")
Back to Journals » Clinical Ophthalmology » Volume 18
Adverse Ocular Impact and Emerging Therapeutic Potential of Cannabis and Cannabinoids: A Narrative Review
Authors Bondok M , Nguyen AXL , Lando L, Wu AY
Received 18 October 2024
Accepted for publication 20 November 2024
Published 29 November 2024 Volume 2024:18 Pages 3529—3556
DOI https://doi.org/10.2147/OPTH.S501494
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mostafa Bondok,1 Anne Xuan-Lan Nguyen,2 Leonardo Lando,3 Albert Y Wu4
1Department of Medicine, Faculty of Medicine, University of British Columbia, Vancouver, BC, Canada; 2Department of Ophthalmology and Visual Sciences, University of Toronto, Toronto, ONT, Canada; 3Ocular Oncology Service, Barretos Cancer Hospital, Barretos, Brazil; 4Department of Ophthalmology, Stanford University School of Medicine, Stanford, CA, USA
Correspondence: Albert Y Wu, Department of Ophthalmology, Stanford University School of Medicine, Stanford, CA, USA, Email [email protected]
Abstract: Cannabis is the most used drug worldwide with an estimated 219 million users. This narrative review aims to explore the adverse effects and therapeutic applications of cannabis and cannabinoids on the eye, given its growing clinical and non-clinical uses. The current literature reports several adverse ocular effects of cannabis and cannabinoids, including eyelid tremor, ptosis, reduced corneal endothelial cell density, dry eyes, red eyes, and neuro-retinal dysfunction. Cannabinoids may transiently impair night vision, depth perception, binocular and monocular contrast sensitivity, and dynamic visual acuity. Cannabinoids are not currently considered a first-line treatment option for any ocular conditions. Δ-9-tetrahydrocannabinol been shown to result in short-term intraocular pressure reduction, but insufficient evidence to support its use in treating glaucoma exists. Potential therapeutic applications of cannabinoids include their use as a second-line agent for treatment-refractory blepharospasm, for dry eye disease given corneal anti-inflammatory properties, and for suppression of pendular nystagmus in individuals with multiple sclerosis, which all necessitate further research for informed clinical practices.
Keywords: cannabis, cannabinoids, adverse effects, therapeutic uses, eye
Introduction
Cannabis is currently the most used drug worldwide, with an estimated 219 million users in 2021,1 and refers to a group of plants that includes Cannabis sativa, Cannabis indica, and Cannabis ruderalis.
Studies have reported the therapeutic efficacy of cannabinoids in treating chronic pain, alleviating spasticity in multiple sclerosis, and serving as an antiemetic.2 Research into cannabinoids’ applications to treat ocular conditions have revealed its potential in treating blepharospasm3–8 and lowering intraocular pressure in glaucoma.9–30 Animal studies demonstrate anti-inflammatory and analgesic properties, corneal regenerative effects,31–40 and retinal neuroprotective effects of cannabinoids.41–54
Several unwanted effects of medical and recreational cannabis use are described in the scientific literature, including nausea, somnolence, and hallucinations.2 Other reports have suggested more substantial effects, including its contribution to the incidence of psychotic disorders.55 As for its effects on the eye, adverse ocular effects of cannabinoids and cannabis reported in contemporary literature include eyelid tremor,56–60 ptosis,61–68 corneal opacification,69,70 reduced corneal endothelial cell count,71 reduced corneal revascularization,72 neuroretinal dysfunction,73–84 retinal vasculature abnormalities,47–52 and impaired extraocular motility.85–101 As ongoing research explores the therapeutic benefits of cannabinoids, the understanding of its adverse effects continues to evolve. Given the growing clinical and non-clinical uses of cannabis and cannabinoids, this article aims to identify adverse ocular effects and assess the emerging potential of cannabinoids in ocular therapeutics.
Brief Historical Context
The growing movement towards the decriminalization and legalization of cannabis1,102,103 necessitates a comprehensive understanding of its physiological effects. In the last decade, there has been a 23% increase in global users:1 a growth rate more rapid than both opiates and cocaine.104 As of 2023, cannabis, commonly referred to as marijuana, pot, weed, grass, or herb, is legal in several countries,102 and 23 states in the United States.103
The use of cannabis for medical purposes has occurred for millennia, with the first historical documentation of its medical use appearing nearly 5000 years ago in Ancient Chinese texts.105 There has been a resurgence of interest in the uses of cannabinoids, the chemical compound in cannabis, to treat several medical conditions in the last few decades.2,106,107
Method of Literature Search
A systematic literature search of Ovid MEDLINE, Ovid Embase, and Scopus from inception of the databases to June 25, 2023, was conducted to identify relevant papers. The search strategy was developed and validated for each database with an academic librarian using both controlled vocabulary (ie, MeSH and Emtree terms) and free-text terms. The search terms used to identify relevant articles across databases are shown in Supplementary Box 1. We further reviewed reference lists of published reviews identified through our search to ensure comprehensive coverage of relevant studies that may have been missed in the initial search. This study was exempt from requiring ethics review by the University of British Columbia Behavioural Research Ethics Board (BREB) given the use of publicly available information, as per TCPS (Article 2.2).108 To enhance accessibility for non-eye care professionals, we have included a brief glossary of relevant ophthalmologic and pharmacologic terms for reference in Supplementary Box 2.
Inclusion and Exclusion Criteria
Studies were included if they discussed adverse ocular effects or therapeutic applications of cannabis or cannabinoids. All forms of cannabinoids were considered, including CBD, THC, as well as synthetic cannabinoids (eg, HU-308, UR-144, XLR-11, Nabilone, Dronabinol, Levoantradol, SR 141716A, WIN55,212–2, GAT211, GAT228, HU211). Any route of administration could be utilized (eg, oral, sublingual, topical). Study abstracts must be written in English, and all study designs were accepted. Observational and experimental studies on human participants were prioritized, while laboratory and animal studies were also considered for supplementation. Studies were excluded if they were not relevant to the research topic, not in English, or not peer reviewed.
Screening and Extraction
Abstracts were screened for relevance by two independent reviewers (MB, LL), and conflicts were resolved through discussion with a third reviewer (AXN). Data extraction of relevant studies was conducted descriptively, and articles were organized by topic, relevance, and conclusions through a collaborative, iterative process.
Pharmacological Effects of Cannabinoids
The cannabis plant species contains approximately 540 natural compounds, over 100 of which are classified as phytocannabinoids (plant-derived cannabinoids) based on their chemical structure.109 The most extensively studied phytocannabinoids are Δ-9-tetrahydrocannabinol (THC) and cannabidiol (CBD), which are the predominant psychotropic and non-psychoactive ingredients, respectively.109 The C. sativa plant has multiple chemotypes that vary in their relative composition of THC and CBD.110
Chemically, phytocannabinoids are a diverse group of isoprenylated resorcinol polyketides. Phytocannabinoids are categorized based on their affinity to the two main cannabinoid receptors: Cannabinoid receptor type 1 (CB1) and Cannabinoid receptor type 2 (CB2).110 CB1 and CB2 receptors belong to a well-known family of G protein-coupled receptors (GPCR), which plays a central role in the endocannabinoid system. CB1 and CB2 are coupled through G proteins, particularly G i/o (inhibitory G protein), to inhibit adenylate cyclase and influence mitogen-activated protein kinase signaling in some contexts.111 CB1 receptors are also coupled through G proteins to various calcium and potassium channels, promoting neuron hyperpolarization.111
Cannabinoid Receptors
The localization of CB1 and CB2 receptors has been delineated using several strategies, each providing unique insights.112 These include messenger RNA in situ hybridization, immunocytochemistry, and quantitative autoradiography.113 CB1 receptors are mainly localized to the brain and central nervous system, while CB2 receptors are predominately localized to the peripheral nervous system and immune system.111,114,115
Most CB1 receptors are located on the pre-terminal axonal segments of neuronal axons, with fewer on other parts of the neuron.116 CB1 receptors can also be found on CCK-positive basket cells,116 on many glutamatergic terminals in the brain,117 and within some peripheral tissues, including the liver,118 pancreas,119 skeletal muscle,120 and adipocytes.121 CB2 receptors are expressed on immune cells,115 neuronal cells,122 as well as cells involved in bone mass regulation.123
The human body produces endogenous cannabinoids called endocannabinoids.112 The endocannabinoid system consists of cannabinoid receptors and the enzymes responsible for the synthesis and degradation of endocannabinoids.112 Endogenous cannabinoids include arachidonoyl ethanolamide (anandamide) and 2-arachidonoyl glycerol (2-AG).111 These endogenous cannabinoids activate CB1 and CB2 receptors, amongst other GPCRs and ion channels.124 The simple conceptual framework of agonists and antagonists is not enough to understand the complex pathways within the endocannabinoid system,112 with a complete understanding requiring an understanding of partial agonism,125 functional selectivity,126 and inverse agonism.127
Safety Considerations
The psychoactive cannabinoid, THC, produces many of the adverse effects of cannabis, while the non-psychoactive CBD is credited for its therapeutic effects.107,128 Non-medical cannabinoid products have differences in their relative concentrations of CBD and THC.110 Retailers who sell cannabinoids are not subject to the same strict regulations as medical prescriptions.129 CBD preparations of these products are often inaccurate,130,131 with CBD and THC concentrations often mislabeled.132,133 Individuals who use cannabis for self-medication report treating pain, anxiety, depression, headache/migraine, nausea, and muscle spasticity.134 The CBD concentrations from retail products are often lower levels than those used in clinical trials and may even contain THC levels that exceed legal limits.130 Meanwhile, medical-grade cannabinoids, both synthetic or plant-derived, have more accurate concentrations of THC and CBD.129 Plant-derived or synthetic CBD have no pharmacological differences when tested in vitro.135
Information on cannabinoid drug interactions is scarce,136 which raises safety concerns. The mechanisms of these drug interactions include CBD’s inhibition of drug transport,137 enzyme inhibition,138 and enzyme induction.139 Cannabis and cannabinoids can have adverse psychiatric effects, such as the increased risk of psychotic disorders, anxiety or panic attacks in naïve users, structural and functional alterations to the brain, mood disturbances and depression, and risks of lung cancer when smoked.140 Consequently, medical cannabis is contraindicated in patients with unstable cardiovascular or respiratory disease, and those with a personal or strong family history of psychosis.141
Cannabinoids and the Ocular Response
The primary mechanism of action of cannabinoids on the eye is through CB1 and CB2 receptors.142 These GPCRs are part of the extensive endocannabinoid system throughout the body.143 Both receptors play a crucial role in modulating the release of neurotransmitters143 and represent a nuanced interplay between the endocannabinoid system and neuronal health.
CB1 receptors are located in the central nervous system, including the eyes, and have been shown to provide neuroprotection to retinal cells, particularly in reducing excitotoxicity, inflammation, and oxidative stress.142 CB1 receptors are also located on the corneal epithelium and endothelium.144 While activation of CB1 receptors has been associated with neuroprotective effects, chronic or excessive CB1 activation, often with the use of exogenous cannabinoids like THC, can potentially cause neurotoxicity.
While some studies suggest CB2 expression in the eyes,145 this topic remains controversial.142 They have been shown to mediate immune and inflammatory responses and contribute to aqueous humor turnover, which can ultimately also promote neuroprotection by suppressing inflammation and immune-mediated damage.22,40,146
Barriers to Ocular Drug Delivery to the Eye
On the ocular level, topical administration of drugs is preferred as it can reduce adverse effects from systemic routes of administration.147 However, only 3–5% of the administered dose reaches the eye due to structural and dynamic barriers.148 When drugs are administered orally, only 1–2% reach the eye,149 and they present with greater systemic adverse effects. Furthermore, orally administrated drugs must pass through the gastrointestinal tract, traverse the bloodstream, and cross the uve-ocular barriers.149 The eye is considered immune privileged due to these blood-ocular barriers, which consist of the blood-aqueous barrier (BAB) in the anterior segment and the blood-retinal barrier (BRB) in the posterior segment of the eye.150 Intravenous and intramuscular routes of administration must overcome the BRB to reach therapeutic targets in the eye.
