")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Analysis of Prognostic Risk Factors in Children with Disorders of Consciousness Undergoing Hyperbaric Oxygen Therapy
Authors Zhao L, Li S, Liu Y, Di Z, Li H
Received 15 January 2025
Accepted for publication 21 May 2025
Published 30 June 2025 Volume 2025:18 Pages 3803—3812
DOI https://doi.org/10.2147/JMDH.S517708
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Long Zhao, Sha Li, Yansong Liu, Zhijuan Di, Hongling Li
The Second Department of Rehabilitation, The Second Hospital of Hebei Medical University, Shijiazhuang, 050000, People’s Republic of China
Correspondence: Hongling Li, The Second Department of Rehabilitation, The Second Hospital of Hebei Medical University, No. 215 Heping West Road, Shijiazhuang City, Hebei Province, 050000, People’s Republic of China, Tel +86-031166002999, Email [email protected]
Background and Objective: Disorders of consciousness (DOC) are serious neurological conditions in children, often caused by brain injury, infection, or hypoxia, with limited effective treatments. Hyperbaric oxygen therapy (HBOT) has emerged as a promising adjunctive approach due to its potential to improve cerebral oxygenation and promote neural repair. However, the prognostic factors influencing treatment outcomes in pediatric DOC remain unclear. This study aimed to identify the risk factors for prognosis of children with DOC undergoing HBOT.
Methods: A retrospective analysis was conducted on 255 children diagnosed with DOC who received HBOT at the Second Hospital of Hebei Medical University from January 2010 to January 2024. Clinical data, including demographic information, etiology, Glasgow Coma Scale (GCS) scores, Coma Recovery Scale-Revised (CRS-R), treatment timing, and comorbidities, were collected. According to the Glasgow Outcome Scale (GOS) score, the children were divided into poor prognosis group and good prognosis group. Logistic regression analysis was performed to identify independent risk factors for poor prognosis.
Results: Age < 12 years (OR: 0.319, 95% CI: 0.113– 0.901), late timing of HBOT intervention (OR: 41.667, 95% CI: 2.122– 818.296), low HBOT frequency (OR: 0.092, 95% CI: 0.019– 0.441), low GCS score before HBOT (OR: 0.523, 95% CI: 0.362– 0.756), low CRS-R score before HBOT (OR: 0.419, 95% CI: 0.226– 0.780), and hypoxic-ischemic encephalopathy (OR: 4.885, 95% CI: 1.508– 15.826) were risk factors for poor prognosis in DOC children (P < 0.05). Low GCS score before treatment was an independent risk factor for poor prognosis in DOC children after traumatic brain injury (P < 0.05), low CRS-R score before treatment was an independent risk factor for poor prognosis in DOC children after encephalitis (P < 0.05), and late timing of HBOT, low HBOT frequency and low CRS-R score before HBOT were independent risk factors for poor prognosis in DOC children after hypoxic-ischemic encephalopathy (P < 0.05).
Conclusion: This study highlights the clinical value of early HBOT intervention and baseline neurological status in predicting recovery in children with DOC. Identifying these risk factors can help optimize treatment decisions and improve long-term neurological outcomes.
