")
Back to Journals » Journal of Pain Research » Volume 18
Analysis and 15-Year Projections of the Global Burden of Tension-Type Headache by Sex from 1990 to 2021: A Systematic Review of GBD 2021 Data
Authors Xu H, Qin X, Zhao G, Feng Z, You S
Received 15 December 2024
Accepted for publication 7 July 2025
Published 10 July 2025 Volume 2025:18 Pages 3505—3517
DOI https://doi.org/10.2147/JPR.S512335
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rune Häckert Christensen
Hongli Xu,1,* Xiaoyan Qin,2,* Guoli Zhao,3 Zeguo Feng,3 Shaohua You3
1Medical Big Data Research Center, Medical Innovation Research Department of PLA General Hospital, Beijing, 100853, People’s Republic of China; 2Department of Clinical Laboratory, Shijingshan teaching hospital of Capital Medical University, Beijing shijingshan Hospital, Beijing, 100049, People’s Republic of China; 3Department of Pain Medicine, The First Medical Center of Chinese PLA General Hospital, Beijing, 100853, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shaohua You, Department of Pain Medicine, The First Medical Center of Chinese PLA General Hospital, Beijing, 100853, People’s Republic of China, Email [email protected]
Background: Tension-type headache (TTH) is a prevalent primary headache disorder significantly impacting quality of life and healthcare resource utilization, with females typically bearing a higher disease burden. However, comprehensive analyses and predictive studies on the global TTH burden stratified by gender are currently lacking.
Aim: This study utilized data from the Global Burden of Disease (GBD) Study to analyze the global burden of tension - type headache by sex from 1990 to 2021 and conducted a 15 - year projection (up to 2036).
Methods: We conducted a systematic review of GBD 2021 data, employing Joinpoint regression analysis and decomposition analysis to assess TTH incidence, prevalence, YLDs, and DALYs. Additionally, we used the ARIMA model for a 15-year predictive analysis of TTH burden trends.
Results: From 1990 to 2021, global female TTH cases rose from 669.54 million (95% UI: 586.2– 751.8 million) to 1.04 billion (95% UI: 923.0– 1.1 billion), with incidence increasing from 242.9 million (95% UI: 218.8– 267.0 million) to 369.86 million (95% UI: 332.5– 407.2 million). Male cases grew from 616.82 million (95% UI: 537.2– 696.4 million) to 970 million (95% UI: 851.0– 1.0 billion). Decomposition analysis indicated population growth was the primary driver of the increase in female TTH prevalence. Projections suggest that by 2036, the incidence will reach 9,174.84 per 100,000 females (95% UI: 8,854.8– 9,494.9), prevalence will be 25,135.1 per 100,000 females (95% UI: 23,977.2– 26,283.0), YLD rate will be 62.76 per 100,000 females (95% UI: 58.8– 66.7), and DALY rate will be 60.97 per 100,000 females (95% UI: 56.7– 65.2).
Conclusion: This study highlights the significance of gender in TTH burden, particularly the heightened risk for females. Through temporal trend analysis and predictive modeling, we provide insights into future TTH disease trajectories, aiding global public health policy formulation and healthcare resource allocation.
Keywords: tension-type headache, gender differences, disease burden decomposition, joinpoint regression analysis, epidemiological trends, predictive modeling
Introduction
Tension-Type Headache (TTH), a highly prevalent primary headache, is characterized by bilateral, pressing, or constricting pain without accompanying symptoms such as photophobia, phonophobia, or nausea.1 The pain intensity associated with TTH is typically mild to moderate,2 making it the most common yet frequently overlooked primary headache. However, TTH has a significant impact on patients’ quality of life, work efficiency, and utilization of medical resources, posing a substantial public health issue.3 An estimated 882.4 million new cases of TTH were reported globally in 2017.4 The lifetime prevalence of TTH ranges from 30% to 78%,5,6 making it a major health issue affecting individuals across all age groups and socioeconomic strata.
Significant gender disparities exist in the disease burden of TTH. This phenomenon has been documented in various studies, with female patients consistently reporting higher prevalence rates compared to males.1,4,7 In 2016, the global age-standardized prevalence rates for TTH were 30.8% (28.0 to 34.0) for women and 21.4% (19.2 to 23.9) for men.8 These disparities may be attributable to several factors, including hormonal, psychological, and socio-cultural differences.9 A population-based survey indicated that hormonal changes, particularly during menstruation, significantly trigger headaches in women, a correlation less pronounced in men.10 Additional research has shown that women with TTH frequently report higher levels of anxiety and depression, which may exacerbate headache symptoms and overall disability.11 Moreover, women exhibit a greater number of active trigger points and lower pain thresholds, suggesting increased sensitivity to pain.12 The impact of TTH on work efficiency and overall quality of life is substantial, particularly for women, who often report decreased work productivity due to headaches. This underscores the socio-economic implications of TTH, especially for women who may already face additional challenges in the workplace.13,14 The unequal burden of TTH among women highlights the necessity of adopting gender-sensitive approaches in research, clinical practice, and public health policies.