With topical drug delivery to anterior eye segment structures, only about 3–5% of the applied dose is effective due to protein interactions in the tear film, tear turnover rate, and drug removal through the blinking reflex.151 Physiological barriers present additional challenges for therapeutic targets in the anterior segment, as drugs must pass through several layers. After administration, a drug interacts with the lacrimal fluid (tears), forming a tear film that consists of a lipophilic external, aqueous middle, and mucin inner layer containing electrolytes, lipids, and proteins, which can partially hydrolyze the drug and thus reduce bioavailability.152 The tear turnover rate and blinking reflex result in a short contact time of the drug with ocular surface tissue. Loss of ophthalmic solution via nasolacrimal drainage or systemic absorption via the conjunctiva is a dynamic barrier to drug delivery.152 The corneal epithelial layer comprises a single layer of basal cells and several layers of stratified squamous epithelial cells held together by tight junctions. These cells serve as a barrier against drug penetration via paracellular and transcellular transport pathways.152 Once reaching the anterior chamber, drugs may bind to melanin pigments in the uvea, thus reducing bioavailability in the anterior chamber.153 Topical administration is favorable in the treatment of conjunctivitis, blepharitis, glaucoma, or anterior uveitis.154 When drugs targeting the anterior chamber are delivered systemically, they must overcome the BAB, which consists of the endothelium of the iris/ciliary blood vessels and the non-pigmented ciliary epithelium.155
Drug administration to the posterior segment of the eye occurs via intravitreal, transscleral, subretinal, and topical modes of administration, with the latter being less suitable due to the anatomical specificities of the eye.156 Topical ocular administration targeting structures in the posterior segment must cross the tear film, conjunctiva, cornea, aqueous humor, and vitreous humor. For this reason, posterior segment targets typically require intravitreal and subretinal administration.149
Ocular Teratogenic Effects
A study using pregnant mice found that prenatal exposure to cannabis smoke for 5 minutes each day during gestation resulted in 17% thinner retinas in young adulthood, but this result normalized in older adulthood.157 A longitudinal cohort study of 794,099 infants in Quebec, Canada revealed that prenatal substance exposure was significantly associated with childhood eye disorder hospitalization.158 Exposure to illicit drugs in utero, including smoked cannabis, was also shown to result in reduced visual acuity, nystagmus, and delayed visual maturation in a case series of 20 patients.159 However, these findings were not specific to cannabis exposure, as many participants in the study were known users of other illicit substances (including benzodiazepines and opiates),159 making cannabis-related effects inconclusive.
Adverse Ocular Effects — Anterior Segment
Red Eyes in Cannabis Users
Smoked cannabis causes acute, transient conjunctival injection, or red eye, among users.100,160 Hence, this is one of the most sensitive objective signs of cannabis use, with one study reporting that 94% of drug-impaired drivers with a positive THC blood sample have red eyes.100 THC induces vasodilation through binding cannabinoid receptors in the eye. These on-target effects increase blood flow to the conjunctiva, leading to conjunctival redness. Animal models suggest the degree of THC-induced vasodilation is dose-dependent.161
Dry Eyes and Cannabis
A study on THC’s role in aqueous deficiency dry eye (ADDE) found that CB1 receptors are expressed in cholinergic neuronal axons innervating lacrimal gland cells.162 CB1 activation by THC reduced tearing in male mice, but this was not seen in female mice.162 Other studies on mice have implicated endocannabinoid receptors’ multi-factorial role in dry eye disease (DED).163. A theoretical benefit of cannabis to treat DED through THC-mediated pain relief and CBD-mediated anti-inflammation has been proposed.163 In contrast, dry eye symptoms have been reported by cannabis users in several studies. In a study on medical cannabis users, 8.7% reported dry eyes.164 In a randomized control trial of smoked cannabis for chronic neuropathic pain, dry eyes were one the most common drug-related adverse reactions in the group that received the 9.4% THC formulation.165 A study of orally administered nabilone, a synthetic cannabinoid, also reported dry eyes as a side effect.166
Decreased Corneal Endothelial Cell Density in Cannabis Users
As discussed earlier, CB1 receptors are predominantly located in the corneal epithelium and endothelium.144 A study on cannabis users found a decreased corneal endothelial cell density among chronic users,71 likely due to cannabinoid toxicity as CB1 receptors are prominent in the anterior eye segment.
Topical THC Eyedrops Cause Corneal Opacification in Animal Studies
Experimental studies on the topical application of THC eyedrops in animal studies have demonstrated corneal opacification following administration in cats,69,70 as shown in Table 1. This is thought to occur due to decreased corneal hydration, as activated CB1 receptors inhibit corneal endothelial cell pumping action, attenuating aqueous humor removal from the cornea, which is needed to maintain corneal transparency.70,167.
 |
Table 1 Summary of Studies on the Effects of Cannabis on the Cornea |
Cannabis Effects on Pupils
Cannabis’ effects on pupil size are conflicting. Several studies suggest acute cannabis smoking causes pupillary constriction.169–171 Meanwhile, other studies report pupillary dilation following acute cannabis smoking,100,160,172 likely mediated by sympathetic stimulation.172 A study of 39 synthetic cannabinoid UR-144 users found pupillary dilatation and, less commonly, pupillary constriction.56 Other studies found that smoking cannabis promoted abnormal pupillary reactions to light,160,171 including a decrease in contraction velocity after a light stimulus,169 or more simply reported as a “decreased” pupillary light reflex.160,171
Adverse Ocular Effects — Posterior Segment
Scotopic Vision
GPR55 is expressed in rod photoreceptors and has been implicated in mediating scotopic night vision in animal models.173 The cellular mechanism by which this occurs was delineated using tadpoles, whereby CB1 receptor activation improved visual contrast sensitivity under low-light conditions.174 Several reports describe anecdotal evidence of improvements in night vision after smoking cannabis,175–177, a strategy fishermen use.175 A study in nature evaluating self-reported vision changes after smoked cannabis found that 68% of participants had worsened glare and halos, and 74% felt smoking cannabis diminished their ability to drive at night.178 Similarly, a study of 64 healthy volunteers found reductions in night vision when measured at 20 minutes after smoking cannabis.179 With limited and conflicting evidence, whether cannabis transiently improves night vision in humans remains inconclusive.
Visual Acuity
The effects of cannabis on static visual acuity are not fully elucidated. Ortiz-Peregrina et al found a reduction in static vision following smoking cannabis,178 while Adams et al found no differences in low and high-contrast conditions after smoking cannabis.87 Brown et al demonstrated that cannabis use produces dose-dependent reductions in dynamic visual acuity.180 At an oral dose of 20 mg, while THC provided mild analgesic effects, it also led to blurred vision in cancer patients.181 As for long-term effects, one study demonstrated visual acuity deficits in chronic (>10 years) cannabis users.172 A case-control study found delayed ganglion cells action potential transmission in regular cannabis smokers.74
Reduced Contrast Sensitivity
Contrast sensitivity is another visual function measure. A 30% reduction in binocular and nearly 50% reduction in monocular contrast sensitivity has been demonstrated following smoking cannabis,178,179 even after consideration of the potential contributions of attention and vigilance.182 Another study found contrast sensitivity reductions in cannabis users only in low luminance conditions.98
Neuroretinal Dysfunction in Cannabis Users
Neuroretinal dysfunction was a documented effect of cannabis on the retina through several studies involving humans. Hallucinogen Persisting Perception Disorder (HPPD), a condition whereby users of hallucinogens continue to experience perceptual disorders for months to years after discontinued drug use, has been reported following heavy cannabis smoking73 (Table 2). One study reported relative and absolute scotomas in five subjects measured through campimetry, as well as pathological changes identified on visual evoked potential (VEP) and electroretinogram (ERG) testing in individuals with polysubstance use disorders.75 However, in addition to using cannabis, most study participants also used cocaine, and all used heroin.75 Another case report found transient alternations in photoreceptor function on ERG following acute cannabis inhalation.76 In a case report of a 25-year-old chronic cannabis smoker with unilateral blurred vision and several subretinal blebs, subretinal blebs resolved after cannabis smoking cessation.77 It is difficult to ascertain whether this was due to the cannabis smoking, as the patient was not re-challenged to see if the blebs reappear if cannabis use was reinitiated.77 A study that involved 60 former synthetic cannabinoid users found no significant retinal changes on OCT.78
 |
Table 2 Summary of Studies on the Effects of Cannabis on the Retina and Retinal Vasculature |
Pattern and flash ERGs have helped investigate synaptic transmission abnormalities in cannabis users. Case-control studies of long-term cannabis smokers have reported ganglion cell dysfunction through delayed action potential transmission,74,80 which was found to occur at the central retinal level82 (Table 2). A later study found the degree of this dysfunction to be associated with the quantity of cannabis smoked.83 In addition, other studies have found sustained abnormal visual transmission through decreased amplification by amacrine cells in long-term cannabis smokers.79 Delayed bipolar cell neuroretinal processing has also been delineated,80,81 and confirmed to be due to On and Off pathway dysfunction in cannabis smokers81 (Table 2). Furthermore, a study on mice found functional loss and increased apoptosis in photoreceptor cells following 1 or 2 mg/kg intraperitoneal THC exposure daily for two months.84
Retinal Vasculature Abnormalities in Cannabis Users
Several case reports have proposed associations between cannabis use and abnormalities in retinal vasculature. One case report demonstrated central retinal vein occlusion only minutes following cannabis smoking in an otherwise health 18-year-old male.48 Another case reported branch retinal artery occlusion and acute maculopathy in a 21-year-old man, and suggested this may be due to long-term heavy cannabis smoking183 (Table 2). A case report of monocular vision loss following hemorrhagic macular infarction in a 55-year-old man was suggested as being associated with his long-term cannabis smoking33; however, the event seems to be more temporally related to his pregabalin and alcohol overdose in a suicide attempt the previous night.47 Given the lack of observational studies or larger case series to substantiate these findings, the proposed associations between cannabis use and retinal vascular abnormalities should be interpreted cautiously until more robust, population-based research is available.
Animal studies have demonstrated the dose-dependent effects of abnormal cannabidiol (abn-CBD), a synthetic CBD, through pre-contracted retinal arteriole vasodilation.51,184 This is consistent with a cross-sectional study of 8 participants, whereby an oral dose of 7.5 mg dronabinol, a synthetic cannabinoid and THC derivative, significantly decreased retinal arteriovenous passage time.52 This effect was further verified in a randomized clinical trial of 24 individuals, which found increased optic nerve head blood flow following 5 mg oral administration of dronabinol.50 An observational study on 106 young adults found that mean arteriolar diameter was significantly wider amongst frequent cannabis smokers compared to controls,49 which may represent residual vasodilatory effects from cannabis smoking or impaired autoregulation resulting from chronic cannabis use49 (Table 2).
