HF, hip fracture; ASA, American Society of Anesthesiologists; LOS, length of hospital stay; DVT, deep vein thrombosis; RCT, randomized controlled trial.
Data Sharing Statement
All the data supporting the study findings are within the paper. Additional detailed information is available from the corresponding author (Junfei Guo) on reasonable request.
Acknowledgments
We thank Home for Researchers editorial team (www.home-for-researchers.com) for improving the English language in this paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by the Science and Technology Program of Xi’an, Shaanxi Province (No. 24YXYJ0085), and Postdoctoral Fund of Shaanxi Province (No. 2023BSHGZZHQYXMZZ02). The funders did not have any role in the design of the study and collection, analysis, and interpretation of data and in writing the paper.
Disclosure
The authors confirm that this is an original paper and has not been previously published or submitted to another journal. There are no conflicts of interest related to the study design or its results.
References
1. Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence and mortality of Hip fractures in the United States. JAMA. 2009;302(14):1573–1579. doi:10.1001/jama.2009.1462
2. Søgaard A, Holvik K, Meyer H, et al. Continued decline in Hip fracture incidence in Norway: a NOREPOS study. Osteoporosis Int. 2016;27(7):2217–2222. doi:10.1007/s00198-016-3516-8
3. Patel V, Champaneria R, Dretzke J, Yeung J. Effect of regional versus general anaesthesia on postoperative delirium in elderly patients undergoing surgery for Hip fracture: a systematic review. BMJ Open. 2018;8(12):e020757. doi:10.1136/bmjopen-2017-020757
4. Omari A, Madsen CM, Lauritzen JB, Jørgensen HL, Vojdeman FJ. Comorbidity and mortality after Hip fracture in nineteen thousand six hundred and eighty two patients aged eighteen to sixty five years in Denmark from 1996 to 2012. Int Orthop. 2019;43(11):2621–2627. doi:10.1007/s00264-019-04323-z
5. Guo J, Xu X, Geng Q, et al. Efficacy of surgical intervention over conservative management in intertrochanteric fractures among nonagenarians and centenarians: a prospective cohort study. Int J Surg. 2024;110(5):2708–2720.
6. Guo J, Zhang Y, Hou Z. Intramedullary fixation does not cause a large amount of hidden blood loss in elderly patients with intertrochanteric fractures. Clin Interv Aging. 2021;16:475–486. doi:10.2147/CIA.S301737
7. Haentjens P, Magaziner J, Colón-Emeric CS, et al. Meta-analysis: excess mortality after Hip fracture among older women and men. Ann Intern Med. 2010;152(6):380–390. doi:10.7326/0003-4819-152-6-201003160-00008
8. Sobolev B, Guy P, Sheehan KJ, et al. Time trends in hospital stay after Hip fracture in Canada, 2004-2012: database study. Arch Osteoporos. 2016;11:13. doi:10.1007/s11657-016-0264-5
9. Rapp K, Büchele G, Dreinhöfer K, Bücking B, Becker C, Benzinger P. Epidemiology of Hip fractures: systematic literature review of German data and an overview of the international literature. Z Gerontol Geriatr. 2019;52(1):10–16. doi:10.1007/s00391-018-1382-z
10. Schemitsch EH, Sprague S, Heetveld MJ, et al. Loss of independence after operative management of femoral neck fractures. Journal of Orthopaedic Trauma. 2019;33(6):292–300. doi:10.1097/BOT.0000000000001444
11. Huang YF, Liang J, Shyu YL. Number of comorbidities negatively influence psychological outcomes of the elderly following hip fracture in Taiwan. J Aging Health. 2016;28(8):1343–1361. doi:10.1177/0898264315618922
12. Leal J, Gray AM, Prieto-Alhambra D, et al. Impact of Hip fracture on hospital care costs: a population-based study. Osteoporos Int. 2016;27(2):549–558. doi:10.1007/s00198-015-3277-9
13. Cheung CL, Ang SB, Chadha M, et al. An updated Hip fracture projection in Asia: the Asian Federation of Osteoporosis Societies study. Osteoporos Sarcopenia. 2018;4(1):16–21. doi:10.1016/j.afos.2018.03.003
14. Anthony CA, Duchman KR, Bedard NA, et al. Hip fractures: appropriate timing to operative intervention. J Arthroplasty. 2017;32(11):3314–3318. doi:10.1016/j.arth.2017.07.023
15. Cha YH, Ha YC, Yoo JI, Min YS, Lee YK, Koo KH. Effect of causes of surgical delay on early and late mortality in patients with proximal Hip fracture. Arch Orthop Trauma Surg. 2017;137(5):625–630. doi:10.1007/s00402-017-2674-2
16. Al-Ani AN, Samuelsson B, Tidermark J, et al. Early operation on patients with a Hip fracture improved the ability to return to independent living. A prospective study of 850 patients. The Journal of Bone and Joint Surgery American. 2008;90(7):1436–1442.