Keywords: hyperbaric oxygen, children, disorders of consciousness, prognosis, influencing factor
Introduction
The response of the human body to itself and its surrounding environment, as well as the level of wakefulness, is called consciousness, which is closely related to the cerebral cortex and brainstem ascending reticular activating system (ARAS). When the brain is damaged, the connections between various brain regions are damaged, thus leading to disorders of consciousness (DOC).1 DOC has a multitude of associated causes including trauma, infection, hypoxia, etc. According to different clinical manifestations, it can be classified into coma, vegetative state (VS)/unresponsive wakefulness syndrome (UWS), minimal consciousness state (MCS), and emergence of MCS (eMCS).2
Although there are many methods for treating DOC in clinical practice, the therapeutic effects are not satisfactory. Mild cases can transition from coma to wakefulness, but a large proportion of patients are in long-term DOC, which not only seriously affects their quality of life, but also increases the burden on families, healthcare services and society.3 Especially for DOC in children with underdeveloped nervous systems and high brain plasticity, timely and effective active treatment is crucial for their recovery of consciousness and prognosis. The prognosis and recovery of DOC patients are affected by many factors. However, most studies focus on adults but few on the factors affecting the prognosis and recovery of DOC in children. In addition, due to the unique developmental characteristics of children, their injury mechanisms are different from those of adults. Consequently, research on adult DOC and evidence-based medicine cannot accurately make effective recommendations for pediatric DOC.4
Hyperbaric oxygen therapy (HOBT) is indeed considered an additional, adjunctive procedure in the treatment of DOC.5 By allowing patients to inhale nearly pure oxygen at pressures higher than normal atmospheric levels, HBOT aims to enhance oxygen delivery to tissues, including hypoxic brain areas, potentially promoting neuroplasticity and recovery of consciousness. HBOT has been shown to increase cerebral blood oxygen content and partial pressure, enhancing oxygen supply to injured areas. It also helps alleviate cerebral edema, reduce intracranial pressure, promote the formation of collateral circulation, and accelerate recovery in patients with DOC.6 Its safety and non-invasiveness make it particularly appealing, especially in pediatric patients where more invasive procedures may pose higher risks. Some observational studies and smaller clinical trials have reported positive effects of HBOT on prognosis, mortality, and disability rates in patients with disorders of consciousness.7–9 While HBOT has a favorable safety profile, its clinical benefits for DOC have not yet been conclusively established within the available evidence, and research on its therapeutic effects in children with DOC remains limited. This study analyzed potential risk factors for outcome of HBOT in children with disorders of DOC, so as to provide reference and guidance for future treatment of DOC in children.
Materials and Methods
Subjects
A retrospective analysis was conducted on 255 DOC children undergoing HBOT at the Second Hospital of Hebei Medical University from January 2010 to January 2024. The inclusion criteria were as follows: (1) patients met the diagnostic criteria for DOC,10 and brain damage was the only cause of DOC; (2) patients had a course of disease < 3 months; (3) patients aged < 18 years; (4) patients had stable vital signs; (5) the family members of the children agreed to and received rehabilitation assessment and treatment; (6) the overall frequency of HBOT was not less than 10. The exclusion criteria included: (1) patients with underlying developmental, psychiatric and neurological disorders prior to the onset of DOC; (2) patients with rapidly deteriorated condition during treatment or an inability to continue treatment; (3) patients without complete medical records; (4) patients with contraindications for HBOT such as bleeding tendencies, untreated pneumothorax and epilepsy.
HBOT Therapy
All children underwent routine monitoring of blood pressure, electrocardiogram (ECG) and blood oxygen saturation. HBOT was performed using a medical hyperbaric chamber with three locks and seven doors (YC3200/0.3–22VII, Hoto Oxygen Industrial, Yantai). The chamber was pressurized with air to 1.4–2.0 atmosphere absolute (ATA) over a period of 25 minutes, after which the treatment protocol was carried out as scheduled. Infants were pressurized at 1.4–1.6 ATA, children with severe conditions or complications such as otorrhea and rhinorrhea at 1.6–1.8 ATA, and children with stable conditions at 1.8–2.0 ATA. After pressure stabilization, pure oxygen was inhaled for 30 minutes twice, with a 10-minute interval of air inhalation between the two oxygen sessions, followed by a 25-minute decompression phase. Each complete session lasted 120 minutes and was performed once per day. The treatment consisted of two courses, each lasting 30 days, with a 5–7 day rest period between the courses. To ensure safety and treatment efficacy, the pressure ranges during HBOT were selected based on patient age, clinical stability, and existing guidelines. Infants were treated at 1.4–1.5 ATA to minimize the risks of barotrauma and oxygen toxicity, as their lungs are structurally immature and their antioxidant capacity is limited. Children with severe conditions or complications such as otorrhea or rhinorrhea received HBOT at 1.6–1.75 ATA, following recommendations for vulnerable pediatric populations. Clinically stable children were treated at 1.8–2.0 ATA, which is within the range commonly used in older pediatric patients with sufficient physiological resilience. The classification of HBOT timing (≤7 days, 8–14 days, 15–30 days, >30 days) and treatment frequency (10–20 times, 21–30 times, >30 times) in this study was based on clinical experience and the practical treatment patterns observed in our institution.