Over the past three decades, a substantial body of research has advanced our understanding of the epidemiology of TTH. However, the long - term trends in the disease burden of TTH, particularly among women, remain inadequately described. Moreover, no scholars have predicted the future disease burden of TTH. This lack of knowledge hinders our ability to formulate effective and targeted interventions that can alleviate the global burden of TTH.
Against this backdrop, this study utilizes data from the Global Burden of Disease (GBD) Study, a comprehensive resource for the systematic collection of epidemiological data.15 The GBD database we rely on employs well - recognized diagnostic criteria for the diagnosis of tension - type headaches to distinguish them from other types of primary headaches, such as migraines and cluster headaches. The aim is to investigate the long - term trends in the global burden of TTH from 1990 to 2021. By examining the incidence, prevalence, years lived with disability (YLD), and disability - adjusted life years (DALY), and disaggregating these indicators by sex, this study intends to provide a broad overview of the changes in the disease burden of TTH. Specifically, this study focuses on the TTH burden among women and the prediction of the disease burden over the next 15 years. It aims to elucidate the profound impact of gender differences on the disease and to inform the development of more targeted prevention and treatment strategies.
Methods
Overview
The GBD 2021 analysis of disease and injury burden utilized 100,983 data sources from 204 countries and territories to estimate the most recent information on DALYs, years of life lost (YLLs), YLDs and healthy life expectancy for 371 diseases and injuries.16 Data were gathered from vital registration systems, verbal autopsies, censuses, household surveys, disease-specific registries, health service contact data, and various other sources.17 The Global Health Data Exchange GBD Results Tool was used to gather data on the global TTH burden from 1990 to 2021. The GBD study provides all age-standardized rates, age-specific rates, and data with 95% uncertainty intervals (UI).
The Ethics Committee of the First Medical Center of the Chinese PLA General Hospital determined that approval for this study was not required, as the GBD disease burden data used in this study are publicly accessible at https://vizhub.healthdata.org/gbd-results/.
Joinpoint Regression Analysis
The joinpoint regression model, a set of linear statistical models, was used to evaluate temporal trends in the global disease burden of TTH. The Joinpoint software (version 4.9.1.0; National Cancer Institute, Rockville, MD, USA) was employed to construct this model. In this study, the annual percentage change (APC) and the average annual percentage change (AAPC) were applied to analyze the incidence, prevalence, YLDs, and DALYs rates of TTH. An APC > 0 indicates that the incidence, prevalence, YLDs, or DALYs rates of TTH have increased over time in the current period; an APC < 0 signifies that these rates have decreased over time; and an APC = 0 suggests no temporal change in these rates. Similarly, an AAPC > 0 indicates that the incidence, prevalence, YLDs, or DALYs rates of TTH have increased over the entire period; an AAPC < 0 shows a decrease over the entire period; and when AAPC = APC, it suggests a monotonic increase or decrease in the incidence, prevalence, YLDs, or DALYs rates of TTH. Statistical significance was defined as a P value of less than 0.05.
Decomposition Analysis
We performed a decomposition analysis to thoroughly assess the contributions to the increase in the incidence, prevalence, YLDs, or DALYs from TTH from 1990 to 2021. These determinants include the impacts of population growth, population aging, and epidemiological changes. Epidemiological changes refer to the age- and population-adjusted mortality and incidence rates at the foundational level.
Predicted Analysis
The ARIMA forecasting model was utilized to predict data for the 15 years following 2021. The ARIMA (p, d, q) model, commonly referred to as the Autoregressive Integrated Moving Average model, comprises three key components: AR (autoregression) where p represents the number of autoregressive terms, d (differencing) which indicates the order of differencing required to achieve stationarity in the time series, and MA (moving average) where q denotes the number of moving average terms.18
To ensure the validity and reliability of the ARIMA models used in this study, several steps were taken to verify the underlying assumptions of the models. Firstly, the assumption of stationarity was rigorously tested using the Augmented Dickey-Fuller (ADF) test. The ADF test results confirmed that the time series data became stationary after applying the appropriate differencing order (d) as recommended by the auto.arima() function. This step is crucial as ARIMA models require the time series to be stationary for accurate forecasting. Secondly, to validate the adequacy of the fitted ARIMA models, we carefully examined the autocorrelation function (ACF) and partial autocorrelation function (PACF) plots of the model residuals. The analysis of these plots revealed no significant remaining autocorrelations, providing strong evidence that the models had successfully captured the underlying patterns and structures within the data. The modeling process involved the use of time series analysis to capture the temporal dynamics of age-standardized rates. This was efficiently carried out using the auto.arima() function from the forecast package in R. The auto.arima() function is particularly useful as it automatically identifies the most suitable ARIMA model by selecting the optimal differencing order, autoregressive terms, and moving average terms that minimize the Akaike Information Criterion (AIC) or another specified criterion. This automated approach ensures that the best possible model is chosen for the data at hand.
For the purpose of fitting the ARIMA models and generating forecasts, we employed the “forecast” package (version 8.23.0) in R (version 4.4.2, available at http://www.r-project.org). The combination of these tools provided a robust framework for our time series analysis and forecasting efforts.