17. Orosz GM, Magaziner J, Hannan EL, et al. Association of timing of surgery for Hip fracture and patient outcomes. JAMA. 2004;291(14):1738–1743. doi:10.1001/jama.291.14.1738
18. Siegmeth AW, Gurusamy K, Parker MJ. Delay to surgery prolongs hospital stay in patients with fractures of the proximal femur. The Journal of Bone and Joint Surgery British. 2005;87(8):1123–1126.
19. Simunovic N, Devereaux PJ, Sprague S, et al. Effect of early surgery after Hip fracture on mortality and complications: systematic review and meta-analysis. Cmaj. 2010;182(15):1609–1616. doi:10.1503/cmaj.092220
20. Bretherton CP, Parker MJ. Early surgery for patients with a fracture of the Hip decreases 30-day mortality. Bone Joint J. 2015;97-b(1):104–108. doi:10.1302/0301-620X.97B1.35041
21. Shiga T, Wajima Z, Ohe Y. Is operative delay associated with increased mortality of Hip fracture patients? Systematic review, meta-analysis, and meta-regression. Can J Anaesth. 2008;55(3):146–154. doi:10.1007/BF03016088
22. Hagino T, Ochiai S, Senga S, et al. Efficacy of early surgery and causes of surgical delay in patients with Hip fracture. J Orthop. 2015;12(3):142–146. doi:10.1016/j.jor.2015.01.013
23. White SM, Griffiths R, Holloway J, Shannon A. Anaesthesia for proximal femoral fracture in the UK: first report from the NHS hip fracture anaesthesia network. Anaesthesia. 2010;65(3):243–248. doi:10.1111/j.1365-2044.2009.06208.x
24. George J, Sharma V, Farooque K, Mittal S, Trikha V, Malhotra R. Factors associated with delayed surgery in elderly Hip fractures in India. Arch Osteoporos. 2021;16(1):7. doi:10.1007/s11657-020-00858-6
25. Uzoigwe CE, Burnand HG, Cheesman CL, Aghedo DO, Faizi M, Middleton RG. Early and ultra-early surgery in Hip fracture patients improves survival. Injury. 2013;44(6):726–729. doi:10.1016/j.injury.2012.08.025
26. Hapuarachchi KS, Ahluwalia RS, Bowditch MG. Neck of femur fractures in the over 90s: a select group of patients who require prompt surgical intervention for optimal results. J Orthop Traumatol. 2014;15(1):13–19. doi:10.1007/s10195-013-0248-9
27. Kavak M, Oğuz S, Akkoyun Z, İnan U. Predictive factors associated with thirty-day mortality in geriatric patients with Hip fractures. Acta Orthop Traumatol Turc. 2022;56(4):240–244. doi:10.5152/j.aott.2022.21407
28. Seckel T, Mahoney K, Hewitt C, Liu H, Ang D. Outcomes after definitive surgery for nonagenarians with isolated hip fractures within 24 hours of admission. Am Surg. 2023;89(5):1821–1828. doi:10.1177/00031348211067994
29. Fractured neck of femur. prevention and management. summary and recommendations of a report of the royal college of physicians. J R Coll Physicians Lond. 1989;23(1):8–12.
30. Brox WT, Roberts KC, Taksali S, et al. The American Academy of orthopaedic surgeons evidence-based guideline on management of hip fractures in the elderly. The Journal of Bone and Joint Surgery American. 97;14:1196–1199.