Adverse Ocular Effects — Adnexal Structures
Cannabis and Cannabinoids May Cause Transient Eyelid Tremors
Several studies have reported transient eyelid tremors as a physical symptom after synthetic cannabinoid56,59 and cannabis use58,59 (Table 3). Eyelid tremor is an umbrella term referring to involuntary and intermittent eyelid muscle spasms.61 While both blepharospasm and eyelid tremor involve abnormal eyelid movements, they are different in their underlying causes, associated symptoms, and clinical presentation.61 These reports do not provide clinical detail about the cannabis and cannabinoid related eyelid tremors and may instead refer to temporary tremors distinct from true blepharospasm,56–59,61 as demonstrated in Table 3. One study of 302 participants noted eyelid tremors in 86.1% of subjects with THC blood levels greater than 1 μg/L by a drug recognition expert (DRE) examination,59 while another study demonstrated 6 out of 18 individuals in driving cases who tested positive for synthetic cannabinoid XLR-11 had eyelid tremors.57 In a study of drug-impaired driving cases, 39 participants with UR-144 concentrations ranging from trace levels to 17 ng/mL, eyelid tremors were among the most reported signs56 Stress and fatigue are common causes of eyelid tremors,186 which may be a confounder to the presence of eyelid tremors in the drug-impaired drivers within these studies.56–59
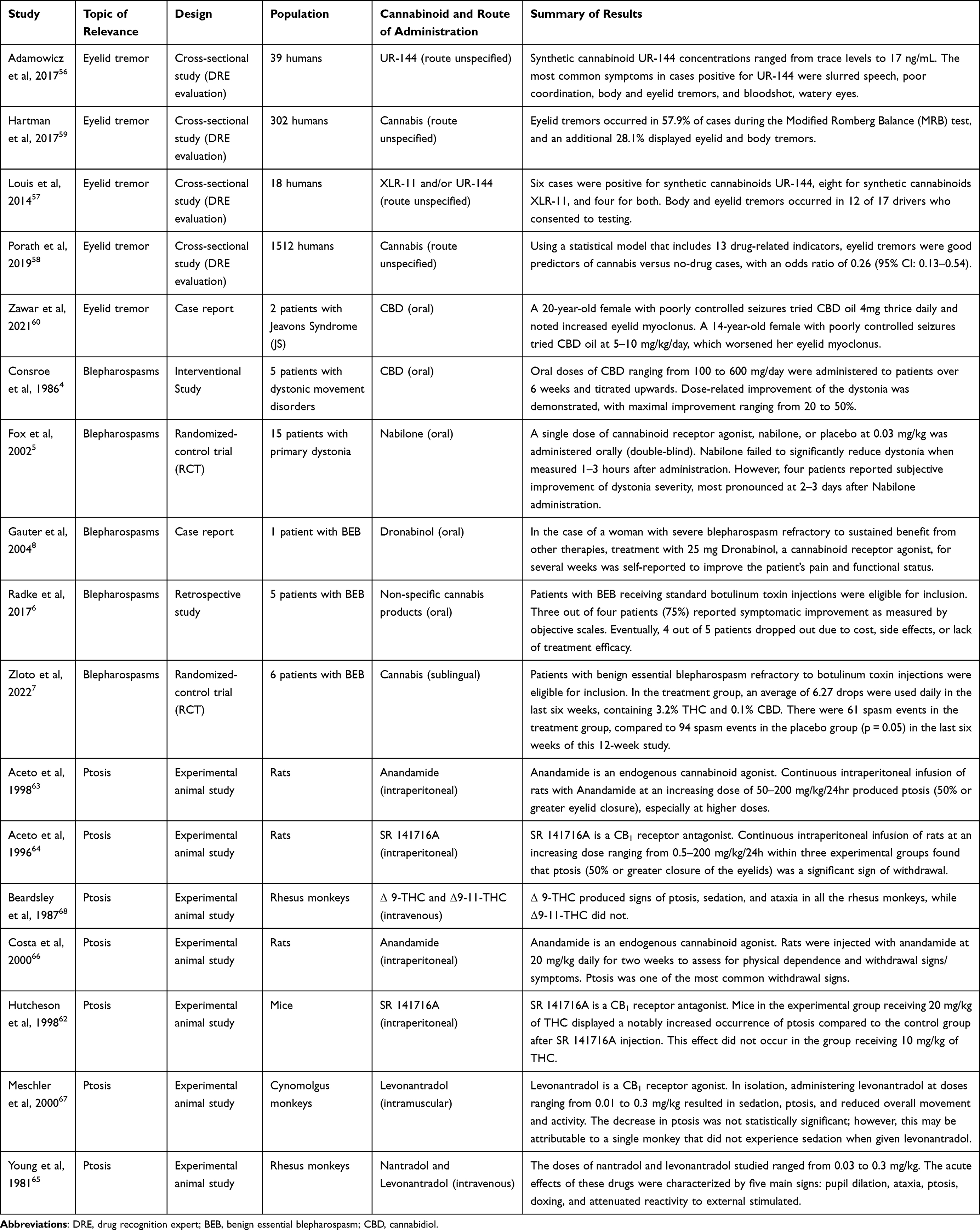 |
Table 3 Summary of Studies on the Effects of Cannabis on the Eyelids |
An interventional study of 5 patients with dystonic movement disorder received oral CBD at doses starting at 100 mg/day, up to 600 mg/day over 6 weeks and found dose-related improvement of dystonia, with maximal improvement ranging from 20–50%4 (Table 3). Benign essential blepharospasm (BEB) is a bilateral focal dystonia characterized by episodic contraction of the eyelid protractor muscles that causes progressive spasms. In a retrospective study of 5 patients with Benign Essential Blepharospasm (BEB) refractory to botulism toxin injections (defined by the researchers as patients with residual symptoms despite being on long-term botulinum toxin therapy), participants received varying doses of oral CBD (5 to 47.5mg) and THC (2.5 to 25 mg) and all but one patient discontinued treatment due to cost, side effects, or lack of treatment efficacy.6 A case report of a woman with severe BEB refractory to botulism toxin injections received oral dronabinol 25 mg for several weeks and reported improved pain and functional status.8 More recently, a randomized controlled trial involving 6 patients with blepharospasm demonstrated the efficacy of 3.2% THC and 0.1% CBD containing drops administered sublingually in the treatment of blepharospasms, as a second-line therapeutic option in patients who repeatedly fail (eg, showed no improvement) first-line treatment using botulinum toxin injections7 (Table 3).
Cannabinoids May Result in Ptosis or Droopy Eyelid
Ptosis, also known as droopy eyelid or blepharoptosis, is characterized by an abnormally low upper eyelid margin position, which may cause visual disturbances or lead to cosmetic concerns.187 Ptosis in the setting of cannabinoid use is classified as having an acquired etiology, as opposed to congenital or involutional causes. One human study of impaired drivers found that 85.6% of blood THC-positive drivers had ptosis identified on field sobriety tests100 (Table 3). This study did not define how ptosis was measured or defined.
Animal model studies have demonstrated ptosis resulting from intraperitoneal Anandamide,63 intraperitoneal SR 141716A,62 as well as cannabinoids administered intravenous or intramuscularly65,67,68 (Table 3). Meanwhile, others have reported ptosis as part of cannabinoid withdrawal.64,66 While most of these studies defined ptosis, whether this effect is chronic, or transient has not been described. Similarly, murine models demonstrated that ptosis resulted from intraperitoneal anandamide, an endogenous cannabinoid.63,66 In a study of non-human primates, rhesus monkeys developed ptosis following acute exposure to intravenous Δ-9-THC but not Δ-11-THC.65,68 Another study on cynomolgus monkeys treated with intramuscular levonantradol, a synthetic THC analog, at doses ranging from 0.01 to 0.03 mg/kg experienced ptosis, but this did not reach statistical significance.67 Overall, animal studies have demonstrated strong evidence that cannabinoids may be associated with ptosis. Observational studies on cannabinoids and cannabis users may provide further insight into potential unwanted effect in humans.
Topical THC Eyedrops and Eyelid Swelling
One study exploring whether topical 1% THC eyedrop administration can decrease intraocular pressure (IOP) reported that 4 out of 28 participants dropped out due to acute burning sensation and “lid swelling”.14 However, 3 out of 4 participants who dropped out were in the control group that received light mineral oil, not THC.14 Based on these findings, it cannot be concluded that THC drops cause acute eyelid swelling.
 |
Table 4 Summary of Studies on the Effects of Cannabis on Extraocular Muscle Functioning |
Oculomotor Control
Cannabis and cannabinoid effects on extraocular motility have been examined in the context of intoxication from recreational use and as side effects following medical uses85–101 (Table 4). Early investigations compared the impact of smoked cannabis and drinking alcohol on ocular movements, and found that alcohol impaired saccades and smooth pursuit, while cannabis did not.85,86,191 Long-term heavy cannabis use may influence static visual acuity, potentially affecting visual performance and promoting changes in psychomotor performance, including ocular motor control.96 Long-term studies by Huestegge et al investigated inhaled cannabis’ persistent effects on oculomotor function and eye movement control during reading in a cross-sectional study. In the study, 20 long-term cannabis users (without acute THC intoxication) had prolonged fixation time, increased text revisiting, and longer word viewing times compared to non-users, suggesting that even subtle deficits in essential oculomotor control can impact reading performance89,90 (Table 4). Potential sustained alterations, including increased fixation time, delayed response times, altered saccadic amplitudes, extended text recheck, and elongation of word visualization were also identified in chronic cannabis users.89,90
Stereopsis
A reduction in three-dimensional vision following smoking cannabis was demonstrated through a deterioration in stereoacuity178,179 (Table 4), defined as the ability to detect differences in the depth of field.178 Other studies have shown a reduction in binocular depth inversion, a sensitive measure of impaired visual information processing, for up to 192 hours after cannabis resin at a dose of 3.0–4.0 mg/kg in seven healthy volunteers192 and permanent reductions in chronic cannabis smokers when measured using a random-dot stereogram.193 As cannabinoids’ effects on extraocular motility implicate a complex interplay with various aspects of visual functioning, including ocular tracking, gaze stability, and nystagmus, further research is needed to investigate these effects.
Gaze Stability and Nystagmus
Beyond gaze stability, cannabinoids have been associated with eye deviation,91 possibly due to alterations of neural pathways involved in eye movement coordination and control.91,93 One case reported conjugate dextrodeviation of the eyes from cannabis intoxication after inadvertent ingestion, with effects lasting six weeks91 (Table 4). Several studies of impaired drivers found horizontal gaze nystagmus a common sobriety examination finding,58,189 which was later tested on 44 human participants, 43 (98%) of which exhibited HGN after smoking cannabis within the three-hour impairment window190 (Table 4).
Thyroid Storm
A case was reported on a 25-year-old man with Graves’ disease who passed away following a thyroid storm, which was thought to have been triggered by smoking synthetic cannabinoids the morning of his presentation to the hospital.194 No other cases have been reported.
Therapeutic Applications of Cannabis and Cannabinoids
Corneal Anti-Inflammatory Properties in Animal Studies
Studies have demonstrated potential therapeutic effects through acute ‘cannabinoid-associated anti-inflammatory, analgesic, and regenerative effects on the cornea,31–40,168 as summarized in Table 1. These include topical cannabinoid receptor agonist WIN55,212-2.34–36,168 Furthermore, in vitro human and in vivo animal studies have demonstrated reduced corneal neovascularization through CB1 receptor antagonism.72,195 Additional studies investigating these potential therapeutic effects are needed.196
Pterygium
Cannabinoid receptor differential expression in patients with pterygium, a wedge-shaped fibrovascular outgrowth that originates in the conjunctiva and extends into the cornea,197 has been reported. This may imply a potential role of cannabinoid targets in the understanding of pterygium.197
Retina Neuroprotective Effects in Animal Studies
The therapeutic potential of cannabinoids on the retina has been explored through several animal studies. A 2008 study that claimed neuroprotective and anti-inflammatory CBD effects on the retina was retracted in 2014 by the journal editors as the findings were not supported by the presented research data.198 Rat model glaucoma studies have demonstrated that intravenous THC or synthetic cannabinoid HU-211 injections significantly reduce retinal ganglion cell (RGC) death,42,43 likely mediated by IOP reduction42 (Table 2). Topical administration of cannabinoid receptor agonist WIN 55212-2 has demonstrated similar neuroprotective effects in rat ischemic models of retinal ganglion cell loss.44 Two studies demonstrated the neuroprotective effects of intraperitoneal synthetic cannabinoid HU-211 injections in rats following optic nerve crush injuries, including a metabolic and electrophysiological deficit reduction,45 and regenerative growth following injury46 (Table 2). Accordingly, while cannabinoid retinal neuroprotective effects have been illustrated in animal studies, this has yet to be demonstrated in the human retina.
