")
Back to Journals » Journal of Asthma and Allergy » Volume 18
Advances in Understanding Recurrent Pulmonary Infections Following Foreign Body Aspiration: A Narrative Review
Authors Tang Q, Chen X, Ran K, Yang X, Yuan T, Li J, Zheng J, Xu C , Li H, Zhao Y, Wang J
Received 25 February 2025
Accepted for publication 10 July 2025
Published 15 July 2025 Volume 2025:18 Pages 1093—1103
DOI https://doi.org/10.2147/JAA.S524781
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Qian Tang,1,* Xing Chen,2,3,* Kunjie Ran,4 Xueqin Yang,1 Ting Yuan,1 Juanjuan Li,1 Juan Zheng,1 Chen Xu,1 Heping Li,1 Yang Zhao,1 Jingsong Wang1
1Department of Pharmacy, Guangyuan Central Hospital, Guangyuan, Sichuan, People’s Republic of China; 2School of Stomatology, North Sichuan Medical College, Nanchong, Sichuan, People’s Republic of China; 3Department of Stomatology, Guangyuan Central Hospital, Guangyuan, Sichuan, People’s Republic of China; 4Department of Pharmacy, The First People’s Hospital of Guangyuan, Guangyuan, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jingsong Wang, Department of Pharmacy, Guangyuan Central Hospital, Guangyuan, Sichuan, People’s Republic of China, Email [email protected] Yang Zhao, Department of Pharmacy, Guangyuan Central Hospital, Guangyuan, Sichuan, People’s Republic of China, Email [email protected]
Abstract: Recurrent pulmonary infections (RPIs) represent a common yet clinically complex entity, primarily triggered by aspiration or the presence of foreign bodies. They are notoriously insidious and challenging to detect clinically. These infections typically involve the invasion of bacteria, viruses, or fungi, leading to inflammation and damage of lung tissue. The development of RPIs may also arise from the interplay of multiple factors. Due to their inherent complexity and association with poor prognosis, RPIs constitute a significant cause of mortality stemming from pulmonary infections. Understanding the risk factors associated with RPIs secondary to foreign body aspiration is crucial for effective clinical management. This narrative review synthesizes current knowledge on the pathogenesis, diagnosis, management, and prevention of RPIs caused by foreign body aspiration. We emphasize the heightened vulnerability of pediatric and elderly populations. The review delineates characteristic clinical presentations and outlines appropriate diagnostic modalities. Furthermore, it provides perspectives on antimicrobial therapy and the critical importance of foreign body removal. The synthesis aims to inform future research directions, preventive strategies, and therapeutic approaches, ultimately seeking to improve patient outcomes and mitigate the risk of recurrent infections.
Keywords: foreign body aspiration, pulmonary infection, recurrence, diagnosis and treatment, prevention
Introduction
Pneumonia has persisted as a leading global cause of mortality for decades.1,2 According to the Global Burden of Disease Report 2021, pneumonia caused 2.1 million deaths between 1990–2021, predominantly affecting children under 5 years and adults over 70 years.3 Foreign body aspiration represents a significant etiological contributor to pneumonia, particularly prevalent in these age groups.4,5 The aspirated foreign body, due to its highly concealed nature and tendency to evade detection during examinations, leading to prolonged pulmonary retention,6,7 predispose to infections such as bacterial, viral, or fungal pathogens,8 and failure to promptly diagnose and remove the foreign body often precipitates recurrent pulmonary infections (RPIs), severe complications, and mortality,9,10 imposing substantial societal and familial burdens.11
RPIs (typically defined as ≥2 episodes within 1 year or ≥3 episodes at any time) may arise from diverse etiologies, with foreign body aspiration representing a significant and modifiable cause, particularly prevalent in children.5 Furthermore, migration of foreign bodies,12 aspiration secondary to gastroesophageal reflux,13,14 and unreported/unrecognized aspiration history (due to patient amnesia or communication barriers),15 constitute key risk factors for recurrent infections. These and other aspiration-related risk factors collectively predispose to RPIs. Additionally, elderly patients with neurological disorders (Parkinson’s disease, Alzheimer’s disease, etc.) exhibit heightened susceptibility due to dysphagia-induced aspiration, wherein delayed recognition severely compromises quality of life.16 Critically, prompt diagnosis and complete foreign body removal are pivotal for terminating infection recurrence and preventing complications.
This review aims to synthesize the clinical features, diagnosis, management, and prevention strategies for aspiration-induced RPIs, with focused attention on pediatric and elderly populations with comorbidities. By elucidating population-specific risk factors, emphasizing optimized utilization of imaging and bronchoscopy for enhanced foreign body detection, and underscoring the imperative of foreign body extraction, alongside discussion of preventive measures, this work seeks to elevate clinical awareness. Ultimately, we aspire to improve diagnostic rates and cure efficacy, thereby reducing infection recurrence, ameliorating patient prognosis, and lowering associated mortality and disease burden. Concurrently, this review endeavors to provide insights for refining early identification, precision interventions, and long-term management in high-risk individuals.