31. Swift C, Ftouh S, Langford P, Chesser TS, Johanssen A. Interdisciplinary management of Hip fracture. Clin Med. 2016;16(6):541–544. doi:10.7861/clinmedicine.16-6-541
32. Sasabuchi Y, Matsui H, Lefor AK, Fushimi K, Yasunaga H. Timing of surgery for Hip fractures in the elderly: a retrospective cohort study. Injury. 2018;49(10):1848–1854. doi:10.1016/j.injury.2018.07.026
33. Sheehan KJ, Sobolev B, Guy P. Mortality by timing of hip fracture surgery: factors and relationships at play. The Journal of Bone and Joint Surgery American. 99(20):e106.
34. Tarrant SM, Kim RG, McGregor KL, Palazzi K, Attia J, Balogh ZJ. Dual antiplatelet therapy and surgical timing in geriatric hip fracture. Journal of Orthopaedic Trauma. 2020;34(10):559–565. doi:10.1097/BOT.0000000000001779
35. Bhandari M, Solomon CG, Swiontkowski M. Management of acute hip fracture. New England Journal of Medicine. 2017;377(21):2053–2062. doi:10.1056/NEJMcp1611090
36. Liu Z, Du Z, Lu H, Fu Z, Xu H. Delay between admission and surgery as a potential risk factor for postoperative morbidity and mortality in elderly patients with Hip fractures: a retrospective study. Journal of Orthopaedic Science: Official Journal of the Japanese Orthopaedic Association. 2023;28(5):1124–1130. doi:10.1016/j.jos.2022.07.010
37. Majumdar SR, Beaupre LA, Johnston DW, Dick DA, Cinats JG, Jiang HX. Lack of association between mortality and timing of surgical fixation in elderly patients with Hip fracture: results of a retrospective population-based cohort study. Medical Care. 2006;44(6):552–559. doi:10.1097/01.mlr.0000215812.13720.2e
38. Smektala R, Endres HG, Dasch B, et al. The effect of time-to-surgery on outcome in elderly patients with proximal femoral fractures. BMC Musculoskelet Disord. 2008;9:171. doi:10.1186/1471-2474-9-171
39. Moran CG, Wenn RT, Sikand M, Taylor AM. Early mortality after Hip fracture: is delay before surgery important? The Journal of Bone and Joint Surgery American Volume. 2005;87(3):483–489. doi:10.2106/JBJS.D.01796
40. Wenk M, Frey S. Elderly Hip fracture patients: surgical timing and factors to consider. Curr Opin Anaesthesiol. 34(1):33–39. doi:10.1097/ACO.0000000000000941.
41. Seong YJ, Shin WC, Moon NH, Suh KT. Timing of hip-fracture surgery in elderly patients: literature review and recommendations. Hip & Pelvis. 2020;32(1):11–16. doi:10.5371/hp.2020.32.1.11
42. Ventura C, Trombetti S, Pioli G, Belotti LM, De Palma R. Impact of multidisciplinary Hip fracture program on timing of surgery in elderly patients. Osteoporos Int. 2014;25(11):2591–2597. doi:10.1007/s00198-014-2803-5
43. Vidán MT, Sánchez E, Gracia Y, Marañón E, Vaquero J, Serra JA. Causes and effects of surgical delay in patients with Hip fracture: a cohort study. Ann Intern Med. 2011;155(4):226–233. doi:10.7326/0003-4819-155-4-201108160-00006
44. Ricci WM, Brandt A, McAndrew C, Gardner MJ. Factors affecting delay to surgery and length of stay for patients with Hip fracture. Journal of Orthopaedic Trauma. 2015;29(3):e109–14. doi:10.1097/BOT.0000000000000221
45. Hershkovitz A, Polatov I, Beloosesky Y, Brill S. Factors affecting mortality of frail Hip-fractured elderly patients. Arch Gerontol Geriatr. 2010;51(2):113–116. doi:10.1016/j.archger.2009.09.003
46. Ali I, Vattigunta S, Jang JM, et al. Racial disparities are present in the timing of radiographic assessment and surgical treatment of hip fractures. Clinical Orthopaedics and Related Research. 2020;478(3):455–461. doi:10.1097/CORR.0000000000001091
47. Gitajn IL, Werth P, Fernandes E, et al. Association of patient-level and hospital-level factors with timely fracture care by race. JAMA Netw Open. 2022;5(11):e2244357. doi:10.1001/jamanetworkopen.2022.44357
48. Ashouri F, Al-Jundi W, Patel A, Mangwani J. Management of warfarin anticoagulation in patients with fractured neck of femur. ISRN Hematol. 2011;2011:294628. doi:10.5402/2011/294628