Retinal ischemia plays a role in various ocular pathologies, including diabetic retinopathy and glaucoma.185 One study demonstrated that the TRPA1 receptor is a critical element in cell death following the early stages of ischemia.185 By using synthetic cannabinoid receptor agonists, a decrease in lactate dehydrogenase (LDH) was demonstrated in chick retinal models.185 LDH was used as a cell death marker in the study.185 The therapeutic potential of cannabinoids in retinal degenerative etiologies has been explored using animal models. A mouse model study utilizing the CB1 agonist SR141716A found photoreceptor loss recovery following degeneration41 (Table 2).
Applications in Diabetic Retinopathy
Differential expression of endocannabinoids in the ocular tissues of diabetics has been documented, including differences in endocannabinoid concentrations in diabetic patient aqueous humor146 and higher endocannabinoid (AEA and 2-AG) levels in specific anatomical locations within ocular tissue in the post-mortem eye tissue of diabetic retinopathy patients.188 Differential levels of endocannabinoids in the aqueous humor of diabetic and non-diabetic patients may offer a novel therapeutic target for diabetic retinopathy. Given previous studies suggesting endocannabinoids may offer neuroprotection through anti-inflammatory activity, elevated levels of endocannabinoids may be a mechanism for counteracting inflammation in diabetic retinopathy.188
Applications in Glaucoma
Glaucoma is a heterogenous group of irreversible diseases characterized by damage to the optic nerve.199 Therapies focused on reducing IOP are still the primary strategy to prevent disease progression, as IOP remains one of the few modifiable risk factors for glaucoma management.199 Therapeutic and adverse effects of cannabinoids on IOP have been researched by nine groups involving a total of 112 individuals,9–30 with most studies focusing on primary open-angle glaucoma (Table 5).
 |
Table 5 Studies on the Effects of Cannabis on Intraocular Pressure |
Cannabinoids have been shown to promote an IOP decrease in animal and clinical investigations which date back to the 1980s. In 1976, Cohen described a 30% drop in IOP levels for 4–5 hours following smoking of a mean of 103 mg THC in 7 out of 11 individuals with open-angle glaucoma.10 In 1977, a prospective study with 10 subjects receiving intravenous (mean 1.5 or 3.0 mg), weight-adjusted THC experienced a 51% IOP-reduction from baseline.11 It was later found that the BW146Y chemical derivative exhibited a noteworthy independent reduction in intraocular pressure, while BW29Y did not effectively lower intraocular pressure, with both compounds showing mild side effects19 (Table 5).
Subsequent studies have supported short-term THC IOP-reducing effects, thought to occur through aqueous humor outflow mechanisms and trabecular meshwork cell signaling.30 In 2018, an animal study indicated that THC lowers IOP by activating CB1 and GPR18 receptors, whereas CBD was found to potentially interfere with the IOP-related effects of THC16 (Table 5). Altinsoy et al also investigated cannabinoids’ potential counter-benefits in rabbits through the impact of anandamide on endotoxin-induced uveitis.25 The authors eventually concluded that this endogenous cannabinoid ligand can exacerbate uveitis despite the background IOP-reducing benefit.25 While THC has been shown to lower IOP, the effects of other cannabinoids (eg, CBD) and endogenous ligands (eg, anandamide) require further investigation.
Synthetic cannabinoids have also been tried in patients with glaucoma who have not achieved adequate IOP control (<22 mmHg) despite being on two or more topical pharmacotherapies, suggesting a potential therapeutic role in refractory cases.17 Particularly, the synthetic cannabinoid WIN55212-2 was shown to help decrease IOP in the eyes of 8 patients with glaucoma. In 2006, Tomida et al conducted a pilot study administering sublingual CBD or THC and found a short-term reduction in IOP reduction following 5 mg THC, which was well tolerated in patients.20 No IOP reduction was seen with 20 mg CBD, while short-term increased IOP was demonstrated with 40 mg CBD20 (Table 5).
Given the limited evidence of long-term efficacy in treating glaucoma,200–202 cannabinoids are considered ineffective or suboptimal therapeutic options.203,204 This is because of their short duration of action and the incidence of undesirable psychotropic and systemic side effects.201,203,204 Similarly, according to the National Academies of Science (NAS) report on the health effects of cannabis and cannabinoids, it was concluded that given the lack of evidence of continual IOP reducing effects, cannabinoids show limited potential in the treatment of glaucoma.205
Notably, a study of 18 patients with glaucoma inhaled THC led to increased heart rates and lowered intraocular and blood pressure, with hypotensive effects becoming evident after 60 to 90 minutes of use, generally followed by a reduction in intraocular pressure.15 Until cannabinoids can be demonstrated to work at least as effectively and with fewer side effects as current glaucoma therapies, cannabis and cannabinoids have yet to be considered a reliable option for treating glaucoma.203,204 In summary, the long-term efficacy of cannabinoids in disease control have yet to be determined.201,202,205
Cannabinoids in the Treatment of Blepharospasms
A childhood genetic idiopathic generalized epilepsy, Jeavons Syndrome (JS), is partially characterized by eyelid myoclonia. Oral CBD oil seemed to exacerbate eyelid myoclonus in two individuals with JS and poorly controlled seizures when trialed at 4 mg thrice daily, or 5–10mg/kg/day.60 A double-masked randomized control trial using a single dose of 0.03 mg/kg oral nabilone, a cannabinoid receptor agonist, did not demonstrate any significant acute reduction in blepharospasm when compared to placebo5 (Table 3). Meanwhile, other studies have demonstrated that cannabis and cannabinoids may be a potential medical treatment for patients with blepharospasms who showed no improvement following repeat treatments with conventional, first-line treatment using botulinum toxin injections3,4,6,8 (Table 3).
Applications in Pendular Nystagmus
A case reported a 30% reduction in nystagmus at the primary position and improved visual acuity after acute smoking 10 mg cannabis in a patient with congenital horizontal nystagmus.94 Another study reported suppressed pendular nystagmus and improved visual acuity in an individual with multiple sclerosis after smoking cannabis, but not with nabilone tablets or THC- containing capsules (trialed up to 40 mg THC per day).101
Limitations and Future Directions
The authors recognize that this review, by focusing on the ocular therapeutic and side effects, may have left unanswered components of cannabis’ complex mechanism of action on the eye. We also recognize that less researched cannabinoids, such as cannabigerol, cannabinol, and cannabichromene, as well as terpenes, including myrcene, limonene, and pinene, were also not discussed due to the large breadth of the topics. Cannabis and cannabinoid molecular targets, active components, and functions in the eye should continue to be explored.
Future studies should consider exploring the following research areas to address current gaps in the scientific literature:
Conclusions
Cannabinoids are not currently considered a first-line treatment option for any ocular conditions. Cannabinoids may cause eyelid tremors and ptosis, while paradoxically demonstrating therapeutic potential as a second-line agent for treatment-refractory blepharospasm. Several animal studies have demonstrated cannabinoids’ anti-inflammatory and regenerative effects on the cornea. Meanwhile, dry eye symptoms are a common side-effect of cannabis use. Cannabinoid retinal neuroprotective effects have only been demonstrated in animal studies. Neuro-retinal dysfunction has been substantiated in cannabis smokers, with evidence of partial reversibility with cannabis smoking cessation. Case reports have alluded to retinal vasculature abnormalities with heavy cannabis smoking. Cannabis and cannabinoids may decrease intraocular pressure in the short-term. There is insufficient evidence to support the use of cannabis and cannabinoids in glaucoma treatment given the absence of long-term therapeutic benefit, neurocognitive and systemic side-effects, and the present availability of more effective therapies. Studies have documented that cannabis and cannabinoids disrupt extraocular motility, including smooth pursuit, gaze stabilization, ocular motor control, fixation time, and eye deviation. Case reports demonstrate suppressed pendular nystagmus following smoking cannabis in individuals with multiple sclerosis.
Funding
This work was supported by an unrestricted grant from Research to Prevent Blindness and the National Eye Institute (NEI P30-EY026877) to the Stanford Department of Ophthalmology.
Disclosure
The authors have no financial or proprietary interest in any materials discussed in this article.
References
1. United Nations. World drug report. 2023. Available from: https://www.unodc.org/unodc/en/data-and-analysis/world-drug-report-2023.html.
2. Whiting PF, Wolff RF, Deshpande S, et al. Cannabinoids for medical use: a systematic review and meta-analysis. JAMA. 2015;313(24):2456–2473. doi:10.1001/JAMA.2015.6358
3. Koppel BS. Cannabis in the treatment of dystonia, dyskinesias, and tics. Neurotherapeutics. 2015;12(4):788–792. doi:10.1007/S13311-015-0376-4
4. Consroe P, Sandyk R, Snider SR. Open label evaluation of cannabidiol in dystonic movement disorders. Int J Neurosci. 1986;30(4):277–282. doi:10.3109/00207458608985678
5. Fox SH, Kellett M, Moore AP, Crossman AR, Brotchie JM. Randomised, double-blind, placebo-controlled trial to assess the potential of cannabinoid receptor stimulation in the treatment of dystonia. Mov Disord. 2002;17(1):145–149. doi:10.1002/MDS.1280
6. Radke PM, Mokhtarzadeh A, Lee MS, Harrison AR. Medical cannabis, a beneficial high in treatment of blepharospasm? An early observation. Neuro Ophthalmology. 2017;41(5):253–258. doi:10.1080/01658107.2017.1318150
7. Zloto O, Weisman A, Avisar I, et al. Medical cannabis oil for benign essential blepharospasm: a prospective, randomized controlled pilot study. Graefes Arch Clin Exp Ophthalmol. 2022;260(5):1707–1712. doi:10.1007/s00417-021-05533-1
8. Gauter B, Rukwied R, Konrad C. Cannabinoid agonists in the treatment of blepharospasm — a case report study. Neuro Endocrinol Lett. 2004;25(1–2):45–48.