Recurrent Pulmonary Infections
Clinical Characteristics
RPIs from foreign body aspiration manifest clinically with recurrent cough, dyspnea, wheezing, and fever.8 Auscultation reveals tracheal slapping sounds, wheezes, and unilateral diminished or absent breath sounds.17 Imaging demonstrates recurrent consolidation in identical lung segments, mediastinal shift, atelectasis, hyperinflation, or obstructive pneumonia with air-trapping.18,19 Pediatric patients may additionally exhibit failure to thrive, thoracic deformities, and digital clubbing.17,20
Reasons
Failure to promptly detect aspirated foreign bodies leads to their prolonged retention in the lungs, ultimately causing RPIs.6,15 RPIs from occult aspiration often lack documented aspiration history and are most prevalent in children.21–24Their underdeveloped chewing function and cough reflex typically prevent spontaneous expulsion of aspirated objects.25,26 In elderly patients, neurological disorders (including epilepsy, Parkinson’s disease and stroke),27–31 impair swallowing and cough efficacy, allowing retained foreign bodies and pathogens to persistently irritate lung tissue.10,32–34 Repeated aspirations particularly predispose to recurrent infections.35–42
Aspiration during altered states of consciousness (such as shock, general anesthesia and intoxication) also lacks witnessed history, foreign bodies are only discovered upon recurrent infection episodes.43 Certain medications and anatomical abnormalities further increase aspiration risk. Pharmacological contributors include sedative-hypnotics, anticholinergics, antipsychotics, and anxiolytics.44 Structural or physiological esophageal alterations—such as systemic sclerosis and tracheoesophageal fistulae—constitute additional risk factors.45 Moreover, patients with nasogastric/nasointestinal tubes or tracheal intubation/tracheostomy may experience pulmonary inoculation via spillage of gastroesophageal contents,46 or aspiration of oropharyngeal colonizing pathogens.47,48
During bronchoscopy, migrated foreign bodies may evade detection, while pathogen-laden objects can disseminate to other lung regions, triggering recurrent infections.49–51 Additionally, non-metallic inorganic or small foreign bodies often elude radiographic identification, permitting prolonged airway retention with persistent pulmonary irritation and inflammation.52 Meanwhile, objects obscured by granulation tissue, mucus, or purulent exudate also complicate detection.53 Although antimicrobial therapy may temporarily alleviate symptoms during exacerbations, discontinuation permits pathogen resurgence and infection recurrence unless the foreign body is removed.21,54,55
Pathogenesis
The pathogenesis of RPIs secondary to foreign body aspiration involves multiple interconnected mechanisms. Microbial colonization and infection constitute a primary pathway: aspirated foreign bodies provide niches for bacterial, viral, or fungal adherence and proliferation, directly inciting pulmonary infection.8,16 Repeated aspiration episodes further introduce oropharyngeal colonizing flora into the lower respiratory tract, exacerbating established infections.46 Host inflammatory responses represent a second critical axis: prolonged foreign body retention triggers sustained inflammation with elevated proinflammatory cytokines (including IL-6, IL-1β, TNF-α).56 Chronic inflammation subsequently promotes granulomatous tissue formation, progressively obstructing airways.57 Airway barrier disruption completes a self-perpetuating cycle: mechanical obstruction by foreign bodies or granulomas causes regional hypoventilation and mucosal injury. This impairs mucociliary clearance and increases susceptibility to further aspiration, establishing a vicious cycle of “Foreign body-Pulmonary infection-Inflammation-Barrier compromise”. Cumulatively, these processes drive progressive lung dysfunction and endobronchial complications (Figure 1).6,8,18,25,58
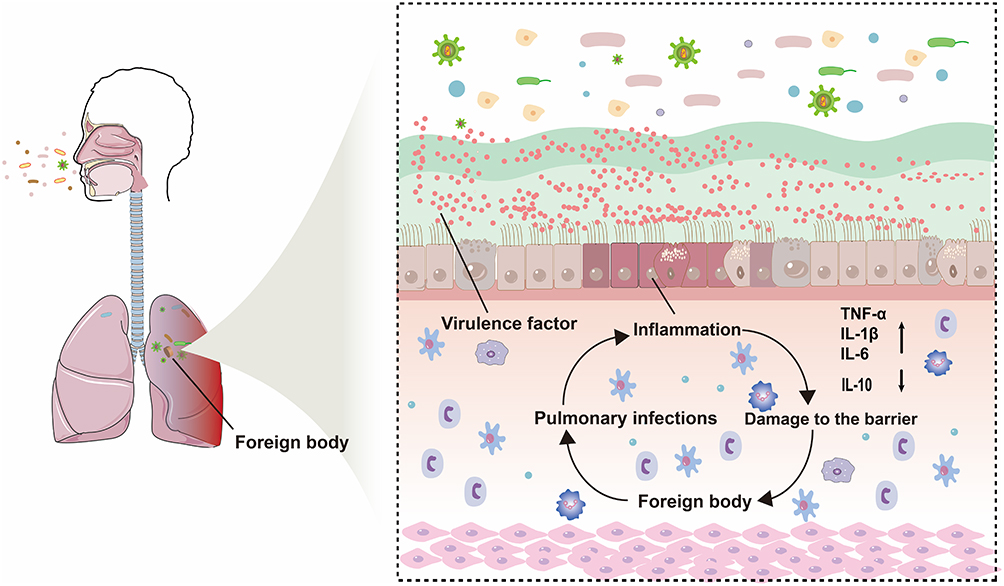 |
Figure 1 Recurrent pulmonary infections caused by foreign body aspiration. |
Diagnosis
Clinical Assessment
Preliminary diagnosis of RPIs triggered by foreign body aspiration relies heavily on thorough clinical assessment, encompassing history taking, symptom analysis, and critical physical examination. Meticulous inquiry into aspiration history, even suspected or remote episodes, is essential.15 Concurrent evaluation for underlying conditions—such as gastroesophageal reflux, neurological disorders (cerebral palsy and post-stroke sequelae), swallowing dysfunction, and structural or functional esophageal abnormalities (achalasia and hiatal hernia, etc).—is imperative, as these factors significantly elevate the risk of foreign body aspiration and recurrent infections.10,59
Recurrent respiratory symptoms constitute core indicators, including persistent or recurrent cough (particularly irritative choking cough), sputum production, dyspnea manifestations (such as tachypnea and wheezing), and systemic symptoms like fever.15,60,61 Additionally, recurrent or persistent symptoms, along with symptom correlation with feeding/posture, provide crucial diagnostic clues.62
Physical examination, equally vital as history, is pivotal for clinical diagnosis.17,63 Auscultation may reveal focal, persistent, or recurrent abnormal breath sounds—such as wheezes, crackles (dry or moist rales), or diminished breath sounds—especially in specific lobes/segments.17 Percussion may demonstrate dullness or hyperresonance.64 Children may exhibit signs of respiratory distress, including inspiratory retractions and perioral cyanosis.65,66 These signs facilitate rapid lesion localization and severity assessment by clinicians.
Comprehensive analysis of clinical assessment (history, symptoms, and physical examination) not only suggests possible RPIs due to foreign body aspiration but also aids in identifying high-risk patients and guiding subsequent investigative selection.
Core Diagnostic Investigations
When clinical assessment strongly suggests RPIs secondary to foreign body aspiration, radiographic imaging and bronchoscopy serve as primary diagnostic tools (Table 1).
 |
Table 1 Comparison of Different Examination Methods |
Chest radiography is typically the initial imaging modality, potentially revealing parenchymal infiltrates, atelectasis, hyperinflation, mediastinal shift, or directly visualizing radiopaque foreign bodies.15,60 However, its sensitivity and specificity are suboptimal, especially for radiolucent foreign bodies or small lesions.67 Crucially, negative results cannot exclude the diagnosis. Chest computed tomography (CT) constitutes the most reliable imaging method for diagnosing foreign body aspiration and evaluating complications, including recurrent pneumonia, lung abscess, and bronchiectasis.68,71–74 Furthermore, high-resolution CT precisely localizes infectious foci, quantifies lung damage (including inflammation, consolidation, emphysema, bronchiectasis), and detects most foreign bodies (including some radiopaque types), proving particularly valuable in chronic or recurrent cases. Limitations include higher radiation exposure than radiography, elevated cost, and potential missed diagnoses of certain foreign bodies (minute or vegetable matter) or locations.74,77–79
Bronchoscopy remains the gold standard for diagnosing and treating endobronchial foreign bodies.15,54 It enables direct airway visualization, confirming the presence, location, and nature of foreign bodies under direct vision—a capability unmatched by other modalities. Bronchoscopy is strongly recommended for patients with high clinical suspicion but negative CT findings.15,54 Simultaneously, it permits therapeutic foreign body extraction, constituting definitive etiological management.80 Direct visualization also facilitates collection of deep airway secretions or bronchoalveolar lavage fluid (BALF) for microbiological culture and cytological analysis, enhancing pathogen detection rates.10,75
Ancillary Diagnostic Investigations
Certain laboratory tests provide supportive information for infection status assessment but cannot independently confirm foreign body presence. Complete blood count may reveal elevated white blood cell count, neutrophil percentage, C-reactive protein (CRP), and procalcitonin (PCT), indicating bacterial infection and inflammatory response, thereby aiding in evaluating infection severity and activity.60 However, these hematological parameters lack specificity, as abnormalities occur across infectious diseases. Conversely, culturing, smearing, and molecular testing of sputum or BALF aim to identify causative pathogens and their antibiotic susceptibility, guiding antimicrobial therapy.81 Positive results require clinical correlation to distinguish colonization from true pathogens.