Result
Descriptive Analysis
Table 1 presents comprehensive epidemiological data on TTH for the global population in 2021, encompassing prevalence, incidence, YLDs and DALYs, stratified by gender. Globally, the total number of TTH cases was 2.01 billion (95% UI 1.78 to 2.27), with women accounting for 1.04 billion (95% UI 0.92 to 1.18) and men for 0.97 billion (95% UI 0.85 to 1.10). The age-standardized prevalence rates per 100,000 were 24,764.77 (95% UI 21,863.62 to 27,954.74) globally, 25,634.41 (95% UI 22,631.48 to 28,974.28) among women, and 23,880.79 (95% UI 21,046.24 to 26,935.06) among men. Incidence data also indicated higher rates among women compared to men, both in absolute numbers and age-standardized rates. Notably, since no deaths were attributed to headache as the primary cause, YLDs were equivalent to DALYs. The burden of DALYs and YLDs was slightly higher in women. Globally, the total DALYs due to TTH were 4,596,785 (95% UI 1,347,301 to 15,012,933), with women contributing 2,567,597 (95% UI 788,725 to 7,674,299) and men 2,029,188 (95% UI 558,294 to 7,054,295). The age-standardized DALYs per 100,000 were 55.69 (95% UI 16.13 to 185.07) globally, 62 (95% UI 18.8 to 189.03) among women, and 49.35 (95% UI 13.44 to 172.38) among men.
 |
Table 1 2021 Global Burden of TTH by Sex: Prevalence, Incidence, YLDs and DALYs |
The prevalence, incidence, YLDs, and DALYs of TTH exhibit variations across different age groups, with gender-specific differences observed. Notably, the disease burden is consistently higher in women across all age stages. The incidence of TTH among women and men show bimodal age distributions, peaking at ages 10–14 and 25–29 for both genders. The prevalence, however, exhibits a unimodal distribution, reaching its peak at ages 30–34 for both men and women. The DALY numbers also follow a unimodal age distribution, peaking at ages 35–39. Figure 1 illustrates the prevalence, incidence, YLDs and DALYs of TTH among women and men across different age groups in 2021, represented in both absolute numbers (A, C, E, G) and age-standardized rates (B, D, F, H).
 |
Figure 1 Global Prevalence, Incidence, YLD, and DALY of TTH in 2021 by Gender.(A) prevalence; (B) ASPR; (C) incidence; (D) ASIR; (E) YLDs; (F) AS-YLD; (G) DALYs; (H) ASDR. Abbreviations: TTH, tension-type headache; YLDs, years lived with disability; DALYs, disability-adjusted life-years; ASPR, Age-Standardized Prevalence Rate; ASIR, Age-Standardized Incidence Rate; AS-YLD, Age-Standardized Years Lived with Disability; ASDR, age-standardized DALY rate. |
The study results indicate that the global burden of TTH has been on an upward trend from 1990 to 2021, with women constantly bearing a higher burden than men. Detailed age-specific data are provided in Tables S1–S4. Notably, the number of women affected by TTH increased from 669.54 million (95% UI: 586.17 to 763.31 million) in 1990 to 1.04 billion (95% UI: 0.92 to 1.18 billion) in 2021. Similarly, the number of affected men rose from 616.82 million (95% UI: 537.23 to 705.26 million) to 0.97 billion (95% UI: 0.85 to 1.10 billion). In terms of incidence, the number of new female cases grew from 242.94 million (95% UI: 211.83 to 272.39 million) to 369.86 million (95% UI: 324.50 to 413.11 million), while for men, it increased from 227.36 million (95% UI: 197.20 to 255.92 million) to 349.19 million (95% UI: 3.04 to 39.03 billion). Since there are no deaths directly attributable to TTH, YLD is equivalent to DALY. Women’s YLD increased from 1,598,918 (95% UI: 484,063 to 4,995,532) to 2,567,597 (95% UI: 788,725 to 7,674,299), and men’s from 1,249,770 (95% UI: 336,750 to 4,481,443) to 2,029,188 (95% UI: 558,294.1 to 7,054,295). Figure 2 illustrates the trends in the burden of TTH in women and men globally from 1990 to 2021, including all age data and age-standardized rates of prevalence, incidence, YLD, and DALY.