9. Adelli GR, Bhagav P, Taskar P, et al. Development of a Δ 9 -tetrahydrocannabinol amino acid-dicarboxylate prodrug with improved ocular bioavailability. Invest Ophthalmol Vis Sci. 2017;58(4):2167–2179. doi:10.1167/IOVS.16-20757
10. Cohen S. The 94-day cannabis study. Ann N Y Acad Sci. 1976;282(1):211–220. doi:10.1111/J.1749-6632.1976.TB49900.X
11. Cooler P, Gregg JM. Effect of delta-9-tetrahydrocannabinol on intraocular pressure in humans. South Med J. 1977;70(8):951–954. doi:10.1097/00007611-197708000-00016
12. Green K, Roth M. Ocular effects of topical administration of delta 9-tetrahydrocannabinol in man. Arch Ophthalmol. 1982;100(2):265–267. doi:10.1001/ARCHOPHT.1982.01030030267006
13. Hepler RS, Frank IR. Marihuana smoking and intraocular pressure. JAMA Netw. 1971;217:1392. doi:10.1001/jama.1971.03190100074023
14. Jay WM, Green K. Multiple-drop study of topically applied 1% delta 9-tetrahydrocannabinol in human eyes. Arch Ophthalmol. 1983;101(4):591–593. doi:10.1001/ARCHOPHT.1983.01040010591012
15. Merritt JC, Crawford WJ, Alexander PC, Anduze AL, Gelbart SS. Effect of marihuana on intraocular and blood pressure in glaucoma. Ophthalmology. 1980;87(3):222–228. doi:10.1016/S0161-6420(80)35258-5
16. Miller S, Daily L, Leishman E, Bradshaw H, Straiker A. Δ 9 -tetrahydrocannabinol and cannabidiol differentially regulate intraocular pressure. Invest Ophthalmol Vis Sci. 2018;59(15):5904–5911. doi:10.1167/IOVS.18-24838
17. Newell FW, Stark P, Jay WM, Schanzlin DJ. Nabilone: a pressure-reducing synthetic benzopyran in open-angle glaucoma. Ophthalmology. 1979;86(1):156–160. doi:10.1016/S0161-6420(79)35539-7
18. Porcella A, Maxia C, Gessa GL, Pani L. The synthetic cannabinoid WIN55212-2 decreases the intraocular pressure in human glaucoma resistant to conventional therapies. Eur J Neurosci. 2001;13(2):409–412. doi:10.1046/J.0953-816X.2000.01401.X
19. Tiedeman JS, Shields MB, Weber PA, et al. Effect of synthetic cannabinoids on elevated intraocular pressure. Ophthalmology. 1981;88(3):270–277. doi:10.1016/S0161-6420(81)35052-0
20. Tomida I, Azuara-Blanco A, House H, Flint M, Pertwee RG, Robson PJ. Effect of sublingual application of cannabinoids on intraocular pressure: a pilot study. J Glaucoma. 2006;15(5):349–353. doi:10.1097/01.IJG.0000212260.04488.60
21. Mohamed N, Meyer D. Intraocular pressure-lowering effect of oral paracetamol and its in vitro corneal penetration properties. Clin Ophthalmol. 2013;7:219–227. doi:10.2147/OPTH.S38473
22. Fischer KM, Ward DA, Hendrix DVH. Effects of a topically applied 2% delta-9-tetrahydrocannabinol ophthalmic solution on intraocular pressure and aqueous humor flow rate in clinically normal dogs. Am J Vet Res. 2013;74(2):275–280. doi:10.2460/AJVR.74.2.275
23. Zhan GL, Camras CB, Palmberg PF, Toris CB. Effects of marijuana on aqueous humor dynamics in a glaucoma patient. J Glaucoma. 2005;14(2):175–177. doi:10.1097/01.IJG.0000151882.07232.1D
24. Rapino C, Tortolani D, Scipioni L, Maccarrone M. Neuroprotection by (endo) Cannabinoids in glaucoma and retinal neurodegenerative diseases. Curr Neuropharmacol. 2018;16(7):959–970. doi:10.2174/1570159X15666170724104305
25. Altinsoy A, Dileköz E, Kul O, et al. A cannabinoid ligand, anandamide, exacerbates endotoxin-induced uveitis in rabbits. J Ocul Pharmacol Ther. 2011;27(6):545–552. doi:10.1089/JOP.2011.0049
26. Afflitto GG, Aiello F, Scuteri D, Bagetta G, Nucci C. CB1R, CB2R and TRPV1 expression and modulation in in vivo, animal glaucoma models: a systematic review. Biomed Pharmacother. 2022;150. doi:10.1016/J.BIOPHA.2022.112981
27. Maguire G, Eubanks C, Ayoub G. Neuroprotection of retinal ganglion cells in vivo using the activation of the endogenous cannabinoid signaling system in mammalian eyes. Neuronal Signal. 2022;6(1). doi:10.1042/NS20210038
28. Green K. Marijuana smoking vs cannabinoids for glaucoma therapy. Arch Ophthalmol. 1998;116(11):1433–1437. doi:10.1001/ARCHOPHT.116.11.1433
29. Somvanshi RK, Zou S, Kadhim S, Padania S, Hsu E, Kumar U. Cannabinol modulates neuroprotection and intraocular pressure: a potential multi-target therapeutic intervention for glaucoma. Biochim Biophys Acta. 2022;1868(3):166325. doi:10.1016/J.BBADIS.2021.166325
30. Aebersold AS, Song ZH. The effects of cannabidiol on aqueous humor outflow and trabecular meshwork cell signaling. Cells. 2022;11. doi:10.3390/CELLS11193006
31. Toguri JT, Caldwell M, Kelly MEM. Turning down the thermostat: modulating the endocannabinoid system in ocular inflammation and pain. Front Pharmacol. 2016;7. doi:10.3389/FPHAR.2016.00304.
32. Murataeva N, Miller S, Dhopeshwarkar A, et al. Cannabinoid CB2R receptors are upregulated with corneal injury and regulate the course of corneal wound healing. Exp Eye Res. 2019;182:74–84. doi:10.1016/J.EXER.2019.03.011
33. Yang H, Wang Z, Capó-Aponte JE, Zhang F, Pan Z, Reinach PS. Epidermal growth factor receptor transactivation by the cannabinoid receptor (CB1) and transient receptor potential vanilloid 1 (TRPV1) induces differential responses in corneal epithelial cells. Exp Eye Res. 2010;91(3):462–471. doi:10.1016/J.EXER.2010.06.022
34. Murataeva N, Li S, Oehler O, et al. Cannabinoid-induced chemotaxis in bovine corneal epithelial cells. Invest Ophthalmol Vis Sci. 2015;56(5):3304–3313. doi:10.1167/IOVS.14-15675
35. Patwardhan AM, Jeske NA, Price TJ, Gamper N, Akopian AN, Hargreaves KM. The cannabinoid WIN 55,212-2 inhibits transient receptor potential vanilloid 1 (TRPV1) and evokes peripheral antihyperalgesia via calcineurin. Proc Natl Acad Sci. 2006;103(30):11393–11398. doi:10.1073/PNAS.0603861103
36. Bereiter DA, Bereiter DF, Hirata H. Topical cannabinoid agonist, WIN55,212-2, reduces cornea-evoked trigeminal brainstem activity in the rat. Pain. 2002;99(3):547–556. doi:10.1016/S0304-3959(02)00271-3
37. Thapa D, Cairns EA, Szczesniak AM, Toguri JT, Caldwell MD, Kelly MEM. The Cannabinoids Δ 8 THC, CBD, and HU-308 act via distinct receptors to reduce corneal pain and inflammation. Cannabis Cannabinoid Res. 2018;3(1):11–20. doi:10.1089/CAN.2017.0041
38. Murataeva N, Daily L, Taylor X, et al. Evidence for a GPR18 role in chemotaxis, proliferation, and the course of wound closure in the cornea. Cornea. 2019;38(7):905–913. doi:10.1097/ICO.0000000000001934
39. Thapa D, Cairns EA, Szczesniak AM, et al. Allosteric Cannabinoid Receptor 1 (CB1) ligands reduce ocular pain and inflammation. Molecules. 2020;25(2):417. doi:10.3390/MOLECULES25020417
40. Toguri JT, Lehmann C, Laprairie RB, et al. Anti-inflammatory effects of cannabinoid CB 2 receptor activation in endotoxin-induced uveitis. Br J Pharmacol. 2014;171(6):1448–1461. doi:10.1111/bph.12545
41. Chen Y, Luo X, Liu S, Shen Y. Neuroprotective effect of cannabinoid receptor 1 antagonist in the MNU-induced retinal degeneration model. Exp Eye Res. 2018;167:145–151. doi:10.1016/J.EXER.2017.11.001
42. Crandall J, Matragoon S, Khalifa YM, et al. Neuroprotective and intraocular pressure-lowering effects of (–)Δ9-Tetrahydrocannabinol in a rat model of glaucoma. Ophthalmic Res. 2007;39(2):69–75. doi:10.1159/000099240
43. Liu HF, He Y, Jia J, Ji ML, Xi JW. Clinical study on intravitreal injection of cannabinoid HU-211 for optic nerve damage in glaucoma rats. Guoji Yanke Zazhi. 2014;14:1584–1586. doi:10.3980/J.ISSN.1672-5123.2014.09.06
44. Pinar-Sueiro S, Zorrilla Hurtado JÁ, Veiga-Crespo P, Sharma SC, Vecino E. Neuroprotective effects of topical CB1 agonist WIN 55212-2 on retinal ganglion cells after acute rise in intraocular pressure induced ischemia in rat. Exp Eye Res. 2013;110:55–58. doi:10.1016/J.EXER.2013.02.009
45. Yoles E, Belkin M, Schwartz M. HU-211, a nonpsychotropic cannabinoid, produces short- and long-term neuroprotection after optic nerve axotomy. J Neurotrauma. 1996;13(1):49–57. doi:10.1089/NEU.1996.13.49
46. Zalish M, Lavie V. Dexanabinol (HU-211) has a beneficial effect on axonal sprouting and survival after rat optic nerve crush injury. Vision Res. 2003;43(3):237–242. doi:10.1016/S0042-6989(02)00494-7
47. Aktaş S, Tetikoğlu M, İnan S, Aktaş H, Özcura F. Unilateral hemorrhagic macular infarction associated with marijuana, alcohol and antiepileptic drug intake. Cutan Ocul Toxicol. 2016;36(1):88–95. doi:10.3109/15569527.2016.1141420
48. Corvi F, Querques G, Lattanzio R, Preziosa C, Parodi MB, Bandello F. Central retinal vein occlusion in a young patient following cannabis smoke inhalation. Eur J Ophthalmol. 2014;24(3):437–440. doi:10.5301/EJO.5000400
49. Hill M, Wong TY, Davis M, Meier MH. Associations between cannabis use and retinal vessel diameter in young adults. Schizophr Res. 2020;219:62–68. doi:10.1016/J.SCHRES.2019.02.016
50. Hommer N, Kallab M, Szegedi S, et al. The effect of orally administered dronabinol on optic nerve head blood flow in healthy subjects-a randomized clinical trial. Clin Pharmacol Ther. 2020;108(1):155–161. doi:10.1002/CPT.1797
51. MacIntyre J, Dong A, Straiker A, et al. Cannabinoid and lipid-mediated vasorelaxation in retinal microvasculature. Eur J Pharmacol. 2014;735:105–114. doi:10.1016/J.EJPHAR.2014.03.055
52. Plange N, Arend KO, Kaup M, et al. Dronabinol and retinal hemodynamics in humans. Am J Ophthalmol. 2007;143(1):173–174. doi:10.1016/J.AJO.2006.07.053
53. Kalenderoglu A, Orum MH, Karadag AS, et al. Increases in retinal nerve fiber layer thickness may represent the neuroprotective effect of cannabis: an optical coherence tomography study. J Addict Dis. 2020;38(3):280–290. doi:10.1080/10550887.2020.1754109
54. Spyridakos D, Papadogkonaki S, Dionysopoulou S, Mastrodimou N, Polioudaki H, Thermos K. Effect of acute and subchronic administration of (R)-WIN55,212-2 induced neuroprotection and anti inflammatory actions in rat retina: CB1 and CB2 receptor involvement. Neurochem Int. 2021;142:104907. doi:10.1016/J.NEUINT.2020.104907
55. Di Forti M, Quattrone D, Freeman TP, et al. The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): a multicentre case-control study. Lancet Psychiatry. 2019;6(5):427–436. doi:10.1016/S2215-0366(19)30048-3
56. Adamowicz P, Gieroń J, Gil D, Lechowicz W, Skulska A, Tokarczyk B. The effects of synthetic cannabinoid UR-144 on the human body-A review of 39 cases. Forensic Sci Int. 2017;273:e18–e21. doi:10.1016/J.FORSCIINT.2017.02.031
57. Louis A, Peterson BL, Couper FJ. XLR-11 and UR-144 in Washington State and State of Alaska Driving Cases. J Anal Toxicol. 2014;38(8):563–568. doi:10.1093/JAT/BKU067
58. Porath AJ, Beirness DJ. Predicting categories of drugs used by suspected drug-impaired drivers using the drug evaluation and classification program tests. Traffic Inj Prev. 2019;20(3):255–263. doi:10.1080/15389588.2018.1562178
59. Hartman RL, Richman JE, Hayes CE, Huestis MA. Drug Recognition Expert (DRE) examination characteristics of cannabis impairment. Accid Anal Prev. 2016;92:219–229. doi:10.1016/J.AAP.2016.04.012
60. Zawar I, Franic L, Kotagal P, Knight EP. Exacerbation of eyelid myoclonia in patients with epilepsy and eyelid myoclonia receiving cannabidiol. Epileptic Disord. 2021;23(6):906–910. doi:10.1684/EPD.2021.1338
61. Nguyen AX, Candidate CM, Albert I, Wu Y, Wu AY. Association between cannabis and the eyelids: a comprehensive review. Clin Exp Ophthalmol. 2020;48(2):230–239. doi:10.1111/CEO.13687
62. Hutcheson DM, Tzavara ET, Smadja C, et al. Behavioural and biochemical evidence for signs of abstinence in mice chronically treated with Δ-9-tetrahydrocannabinol. Br J Pharmacol. 1998;125(7):1567–1577. doi:10.1038/SJ.BJP.0702228
63. Aceto MD, Scates SM, Razdan RK, Martin BR. Anandamide, an endogenous cannabinoid, has a very low physical dependence potential. J Pharmacol Exp Ther. 1998;287(2):598–605.