Cost-Effectiveness Considerations
Selecting the optimal diagnostic pathway necessitates balancing diagnostic efficacy, invasiveness, risk, and cost. Initial judgment based on clinical symptoms, signs, and risk factors helps avoid excessive testing. Due to its high sensitivity, chest CT has become the preferred imaging modality for suspected RPIs from foreign body aspiration, effectively evaluating pulmonary lesions and detecting most foreign bodies.74,77–79 Conventional chest radiography offers limited value owing to low sensitivity but retains utility in specific scenarios (emergency screening) because of its accessibility and low cost.15,60,67 Fluoroscopy provides limited information with operator-dependent variability and non-negligible radiation exposure.82
For patients with RPIs and clinical/CT findings suggestive of foreign bodies, diagnostic bronchoscopy is the definitive step for confirmation and cure. Even with negative CT, bronchoscopy should be actively considered if clinical suspicion remains high (classic history + signs).15,83 Although costly, it addresses the fundamental need for foreign body removal, preventing subsequent recurrent infections and associated expenses. A “low-dose chest CT followed by bronchoscopy when indicated” strategy demonstrates favorable cost-effectiveness.84
Treatments
General Treatments
Maintaining airway patency is essential, and the decision to administer oxygen therapy should be based on the severity of dyspnea.85 It is also essential to monitor the patient’s vital signs, including continuous assessment of oxygen saturation, heart rate, blood pressure, electrolyte balance, internal environment status, and the function of other vital organs, while providing timely symptomatic management.1
Anti-Infection Treatments
The pathogenic bacteria associated with RPIs caused by foreign body aspiration are related to the site of infection. Therefore, the selection of empirical antimicrobial therapy should be based on the common pathogens in community-acquired pneumonia (CAP) and hospital-acquired pneumonia (HAP), as well as the local microbial epidemiology and resistance patterns.86
Common pathogenic bacteria in CAP include Streptococcus pneumoniae, Staphylococcus aureus, Haemophilus influenzae, and Pseudomonas aeruginosa.17,46,87–90 Some patients may present with viral infections or a combination of viral and bacterial infections, with the most frequently identified viruses being rhinoviruses, adenoviruses, respiratory syncytial virus, influenza A viruses, and coronaviruses. Symptomatic supportive treatment is primarily employed for viral infections, without the standalone use of antimicrobial agents.2,91 For bacterial infections, antimicrobial treatment can be guided by the common pathogenic bacteria, selecting β-lactams such as amoxicillin-clavulanate, fluoroquinolones like levofloxacin, and macrolides such as azithromycin.43,92
For complicated infections, empirical combination therapy with two agents may be chosen, including β-lactams plus fluoroquinolones or aminoglycosides.93 In cases where bacterial cultures yield multidrug-resistant organisms, treatment options based on susceptibility results may include piperacillin-tazobactam, cefepime, carbapenems, linezolid, or vancomycin.94
Routine treatment with anti-anaerobic agents is not recommended for either CAP or HAP. However, when patients present with oral diseases, empyema, or pulmonary abscesses, clindamycin or metronidazole may be administered to cover anaerobic bacteria.1,46,93,94
In conclusion, for pulmonary infections resulting from foreign body aspiration, empirical antimicrobial therapy should aim to cover both Gram-negative and Gram-positive bacteria, with targeted therapy adjusted following the results of cultures and susceptibility tests.
Remove Foreign Body
Timely Imaging examinations can detect and localize pulmonary foreign bodies, while bronchoscopy is the primary method for managing foreign bodies, facilitating their timely identification and removal, thus reducing the recurrence infections of pulmonary.68 Bronchoscopes are classified into rigid and flexible types, and there is ongoing debate regarding which is preferable.95 Rigid bronchoscopy may be chosen for patients with unstable respiration, significant bleeding, or foreign bodies located in the central airways.96,97 Flexible bronchoscopy is suitable for children, patients requiring repeated procedures, or those with foreign bodies in peripheral airways.98–101 The choice of bronchoscope should consider the location, size of the foreign body, and tracheal diameter preoperatively.102,103 Additionally, if a flexible bronchoscope fails to retrieve a foreign body, it may be used in conjunction with a rigid bronchoscope.104 During bronchoscopy, to prevent fail to pinpoint in diagnosis due to granulation tissue or purulent secretions enveloping the foreign body, saline can be used for repeated irrigation, or local adrenaline may be applied. If necessary, preemptive anti-infective treatment or corticosteroids can be administered to mitigate inflammation before re-evaluating with bronchoscopy.54,100,105 Following the removal of pulmonary foreign bodies, early bronchoalveolar lavage can promote the absorption and resolution of pulmonary inflammation.106 Surgical foreign body removal may be indicated when objects are excessively large, or when bronchoscopy is contraindicated (due to bronchiectasis/abscess) or has failed.107
Treatment of Underlying Conditions
Timely treatment for RPIs induced by different types of foreign body aspiration is crucial. Active management of underlying conditions is recommended, such as using medications to suppress gastroesophageal reflux in affected patients.13,108 For patients with neurological disorders leading to swallowing difficulties, such as stroke, epilepsy, and Parkinson’s disease, proactive rehabilitation exercises should be encouraged.109,110 Patients with oral diseases should receive appropriate treatment and maintain regular oral hygiene.111–113
Other Treatments
The use of corticosteroids for treating pulmonary infections caused by foreign body aspiration remains controversial and is not routinely recommended. They should only be used when deemed necessary, such as nebulized budesonide for alleviating airway inflammatory response. And requiring comprehensive consideration of clinical manifestations, number of affected lobes, extent/density of consolidation, CRP and LDH levels, alongside daily efficacy assessment.93,114,115
Prevention
For infants and young children, this age group represents the highest-risk population for foreign body aspiration, necessitating targeted preventive measures. Firstly, primary interventions focus on optimizing feeding techniques: maintain infants/toddlers in a semi-upright position (approximately 30–45 degrees) during feeding, avoiding supine positioning for milk or meals. Secondly, adapt feeding methods by using nipples with appropriate flow rates and introducing complementary foods following the principle of progressing from thin to thick textures and fine to coarse consistencies, ensuring food properties match developmental stages. Concurrently, strict restriction of high-risk choking foods—such as whole nuts, whole grapes—is crucial.116–121 Finally, caregivers must learn the Heimlich maneuver for emergencies.122
Children should remain seated while eating under parental supervision, with restrictions on inappropriate behaviors (running/jumping, talking during meals); heightened vigilance is required when children consume high-risk foods. During play, minimize exposure to small objects like button batteries, toy parts, and coins to reduce RPIs at the source.123
For elderly patients with underlying conditions (such as gastroesophageal reflux, stroke, dysphagia, immunodeficiency), relevant vaccinations can prevent RPIs induced by aspiration.41,90,124 Dysphagic patients should receive swallowing rehabilitation and appropriate food texture selection.109,110 Bedridden or dependent individuals require rigorous oral hygiene and regular professional dental cleaning; active treatment of oral diseases reduces oropharyngeal colonizing bacteria.111–113 Additionally, elevate the bed head by 35–40° (if no contraindications) and adopt suitable feeding postures.125 Psychiatric patients require guided use of antipsychotics, antihistamines, and anticholinergics, with supervised per-dose administration when necessary.44,126 Patients undergoing general anesthesia must fast ≥8 hours and abstain from fluids ≥2 hours preoperatively.43 Unconscious individuals (due to intoxication, shock) should be placed prone or semi-recumbent.127 Patients with esophageal disorders warrant comprehensive nursing support, with surgery if indicated.45
Conclusion and Prospect
RPIs caused by foreign body aspiration are more commonly observed in pediatric and geriatric populations. Additionally, patients with swallowing dysfunction, compromised immune function, and those who are unable to care for themselves are also at higher risk for RPIs induced by foreign bodies, which can impose significant lifestyle stress and economic burdens on families. To reduce the incidence of RPIs caused by foreign bodies, the most effective strategies to reduce their incidence involve improving diagnostic rates, the selection of appropriate antimicrobial interventions, and the implementation of effective preventive strategies.