 |
Figure 2 Trends in the global burden of TTH among men and women from 1990 to 2021.(A) prevalence; (B) incidence; (C) YLDs; (D) DALYs. Abbreviations: TTH, tension-type headache; YLDs, years lived with disability; DALYs, disability-adjusted life-years; ASPR, Age-Standardized Prevalence Rate; ASIR, Age-Standardized Incidence Rate; AS-YLD, Age-Standardized Years Lived with Disability; ASDR, age-standardized DALY rate. |
Joinpoint Regression Analysis
Joinpoint regression analysis reveals that the global burden of TTH from 1990 to 2021 exhibited significant disparities and fluctuations across different genders and periods. The age-standardized incidence rate data indicates that among females, a marked decrease occurred from 1990 to 2001, with an APC of −0.18 (95% confidence interval [CI]: −0.19 to −0.16). Subsequently, from 2001 to 2017, the decline decelerated to −0.10 (95% CI: −0.11 to −0.10), followed by a slight upward trend from 2017 to 2021, with an APC of 0.07 (95% CI: 0.02 to 0.13). The AAPC overall was −0.11 (95% CI: −0.11 to −0.10). In contrast, for males from 1990 to 2021, the age-standardized incidence rate showed greater volatility, yet maintained a relatively stable decreasing trend with an overall AAPC of −0.02 (95% CI: −0.04 to −0.01). Regarding the age-standardized prevalence rate, females experienced an APC fluctuating from −0.10 to 0.12 across different periods, resulting in an overall AAPC of −0.04 (95% CI: −0.05 to −0.03), indicating a slight downward trend. Males, on the other hand, saw their prevalence rate APC vary from −0.08 to 0.26, with an overall AAPC of 0.02 (95% CI: 0.00 to 0.03), signifying a slight upward trend. The data on age-standardized YLDs shows that females had an APC ranging from −0.18 to 0.07 across different periods, yielding an overall AAPC of −0.11 (95% CI: −0.11 to −0.10), reflecting a marked decrease. Conversely, males exhibited an APC from −0.08 to 0.12, with an overall AAPC of −0.02 (95% CI: −0.04 to −0.01), indicating a relatively stable decrease. Lastly, concerning the age-standardized DALYs, females had an APC fluctuating from −0.07 to 0.12 across different periods, resulting in an overall AAPC of −0.03 (95% CI: −0.04 to −0.02), indicating a slight downward trend. Males, however, saw their DALYs APC vary from −0.05 to 0.24, with an overall AAPC of 0.02 (95% CI: 0.01 to 0.03), signifying a slight upward trend. The detailed results of the Joinpoint regression analysis are presented in Tables S5 and S6 and Figures S1–S12.
Decomposition Analysis of TTH Burden
Decomposition analysis reveals a significant increase in the global burden of TTH, as measured by prevalence, incidence, YLD, and DALY, from 1990 to 2021. Regarding prevalence, the increase among females (1,124,741.3) was notably higher than among males (888,409.3). This increase in females was predominantly driven by population growth (2,511,679, 223.31%), despite negative aging effects (−1,057,073, −93.98%) and a slight reduction due to epidemiological changes (−329,864.54, −29.33%). Conversely, males experienced lower growth with significant population growth (2,106,68, 237.13%) and greater aging effects (−1,209,36, −136.13%), with marginally less burden alleviation from epidemiological changes (−8,916.07, −1.00%). On the incidence front, females demonstrated a more pronounced rise (356,924.3), primarily due to population growth (813,399.4, 227.89%), negative aging effects (−401,242.5, −112.42%), and slight alleviation from epidemiological changes (−55,232.63, −15.47%). Males saw a lower increase (254,249.0) with significant population growth (685,817.8, 269.74%), greater aging effects (−482,595.8, −189.81%), and a burden increase from epidemiological changes (51,027.06, 20.07%). Concerning YLDs, the increase among females (8,790.58) far exceeded that of males (6,989.47). This increase primarily resulted from substantial population growth (females: 6,849.87, 77.92%; males: 4,920.70, 70.40%) and aging (females: 3,468.57, 39.46%; males: 2,449.08, 35.04%). However, the reduction in burden from epidemiological changes (−1,527.86, −17.38%) was significantly more pronounced in females than in males (−380.31, −5.44%). For DALYs, the overall increase was notably higher among females (10,659.97) compared to males (4,266.36). Population growth was the primary driver in females (7,063.481, 116.00%) and also significant in males (5,037.14, 107.68%). While aging effects were lower in females (648.33, 10.65%), the burden reduction from epidemiological changes (−1,622.53, −26.65%) was considerably greater than in males (−379.25, −8.11%). The detailed results of the decomposition analysis are presented in Figure 3 and Table 2.
 |
Table 2 Decomposition Analysis of Global TTH Among Women and Men from 1990 to 2021 |
 |
Figure 3 Decomposition analysis of global female and male TTH from 1990 to 2021.This figure depicts the impacts of global population growth, aging, and epidemiological changes on the disease burden associated with TTH. The black dots in the figure represent the overall values of the changes contributed by all three components. For each component, the magnitude of a positive value indicates a corresponding increase in the disease burden caused by that component; conversely, the magnitude of a negative value indicates a corresponding decrease in the disease burden caused by that component. Abbreviations: TTH, tension - type headache; YLDs, years lived with disability; DALYs, disability - adjusted life years. |
Prediction Analysis of HHT Burden
The age-standardized prevalence, incidence, YLD, and DALY rates of global TTH exhibit varying changes over time. We conducted a fifteen-year forecast of the aforementioned metrics using the ARIMA model. Through automated selection, we have obtained an ARIMA (3,1,0) model for the time series of female incidence rates. The parameters are ar1 = 0.7722, ar2 = 0.4256, and ar3 = −0.5828. The standard errors for these parameters are 0.2203, 0.3672, and 0.2326, respectively, indicating that these parameters are statistically significant. The residual variance of the model is 25.61, and the log-likelihood value is −91.75. The information criteria (AIC, AICc, BIC) are 191.49, 193.03, and 197.23, respectively. These metrics are relatively small, indicating that the model has high parsimony and accuracy in fitting the data. On the training set, the model’s error metrics are as follows: ME (Mean Error): −1.193726, RMSE (Root Mean Squared Error): 4.733534, MAE (Mean Absolute Error): 3.303877, MPE (Mean Percentage Error): −0.01293913, MAPE (Mean Absolute Percentage Error): 0.03580706, MASE (Mean Absolute Scaled Error): 0.4494071, ACF1 (Autocorrelation of residuals at lag 1): −0.04729405. These error metrics indicate that the model’s predictions perform reasonably well on the training set, with relatively small errors and low residual autocorrelation. Table S7 provides the ARIMA model parameter results for other metrics’ time series. According to the predictions, by the year 2036, the global incidence rates for TTH among females and males will reach 9174.84 and 8630.16 cases per 100,000 population, respectively. Prevalence rates are 25,135.11 for females and 23,700.76 for males per 100,000 population. YLDs rates are 62.76 for females and 49.81 for males, while DALYs rates are 60.97 for females and 50.08 for males per 100,000 population. See Figure 4 and Tables S8–S15 for details.