Observation Indicators
Retrospective data on the children was collected, including gender, age, etiology, timing, frequency, and pressure of HBOT. Additionally, Glasgow Coma Scale (GCS) and Coma Recovery Scale-Revised (CRS-R) scores were recorded upon admission. Prognosis following HBOT treatment was evaluated using Glasgow Outcome Scale (GOS) scores at the 3-month follow-up after discharge.
GCS scoring:11 Children aged ≥ 4 years were scored using the GCS, while those aged < 4 years by the modified GCS, also known as the Children Coma Scale (CCS), with a score of 15 as clear consciousness, 12–14 as mild DOC, 9–11 as moderate DOC, and < 8 as a coma state.
CRS-R scoring:12 This scale included six subscales on auditory, visual, motor, verbal, communication and arousal levels, with a total score of 23. A higher score indicated milder DOC and clearer consciousness. VS/UWS was diagnosed by auditory score ≤ 2, visual score ≤ 1, motor score ≤ 2, verbal score ≤ 2, communication score of 0, or arousal score ≤ 2. MCS was determined by auditory score of 3–4, visual score of 2–5, motor score of 3–5, verbal score of 3, communication score of 1, or arousal score of 3.
GOS scoring:13 A higher score indicated milder craniocerebral injury, with 1–3 as poor prognosis and 4–5 as good prognosis. Based on the prognosis, the children were divided into poor prognosis group (score, 1–3) and good prognosis (score, 4–5).
Statistical Methods
The data were analyzed using SPSS version 26.0 statistical software. Normality was assessed using the Shapiro–Wilk test, and homogeneity of variance was checked to determine the appropriate statistical methods. For normally distributed continuous data, variables were presented as mean ± standard deviation, while skewed data were reported as median and interquartile range (IQR). To ensure the validity of statistical methods, we calculated the required sample size based on preliminary data, ensuring adequate power to detect significant changes in GCS and CRS-R scores. For comparisons of pre- and post-treatment scores, paired t-tests were used for normally distributed data meeting the assumptions, while the Wilcoxon signed-rank test was applied for skewed data. Enumeration data were analyzed using the Chi-square test or Fisher’s exact test. Additionally, binary logistic regression analysis was performed to identify risk factors affecting prognosis post-HBOT, adjusting for potential confounders. A p-value of < 0.05 was considered statistically significant.
Results
Influencing Factor Analysis of Prognosis in DOC Children After HBOT
According to the follow-up results, the 255 children were divided into a good prognosis group (n = 182, 71.4%) and a poor prognosis group (n = 73, 28.6%). The two groups showed statistically significant differences in age, etiology, timing of HBOT, HBOT frequency, rehabilitation therapy, GCS and CRS-R scores before treatment, with statistically significant differences (P < 0.05), as seen in Table 1. Multivariate logistic regression analysis suggested that age < 12 years, late timing of HBOT, low HBOT frequency, low GCS score before HBOT, low CRS-R score before HBOT, and DOC caused by hypoxic-ischemic encephalopathy were risk factors for poor prognosis in DOC children (P < 0.05) (Table 2).
 |
Table 1 Comparison of General Data Between Good and Poor Prognosis Groups |
 |
Table 2 Multivariate Logistic Regression Analysis |
Influencing Factor Analysis of Prognosis in DOC Children Caused by Different Etiologies
Univariate analysis showed that among DOC children caused by traumatic brain injury, there were statistically significant differences in age, timing of HBOT, HBOT frequency, rehabilitation therapy, GCS score before treatment, and CRS-R score before treatment between the good prognosis group and the poor prognosis group (P < 0.05) (Table 3). In DOC children caused by encephalitis, GCS and CRS-R scores before treatment also had statistically significant differences between the good prognosis group and the poor prognosis group (P < 0.05), as displayed in Table 4. The good and poor prognosis groups of DOC children caused by hypoxic-ischemic encephalopathy also presented statistically significant differences in age, timing of HBOT, HBOT frequency, GCS score before treatment, and CRS-R score before treatment (P < 0.05) (Table 5). Based on multivariate logistic regression analysis, it was found that low GCS score before treatment was a risk factor for poor prognosis in DOC children after traumatic brain injury (P < 0.05), and low CRS-R score before treatment was a risk factor for poor prognosis in DOC children after encephalitis (P < 0.05), as shown in Table 6.