On one hand, rational selection of diagnostic tools for aspiration-induced RPIs enables timely confirmation of foreign body size/location while reducing unnecessary bronchoscopies. Compared to bronchoscopy, imaging investigations offer higher patient acceptance but require balancing radiation exposure against diagnostic value. Advancements in artificial intelligence (AI) now enable reduced radiation exposure without compromising image quality. Enhancing physicians’ image interpretation skills and diagnostic proficiency—cultivated through extensive clinical experience—remains vital. Future research should explore AI-assisted imaging analysis to boost diagnostic efficiency and cost-effectiveness. For patients undiagnosed by chest CT but with high suspicion of aspiration-induced recurrent pulmonary infection, timely bronchoscopy facilitates both foreign body removal and definitive diagnosis. However, even when performed by experienced clinicians using optimal bronchoscopes, complications remain non-negligible. Bronchoscopy may also exacerbate inflammation by irritating infected bronchial mucosa. Thus, we recommend prioritizing bronchoscopy only with clear aspiration history and clinical manifestations. Patients without documented aspiration history should first undergo CT to evaluate for foreign bodies and assess pulmonary infection severity; bronchoscopy should then be considered based on CT findings and clinical status. Future studies should optimize bronchoscopic techniques to minimize complications and develop more efficient diagnostic tools.
On the other hand, early and precise antimicrobial therapy post-diagnosis is essential. Empirical broad-spectrum antibiotics (third-generation cephalosporins) may be initiated pending pathogen identification. Obtain paired blood cultures before first antibiotic dose. Ensure sputum sample adequacy for culture (>25 leukocytes and <10 squamous epithelial cells per low-power field); bronchoalveolar lavage fluid (BALF) should yield isolated pathogens. Confirmed pathogens warrant targeted antimicrobials to reduce resistance development. Pathogen profiles are dynamic; therefore, antibiotic selection must consider local epidemiology, resistance patterns, and nosocomial infection data—not solely guidelines.
Finally and most critically, the current absence of dedicated guidelines for managing aspiration-induced RPIs underscores the paramount importance of prevention—especially in high-risk children and elderly populations. Recurrent pediatric pulmonary infections warrant prompt screening for aspiration etiology. For elderly individuals with dysphagia, immunosuppression, or dependence, maintaining oral hygiene reduces aspiration-related infections. Future research should explore multidisciplinary prevention models integrating medical, nursing, and rehabilitative resources—including regular home visits by community physicians/nurses/therapists. Additionally, detailed treatment guidelines addressing special populations and complex cases are urgently needed to standardize clinical management.
In summary, pulmonary infections resulting from foreign body aspiration possess a strong tendency to be covert, and the affected populations exhibit specific characteristics. When physicians encounter repeated pulmonary infections in special populations and suspect foreign body aspiration, timely bronchoscopic examination is crucial to rule out or confirm pulmonary infections caused by foreign body aspiration.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Sichuan Provincial Hospital Association Youth Pharmacist Research Special Fund Project (YP2202438).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Metlay JP, Waterer GW, Long AC, et al. Diagnosis and treatment of adults with community-acquired pneumonia. an official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019;7(200):e45–e67. doi:10.1164/rccm.201908-1581ST
2. Tural-Kara T, Özdemir H, Yıldız N, et al. Underlying diseases and causative microorganisms of recurrent pneumonia in children: a 13-year study in a university hospital. J Trop Pediatr. 2019;3(65):224–230. doi:10.1093/tropej/fmy037
3. Infections GLR, Collaborators AR. Global, regional, and national incidence and mortality burden of non-COVID-19 lower respiratory infections and aetiologies, 1990-2021: a systematic analysis from the global burden of disease study 2021. Lancet Infect Dis. 2024;9(24):974–1002.
4. Gupte T, Knack A, Cramer JD. Mortality from aspiration pneumonia: incidence, trends, and risk factors. Dysphagia. 2022;37(6):1493–1500. doi:10.1007/s00455-022-10412-w
5. Lodha R, Puranik M, Natchu UCM, Kabra SK. Recurrent pneumonia in children: clinical profile and underlying causes. Acta Paediatrica. 2002;11(91):1170–1173. doi:10.1111/j.1651-2227.2002.tb00123.x
6. Baseer KAA, Sakhr H. Clinical profile and risk factors of recurrent pneumonia in children at Qena governorate, Egypt. Int J Clin Pract. 2021;4(75):e13695.
7. Gilchrist BF, Valerie EP, Nguyen M, Coren C, Klotz D, Ramenofsky ML. Pearls and perils in the management of prolonged, peculiar, penetrating esophageal foreign bodies in children. J Pediatric Surg. 1997;10(32):1429–1431. doi:10.1016/S0022-3468(97)90554-6
8. Torres A, Cilloniz C, Niederman MS, et al. Pneumonia. Nat Rev Dis Primers. 2021;1(7):25.
9. Wald ER. Recurrent and nonresolving pneumonia in children. Seminars Respiratory Infections. 1993;1(8):46–58.
10. Panitch HB. Evaluation of recurrent pneumonia. Pediatr Infect Dis J. 2005;3(24):265–266. doi:10.1097/01.inf.0000156419.60574.16
11. Trandafir LM, Boiculese LV, Dimitriu G, MJE-H M, Conference B. Recurrent respiratory tract infections in children. 2017 E-Health and Bioengineering Conference (EHB). 2017;741–744.