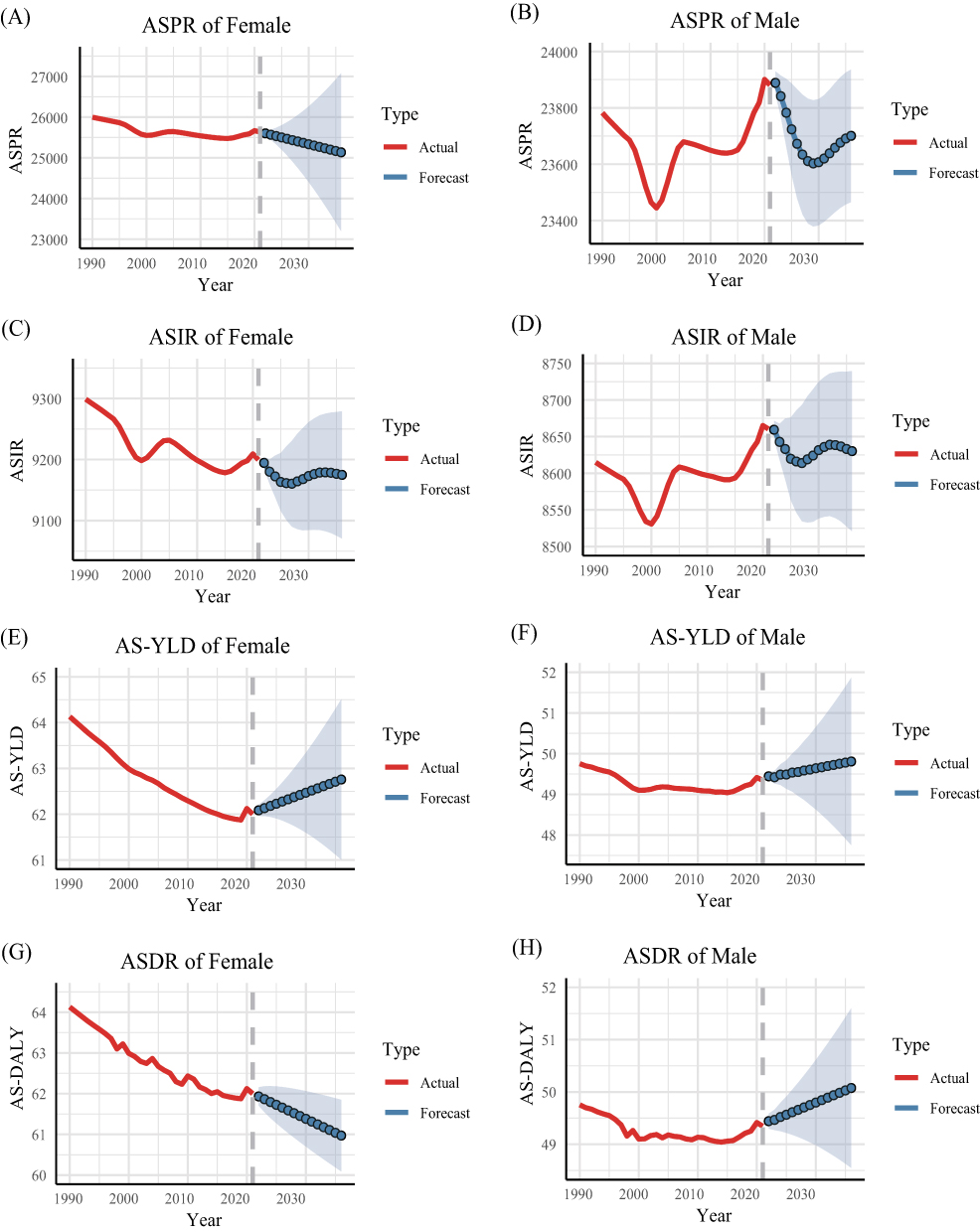 |
Figure 4 Predictive Analysis of the 15-Year Disease Burden for Global TTH in Women and Men.(A) ASPR of female; (B) ASPR of male; (C) ASIR of female; (D) ASIR of male; (E) AS-YLD of female; (F) AS-YLD of male; (G) ASDR of female; (H) ASDR of male. Abbreviations: TTH, tension-type headache; ASPR, Age-Standardized Prevalence Rate; ASIR, Age-Standardized Incidence Rate; AS-YLD, Age-Standardized Years Lived with Disability; ASDR, age-standardized DALY rate. |
Discussion
The epidemiological burden of TTH globally exhibits significant gender disparities. The 2021 data indicates that women have higher prevalence, incidence, YLDs and DALYs compared to men. Specifically, the global total of TTH patients was 2.01 billion (95% UI: 1.78 to 2.27 billion), with women and men comprising 1.04 billion and 0.97 billion, respectively. The age-standardized prevalence for women was 25,634.41 per 100,000 (95% UI: 22,631.48 to 28,974.28), and for men, it was 23,880.79 per 100,000 (95% UI: 21,046.24 to 26,935.06). From 1990 to 2021, the global burden of TTH increased, with women experiencing higher growth in prevalence, incidence, and DALYs than men. Prediction models suggest that by 2036, the age-standardized incidence and prevalence for women will be 9,174.84 and 25,135.11 per 100,000 cases, respectively; for men, they will be 8,630.16 and 23,700.76 per 100,000 cases. Joinpoint regression analysis reveals that the age-standardized incidence for women significantly declined from 1990 to 2001, slowed in decline until 2017, and then slightly increased from 2017 to 2021. Population growth and aging are primary drivers of the increased TTH burden, with epidemiological changes showing more significant mitigating effects in women.