49. Starks I, Cooke S, Docker C, Raine A. Warfarinized patients with proximal femoral fractures: survey of UK clinical practice. Eur J Trauma Emerg Surg. 2009;35(3):287. doi:10.1007/s00068-008-8070-4
50. Green L, Bolton-Maggs P, Beattie C, et al. British society of haematology guidelines on the spectrum of fresh frozen plasma and cryoprecipitate products: their handling and use in various patient groups in the absence of major bleeding. Br J Haematol. 2018;181:54–67. doi:10.1111/bjh.15167
51. National Institute for Health and Clinical Excellence (NICE). Hip Fracture: Evidence Update March 2013: A Summary of Selected New Evidence Relevant to NICE Clinical Guideline 124 “The Management of Hip Fracture in Adults” 2011. London: National Institute for Health and Clinical Excellence (NICE) National Institute for Health and Clinical Excellence; 2013.
52. Steiner T, Poli S, Griebe M, et al. Fresh frozen plasma versus prothrombin complex concentrate in patients with intracranial haemorrhage related to vitamin K antagonists (INCH): a randomised trial. Lancet Neurol. 2016;15(6):566–573. doi:10.1016/S1474-4422(16)00110-1
53. Meinig R, Jarvis S, Orlando A, et al. Is anticoagulation reversal necessary prior to surgical treatment of geriatric Hip fractures? J Clin Orthop Trauma. 2020;11(Suppl 1):S93–s99. doi:10.1016/j.jcot.2019.10.004
54. Dahlberg S, Schött U, Kander T. The effect of vitamin K on prothrombin time in critically ill patients: an observational registry study. J Intensive Care. 2021;9(1):11. doi:10.1186/s40560-020-00517-5
55. Levack AE, Moore HG, Stephan SR, et al. Chronic warfarin anticoagulation in hip fracture patients delays surgery and is associated with increased risk of postoperative complications: a multicenter propensity-score-matched analysis. Journal of Orthopaedic Trauma. 2023;37(2):57–63. doi:10.1097/BOT.0000000000002484
56. Horlocker TT, Vandermeuelen E, Kopp SL, Gogarten W, Leffert LR, Benzon HT. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American society of regional anesthesia and pain medicine evidence-based guidelines. Reg Anesth Pain Med. 2018;43(3):263–309. doi:10.1097/AAP.0000000000000763
57. Rudasill SE, Liu J, Kamath AF. Revisiting the international normalized ratio threshold for bleeding risk and mortality in primary total hip arthroplasty: a national surgical quality improvement program analysis of 17,567 patients. The Journal of Bone and Joint Surgery American Volume. 2020;102(1):52–59. doi:10.2106/JBJS.19.00160
58. Tamim H, Habbal M, Saliba A, et al. Preoperative INR and postoperative major bleeding and mortality: a retrospective cohort study. J Thromb Thrombolysis. 2016;41(2):301–311. doi:10.1007/s11239-015-1235-1
59. Bernate JD, López AM, Rojas Liévano J, et al. Preoperative anticoagulation and its impact on surgical timing and postoperative outcomes in hip fracture surgery: a retrospective study at an orthogeriatrics clinical care center in Colombia. Eur J Orthop Surg Traumatol. 2025;35(1):170. doi:10.1007/s00590-025-04286-5
60. Yassa R, Khalfaoui MY, Hujazi I, Sevenoaks H, Dunkow P. Management of anticoagulation in Hip fractures: a pragmatic approach. EFORT Open Reviews. 2017;2(9):394–402. doi:10.1302/2058-5241.2.160083
61. Grandone E, Ostuni A, Tiscia GL, Marongiu F, Barcellona D. Management of patients taking oral anticoagulants who need urgent surgery for hip fracture. Semin Thromb Hemost. 2019;45(2):164–170. doi:10.1055/s-0039-1678718
62. Danford NC, Logue TC, Boddapati V, Mjj A, Fl A, Rosenwasser MP. Debate update: surgery after 48 hours of admission for geriatric hip fracture patients is associated with increase in mortality and complication rate: a study of 27,058 patients using the national trauma data bank. Journal of Orthopaedic Trauma. 2021;35(10):535–541. doi:10.1097/BOT.0000000000002075
63. Pincus D, Ravi B, Wasserstein D, et al. Association between wait time and 30-day mortality in adults undergoing hip fracture surgery. JAMA. 2017;318(20):1994–2003. doi:10.1001/jama.2017.17606