12. Roshy RJ, Srinivasan R, Krishna S, Shubha AM. Recurrent pneumonia owing to migratory peanut foreign body. Paediatrics Intl Child Health. 2023;42(3–4):148–151. doi:10.1080/20469047.2023.2209486
13. Lupu S, Buga G, Buga AML, et al. Is there a potential link between gastroesophageal reflux disease and recurrent respiratory tract infections in children? Diagnostics. 2023;13(13):2310. doi:10.3390/diagnostics13132310
14. Ciftçi E, Güneş M, Köksal Y, Ince E, Doğru U. Underlying causes of recurrent pneumonia in Turkish children in a university hospital. J Trop Pediatr. 2003;4(49):212–215. doi:10.1093/tropej/49.4.212
15. Babalola O, Kanchustambham V. A case of occult pistachio-shell endobronchial foreign body causing recurrent pneumonia. Cureus. 2023;4(15):e37686.
16. Dang TT, Majumdar SR, Marrie TJ, Eurich DT. Recurrent pneumonia: a review with focus on clinical epidemiology and modifiable risk factors in elderly patients. Drugs Aging. 2015;1(32):13–19. doi:10.1007/s40266-014-0229-6
17. FMd B, Bush A. Recurrent lower respiratory tract infections in children. Br Med J. 2018;000(362):k2698.
18. Ding G, Wu B, Vinturache A, Cai C, Lu M, Gu H. Tracheobronchial foreign body aspiration in children. Medicine. 2020;99(22):e20480. doi:10.1097/MD.0000000000020480
19. Zerella JT, Dimler M, McGill LC, Pippus KJ. Foreign body aspiration in children: value of radiography and complications of bronchoscopy. J Pediatric Surg. 1998;33(11):1651–1654. doi:10.1016/S0022-3468(98)90601-7
20. Özçelik T, Can Oksay S, Girit S. Diagnostic approach to the etiology of recurrent pneumonia in children. Pediatric pulmonology. 2024;59(12):3650–3659. doi:10.1002/ppul.27275
21. Zhang X, Shi Q. Tracheobronchial foreign body in children with an insidious medical history. J Coll Physicians Surg Pak. 2024;34(6):740–741.
22. Schmidt H, Manegold BC. Foreign body aspiration in children. Surg Endosc. 2000;7(14):644–648. doi:10.1007/s004640000142
23. Wolach B, Raz A, Weinberg J, Mikulski Y, Ari JB, Sadan N. Aspirated foreign bodies in the respiratory tract of children: eleven years experience with 127 patients. Int J Pediatric Otorhinolaryngol. 1994;1(30):1–10. doi:10.1016/0165-5876(94)90045-0
24. Baharloo F, Veyckemans F, Francis C, Biettlot MP, Rodenstein DO. Tracheobronchial foreign bodies: presentation and management in children and adults. Chest. 1999;5(115):1357–1362.
25. Rovin JD, Rodgers BM. Pediatric foreign body aspiration. Pediatrics in Rev. 2000;3(21):86–90. doi:10.1542/pir.21.3.86
26. Bergamini M, Kantar A, Cutrera R, Ipci G. Analysis of the literature on chronic cough in children. The Open Respiratory Medicine Journal. 2017;000(11):1–9. doi:10.2174/1874306401711010001
27. Torres A, Peetermans WE, Viegi G, Blasi F. Risk factors for community-acquired pneumonia in adults in Europe: a literature review. Thorax. 2013;11(68):1057–1065. doi:10.1136/thoraxjnl-2013-204282
28. Lange P, Vestbo J, Nyboe J. Risk factors for death and hospitalization from pneumonia. A prospective study of a general population. Eur Respir J. 1995;10(8):1694–1698. doi:10.1183/09031936.95.08101694
29. Bosch X, Formiga F, Cuerpo S, Torres B, Rosón B, López-Soto A. Aspiration pneumonia in old patients with dementia. Prognostic factors of mortality. Eur J Internal Med. 2012;8(23):720–726. doi:10.1016/j.ejim.2012.08.006
30. Hannawi Y, Hannawi B, Rao CPV, Suarez JI, Bershad EM. Stroke-associated pneumonia: major advances and obstacles. Cerebrovascular Dis. 2013;5(35):430–443. doi:10.1159/000350199
31. Taylor JK, Fleming GB, Singanayagam A, Hill AT, Chalmers JD. Risk factors for aspiration in community-acquired pneumonia: analysis of a hospitalized UK cohort. Am J Med. 2013;11(126):995–1001. doi:10.1016/j.amjmed.2013.07.012
32. Cabré M, Serra-Prat M, Force L, Almirall J, Palomera E, Clavé P. Oropharyngeal dysphagia is a risk factor for readmission for pneumonia in the very elderly persons: observational prospective study. J Gerontology Series A. 2014;3(69):330–337. doi:10.1093/gerona/glt099
33. Marik PE, Kaplan D. Aspiration pneumonia and dysphagia in the elderly. Chest. 2003;1(124):328–336. doi:10.1378/chest.124.1.328
34. Almirall J, Rofes L, Serra-Prat M, et al. Oropharyngeal dysphagia is a risk factor for community-acquired pneumonia in the elderly. Eur Respir J. 2013;4(41):923–928. doi:10.1183/09031936.00019012
35. Jang G, Song JW, Kim HJ, Kim EJ, Jang JG, Cha S-I. Foreign-body aspiration into the lower airways in adults; multicenter study. PLoS One. 2022;7(17):e0269493. doi:10.1371/journal.pone.0269493
36. Teramoto S, Matsuse T, Ouchi Y. Foreign body aspiration into the lower airways may not be unusual in older adults. Chest. 1998;6(113):1733–1734. doi:10.1378/chest.113.6.1733
37. Birnkrant DJ. The assessment and management of the respiratory complications of pediatric neuromuscular diseases. Clin Pediatrics. 2002;5(41):301–308. doi:10.1177/000992280204100502
38. Smith PE, Wiles CM. Cough responsiveness in neurogenic dysphagia. J Neurol Neurosurg Psychiatry. 1998;3(64):385–388. doi:10.1136/jnnp.64.3.385
39. Ishifuji T, Sando E, Kaneko N, et al. Recurrent pneumonia among Japanese adults: disease burden and risk factors. BMC Pulm Med. 2017;1(17):12. doi:10.1186/s12890-016-0359-1
40. Noguchi S, Yatera K, Kato T, et al. Impact of the number of aspiration risk factors on mortality and recurrence in community-onset pneumonia. 2017;000(12):2087–2094.