 |
Table 3 Univariate Analysis of DOC Children After Traumatic Brain Injury |
 |
Table 4 Univariate Analysis of DOC Children After Encephalitis |
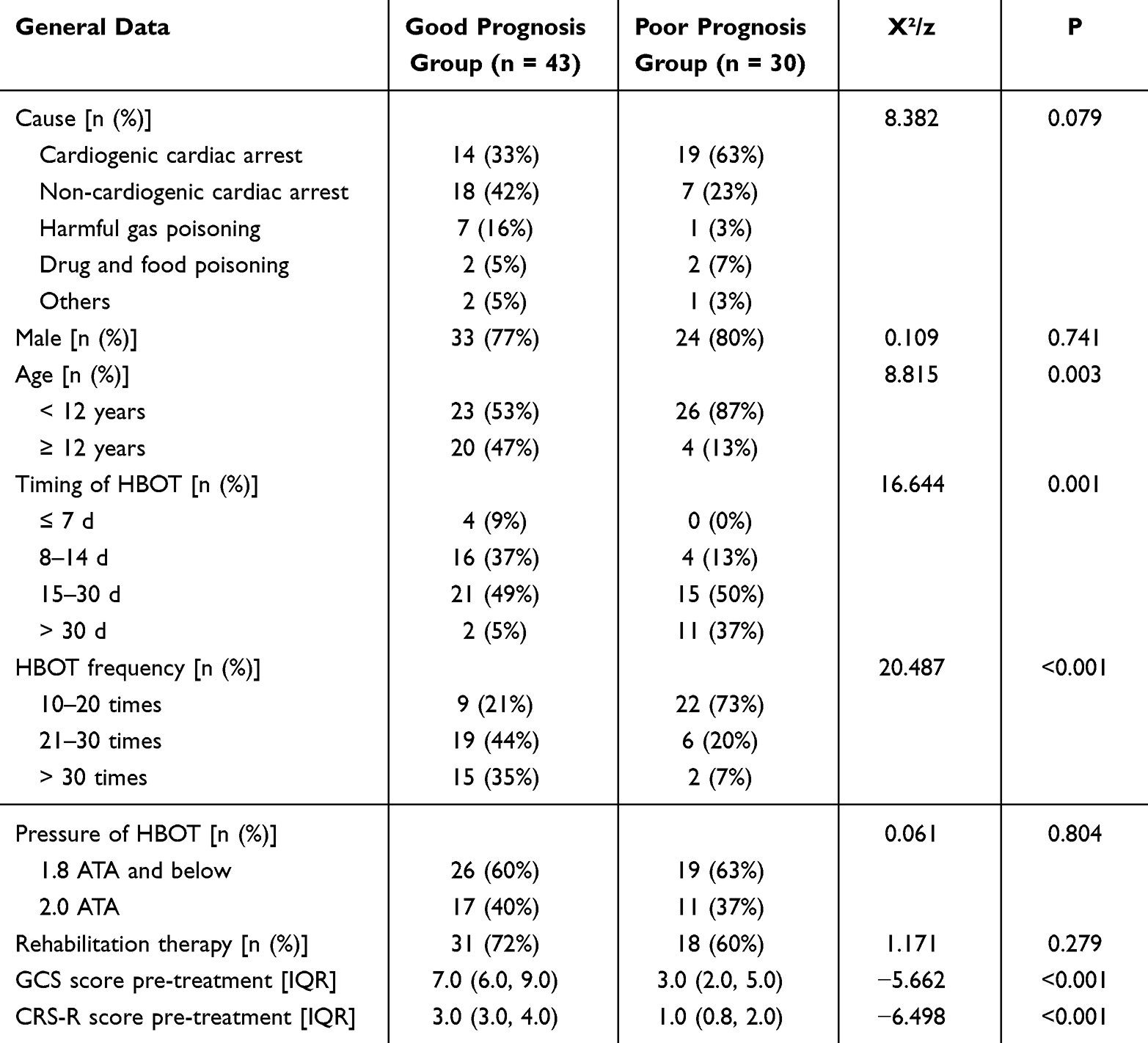 |
Table 5 Univariate Analysis of DOC Children After Hypoxic-Ischemic Encephalopathy |
 |
Table 6 Multivariate Analysis of Prognosis in DOC Children Caused by Different Etiologies |
Discussion
As confirmed in numerous previous studies, HBOT can promote awakening, improve state of consciousness and prognosis, and reduce mortality rate in patients with DOC. Moreover, GCS score, GOS score and cognitive function are also improved after HBOT.14–16 HBOT can effectively improve cognitive outcomes in patients with mild traumatic brain injury by improving cerebral hypoxia and alleviating cerebral injury.17 A meta-analysis has shown that patients receiving HBOT achieve significant improvements in GCS and GOS scores, with a low overall mortality rate.18
In our study, prognostic factor analysis found that DOC children aged ≥ 12 years presented a better prognosis than those aged < 12 years, with a statistically significant difference. Multiple studies abroad have also shown that younger children with cerebral injury have poorer cognitive and psychological recovery.19,20 A study showed that younger children with cerebral injury exhibit poorer prognosis. Compared with children aged 7 years and above, those under 2 years old present the worst recovery of neurobehavioral function after cerebral injury, and neurological damage has the greatest impact on prognosis at the early stage of skill development,21 which may be related to their immature brain development and incomplete myelination. Younger children without well-developed neural networks may experience neuronal damage after cerebral injury, which can affect the normal development of brain structure and function.22 Consequently, the poorer prognosis that younger children with DOC may experience may be attributed to their immature brain development, incomplete myelination, and the increased susceptibility of neural networks to injury during critical periods of skill formation.