64. Chang W, Lv H, Feng C, et al. Preventable risk factors of mortality after Hip fracture surgery: systematic review and meta-analysis. Int J Surg. 2018;52:320–328. doi:10.1016/j.ijsu.2018.02.061
65. Borges FK, Bhandari M, Guerra-Farfan E. Accelerated surgery versus standard care in Hip fracture (HIP ATTACK): an international, randomised, controlled trial. Lancet. 2020;395(10225):698–708. doi:10.1016/S0140-6736(20)30058-1
66. Yaacobi E, Marom O, Gutman N, Zabarqa S, Brin Y, Ohana N. Mortality following surgery for geriatric Hip fractures: is it the timing or the co-morbidities? Hip Int. 2022;32(2):271–275. doi:10.1177/1120700020945942
67. Klestil T, Röder C, Stotter C, et al. Impact of timing of surgery in elderly Hip fracture patients: a systematic review and meta-analysis. Sci Rep. 2018;8(1):13933. doi:10.1038/s41598-018-32098-7
68. Kanthasamy S, To K, Webb JI, Elbashir M, Parker MJ. Timing of surgery for internal fixation of intracapsular Hip fractures and complications at 1 year; a 32 year clinical study of 2,366 patients at a single center. Injury. 2022;53(2):584–589. doi:10.1016/j.injury.2021.11.038
69. Shani M, Yahalom R, Comaneshter D, et al. Should patients treated with oral anti-coagulants be operated on within 48 h of Hip fracture? J Thromb Thrombolysis. 2021;51(4):1132–1137. doi:10.1007/s11239-020-02261-x
70. Lizaur-Utrilla A, Martinez-Mendez D, Collados-Maestre I, Miralles-Muñoz FA, Marco-Gomez L, Lopez-Prats FA. Early surgery within 2 days for Hip fracture is not reliable as healthcare quality indicator. Injury. 2016;47(7):1530–1535. doi:10.1016/j.injury.2016.04.040
71. Vitiello R, Pesare E, Capece G, et al. Surgical timing and clinical factor predicting in-hospital mortality in older adults with Hip fractures: a neuronal network analysis. J Orthop Traumatol. 2025;26(1):30. doi:10.1186/s10195-025-00846-x
72. De Luca A, Murena L, Zanetti M, De Colle P, Ratti C, Canton G. Should the early surgery threshold be moved to 72 h in over-85 patients with Hip fracture? A single-center retrospective evaluation on 941 patients. Arch Orthop Trauma Surg. 2023;143(6):3091–3101. doi:10.1007/s00402-022-04509-y
73. Schermann H, Ashkenazi I, Graif N, et al. Would giving priority in surgery timing to the oldest patients result in lower mortality? Int Orthop. 2022;46(8):1701–1706. doi:10.1007/s00264-022-05466-2
74. Sexson SB, Lehner JT. Factors affecting Hip fracture mortality. Journal of Orthopaedic Trauma. 1987;1(4):298–305. doi:10.1097/00005131-198701040-00005
75. Bredahl C, Nyholm B, Hindsholm KB, Mortensen JS, Olesen AS. Mortality after Hip fracture: results of operation within 12 h of admission. Injury. 1992;23(2):83–86. doi:10.1016/0020-1383(92)90037-S
76. Zuckerman JD, Skovron ML, Koval KJ, Aharonoff G, Frankel VH. Postoperative complications and mortality associated with operative delay in older patients who have a fracture of the Hip. The Journal of Bone and Joint Surgery American Volume. 1995;77(10):1551–1556. doi:10.2106/00004623-199510000-00010
77. Khan SK, Kalra S, Khanna A, Thiruvengada MM, Parker MJ. Timing of surgery for Hip fractures: a systematic review of 52 published studies involving 291,413 patients. Injury. 2009;40(7):692–697. doi:10.1016/j.injury.2009.01.010
78. Kenzora JE, McCarthy RE, Lowell JD, Sledge CB. Hip fracture mortality. Relation to age, treatment, preoperative illness, time of surgery, and complications. Clinical Orthopaedics and Related Research. 1984;186:45–56. doi:10.1097/00003086-198406000-00008
79. Griffiths R, Alper J, Beckingsale A, et al. Management of proximal femoral fractures 2011: association of anaesthetists of Great Britain and Ireland. Anaesthesia. 2012;67(1):85–98. doi:10.1111/j.1365-2044.2011.06957.x
80. Weller I, Wai EK, Jaglal S, Kreder HJ. The effect of hospital type and surgical delay on mortality after surgery for Hip fracture. The Journal of Bone and Joint Surgery British. 2005;87(3):361–366.