41. Solh AAE, Brewer T, Okada M, Bashir O, Gough M. Indicators of recurrent hospitalization for pneumonia in the elderly. J Am Geriatr Soc. 2004;12(52):2010–2015. doi:10.1111/j.1532-5415.2004.52556.x
42. Stewart JT. Covert dysphagia and recurrent pneumonia related to antipsychotic treatment. J Psychiatry Neurosci. 2018;2(43):143–144. doi:10.1503/jpn.170147
43. Mandell LA, Niederman MS. Aspiration Pneumonia. New Engl J Med. 2019;7(380):651–663. doi:10.1056/NEJMra1714562
44. Herzig SJ, LaSalvia MT, Naidus E, et al. Antipsychotics and the risk of aspiration pneumonia in individuals hospitalized for nonpsychiatric conditions: a cohort study. J Am Geriatr Soc. 2017;12(65):2580–2586. doi:10.1111/jgs.15066
45. Harowicz MR, Khalifah AA, Cohen KA, et al. Anatomic and pathologic causes of recurrent pulmonary infections. 2023;6(43):e220106.
46. Niederman MS, Cilloniz C. Aspiration pneumonia. Revista Espanola de Quimioterapia. 2022;000(35):73–77. doi:10.37201/req/s01.17.2022
47. Aas JA, Paster BJ, Stokes LN, Olsen I, Dewhirst FE. Defining the normal bacterial flora of the oral cavity. J Clin Microbiol. 2005;11(43):5721–5732. doi:10.1128/JCM.43.11.5721-5732.2005
48. Dewhirst FE, Chen T, Izard J, et al. The human oral microbiome. J Bacteriol. 2010;19(192):5002–5017. doi:10.1128/JB.00542-10
49. Parray T, Abraham E, Apuya JS, Ghafoor AU, Siddiqui MSJTIJo A. Migration of a foreign body from right to left lung. Int J Anesthesiol. 2009;24.
50. Kikuchi R, Isowa N, Tokuyasu H, Kawasaki Y. Intraoperative migration of a nail from the left B10b to the main bronchus. Interactive Cardiovasc and Thoracic Surg. 2007;1(6):92–93.
51. Nasrallah E, Mansour B, Zoabi T, Dalal R, Elias N. Recurrent wandering pneumonia as an unusual presentation of foreign body aspiration. Harefuah. 2018;8(157):495–497.
52. Eyekpegha OJ, Onakpoya UU, Obiajunwa PO, Famurewa OC, Ogunrombi AB. Missed distal tracheal foreign body in consecutive bronchoscopies in a 6-year-old boy. Nigerian J Surg. 2017;1(23):67–70. doi:10.4103/1117-6806.199957
53. Dikensoy O, Usalan C, Filiz A. Foreign body aspiration: clinical utility of flexible bronchoscopy. Postgraduate Medl J. 2002;78(921):399–403. doi:10.1136/pmj.78.921.399
54. Agrawal SR, Shankar SG, Joshi AA, Patekar S, Bradoo RA. Role of bronchoscopy and imaging in long-standing foreign body bronchus presenting as recurrent or non-resolving lower respiratory tract infection. Europ Archiv Oto-Rhino-Laryngol. 2021;5(278):1477–1481. doi:10.1007/s00405-020-06497-4
55. Ali MS, Musani AI, Gaurav K. pulmonary foreign body: an unusual cause of recurrent pneumonia. Archivos de Bronconeumologia. 2018;1(54):39.
56. Nihei M, Okazaki T, Ebihara S, et al. Chronic inflammation, lymphangiogenesis, and effect of an anti-VEGFR therapy in a mouse model and in human patients with aspiration pneumonia. J Pathol. 2015;4(235):632–645. doi:10.1002/path.4473
57. Ma W, Xu Y, Ding Z. Clinical analysis of long-term misdiagnosis of bronchial foreign body for pulmonary infection. Zhejiang Clinl Med J. 2005;9(7).
58. Komatsu R, Okazaki T, Ebihara S, et al. Aspiration pneumonia induces muscle atrophy in the respiratory, skeletal, and swallowing systems. J Cachexia Sarcopenia Muscle. 2018;4(9):643–653. doi:10.1002/jcsm.12297
59. Borrelli O, Battaglia M, Galos F, et al. Non-acid gastro-oesophageal reflux in children with suspected pulmonary aspiration. Digestive Liver Dis. 2010;2(42):115–121. doi:10.1016/j.dld.2009.06.011
60. Yatera K, Yamasaki K. Management of the diagnosis and treatment of pneumonia in an aging society. Internal Med. 2024;
61. Karišik M. Foreign body aspiration and ingestion in children. Acta Clinica Croatica. 2023;62(Suppl1):105–112. doi:10.20471/acc.2023.62.s1.13
62. Liu J, Fukuda H, Kondo E, Sakai Y, Sakai H, Kurita H. Screening of aspiration pneumonia using the modified Mallampati classification tool in older adults. PLoS One. 2024;19(5):e0302384. doi:10.1371/journal.pone.0302384
63. Uno I, Kubo T. Risk Factors for Aspiration Pneumonia among Elderly Patients in a Community-Based Integrated Care Unit: a Retrospective Cohort Study. Geriatrics. 2021;6(4). doi:10.3390/geriatrics6040113
64. Talaie H, Jabari HR, Shadnia S, Pajouhmand A, Nava-Ocampo AA, Youssefi M. Cefepime/clindamycin vs. ceftriaxone/clindamycin for the empiric treatment of poisoned patients with aspiration pneumonia. Acta Bio-Med. 2008;79(2):117–122.
65. Ge L, Chen S, Lin M, Xia X, Jin Y, He S. Clinical characteristics of lipid aspiration pneumonia in 16 children. Zhonghua Er Ke Za Zhi = Chinese Journal of Pediatrics. 2014;52(3):205–208.
66. Stuckey-Schrock K, Hayes BL, George CM. Community-acquired pneumonia in children. Am Family Phys. 2012;86(7):661–667.
67. Zissin R, Shapiro-Feinberg M, Rozenman J, Apter S, Smorjik J, Hertz M. CT findings of the chest in adults with aspirated foreign bodies. Eur Radiol. 2001;4(11):606–611. doi:10.1007/s003300000619
68. Boyd M, Chatterjee A, Chiles C Jr, Chin R. Tracheobronchial foreign body aspiration in adults. Southern Med J. 2009;2(102):171–174. doi:10.1097/SMJ.0b013e318193c9c8
69. Gordon L, Nowik P, Kesheh SM, Lidegran M, Diaz S. Diagnosis of foreign body aspiration with ultralow-dose CT using a tin filter: a comparison study. Emerg Radiol. 2020;4(27):399–404. doi:10.1007/s10140-020-01764-7
70. Schaefer-Prokop C, Klein JS. Digital chest radiography. J Thoracic Imaging. 2003;3(18):123. doi:10.1097/00005382-200307000-00001
71. Pitiot V, Grall M, Ploin D, Truy E, Khalfallah SA. The use of CT-scan in foreign body aspiration in children: a 6 years’ experience. Int J Pediatric Otorhinolaryngol. 2017;000(102):169–173. doi:10.1016/j.ijporl.2017.08.036
72. Tuckett P, Cervin A. Reducing the number of rigid bronchoscopies performed in suspected foreign body aspiration cases via the use of chest computed tomography: is it safe? A literature review. J Laryngology Otol. 2015;000(129):S1–7. doi:10.1017/S0022215114002862
73. Bayramoglu S, Cimilli T, Aksoy S, et al. The role of HRCT versus CXR in children with recurrent pulmonary infections. Clin Imaging. 2005;5(29):317–324. doi:10.1016/j.clinimag.2005.02.001
74. Pochepnia S, Grabczak EM, Johnson E, Eyuboglu FO, Akkerman O, Prosch H. Imaging in pulmonary infections of immunocompetent adult patients. Breathe. 2024;1(20):230186. doi:10.1183/20734735.0186-2023