It has been previously reported that in patients with sudden sensorineural hearing loss, the efficacy of hyperbaric oxygen therapy is significantly influenced by the timing of its initiation.23 Similar to this finding, our study found that the prognosis of patients receiving HBOT ≤ 7 d after injury was better than those who underwent intervention between 15–30 d and > 30 d. Based on our results, HBOT should be given as early as possible within 7 d after onset to ensure stable vital signs in DOC patients. In addition, patients who received 21–30 HBOT sessions and more than 30 sessions had approximately 0.3-fold and 0.1-fold lower risk of poor prognosis, respectively, compared to those who received only 10–20 sessions, indicating that the prognosis of DOC patients is also related to the frequency of HBOT.
In this study, we found that lower Glasgow Coma Scale (GCS) scores at admission were significantly associated with poorer prognosis in children with DOC undergoing HBOT. Specifically, for each 1-point decrease in the GCS score, the odds of poor prognosis increased by approximately 50% (OR = 0.5). This result is consistent with prior studies that have demonstrated the predictive value of GCS across various forms of DOC, including traumatic brain injury and hypoxic-ischemic encephalopathy.24,25 A lower GCS score reflects more severe impairment of consciousness and likely indicates extensive neuronal damage and reduced brain plasticity, both of which can limit the therapeutic effectiveness of interventions such as HBOT.26 In addition, our study also highlighted the Coma Recovery Scale-Revised (CRS-R) as another valuable assessment tool for prognostic evaluation. CRS-R has been widely adopted in both clinical and research settings due to its structured, multi-dimensional approach, which covers auditory, visual, motor, oromotor, communication, and arousal subscales.27 Previous studies have reported that CRS-R is not only useful for diagnosing different states of consciousness but also has predictive value for recovery outcomes.28 Compared to other assessment tools such as the GCS and the Full Outline of UnResponsiveness (FOUR) score, CRS-R provides a more comprehensive profile of neurobehavioral function, which may help refine prognostic judgments in pediatric DOC cases. Our findings suggest that both the GCS and CRS-R serve as significant and complementary prognostic indicators for children with DOC. Lower pre-treatment scores on these scales were associated with an increased likelihood of unfavorable outcomes. These results underscore the importance of early and repeated consciousness assessments, which can assist clinicians in risk stratification, guide therapeutic decision-making, and enhance family counseling during the course of HBOT treatment.