Consistent with previous findings,19 our research indicates that the global total number of TTH patients reached 2.01 billion in 2021, with the number of female patients slightly exceeding that of males. Additionally, our study discovered that the incidence of TTH among both females and males follows a bimodal age distribution, with peaks at 10–14 years and 25–29 years for both genders. The prevalence of TTH surges suddenly during the 10–14 years age group, with no significant difference in incidence between males and females. This age phase corresponds to the early stage of puberty, where sex hormone levels (such as testosterone and estrogen) begin to rise,20 affecting various aspects of the body and mind. Both males and females start exhibiting secondary sexual characteristics, and adolescents may experience emotional instability, heightened feelings of anxiety or depression,21,22 and may also feel pressure from society and peers, particularly regarding appearance, behavior, and social skills.23 At 25–29 years, which is the late stage of puberty, both males and females may face increased pressures related to work, society, and family.24
The research results indicate that the incidence of TTH in women shows a bimodal distribution, while the prevalence does not exhibit such a distribution characteristic. This difference may be related to the natural history of the disease and the survival status of patients. Prevalence is an indicator that comprehensively considers both new and existing cases at a specific time point. In contrast, incidence mainly focuses on the frequency of new cases. The bimodal incidence of TTH may reflect two high - risk stages in a woman’s life. However, the calculation of prevalence includes all existing cases, regardless of when these cases were first diagnosed. Since TTH is typically a long - lasting disease, once patients are diagnosed with TTH, they tend to remain counted as part of the affected population for a long period. This long - term disease state may lead to a smoother prevalence curve, masking the age - specific peaks in the incidence.
We conducted a decomposition analysis of the incidence, prevalence, YLDs and DALYs of TTH between 1990 and 2021 to comprehensively examine the contributing factors. The results indicated that population growth is the primary driver of the increasing burden of TTH, while population aging often plays a negative role. The increase in the burden of TTH is primarily attributable to population growth, which can be understood through several aspects: Firstly, with the continuous global population growth,25 the number of potential patients also increases. The expansion of the population base leads to an increase in the total number of cases and incidence of TTH. Secondly, population growth is usually accompanied by urbanization and industrialization processes. These socio-economic developments bring about changes in lifestyle, such as increased work pressure, faster life pace, and changes in psychological stress,26,27 which may contribute to an increased incidence of TTH. Lastly, with population growth, the pressure on healthcare services also increases. Therefore, population growth may, to some extent, constrain the effectiveness of healthcare services, leading to patients not receiving timely and appropriate treatment, thereby increasing the disease burden.28 It is not surprising that the global aging trend would rather reduce the burden of TTH, as it is usually prevalent among young adults and middle-aged individuals, especially females.29 For females, epidemiological changes significantly alleviated the burden in terms of YLDs (−1,527.86, −17.38%), while the reduction was less pronounced for males (−380.31, −5.44%). Similarly, in terms of DALYs, epidemiological changes led to a more substantial reduction for females (−1,622.5, −26.65%), compared to males (−379.24, −8.11%). This finding not only reflects broader societal changes affecting health behaviors and outcomes differently across genders but also suggests that epidemiological changes in female-specific tension disorders may warrant deeper investigation, possibly linked to changes in diagnostic practices or healthcare utilization.
The Joinpoint analysis results reveal a significant downward trend in the incidence among females from 1990 to 2001, which may be associated with factors such as societal pressures and changes in lifestyle. Subsequently, although the rate of decline slowed, there was a slight upward trend from 2017 to 2021, reflecting an increase in pressures and mental health issues faced by women in recent years. In contrast, the incidence among males exhibited relatively stable changes across different time periods. It is noteworthy that the APC for YLDs and DALYs has exhibited a consistently decreasing trend, indicating that since 1990, global efforts in prevention, medical treatment, and social support for TTH may have undergone certain improvements.17,30 This presents a positive signal in the public health domain, suggesting some progress in reducing disease burden and enhancing quality of life. Such trends hold certain implications for the future development and adjustment of public health strategies.