64. Aceto MD, Scates SM, Lowe JA, Martin BR. Dependence on delta 9-tetrahydrocannabinol: studies on precipitated and abrupt withdrawal. J Pharmacol Exp Ther. 1996;278(3):1290–1295.
65. Young AM, Katz JL, Woods JH. Behavioral effects of levonantradol and nantradol in the rhesus monkey. J Clin Pharmacol. 1981;21(S1):348S–360S. doi:10.1002/J.1552-4604.1981.TB02614.X
66. Costa B, Giagnoni G, Colleoni M. Precipitated and spontaneous withdrawal in rats tolerant to anandamide. Psychopharmacology. 2000;149(2):121–128. doi:10.1007/S002139900360
67. Meschler JP, Clarkson FA, Mathews PJ, Howlett AC, Madras BK. D(2), but not D(1) dopamine receptor agonists potentiate cannabinoid-induced sedation in nonhuman primates. J Pharmacol Exp Ther. 2000;292(3):952–959.
68. Beardsley PM, Scimeca JA, Martin BR. Studies on the agonistic activity of delta 9-11-tetrahydrocannabinol in mice, dogs and rhesus monkeys and its interactions with delta 9-tetrahydrocannabinol. J Pharmacol Exp Ther. 1987;241(2):521–526.
69. Colasanti BK, Powell SR, Craig CR. Intraocular pressure, ocular toxicity and neurotoxicity after administration of delta 9-tetrahydrocannabinol or cannabichromene. Exp Eye Res. 1984;38(1):63–71. doi:10.1016/0014-4835(84)90139-8
70. Colasanti BK, Brown RE, Craig CR. Ocular hypotension, ocular toxicity, and neurotoxicity in response to marihuana extract and cannabidiol. Gen Pharmacol. 1984;15(6):479–484. doi:10.1016/0306-3623(84)90202-7
71. Polat N, Cumurcu B, Cumurcu T, Tuncer İ. Corneal endothelial changes in long-term cannabinoid users. Cutan Ocul Toxicol. 2018;37(1):19–23. doi:10.1080/15569527.2017.1322098
72. Pisanti S, Picardi P, Prota L, et al. Genetic and pharmacologic inactivation of cannabinoid CB1 receptor inhibits angiogenesis. Blood. 2011;117(20):5541–5550. doi:10.1182/BLOOD-2010-09-307355
73. Zobor D, Strasser T, Zobor G, et al. Ophthalmological assessment of cannabis-induced persisting perception disorder: is there a direct retinal effect? Documenta Ophthalmologica. 2015;130(2):121–130. doi:10.1007/S10633-015-9481-2
74. Schwitzer T, Schwan R, Albuisson E, et al. Association between regular cannabis use and ganglion cell dysfunction. JAMA Ophthalmol. 2017;135(1):54–60. doi:10.1001/JAMAOPHTHALMOL.2016.4761
75. Pérez JG, Mato MP, García AS, Rey AD. Intraocular motility, electrophysiological tests and visual fields in drug addicts. Ophthalmic Physiol Opt. 1995;15(5):493–498. doi:10.1016/0275-5408(95)00098-X
76. Schwitzer T, Robert MP, Giersch A, et al. Transient retinal dysfunctions after acute cannabis use. Eur Addict Res. 2016;22(6):287–291. doi:10.1159/000446823
77. Faure C, Schwitzer T, Hansen C, Randhawa S. Diagnostic and therapeutic challenges. Retina. 2016;36(12):2433–2439. doi:10.1097/IAE.0000000000000988
78. Onur OS, Sena K, Onur IU, Karşıdağ C. Evaluation of the effects of synthetic cannabinoids (Bonzai) on choroid and retina. Eur Neuropsychopharmacol. 2016;26:S704. doi:10.1016/S0924-977X(16)31840-5
79. Polli L, Schwan R, Albuisson E, et al. Oscillatory potentials abnormalities in regular cannabis users: amacrine cells dysfunction as a marker of central dopaminergic modulation. Prog Neuropsychopharmacol Biol Psychiatry. 2021:108. doi:10.1016/J.PNPBP.2020.110083.
80. Schwitzer T, Schwan R, Angioi-Duprez K, et al. Delayed bipolar and ganglion cells neuroretinal processing in regular cannabis users: the retina as a relevant site to investigate brain synaptic transmission dysfunctions. J Psychiatr Res. 2018;103:75–82. doi:10.1016/J.JPSYCHIRES.2018.04.021
81. Schwitzer T, Schwan R, Albuisson E, et al. Delayed on- and off-retinal responses of cones pathways in regular cannabis users: an on-off flash electroretinogram case-control study. J Psychiatr Res. 2021;136:312–318. doi:10.1016/J.JPSYCHIRES.2021.02.033
82. Schwitzer T, Henrion ML, Sarre D, et al. Spatial localization of retinal anomalies in regular cannabis users: the relevance of the multifocal electroretinogram. Schizophr Res. 2020;219:56–61. doi:10.1016/J.SCHRES.2019.01.013
83. Schwitzer T, Moreno-Zaragoza A, Dramé L, et al. Variations of retinal dysfunctions with the level of cannabis use in regular users: toward a better understanding of cannabis use pathophysiology. Front Psychiatry. 2022:13. doi:10.3389/FPSYT.2022.959347.
84. Zhang Z, Li R, Lu H, Zhang X. Systemic administration with tetrahydrocannabinol causes retinal damage in BALB/c mice. Hum Exp Toxicol. 2020;39(3):290–300. doi:10.1177/0960327119886037
85. Flom MC, Brown B, Adams AJ, Jones RT. Alcohol and marijuana effects on ocular tracking. Am J Optom Physiol Opt. 1976;53(12):764–773. doi:10.1097/00006324-197612000-00003
86. Baloh RW, Sharma S, Moskowitz H, Griffith R. Effect of alcohol and marijuana on eye movements. Aviat Space Environ Med. 1979;50(1):18–23.
87. Adams AJ, Brown B, Flon MC, Jones RT, Jampolsky A. Alcohol and marijuana effects on static visual acuity. Optometry Vision Sci. 1975;52(11):729–735. doi:10.1097/00006324-197511000-00001
88. Fant RV, Heishman SJ, Bunker EB, Pickworth WB. Acute and residual effects of marijuana in humans. Pharmacol Biochem Behav. 1998;60(4):777–784. doi:10.1016/S0091-3057(97)00386-9
89. Huestegge L, Radach R, Kunert HJ. Long-term effects of cannabis on oculomotor function in humans. J Psychopharmacol. 2009;23(6):714–722. doi:10.1177/0269881108091601
90. Huestegge L, Kunert HJ, Radach R. Long-term effects of cannabis on eye movement control in reading. Psychopharmacology. 2010;209(1):77–84. doi:10.1007/S00213-009-1769-Z
91. Mohan H, Sood GC. Conjugate deviation of the eyes after Cannabis indica intoxication. Br J Ophthalmol. 1964;48(3):160–161. doi:10.1136/BJO.48.3.160
92. Moskowitz H, Sharma S, McGlothlin W. Effect of marihuana upon peripheral vision as a function of the information processing demands in central vision. Percept Mot Skills. 1972;35(3):875–882. doi:10.2466/PMS.1972.35.3.875
93. Ploner CJ, Tschirch A, Ostendorf F, et al. Oculomotor effects of delta-9-tetrahydrocannabinol in humans: implications for the functional neuroanatomy of the brain cannabinoid system. Cereb Cortex. 2002;12(10):1016–1023. doi:10.1093/CERCOR/12.10.1016
94. Pradeep A, Thomas S, Roberts EO, Proudlock FA, Gottlob I. Reduction of congenital nystagmus in a patient after smoking cannabis. Strabismus. 2008;16(1):29–32. doi:10.1080/09273970701821063
95. Wurz GT, Montoya E, DeGregorio MW. Examining impairment and kinetic patterns associated with recent use of hemp-derived Δ8-tetrahydrocannabinol: case studies. J Cannabis Res. 2022;4(1). doi:10.1186/S42238-022-00146-9
96. Yoon JH, San Miguel GG, Vincent JN, et al. Assessing attentional bias and inhibitory control in cannabis use disorder using an eye-tracking paradigm with personalized stimuli. Exp Clin Psychopharmacol. 2019;27(6):578–587. doi:10.1037/PHA0000274
97. Zuurman L, Roy C, Schoemaker RC, et al. Effect of intrapulmonary tetrahydrocannabinol administration in humans. J Psychopharmacol. 2008;22(7):707–716. doi:10.1177/0269881108089581
98. Mikulskaya E, Martin FH. Contrast sensitivity and motion discrimination in cannabis users. Psychopharmacology. 2018;235(8):2459–2469. doi:10.1007/S00213-018-4944-2
99. Bosker WM, Theunissen EL, Conen S, et al. A placebo-controlled study to assess standardized field sobriety tests performance during alcohol and cannabis intoxication in heavy cannabis users and accuracy of point of collection testing devices for detecting THC in oral fluid. Psychopharmacology. 2012;223(4):439–446. doi:10.1007/S00213-012-2732-Y
100. Declues K, Perez S, Figueroa A. A two-year study of Δ 9 tetrahydrocannabinol concentrations in drivers; part 2: physiological signs on Drug Recognition Expert (DRE) and non-DRE examinations. J Forensic Sci. 2018;63(2):583–587. doi:10.1111/1556-4029.13550
101. Schon F, Hart PE, Hodgson TL, et al. Suppression of pendular nystagmus by smoking cannabis in a patient with multiple sclerosis. Neurology. 1999;53(9):2209–2209–a. doi:10.1212/WNL.53.9.2209-A
102. Dugar A. Countries where weed is legal in 2023: guide to Cannabis Law by Country. 2023. Available from: https://greenhealthdocs.com/countries-where-weed-is-legal/.
103. Hansen C, Alas H, EJr D. Where is marijuana legal? A guide to marijuana legalization. US News World Rep. 2023;2023:1.
104. World Health Organization. Alcohol, Drugs and Addictive Behaviours. 2023. Available from: https://www.who.int/teams/mental-health-and-substance-use/alcohol-drugs-and-addictive-behaviours/drugs-psychoactive/cannabis.
105. Friedman D, Sirven JI. Historical perspective on the medical use of cannabis for epilepsy: ancient times to the 1980s. Epilepsy Behav. 2017;70:298–301. doi:10.1016/J.YEBEH.2016.11.033
106. Aggarwal SK, Carter GT, Sullivan MD, ZumBrunnen C, Morrill R, Mayer JD. Medicinal use of cannabis in the United States: historical perspectives, current trends, and future directions. J Opioid Manag. 2009;5(3):153–168. doi:10.5055/JOM.2009.0016
107. Fraguas-Sánchez AI, Torres-Suárez AI. Medical use of cannabinoids. Drugs. 2018;78(16):1665–1703. doi:10.1007/S40265-018-0996-1
108. Panel on Research Ethics. TCPS 2 (2022) – chapter 2: scope and Approach. Government of Canada. Availble from: https://ethics.gc.ca/eng/tcps2-eptc2_2022_chapter2-chapitre2.html.