75. Wälscher J, Gompelmann D. Bronchoscopy. Deutsche Medizinische Wochenschrift. 2016;17(141):1236–1238.
76. Sehgal IS, Dhooria S, Ram B, et al. foreign body inhalation in the adult population: experience of 25,998 bronchoscopies and systematic review of the literature. Respiratory Care. 2015;10(60):1438–1448. doi:10.4187/respcare.03976
77. Ueda A, Nohara K, Fujii N, Nakajima K, Miyauchi Y, Inoue Y. Computed tomography findings of 50 patients diagnosed with aspiration pneumonia: a case series. J General Family Med. 2024;25(6):384–387. doi:10.1002/jgf2.717
78. El Khoury P, Makhoul M, El Hadi C, Haber C, Rassi S. CT scan in children suspected of foreign body aspiration: a systematic review and meta-analysis. Otolaryngol Head Neck Surg. 2024;170(1):1–12. doi:10.1002/ohn.433
79. Goodarzy B, Rahmani E, Farrokhi M, et al. Diagnostic value of chest computed tomography scan for identification of foreign body aspiration in children: a systematic review and meta-analysis. Arch Academic Emergency Med. 2025;13(1):e3. doi:10.22037/aaem.v12i1.2431
80. Xu EM, Xu ZQ, Wang ZN, et al. Experience in the removal of difficult and high risk tracheobronchial foreign body by bronchoscopy. Zhonghua er bi yan hou tou jing wai ke za zhi =. Chin J Otorhinolaryngol Head Neck Surg. 2012;47(12):982–986.
81. Mir M, Soto F, Gomez PAA, et al. Bronchoalveolar lavage cell percentages as diagnostic markers of immune checkpoint inhibitor pneumonitis. Front Med. 2025;12:1582714. doi:10.3389/fmed.2025.1582714
82. Moreau D, Evain JN, Mortamet G, Atallah I. Role of expiratory chest X-ray in pediatric foreign body aspiration. Int J Pediatric Otorhinolaryngol. 2024;183:112033. doi:10.1016/j.ijporl.2024.112033
83. Mise K, Jurcev Savicevic A, Pavlov N, Jankovic S. Removal of tracheobronchial foreign bodies in adults using flexible bronchoscopy: experience 1995-2006. Surg Endosc. 2009;23(6):1360–1364. doi:10.1007/s00464-008-0181-9
84. Çelikkaya ME, Atıcı A, Korkmaz İ, Karadağ M, El Ç, Akçora B. Negative bronchoscopy or computed tomography radiation in children with suspected foreign body aspiration? pros and cons. Tomography. 2025;11(2):17. doi:10.3390/tomography11020017
85. Sugitate R, Muramatsu K, Ogata T, et al. Recurrent pneumonia in three patients with MECP2 duplication syndrome with aspiration as the possible cause. Brain Dev. 2022;7(44):486–491. doi:10.1016/j.braindev.2022.03.005
86. Marin-Corral J, Pascual-Guardia S, Amati F, et al. Aspiration risk factors, microbiology, and empiric antibiotics for patients hospitalized with community-acquired pneumonia. Chest. 2021;1(159):58–72. doi:10.1016/j.chest.2020.06.079
87. Koenen MH, RCAd G, WAAdS P, et al. Mycoplasma pneumoniae carriage in children with recurrent respiratory tract infections is associated with a less diverse and altered microbiota. Ebiomedicine. 2023;000(98):104868. doi:10.1016/j.ebiom.2023.104868
88. Prina E, Ranzani OT, Polverino E, et al. Risk factors associated with potentially antibiotic-resistant pathogens in community-acquired pneumonia. Ann Am Thoracic Soc. 2015;2(12):153–160. doi:10.1513/AnnalsATS.201407-305OC
89. Ishida T, Tachibana H, Ito A, et al. Clinical characteristics of pneumonia in bedridden patients receiving home care: a 3-year prospective observational study. J Infect Chemother. 2015;21(8):587–591. doi:10.1016/j.jiac.2015.04.013
90. Janssens J-P. Pneumonia in the elderly (geriatric) population. Curr Opin Pulm Med. 2005;3(11):226–230.
91. Shoar S, Musher DM. Etiology of community-acquired pneumonia in adults: a systematic review. Pneumonia. 2020;000(12):11. doi:10.1186/s41479-020-00074-3
92. Martin-Loeches I, Torres A, Nagavci B, et al. ERS/ESICM/ESCMID/ALAT guidelines for the management of severe community-acquired pneumonia. Intensive Care Med. 2023;6(49):615–632. doi:10.1007/s00134-023-07033-8
93. Pan D, Chung S, Nielsen E, Niederman MSAP. Seminars in respiratory and critical care medicine. 2024;2(45):237–245.
94. Pan D, Niederman MS. Risk factors and algorithms for the empirical treatment of hospital-acquired pneumonia and ventilator-associated pneumonia. Semin Resp Crit Care Med. 2022;2(43):183–190.
95. Abraham ZS, Bukanu F, Kimario OM, Kahinga AA. Unusual longstanding intrabronchial foreign body masquerading as intractable bronchial asthma in an adult: case report and literature review. Int J Surg Case Rep. 2021;000(86):106340. doi:10.1016/j.ijscr.2021.106340
96. Chantzaras A-P, Panagiotou P, Karageorgos S, Douros K. A systematic review of using flexible bronchoscopy to remove foreign bodies from paediatric patients. Acta Paediatrica. 2022;7(111):1301–1312. doi:10.1111/apa.16351
97. Gang W, Zhengxia P, Hongbo L, et al. Diagnosis and treatment of tracheobronchial foreign bodies in 1024 children. J Pediatric Surg. 2012;11(47):2004–2010. doi:10.1016/j.jpedsurg.2012.07.036
98. Suzen A, Karakus SC, Erturk N. The role of flexible bronchoscopy accomplished through a laryngeal mask airway in the treatment of tracheobronchial foreign bodies in children. Int J Pediatric Otorhinolaryngol. 2019;000(117):194–197. doi:10.1016/j.ijporl.2018.12.006
99. Li P, Jiang G, Li Q. The risks of postoperative complications and prolonged hospital stay in children receiving bronchoscopy. J Pediatric Surg. 2020;7(55):1309–1312. doi:10.1016/j.jpedsurg.2019.05.014
100. Tenenbaum T, Kähler G, Janke C, Schroten H, Demirakca S. Management of foreign body removal in children by flexible bronchoscopy. J Bronchol Int Pulmonol. 2017;1(24):21–28. doi:10.1097/LBR.0000000000000319
101. Hutchinson KA, Turkdogan S, Nguyen LHP. Foreign body aspiration in children. Can Med Assoc J. 2023;9(195):E333. doi:10.1503/cmaj.221393