In the present study, the prognosis for children with DOC due to traumatic brain injury was found to be better than for those with DOC caused by encephalitis or hypoxic-ischemic encephalopathy. The risk of poor prognosis in children with encephalitis or hypoxic-ischemic encephalopathy was approximately 4 times higher than in those with traumatic brain injury, suggesting that the nature of the brain injury is a significant factor in recovery of consciousness in pediatric DOC cases. Similarly, a study have pointed out that the recovery potential of DOC caused by traumatic brain injury is higher than that caused by non-traumatic brain injury.29 Consequently, etiology is also an important factor affecting the prognosis of children with DOC. To be more specific, a low GCS score prior to HBOT is an independent risk factor for poor prognosis in DOC children caused by traumatic brain injury. Previous studies have also confirmed that a low GCS score is independently correlated with poor prognosis in children with traumatic brain injury.30 Moreover, univariate analysis showed that GCS and CRS-R scores before HBOT were prognostic factors for DOC caused by encephalitis, and multivariate analysis only found that low CRS-R score before HBOT was an independent risk factor for poor prognosis in children with DOC caused by encephalitis, which may be related to the superior diagnostic and prognostic validity of CRS-R for VS/UWS and MCS to GCS.31 Our study also demonstrated that late timing of HBOT, low HBOT frequency, and low CRS-R score before HBOT were independent risk factors for poor prognosis in children with DOC after hypoxic-ischemic encephalopathy, which is consistent with previous research results.32 After hypoxic-ischemic encephalopathy, early HBOT can effectively prevent and treat hypoxic damage and functional failure of tissues and organs, improve the repair of cerebral blood vessels, establish collateral circulation, and effectively protect damaged nerve cells.6 At present, there is still controversy over the timing and course of HBOT, and further research is needed for determination.
This study has several limitations. First, as a retrospective study, it is prone to selection bias. Second, some children received concurrent therapies, such as transcranial direct current stimulation, median nerve electrical stimulation, or exercise therapy, which may introduce confounding factors affecting the assessment of HBOT outcomes. Third, the absence of a control group and the exploratory nature of HBOT for DOC introduce limitations in the generalizability and scientific rigor of this study. Additionally, the frequency and pressure of HBOT were converted to categorical variables in this study. Therefore, more analysis for frequency and pressure help to build up clinical settings. Additionally, the assessment indicators used in this study, such as the GCS and CRS-R scores, are somewhat subjective and may vary between evaluators. Therefore, the results require further analysis and validation through multi-center, large-sample prospective studies.
Conclusion
In conclusion, this study identified several key risk factors — including lower GCS and CRS-R scores at admission, longer time from onset to treatment initiation, and fewer HBOT frequency — that were significantly associated with poor prognosis in children with DOC undergoing HBOT These findings highlight the critical importance of early diagnosis, timely intervention, and comprehensive neurological assessment in improving clinical outcomes. In particular, the use of standardized consciousness scales such as GCS and CRS-R can assist clinicians in tailoring treatment plans and setting realistic recovery expectations for families. However, this study has several limitations. It was a single-center retrospective analysis with a limited sample size, and potential confounding factors such as underlying etiology, concurrent treatments, and rehabilitation strategies were not fully controlled. Future prospective multicenter studies with larger cohorts are necessary to validate these findings and explore whether early and repeated HBOT combined with other rehabilitation therapies can further enhance recovery outcomes in pediatric DOC populations.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of The Second Hospital of Hebei Medical University (No. 2023-R137). Written informed consent was obtained from their parent or legal guardian.
Funding
This study did not receive any funding in any form.
Disclosure
All of the authors had no any personal, financial, commercial, or academic conflicts of interest separately.