109. Amin MR, Ali DW. Pharmacology of medical cannabis. Adv Exp Med Biol. 2019;1162:151–165. doi:10.1007/978-3-030-21737-2_8
110. Hanuš LO, Meyer SM, Muñoz E, Taglialatela-Scafati O, Appendino G. Phytocannabinoids: a unified critical inventory. Nat Prod Rep. 2016;33(12):1357–1392. doi:10.1039/C6NP00074F
111. Howlett AC, Barth F, Bonner TI, et al. International union of pharmacology. XXVII. Classification of cannabinoid receptors. Pharmacol Rev. 2002;54(2):161–202. doi:10.1124/PR.54.2.161
112. Mackie K. Cannabinoid receptors: where they are and what they do. J Neuroendocrinol. 2008;20(s1):10–14. doi:10.1111/J.1365-2826.2008.01671.X
113. Tsou K, Brown S, Sañudo-Peña MC, Mackie K, Walker JM. Immunohistochemical distribution of cannabinoid CB1 receptors in the rat central nervous system. Neuroscience. 1998;83(2):393–411. doi:10.1016/S0306-4522(97)00436-3
114. Jordan CJ, Xi ZX. Progress in brain cannabinoid CB2 receptor research: from genes to behavior. Neurosci Biobehav Rev. 2019;98:208–220. doi:10.1016/J.NEUBIOREV.2018.12.026
115. Galiègue S, Mary S, Marchand J, et al. Expression of central and peripheral Cannabinoid receptors in human immune tissues and leukocyte subpopulations. Eur J Biochem. 1995;232(1):54–61. doi:10.1111/J.1432-1033.1995.TB20780.X
116. Nyíri G, Cserép C, Szabadits E, Mackie K, Freund TF. CB1 cannabinoid receptors are enriched in the perisynaptic annulus and on preterminal segments of hippocampal GABAergic axons. Neuroscience. 2005;136(3):811–822. doi:10.1016/J.NEUROSCIENCE.2005.01.026
117. Katona I, Urbán GM, Wallace M, et al. Molecular composition of the endocannabinoid system at glutamatergic synapses. J Neurosci. 2006;26(21):5628–5637. doi:10.1523/JNEUROSCI.0309-06.2006
118. Osei-Hyiaman D, DePetrillo M, Pacher P, et al. Endocannabinoid activation at hepatic CB1 receptors stimulates fatty acid synthesis and contributes to diet-induced obesity. J Clin Invest. 2005;115(5):1298–1305. doi:10.1172/JCI23057
119. Cota D. CB1 receptors: emerging evidence for central and peripheral mechanisms that regulate energy balance, metabolism, and cardiovascular health. Diabetes Metab Res Rev. 2007;23(7):507–517. doi:10.1002/DMRR.764
120. Cavuoto P, McAinch AJ, Hatzinikolas G, Janovská A, Game P, Wittert GA. The expression of receptors for endocannabinoids in human and rodent skeletal muscle. Biochem Biophys Res Commun. 2007;364(1):105–110. doi:10.1016/J.BBRC.2007.09.099
121. Cota D, Marsicano G, Tschöp M, et al. The endogenous cannabinoid system affects energy balance via central orexigenic drive and peripheral lipogenesis. J Clin Investig. 2003;112(3):423–431. doi:10.1172/JCI17725
122. Van Sickle MD, Duncan M, Kingsley PJ, et al. Identification and functional characterization of brainstem cannabinoid CB 2 receptors. Science. 2005;310(5746):329–332. doi:10.1126/science.1115740
123. Ofek O, Karsak M, Leclerc N, et al. Peripheral cannabinoid receptor, CB2, regulates bone mass. PNAS. 2006;103(3):696–701. doi:10.1073/pnas.0504187103
124. Oz M. Receptor-independent effects of endocannabinoids on ion channels. Curr Pharm Des. 2005;12(2):227–239. doi:10.2174/138161206775193073
125. Straiker A, Mackie K. Cannabinoids, electrophysiology, and retrograde messengers: challenges for the next 5 years. AAPS J. 2006;8(2):E272–E276. doi:10.1007/BF02854897
126. Urban JD, Clarke WP, Von Zastrow M, et al. Functional selectivity and classical concepts of quantitative pharmacology. J Pharmacol Exp Ther. 2007;320(1):1–13. doi:10.1124/JPET.106.104463
127. Vásquez C, Lewis DL. The CB1 cannabinoid receptor can sequester G-proteins, making them unavailable to couple to other receptors. J Neurosci. 1999;19(21):9271–9280. doi:10.1523/JNEUROSCI.19-21-09271.1999
128. Fitzcharles MA, Petzke F, Tölle TR, Häuser W. Cannabis-based medicines and medical cannabis in the treatment of nociplastic pain. Drugs. 2021;81(18):2103–2116. doi:10.1007/S40265-021-01602-1
129. Freeman TP, Hindocha C, Green SF, Bloomfield MAP. Medicinal use of cannabis based products and cannabinoids. BMJ. 2019;365. doi:10.1136/BMJ.L1141.
130. Pavlovic R, Nenna G, Calvi L, et al. Quality traits of “cannabidiol oils”: cannabinoids content, terpene fingerprint and oxidation stability of European commercially available preparations. Molecules. 2018;23(5):1230. doi:10.3390/molecules23051230
131. Hazekamp A. The trouble with CBD oil. Med Cannabis Cannabinoids. 2018;1(1):65–72. doi:10.1159/000489287
132. Spindle TR, Sholler DJ, Cone EJ, et al. Cannabinoid content and label accuracy of hemp-derived topical products available online and at national retail stores. JAMA Netw Open. 2022;5(7):e2223019. doi:10.1001/jamanetworkopen.2022.23019
133. Vandrey R, Raber JC, Raber ME, Douglass B, Miller C, Bonn-Miller MO. Cannabinoid dose and label accuracy in edible medical cannabis products. JAMA. 2015;313(24):2491–2493. doi:10.1001/jama.2015.6613
134. Sexton M, Cuttler C, Finnell JS, Mischley LK. A cross-sectional survey of medical cannabis users: patterns of use and perceived efficacy. Cannabis Cannabinoid Res. 2016;1(1):131–138. doi:10.1089/can.2016.0007
135. Maguire RF, Wilkinson DJ, England TJ, O’Sullivan SE. The pharmacological effects of plant-derived versus synthetic cannabidiol in human cell lines. Med Cannabis Cannabinoids. 2021;4(2):86–96. doi:10.1159/000517120
136. Martin JH, Schneider J, Lucas CJ, Galettis P. Exogenous cannabinoid efficacy: merely a pharmacokinetic interaction? Clin Pharmacokinet. 2018;57(5):539–545. doi:10.1007/s40262-017-0599-0
137. Zhu HJ, Wang JS, Markowitz JS, et al. Characterization of P-glycoprotein inhibition by major cannabinoids from marijuana. J Pharmacol Exp Ther. 2006;317(2):850–857. doi:10.1124/JPET.105.098541
138. Jiang R, Yamaori S, Okamoto Y, Yamamoto I, Watanabe K. Cannabidiol is a potent inhibitor of the catalytic activity of cytochrome P450 2C19. Drug Metab Pharmacokinet. 2013;28(4):332–338. doi:10.2133/DMPK.DMPK-12-RG-129
139. Anderson GD, Chan LN. Pharmacokinetic drug interactions with tobacco, cannabinoids and smoking cessation products. Clin Pharmacokinet. 2016;55(11):1353–1368. doi:10.1007/S40262-016-0400-9
140. Cohen K, Weizman A, Weinstein A. Positive and negative effects of cannabis and cannabinoids on health. Clin Pharmacol Ther. 2019;105(5):1139–1147. doi:10.1002/CPT.1381
141. MacCallum CA, Lo LA, Boivin M. “Is medical cannabis safe for my patients?” A practical review of cannabis safety considerations. Eur J Intern Med. 2021;89:10–18. doi:10.1016/J.EJIM.2021.05.002
142. Straiker A, Maguire G, Mackie K, Lindsey J. Localization of cannabinoid CB1 receptors in the human anterior eye and retina. Invest Ophthalmol Vis Sci. 1999;40(10):2442–2448.
143. Wang MTM, Danesh-Meyer HV. Cannabinoids and the eye. Surv Ophthalmol. 2021;66(2):327–345. doi:10.1016/J.SURVOPHTHAL.2020.07.002
144. Nguyen AX, Wu AY. Cannabis and the cornea: a comprehensive review. Ocul Immunol Inflamm. 2021;29(5):1023. doi:10.1080/09273948.2020.1726969
145. Skaper SD, Buriani A, Dal Toso R, et al. The ALIAmide palmitoylethanolamide and cannabinoids, but not anandamide, are protective in a delayed postglutamate paradigm of excitotoxic death in cerebellar granule neurons. Proc Natl Acad Sci. 1996;93(9):3984–3989. doi:10.1073/pnas.93.9.3984
146. Richardson P, Ortori C, Barrett D, O’Sullivan S, Idris I. Endocannabinoids in aqueous humour of patients with or without diabetes. BMJ Open Ophthalmol. 2020;5(1):e000425. doi:10.1136/BMJOPHTH-2019-000425
147. Saraiva SM, Martín-Banderas L, Durán-Lobato M. Cannabinoid-based ocular therapies and formulations. Pharmaceutics. 2023;15(4):1077. doi:10.3390/PHARMACEUTICS15041077
148. Hughes PM, Olejnik O, Chang-Lin JE, Wilson CG. Topical and systemic drug delivery to the posterior segments. Adv Drug Deliv Rev. 2005;57(14):2010–2032. doi:10.1016/J.ADDR.2005.09.004
149. Bonilla L, Espina M, Severino P, et al. Lipid nanoparticles for the posterior eye segment. Pharmaceutics. 2021;14(1):90. doi:10.3390/PHARMACEUTICS14010090
150. Occhiutto ML, Freitas FR, Maranhao RC, Costa VP. Breakdown of the blood-ocular barrier as a strategy for the systemic use of nanosystems. Pharmaceutics. 2012;4(2):252–275. doi:10.3390/PHARMACEUTICS4020252
151. Saraiva SM, Castro-López V, Pañeda C, Alonso MJ. Synthetic nanocarriers for the delivery of polynucleotides to the eye. Eur J Pharm Sci. 2017;103:5–18. doi:10.1016/J.EJPS.2017.03.001
152. Sánchez-López E, Espina M, Doktorovova S, Souto EB, García ML. Lipid nanoparticles (SLN, NLC): overcoming the anatomical and physiological barriers of the eye - Part I - Barriers and determining factors in ocular delivery. Eur J Pharm Biopharm. 2017;110:70–75. doi:10.1016/J.EJPB.2016.10.009
153. Leblanc B, Jezequel S, Davies T, Hanton G, Taradach C. Binding of drugs to eye melanin is not predictive of ocular toxicity. Regul Toxicol Pharmacol. 1998;28(2):124–132. doi:10.1006/RTPH.1998.1243
154. Ameeduzzafar A, Ali J, Fazil M, Qumbar M, Khan N, Ali A. Colloidal drug delivery system: amplify the ocular delivery. Drug Deliv. 2014;23(3):710–726. doi:10.3109/10717544.2014.923065
155. Barar J, Javadzadeh AR, Omidi Y. Ocular novel drug delivery: impacts of membranes and barriers. Expert Opin Drug Deliv. 2008;5(5):567–581. doi:10.1517/17425247.5.5.567
156. Ghate D, Edelhauser HF. Ocular drug delivery. Expert Opin Drug Deliv. 2006;3(2):275–287. doi:10.1517/17425247.3.2.275
157. Zantut PRA, Veras MM, Benevenutto SGM, et al. Lasting effects of prenatal exposure to Cannabis in the retina of the offspring: an experimental study in mice. Int J Retina Vitreous. 2021;7(1):1–11. doi:10.1186/s40942-021-00314-8