When predicting the future 15-year global burden of TTH, the auto.arima function automatically selects different ARIMA models for the time series data of males and females. All model parameters, including autoregressive coefficients, demonstrated statistical significance, highlighting their crucial role in fitting the data.31 The residual variance, log-likelihood values, and information criteria (AIC, AICc, BIC) of the models indicated a high degree of simplicity and accuracy in data fitting. The low AIC and BIC values suggested that the models achieved a good fit while maintaining parsimony.32 Error metrics on the training set showed strong predictive performance, with relatively small errors and low residual autocorrelation. Using the ARIMA models to forecast global TTH prevalence, incidence, YLDs, and DALYs, we observed that both male and female TTH incidence rates are expected to increase by 2036. Furthermore, females are anticipated to have higher prevalence, YLD, and DALY rates compared to males, potentially due to unique physiological and psychosocial factors. These predictions carry significant implications for public health policymakers, emphasizing the need for greater attention to the female population and the timely consideration of gender-specific prevention and treatment strategies to alleviate the burden of TTH.
The general limitations of the GBD study discussed elsewhere33 fully apply to this report. Specifically, in this report, we did not provide burden estimates for different countries and regions, as our focus is on examining the global gender disparities in the burden of TTH since 1990. Moreover, according to the International Classification of Headache Disorders – Third Edition (ICHD-3), TTH can be categorized into infrequent episodic TTH, frequent episodic TTH, chronic TTH, and probable TTH.34 The disease burden of different types of TTH may vary by gender, but no relevant research has been conducted to explore this. Additionally, although our predictions for 2036 are based on rigorous predictive models, these predictions rely on certain assumptions that may be influenced by external factors. Furthermore, our study data span from 1990 onwards; however, the diagnostic criteria for TTH established by the International Headache Society were refined and detailed in 2004 and 2018,1,35,36 differing from the criteria primarily based on clinical symptoms and exclusion of other types of headaches since 1988.37 These changes in diagnostic criteria may impact our study results. Therefore, while our findings provide valuable insights into global gender disparities in TTH, they should be interpreted with caution.
Conclusions
Analysis of global epidemiological data on tension - type headache (TTH) has revealed significant gender disparities, with women experiencing higher prevalence, incidence, and health losses compared to men. Although the observed increase in the burden of TTH is partly attributable to global population growth, our time - trend analysis and 15 - year projections have highlighted specific patterns for different genders. Future public health strategies must comprehensively consider gender, age, and epidemiological changes to develop targeted interventions that effectively reduce the impact of TTH on global health.
Data Sharing Statement
No datasets were generated or analyzed during the current study.
Acknowledgments
We would like to express our gratitude to the other staff members of the First Medical Center of the PLA General Hospital.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ashina S, D MD, J LM, et al. Tension-type headache. Nat Rev Dis Primers. 2021;7(1):24. doi:10.1038/s41572-021-00257-2
2. C CS, R KD, W SJ, et al. A pilot analysis on the efficacy of multiple trigger-point saline injections in chronic tension-type headache: a retrospective observational study. J Clin Med. 2022;11(18). doi:10.3390/jcm11185428.
3. J SL, Hagen K, Linde M, et al. The global prevalence of headache: an update, with analysis of the influences of methodological factors on prevalence estimates. J Headache Pain. 2022;23(1):34. doi:10.1186/s10194-022-01402-2
4. Deuschl G, Beghi E, Fazekas F, et al. The burden of neurological diseases in Europe: an analysis for the global burden of disease study 2017. Lancet Public Health. 2020;5(10):e551–e567. doi:10.1016/S2468-2667(20)30190-0
5. Thorud HS, Aurjord R, Falkenberg HK. Headache and musculoskeletal pain in school children are associated with uncorrected vision problems and need for glasses: a case-control study. Sci Rep. 2021;11(1):2093. doi:10.1038/s41598-021-81497-w
6. Bahceci Simsek I. Association of upper eyelid ptosis repair and blepharoplasty with headache-related quality of life. JAMA Facial Plast Surg. 2017;19(4):293–297. doi:10.1001/jamafacial.2016.2120
7. Yalinay Dikmen P, Ertas M, Kosak S, et al. Primary headaches among gender dysphoric female-to-male individuals: a cross-sectional survey on gender transition experience. Headache. 2021;61(8):1194–1206. doi:10.1111/head.14203
8. Stovner LJ, Nichols E, Steiner TJ. Global, regional, and national burden of migraine and tension-type headache, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. 2018;17(11):954–976. doi:10.1016/S1474-4422(18)30322-3