References
1. Weitzel L, Bavishi S. Disorders of Consciousness. Phys Med Rehabil Clin N Am. 2024;35(3):493–506. doi:10.1016/j.pmr.2024.02.003
2. Kondziella D, Stevens RD. Classifying Disorders of Consciousness: past, Present, and Future. Seminars in neurology. 2022;42(3):239–248. doi:10.1055/a-1883-1021
3. Giacino JT, Katz DI, Schiff ND, et al. Practice Guideline Update Recommendations Summary: disorders of Consciousness: report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology; the American Congress of Rehabilitation Medicine; and the National Institute on Disability, Independent Living, and Rehabilitation Research. Arch Phys Med Rehabil. 2018;99(9):1699–1709. doi:10.1016/j.apmr.2018.07.001
4. Molteni E, Canas LDS, Briand MM, et al. Scoping Review on the Diagnosis, Prognosis, and Treatment of Pediatric Disorders of Consciousness. Neurology. 2023;101(6):e581–e593. doi:10.1212/WNL.0000000000207473
5. Ys L, Zb L, Yang Z, et al. Clinical efficacy of hyperbaric oxygen combined with different timings of right median-nerve electrical stimulation in patients with brain injury-induced disorders of consciousness. Brain Behavior. 2022;12(9):e2716. doi:10.1002/brb3.2716
6. Li S, Di ZJ, Liu ZB, et al. Analysis of the efficacy of hyperbaric oxygen therapy for disorders of consciousness: a retrospective cohort study. Brain Behav. 2024;14(7):e3588. doi:10.1002/brb3.3588
7. Wang J, Xu L, Ge Q, et al. EEG microstate changes during hyperbaric oxygen therapy in patients with chronic disorders of consciousness. Front Neurosci. 2023;17:1145065. doi:10.3389/fnins.2023.1145065
8. Gong XB, Feng RH, Dong HM, et al. Efficacy and Prognosis of Hyperbaric Oxygen as Adjuvant Therapy for Neonatal Hypoxic-Ischemic Encephalopathy: a Meta-Analysis Study. Front Pediatr. 2022;10:707136. doi:10.3389/fped.2022.707136
9. Sahni T, Jain M, Prasad R, et al. Use of hyperbaric oxygen in traumatic brain injury: retrospective analysis of data of 20 patients treated at a tertiary care centre. Br J Neurosurg. 2012;26(2):202–207. doi:10.3109/02688697.2011.626879
10. Alvarez G, Suskauer SJ, Slomine B. Clinical Features of Disorders of Consciousness in Young Children. Archives of Physical Medicine and Rehabilitation. 2019;100(4):687–694. doi:10.1016/j.apmr.2018.12.022
11. Reith FC, Van den Brande R, Synnot A, et al. The reliability of the Glasgow Coma Scale: a systematic review. Intensive Care Medicine. 2016;42(1):3–15. doi:10.1007/s00134-015-4124-3
12. Bodien YG, Vora I, Barra A, et al. Feasibility and Validity of the Coma Recovery Scale-Revised for Accelerated Standardized Testing: a Practical Assessment Tool for Detecting Consciousness in the Intensive Care Unit. Ann Neurol. 2023;94(5):919–924. doi:10.1002/ana.26740
13. McMillan T, Wilson L, Ponsford J, et al. The Glasgow Outcome Scale - 40 years of application and refinement. Nature Reviews Neurology. 2016;12(8):477–485. doi:10.1038/nrneurol.2016.89
14. Fischer I, Barak B. Molecular and Therapeutic Aspects of Hyperbaric Oxygen Therapy in Neurological Conditions. Biomolecules. 2020;10(9). doi:10.3390/biom10091247
15. Chen Y, Wang L, You W, et al. Hyperbaric oxygen therapy promotes consciousness, cognitive function, and prognosis recovery in patients following traumatic brain injury through various pathways. Frontiers in Neurology. 2022;13:929386. doi:10.3389/fneur.2022.929386
16. Sankaran R, Radhakrishnan K, Sundaram KR. Hyperbaric oxygen therapy in patients with hypoxic ischemic encephalopathy. Neurol India. 2019;67(3):728–731. doi:10.4103/0028-3886.263236
17. Liu Z, Wang X, Wu Z, et al. HBOT has a better cognitive outcome than NBH for patients with mild traumatic brain injury: a randomized controlled clinical trial. Medicine. 2023;102(37):e35215. doi:10.1097/MD.0000000000035215
18. Wang F, Wang Y, Sun T, et al. Hyperbaric oxygen therapy for the treatment of traumatic brain injury: a meta-analysis. Neurological Sciences: Official Journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology. 2016;37(5):693–701. doi:10.1007/s10072-015-2460-2
19. Beauchamp MH, Anderson V. Cognitive and psychopathological sequelae of pediatric traumatic brain injury. Handb Clin Neurol. 2013;112:913–920.