81. Bergeron E, Lavoie A, Moore L, et al. Is the delay to surgery for isolated Hip fracture predictive of outcome in efficient systems? The Journal of Trauma. 2006;60(4):753–757. doi:10.1097/01.ta.0000214649.53190.2a
82. Haleem S, Heinert G, Parker MJ. Pressure sores and Hip fractures. Injury. 2008;39(2):219–223. doi:10.1016/j.injury.2007.08.030
83. Sun L, Wang C, Zhang M, Li X, Zhao B. The surgical timing and prognoses of elderly patients with hip fractures: a retrospective analysis. Clin Interv Aging. 2023;18:891–899. doi:10.2147/CIA.S408903
84. Shin WC, Woo SH, Sj L, Kim C, Suh KT, Suh KT. Preoperative prevalence of and risk factors for venous thromboembolism in patients with a hip fracture: an indirect multidetector CT venography study. The Journal of Bone and Joint Surgery American Volume. 2016;98(24):2089–2095. doi:10.2106/JBJS.15.01329
85. Whinney CM. Do Hip fractures need to be repaired within 24 hours of injury? Cleve Clin J Med. 2005;72(3):250–252. doi:10.3949/ccjm.72.3.250
86. Pioli G, Bendini C, Giusti A, et al. Surgical delay is a risk factor of delirium in Hip fracture patients with mild-moderate cognitive impairment. Aging Clin Exp Res. 2019;31(1):41–47. doi:10.1007/s40520-018-0985-y
87. Panth S, Wilson E, Chen B, Clement ND. Accelerated care of patients with hip fractures is associated with lower risk of delirium and infection, and a shorter length of hospital stay: systematic review and meta-analysis of level one evidence. Indian J Orthop. 2024;58(1):1–10. doi:10.1007/s43465-023-01026-x
88. Accelerated care versus standard care among patients with Hip fracture: the HIP ATTACK pilot trial. Cmaj. 2014;186(1):E52–60. doi:10.1503/cmaj.130901
89. Kawakami H, Sasaki H, Kamizono J, Yasutake Y, Fujimoto Y, Taniguchi N. Timely surgical intervention for hip fractures is essential to reinstate ambulatory function on discharge: propensity score matching. JB JS Open Access. 2025;10(1). doi:10.2106/JBJS.OA.24.00037
90. Cai Q, Fu K, Jia W, et al. In-hospital waiting time to surgery and functional outcomes in geriatric Hip fractures: a directed acyclic graph-based preplanned analysis from a prospective multicenter cohort study. Int J Surg. 2023;109(6):1612–1619. doi:10.1097/JS9.0000000000000385
91. Cree AK, Nade S. How to predict return to the community after fractured proximal femur in the elderly. Aust N Z J Surg. 1999;69(10):723–725. doi:10.1046/j.1440-1622.1999.01673.x
92. Doruk H, Mas MR, Yildiz C, Sonmez A, Kýrdemir V. The effect of the timing of Hip fracture surgery on the activity of daily living and mortality in elderly. Arch Gerontol Geriatr. 2004;39(2):179–185. doi:10.1016/j.archger.2004.03.004
93. Lefaivre KA, Macadam SA, Davidson DJ, Gandhi R, Chan H, Broekhuyse HM. Length of stay, mortality, morbidity and delay to surgery in Hip fractures. The Journal of Bone and Joint Surgery British. 2009;91(7):922–927.