102. Murray & nadel’s textbook of respiratory medicine, 2-volume set. 2021.
103. Takahashi H, Suzuki J, Ikeda R, et al. The transition of pediatric tracheobronchial foreign body cases in the past 36 years: a retrospective single-center study in Japan. Tohoku J Exp Med. 2023;261(2):129–137. doi:10.1620/tjem.2023.J062
104. Cravo J, Marques MAT. Endobronchial foreign bodies in adults - Flexible bronchoscopy as a first approach. Pulmonology. 2018;3(24):198–199. doi:10.1016/j.pulmoe.2018.01.003
105. Bajaj D, Sachdeva A, Deepak D. Foreign body aspiration. J Thoracic Dis. 2021;8(13):5159–5175. doi:10.21037/jtd.2020.03.94
106. Ott SR, Lode H. Diagnosis and therapy of aspiration pneumonia. Deutsche Medizinische Wochenschrift. 2006;12(131):624–628. doi:10.1055/s-2006-933707
107. Sezer HF, Eliçora A, Topçu S. Foreign body aspirations with rigid bronchoscopy and esophagoscopy in children. Turk Gogus Kalp Damar Cerrahisi Dergisi. 2024;32(Suppl1):S55–s59. doi:10.5606/tgkdc.dergisi.2024.25688
108. González-Fernández M, Huckabee M-L, Doeltgen SH, Inamoto Y, Kagaya H, Saitoh E. Dysphagia rehabilitation: similarities and differences in three areas of the world. Curr Phys Med Rehabilitat Rep. 2013;4(1):296–306. doi:10.1007/s40141-013-0035-9
109. Momosaki R. Rehabilitative management for aspiration pneumonia in elderly patients. J General Family Med. 2017;1(18):12–15. doi:10.1002/jgf2.25
110. Ebihara S, Ebihara T, Gui P, Osaka K, Sumi Y, Kohzuki M. Thermal taste and anti-aspiration drugs: a novel drug discovery against pneumonia. Curr Pharm Des. 2014;16(20):2755–2759. doi:10.2174/13816128113199990567
111. Mylotte JM. Will maintenance of oral hygiene in nursing home residents prevent pneumonia? J Am Geriatr Soc. 2018;3(66):590–594. doi:10.1111/jgs.15190
112. Kaneoka A, Pisegna JM, Miloro KV, et al. Prevention of healthcare-associated pneumonia with oral care in individuals without mechanical ventilation: a systematic review and meta-analysis of randomized controlled trials. Infect Control Hosp Epidemiol. 2015;8(36):899–906. doi:10.1017/ice.2015.77
113. Miyagami T, Nishizaki Y, Imada R, et al. Dental care to reduce aspiration pneumonia recurrence: a prospective cohort study. Int Dental J. 2024;74(4):816–822. doi:10.1016/j.identj.2023.11.010
114. Sukumaran M, Granada MJ, Berger HW, Lee M, Reilly TA. Evaluation of corticosteroid treatment in aspiration of gastric contents: a controlled clinical trial. Annals of Global Health. 1980;4(47):335–340.
115. Ehira N, Kudoh A, Katagai H, Takazawa T. A successfully treated case of aspiration pneumonia with adult respiratory distress syndrome and shock. Masui Jap J Anesthesiol. 2002;51(5):535–538.
116. Prevention of choking among children. Pediatrics. 2010;125(3):601–607. doi:10.1542/peds.2009-2862
117. Sidell DR, Kim IA, Coker TR, Moreno C, Shapiro NL. Food choking hazards in children. Int J Pediatric Otorhinolaryngol. 2013;77(12):1940–1946. doi:10.1016/j.ijporl.2013.09.005
118. Bentivegna KC, Borrup KT, Clough ME, Schoem SR. Basic choking education to improve parental knowledge. Int J Pediatric Otorhinolaryngol. 2018;113:234–239. doi:10.1016/j.ijporl.2018.08.002
119. Alsada F, Sebastian T, Alzayer Z, et al. Determinants of infants and young children feeding practices among mothers living in Saudi Arabia: a cross-sectional study. BMC Public Health. 2025;25(1):388. doi:10.1186/s12889-025-21606-w
120. Lorenzoni G, Hochdorn A, Beltrame Vriz G, et al. Regulatory and educational initiatives to prevent food choking injuries in children: an overview of the current approaches. Front Public Health. 2022;10:830876. doi:10.3389/fpubh.2022.830876
121. Picheansathian W, Woragidpoonpol P, Baosoung C. Positioning of preterm infants for optimal physiological development: a systematic review. JBI Lib Syst Rev. 2009;7(7):224–259. doi:10.11124/jbisrir-2009-188
122. Paludi MA, Palermo N, Limonti F, et al. A systematic review on suction-based airway clearance devices for foreign body airway obstruction. Int Emerg Nurs. 2025;79:101575. doi:10.1016/j.ienj.2025.101575
123. Reid A, Hinton-Bayre A, Vijayasekaran S, Herbert H. Ten years of paediatric airway foreign bodies in Western Australia. Int J Pediatric Otorhinolaryngol. 2020;129:109760. doi:10.1016/j.ijporl.2019.109760
124. Ghezzi M, Garancini N, Santis RD, et al. recurrent respiratory infections in children with down syndrome: a review. Children-Basel. 2024;2(11).
125. Macht M, White SD, Moss M. Swallowing dysfunction after critical illness. Chest. 2014;6(146):1681–1689. doi:10.1378/chest.14-1133
126. Takada K, Ogawa K, Miyamoto A, et al. Risk factors and interventions for developing recurrent pneumonia in older adults. ERJ Open Res. 2023;9(3):00516–2022. doi:10.1183/23120541.00516-2022
127. Adnet F, Borron SW, Finot MA, Minadeo J, Baud FJ. Relation of body position at the time of discovery with suspected aspiration pneumonia in poisoned comatose patients. Crit Care Med. 1999;27(4):745–748. doi:10.1097/00003246-199904000-00028
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Maintaining Serum Hemoglobin Levels Within the Physiological Range Prevented Bladder Tamponade Recurrence Due to Radiation-Induced Hemorrhagic Cystitis: A Case Report
Ueda N, Sato M, Matsukawa A, Oki Y, Mizuno R, Akiyama M, Tei N, Miyake O
Research and Reports in Urology 2023, 15:395-401
Published Date: 21 August 2023