20. Levin HS, Temkin NR, Barber J, et al. Association of Sex and Age With Mild Traumatic Brain Injury-Related Symptoms: a TRACK-TBI Study. JAMA Netw Open. 2021;4(4):e213046. doi:10.1001/jamanetworkopen.2021.3046
21. Anderson V, Jacobs R, Spencer-Smith M, et al. Does early age at brain insult predict worse outcome? Neuropsychological implications. J Pediatr Psychol. 2010;35(7):716–727. doi:10.1093/jpepsy/jsp100
22. Ismail FY, Fatemi A, Johnston MV. Cerebral plasticity: windows of opportunity in the developing brain. Eur J Paediatr Neurol. 2017;21(1):23–48. doi:10.1016/j.ejpn.2016.07.007
23. Cook NF. The Glasgow Coma Scale: a European and Global Perspective on Enhancing Practice. Crit Care Nurs Clin North Am. 2021;33(1):89–99. doi:10.1016/j.cnc.2020.10.005
24. Kochar A, Borland ML, Phillips N, et al. Association of clinically important traumatic brain injury and Glasgow Coma Scale scores in children with head injury. Emerg Med J. 2020;37(3):127–134. doi:10.1136/emermed-2018-208154
25. Yıldırım E, Murat Özcan K, Palalı M, et al. Prognostic effect of hyperbaric oxygen therapy starting time for sudden sensorineural hearing loss. Eur Arch Otorhinolaryngol. 2015;272(1):23–48. doi:10.1007/s00405-013-2829-x
26. Popernack ML, Gray N, Reuter-Rice K. Moderate-to-Severe Traumatic Brain Injury in Children: complications and Rehabilitation Strategies. J Pediatr Health Care. 2015;29(3):e1–7. doi:10.1016/j.pedhc.2014.09.003
27. Annen J, Filippini MM, Bonin E, et al. Diagnostic accuracy of the CRS-R index in patients with disorders of consciousness. Brain Inj. 2019;33(11):1409–1412. doi:10.1080/02699052.2019.1644376
28. Nekrasova J, Kanarskii M, Borisov I, et al. One-year demographical and clinical indices of patients with chronic disorders of consciousness. Brain Sciences. 2021;11(5):651. doi:10.3390/brainsci11050651
29. Estraneo A, Moretta P, Loreto V, et al. Late recovery after traumatic, anoxic, or hemorrhagic long-lasting vegetative state. Neurology. 2010;75(3):239–245. doi:10.1212/WNL.0b013e3181e8e8cc
30. Soysal E, Horvat CM, Simon DW, et al. Clinical Deterioration and Neurocritical Care Utilization in Pediatric Patients With Glasgow Coma Scale Score of 9–13 After Traumatic Brain Injury: associations With Patient and Injury Characteristics. Pediatr Crit Care Med. 2021;22(11):960–968. doi:10.1097/PCC.0000000000002767
31. Zhang Y, Wang J, Schnakers C, et al. Validation of the Chinese version of the Coma Recovery Scale-Revised (CRS-R). Brain Inj. 2019;33(4):529–533. doi:10.1080/02699052.2019.1566832
32. Estraneo A, Moretta P, Loreto V, et al. Predictors of recovery of responsiveness in prolonged anoxic vegetative state. Neurology. 2013;80(5):464–470. doi:10.1212/WNL.0b013e31827f0f31
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.