158. Auger N, Rhéaume MA, Low N, Lee GE, Ayoub A, Luu TM. Impact of prenatal exposure to opioids, cocaine, and cannabis on eye disorders in children. J Addict Med. 2020;14(6):459–466. doi:10.1097/ADM.0000000000000621
159. Hamilton R, McGlone L, MacKinnon JR, Russell HC, Bradnam MS, Mactier H. Ophthalmic, clinical and visual electrophysiological findings in children born to mothers prescribed substitute methadone in pregnancy. Br J Ophthalmol. 2010;94(6):696–700. doi:10.1136/BJO.2009.169284
160. Bramness JG, Khiabani HZ, Mørland J. Impairment due to cannabis and ethanol: clinical signs and additive effects. Addiction. 2010;105(6):1080–1087. doi:10.1111/J.1360-0443.2010.02911.X
161. Richter JS, Quenardelle V, Rouyer O, et al. A systematic review of the complex effects of cannabinoids on cerebral and peripheral circulation in animal models. Front Physiol. 2018;9:622. doi:10.3389/FPHYS.2018.00622/FULL
162. Thayer A, Murataeva N, Delcroix V, Wager-Miller J, Makarenkova HP, Straiker A. THC regulates tearing via cannabinoid CB1 receptors. Invest Ophthalmol Vis Sci. 2020;61(10):48. doi:10.1167/IOVS.61.10.48
163. Tran BN, Maass M, Musial G, Stern ME, Gehlsen U, Steven P. Topical application of cannabinoid-ligands ameliorates experimental dry-eye disease. Ocul Surf. 2022;23:131–139. doi:10.1016/J.JTOS.2021.12.008
164. Russo EB, Cuttler C, Cooper ZD, Stueber A, Whiteley VL, Sexton M. Survey of patients employing cannabigerol-predominant cannabis preparations: perceived medical effects, adverse events, and withdrawal symptoms. Cannabis Cannabinoid Res. 2022;7(5):706–716. doi:10.1089/CAN.2021.0058
165. Ware MA, Wang T, Shapiro S, et al. Smoked cannabis for chronic neuropathic pain: a randomized controlled trial. CMAJ. 2010;182(14):E694–E701. doi:10.1503/CMAJ.091414
166. Fabre LF, McLendon D. The efficacy and safety of nabilone (a synthetic cannabinoid) in the treatment of anxiety. J Clin Pharmacol. 1981;21(S1):377S–382S. doi:10.1002/J.1552-4604.1981.TB02617.X
167. Colasanti BK. Intraocular pressure, ocular toxicity and neurotoxicity in response to 11-hydroxy-Δ 9 -tetrahydrocannabinol and 1-nantradol. J Ocul Pharmacol. 1985;1(2):123–135. doi:10.1089/JOP.1985.1.123
168. Yang Y, Yang H, Wang Z, et al. Cannabinoid receptor 1 suppresses transient receptor potential vanilloid 1-induced inflammatory responses to corneal injury. Cell Signal. 2013;25(2):501–511. doi:10.1016/J.CELLSIG.2012.10.015
169. Campobasso CP, De Micco F, Corbi G, et al. Pupillary effects in habitual cannabis consumers quantified with pupillography. Forensic Sci Int. 2020;317:110559. doi:10.1016/J.FORSCIINT.2020.110559
170. Selden BS, Clark RF, Curry SC. Marijuana. Emerg Med Clin North Am. 1990;8(3):527–539. doi:10.1016/S0733-8627(20)30257-1
171. Kepler RS, Frank IM, Ungerleider JT. Pupillary constriction after marijuana smoking. Am J Ophthalmol. 1972;74(6):1185–1190. doi:10.1016/0002-9394(72)90741-6
172. Dawson W, Jiménez-Antillon C, Perez J, Zeskind J. Marijuana and vision--after ten years’ use in Costa Rica. Invest Ophthalmol Vis Sci. 1977;16(8):689–699.
173. Bouskila J, Harrar V, Javadi P, et al. Scotopic vision in the monkey is modulated by the G protein-coupled receptor 55. Vis Neurosci. 2016;33:E006. doi:10.1017/S095252381600002X
174. Miraucourt LS, Tsui J, Gobert D, et al. Endocannabinoid signaling enhances visual responses through modulation of intracellular chloride levels in retinal ganglion cells. Elife. 2016;5:e15932. doi:10.7554/eLife.15932
175. Russo EB, Merzouki A, Mesa JM, Frey KA, Bach PJ. Cannabis improves night vision: a case study of dark adaptometry and scotopic sensitivity in kif smokers of the Rif mountains of northern Morocco. J Ethnopharmacol. 2004;93(1):99–104. doi:10.1016/j.jep.2004.03.029
176. West ME. Cannabis and night vision. Nature. 1991;351(6329):703–704. doi:10.1038/351703b0
177. Merzouki A, Mesa JM. Concerning kif, a Cannabis sativa L. preparation smoked in the Rif mountains of northern Morocco. J Ethnopharmacol. 2002;81(3):403–406. doi:10.1016/S0378-8741(02)00119-8
178. Ortiz-Peregrina S, Brown B, Flon MC, Jones RT, Anera RG. Effects of cannabis on visual function and self-perceived visual quality. Sci Rep. 2021;11(1):1–11. doi:10.1038/s41598-021-81070-5
179. Casares-López M, Ortiz-Peregrina S, Castro-Torres JJ, Ortiz C, Martino F, Jiménez JR. Assessing the influence of cannabis and alcohol use on different visual functions: a comparative study. Exp Eye Res. 2022;224:109231. doi:10.1016/J.EXER.2022.109231
180. Brown B, Adams AJ, Haegerstrom-Portnoy G, Jones RT, Flom MC. Effects of alcohol and marijuana on dynamic visual acuity: i. Percept Psychophys. 1975;18(6):441–446. doi:10.3758/BF03204118/METRICS
181. Noyes R, Brunk SF, Avery DH, Canter A. The analgesic properties of delta-9-tetrahydrocannabinol and codeine. Clin Pharmacol Ther. 1975;18(1):84–89. doi:10.1002/CPT197518184
182. Lalanne L, Ferrand-Devouge E, Kirchherr S, et al. Impaired contrast sensitivity at low spatial frequency in cannabis users with early onset. Eur Neuropsychopharmacol. 2017;27(12):1289–1297. doi:10.1016/J.EURONEURO.2017.09.006
183. Ramtohul P, Freund KB, Sarraf D. Branch retinal artery occlusion with paracentral acute middle maculopathy presumably related to heavy cannabis use. Retin Cases Brief Rep. 2022;16(4):403–406. doi:10.1097/ICB.0000000000001051
184. Su EN, Kelly ME, Cringle SJ, Yu DY. Role of endothelium in abnormal cannabidiol-induced vasoactivity in retinal arterioles. Invest Ophthalmol Vis Sci. 2015;56(6):4029–4037. doi:10.1167/IOVS.14-14879
185. Araújo DSM, Miya-Coreixas VS, Pandolfo P, Calaza KC. Cannabinoid receptors and TRPA1 on neuroprotection in a model of retinal ischemia. Exp Eye Res. 2017;154:116–125. doi:10.1016/J.EXER.2016.11.015
186. Why you have that pesky eye twitch — and when to seek help. 2021. Available from: https://health.clevelandclinic.org/why-you-have-that-pesky-eye-twitch-and-when-to-seek-help/.
187. Finsterer J. Ptosis: causes, presentation, and management. Aesthetic Plast Surg. 2003;27(3):193–204. doi:10.1007/s00266-003-0127-5
188. Matias I, Wang JW, Moriello AS, Nieves A, Woodward DF, Di Marzo V. Changes in endocannabinoid and palmitoylethanolamide levels in eye tissues of patients with diabetic retinopathy and age-related macular degeneration. Prostaglandins Leukot Essent Fatty Acids. 2006;75(6):413–418. doi:10.1016/J.PLEFA.2006.08.002
189. Chase PB, Hawkins J, Mosier J, et al. Differential physiological and behavioral cues observed in individuals smoking botanical marijuana versus synthetic cannabinoid drugs. Clin Toxicol. 2016;54(1):14–19. doi:10.3109/15563650.2015.1101769
190. DeGregorio MW, Wurz GT, Montoya E, Kao CJ. A comprehensive breath test that confirms recent use of inhaled cannabis within the impairment window. Sci Rep. 2021;11(1):11. doi:10.1038/S41598-021-02137-X
191. Moskowitz H, Ziedman K, Sharma S. Visual search behavior while viewing driving scenes under the influence of alcohol and marihuana. Hum Fact. 1976;18(5):417–431. doi:10.1177/001872087601800501
192. Emrich HM, Weber MM, Wendl A, Zihl J, Von Meyer L, Hanisch W. Reduced binocular depth inversion as an indicator of cannabis-induced censorship impairment. Pharmacol Biochem Behav. 1991;40(3):689–690. doi:10.1016/0091-3057(91)90383-D
193. Semple DM, Ramsden F, McIntosh AM. Reduced binocular depth inversion in regular cannabis users. Pharmacol Biochem Behav. 2003;75(4):789–793. doi:10.1016/S0091-3057(03)00140-0
194. Ricciardo S, Hastings S. Fatal thyroid storm in the setting of untreated graves disease and use of the synthetic cannabinoid MDMB-4en-PINACA. Am J Forensic Med Pathol. 2023;44(3):223–226. doi:10.1097/PAF.0000000000000852
195. Williams KA, Klebe S. Gene therapy for corneal dystrophies and disease, where are we? Curr Opin Ophthalmol. 2012;23(4):276–279. doi:10.1097/ICU.0B013E3283541EB6
196. Scuteri D, Rombolà L, Hamamura K, et al. Is there a rational basis for cannabinoids research and development in ocular pain therapy? A systematic review of preclinical evidence. Biomed Pharmacother. 2022;146:112505. doi:10.1016/J.BIOPHA.2021.112505
197. Assimakopoulou M, Pagoulatos D, Nterma P, Pharmakakis N. Immunolocalization of cannabinoid receptor type 1 and CB2 cannabinoid receptors, and transient receptor potential vanilloid channels in pterygium. Mol Med Rep. 2017;16(4):5285–5293. doi:10.3892/MMR.2017.7246
198. El-Remessy AB, Tang Y, Zhu G, et al. Neuroprotective effects of cannabidiol in endotoxin-induced uveitis: critical role of p38 MAPK activation. Mol Vis. 2014;20:1227.
199. Passani A, Posarelli C, Sframeli AT, et al. Cannabinoids in glaucoma patients: the never-ending story. J Clin Med. 2020;9(12):1–20. doi:10.3390/JCM9123978
200. Lieberman MF. “Recredicinal” marijuana. Am J Ophthalmol. 2017;177:PXV–XVIII. doi:10.1016/J.AJO.2017.03.006
201. Kaufman PL. Marijuana and glaucoma. Arch Ophthalmol. 1998;116(11):1512–1513. doi:10.1001/ARCHOPHT.116.11.1512
202. Jampel H. American glaucoma society position statement: marijuana and the treatment of glaucoma. J Glaucoma. 2010;19(2):75–76. doi:10.1097/IJG.0B013E3181D12E39
203. Novack GD. Cannabinoids for treatment of glaucoma. Curr Opin Ophthalmol. 2016;27(2):146–150. doi:10.1097/ICU.0000000000000242
204. Rafuse P, Buys YM. Medical use of cannabis for glaucoma. Can J Ophthalmol. 2019;54(1):7–8. doi:10.1016/j.jcjo.2018.11.001
205. National Academies of Sciences E and MH and MDB on PH and PHPC on the HE of MAER and RA. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. Vol. 15. Washington: The National Academies Press; 2017. doi:10.17226/24625
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.