94. Guo J, Di J, Gao X, et al. Discriminative ability for adverse outcomes after hip fracture surgery: a comparison of three commonly used comorbidity-based indices. Gerontology. 2021;23:1–13.
95. Kim B, Lee J, Park S, et al. Elevated ceramides 18:0 and 24:1 with aging are associated with Hip fracture risk through increased bone resorption. Aging. 2019;11(21):9388–9404. doi:10.18632/aging.102389
96. Anthony C, Malaj M, Lokanathan P, Murgatroyd J, O’Connor P. Crossing quartiles: improving time to theatre for patients with Hip fractures in a large UK district general hospital; A quality improvement report. Injury. 2021;52(11):3415–3419. doi:10.1016/j.injury.2021.08.015
97. Sura-Amonrattana U, Tharmviboonsri T, Unnanuntana A, Tantigate D, Srinonprasert V. Evaluation of the implementation of multidisciplinary fast-track program for acute geriatric Hip fractures at a University Hospital in resource-limited settings. BMC Geriatr. 2021;21(1):548. doi:10.1186/s12877-021-02509-y
98. Walsh ME, Cunningham C, Brent L, Savin B, Fitzgerald M, Blake C. Long-term outcome collection after Hip fracture in Ireland: a systematic review of traditional and grey literature. Osteoporos Int. 2023;34(7):1179–1191.
99. Guo J, Ye P, Zhang Q, et al. Is there a “weekend effect” in intertrochanteric fracture surgery? Gerontology. 2021;9:1–12.
100. Kristiansen N, Kristensen P, Nørgård B, Mainz J, Johnsen S. Off-hours admission and quality of Hip fracture care: a nationwide cohort study of performance measures and 30-day mortality. Int J Qual Health Care. 2016;28(3):324–331. doi:10.1093/intqhc/mzw037
101. Thomas CJ, Smith RP, Uzoigwe CE, Braybrooke JR. The weekend effect: short-term mortality following admission with a Hip fracture. Bone Joint J. 2014;96(3):373–378. doi:10.1302/0301-620X.96B3.33118
102. Zhou Y, Li W, Herath C, et al. Off-hour admission and mortality risk for 28 specific diseases: a systematic review and meta-analysis of 251 cohorts. Journal of the American Heart Association. 2016;5(3):e003102. doi:10.1161/JAHA.115.003102
103. Rashid RH, Zubairi AJ, Slote MU, Noordin S. Hip fracture surgery: does time of the day matter? A case-controlled study. Int J Surg. 2013;11(9):923–925. doi:10.1016/j.ijsu.2013.07.003
104. Colais P, Pinnarelli L, Fusco D, Davoli M, Braga M, Perucci CA. The impact of a pay-for-performance system on timing to Hip fracture surgery: experience from the Lazio Region (Italy). BMC Health Serv Res. 2013;13:393. doi:10.1186/1472-6963-13-393
105. Borges FK, Bhandari M, Patel A, et al. Rationale and design of the Hip fracture Accelerated surgical TreaTment And Care tracK (HIP ATTACK) Trial: a protocol for an international randomised controlled trial evaluating early surgery for hip fracture patients. BMJ Open. 2019;9(4):e028537. doi:10.1136/bmjopen-2018-028537
106. Runner R, Moore T, Reisman W. Value of a dedicated Saturday orthopaedic trauma operating room. Journal of Orthopaedic Trauma. 2016;30(1):e24–9. doi:10.1097/BOT.0000000000000441
107. Rae HC, Harris IA, McEvoy L, Todorova T. Delay to surgery and mortality after Hip fracture. ANZ J Surg. 2007;77(10):889–891. doi:10.1111/j.1445-2197.2007.04267.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.