9. Steel SJ, Robertson CE, Whealy MA. Current understanding of the pathophysiology and approach to tension-type headache. Curr Neurol Neurosci Rep. 2021;21(10):56. doi:10.1007/s11910-021-01138-7
10. Karlı N, Baykan B, Ertaş M, et al. Impact of sex hormonal changes on tension-type headache and migraine: a cross-sectional population-based survey in 2,600 women. J Headache Pain. 2012;13(7):557–565. doi:10.1007/s10194-012-0475-0
11. A FM, P CS, J CD, et al. Nociplastic pain: towards an understanding of prevalent pain conditions. Lancet. 2021;397(10289):2098–2110. doi:10.1016/S0140-6736(21)00392-5
12. Cigarán-Méndez M, Jiménez-Antona C, Parás-Bravo P, et al. Active trigger points are associated with anxiety and widespread pressure pain sensitivity in women, but not men, with tension type headache. Pain Pract. 2019;19(5):522–529. doi:10.1111/papr.12775
13. Simić S, Rabi-žikić T, R VJ, et al. Impact of individual headache types on the work and work efficiency of headache sufferers. Int J Environ Res Public Health. 2020;17(18):6918. doi:10.3390/ijerph17186918
14. K CM, W KD, K KB, et al. Gender-specific influence of socioeconomic status on the prevalence of migraine and tension-type headache: the results from the Korean Headache Survey. J Headache Pain. 2013;14(1):82. doi:10.1186/1129-2377-14-82
15. Murray CJL. The Global Burden of Disease Study at 30 years. Nat Med. 2022;28(10):2019–2026. doi:10.1038/s41591-022-01990-1
16. Murray CJL. Findings from the global burden of disease study 2021. Lancet. 2024;403(10440):2259–2262. doi:10.1016/S0140-6736(24)00769-4
17. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2133–2161. doi:10.1016/S0140-6736(24)00757-8
18. Schaffer AL, Dobbins TA, Pearson SA. Interrupted time series analysis using autoregressive integrated moving average (ARIMA) models: a guide for evaluating large-scale health interventions. BMC Med Res Methodol. 2021;21(1):58. doi:10.1186/s12874-021-01235-8
19. Feigin VL, Nichols E, Alam T. Global, regional, and national burden of neurological disorders, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. 2019;18(5):459–480. doi:10.1016/S1474-4422(18)30499-X
20. W MA, B KE, Slater B, et al. The relationship between estrogen and the decline in delta power during adolescence. Sleep. 2017;40(3). doi:10.1093/sleep/zsx008.
21. R PA, A WP, Gurditta K, et al. Mobile phone intervention to reduce youth suicide in rural communities: field test. JMIR Ment Health. 2018;5(2):e10425. doi:10.2196/10425
22. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet Psychiatry. 2022;9(2):137–150. doi:10.1016/S2215-0366(21)00395-3
23. E CA, L FH, Gullet N, et al. Cortisol levels in childhood associated with emergence of attenuated psychotic symptoms in early adulthood. Biol Psychiatry. 2022;91(2):226–235. doi:10.1016/j.biopsych.2021.08.009
24. Lawrence EM, Mollborn S, Hummer RA. Health lifestyles across the transition to adulthood: implications for health. Soc Sci Med. 2017;193:23–32. doi:10.1016/j.socscimed.2017.09.041
25. Lidicker WZ Jr. A Scientist’s Warning to humanity on human population growth. Glob Ecol Conserv. 2020;24:e01232. doi:10.1016/j.gecco.2020.e01232
26. M RS, C RPS, Barthelemy M, et al. Spatial structure of city population growth. Nat Commun. 2022;13(1):5931. doi:10.1038/s41467-022-33527-y
27. V JA, D BA, Von rueden C, et al. Do wealth and inequality associate with health in a small-scale subsistence society? Elife. 2021;10.
28. M QLT, K BS, Bergrath S, et al. Comparing the diagnostic concordance of tele-EMS and on-site-EMS physicians in emergency medical services: a retrospective cohort study. Sci Rep. 2020;10(1):17982. doi:10.1038/s41598-020-75149-8
29. J SJ, K SE, Wang K, et al. Characteristics and gender differences of headache in the veterans health administration: a national cohort study, fiscal year 2008-2019. Neurology. 2022;99(18):e1993–e2005. doi:10.1212/WNL.0000000000200905
30. Vos T, D FA, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2163–2196. doi:10.1016/S0140-6736(12)61729-2
31. Ceylan Z. Estimation of COVID-19 prevalence in Italy, Spain, and France. Sci Total Environ. 2020;729:138817. doi:10.1016/j.scitotenv.2020.138817
32. Kumari S, S SS, Kumar D, et al. Foraging behaviour of Scymnus coccivora Ayyar against cotton mealybug Phenacoccus solenopsis Tinsley. Saudi J Biol Sci. 2021;28(7):3799–3805. doi:10.1016/j.sjbs.2021.03.051
33. A RG, A MG, O JC, et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 Study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
34. Headache classification committee of the International Headache Society (IHS) the international classification of headache disorders. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
35. Olesen J. international classification of headache disorders. Lancet Neurol. 2018;17(5):396–397. doi:10.1016/S1474-4422(18)30085-1
36. Olesen J. The international classification of headache disorders. Rev Neurol. 2005;161(6–7):689–691. doi:10.1016/S0035-3787(05)85119-7
37. Rapoport AM. The diagnosis of migraine and tension-type headache, then and now. Neurology. 1992;42(3 Suppl 2):11–15.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.