")
Back to Journals » International Journal of General Medicine » Volume 18
Analysis of Risk Factors and Development of a Predictive Model for Delirium in ICU Patients: Construction, Validation, and Clinical Implications
Authors Li X, Zhang W , Wang T, Qiu Z, Sun X, Qu W, Zhang G
Received 22 March 2025
Accepted for publication 2 July 2025
Published 5 July 2025 Volume 2025:18 Pages 3727—3737
DOI https://doi.org/10.2147/IJGM.S526749
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Xia Li,1,* Weisong Zhang,2,3,* Tao Wang,4 Zhengfeng Qiu,1 Xuan Sun,1 Wenhao Qu,1 Guopei Zhang1
1Department of Intensive Care Unit, Affiliated Hospital 6 of Nantong University, Yancheng Third People’s Hospital, Yancheng, 224000, People’s Republic of China; 2Department of Thoracic Surgery, Affiliated Hospital 6 of Nantong University, Yancheng Third People’s Hospital, Yancheng, 224000, People’s Republic of China; 3Medical School of Nantong University, Nantong, 226007, People’s Republic of China; 4Department of Anesthesiology, Affiliated Hospital 6 of Nantong University, Yancheng Third People’s Hospital, Yancheng, 224000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guopei Zhang, Email [email protected]
Objective: To analyze the influencing factors contributing to the occurrence of delirium in patients within the Intensive Care Unit (ICU) and to construct a prediction model for delirium in critically ill patients, subsequently verifying its predictive value.
Methods: A prospective study was conducted involving 641 patients admitted between January 2023 and June 2024. A simple random sampling method was employed to develop the predictive model, with a validation set comprising 193 patients, thus creating a training set of 448 patients. Delirium was assessed using the Confusion Assessment Method for the ICU (CAM-ICU). The baseline data of the two patient groups in the training and validation sets were compared. Logistic regression analysis was utilized to identify independent risk factors influencing the onset of delirium. The R programming language was employed to establish a column-line graph model for predicting delirium occurrence in ICU patients. The Bootstrap method facilitated model validation, while calibration curves and Receiver Operating Characteristic (ROC) curves were utilized to evaluate the model’s discriminatory ability and predictive efficacy. Finally, the prediction model was validated using the validation set.
Results: In the training cohort, the incidence of delirium among patients was 35.71%. Logistic regression analysis revealed that the Glasgow Coma Scale (GCS) score (OR=0.421, 95% CI: 0.355– 0.501, P< 0.001), blood urea nitrogen (BUN) (OR=1.169, 95% CI: 1.014– 1.348, P=0.031), emergency surgery (OR=2.735, 95% CI: 1.42– 5.268, P=0.003), use of sedative medications (OR=3.816, 95% CI: 1.968– 7.397, P< 0.001), and postoperative status following major cardiovascular surgery (OR=2.124, 95% CI: 1.205– 3.745, P=0.009) were identified as independent risk factors for delirium in the ICU.
Conclusion: The predictive model developed in this study for the occurrence of delirium in ICU patients has been validated, demonstrating high predictive efficacy and offering significant clinical early warning guidance.
Keywords: delirium, intensive care unit, prediction model, risk factor, nomogram
Introduction
Delirium is a common and serious neuropsychiatric disorder characterized by changes in patients’ cognitive levels and consciousness. It frequently occurs as a complication in patients within intensive care units and is often referred to as ICU delirium.1 According to multiple studies, the incidence of delirium in the ICU can be as high as 45%-87%.2 However, the prevalence of delirium in China is often underestimated. Furthermore, delirium adversely affects the prognosis of ICU patients and is associated with prolonged hospitalization, increased patient pain, and elevated mortality rates.3,4 Therefore, early identification and prevention of ICU delirium may lead to better outcomes for critically ill patients.5 Currently, there are two widely used prediction models for delirium in patients in the ICU abroad: the PRE-DELIRIC model and the E-PRE-DELIRIC model.6,7 However, there are significant discrepancies in the research findings regarding the risk factors for delirium.8–10 Furthermore, there is a lack of independent validation studies of these models specifically for the Chinese population, indicating a need to optimize the models using local data. This study, based on data from ICU patients in China, identifies five independent risk factors for localized delirium: GCS score, BUN, emergency surgery, use of sedatives, and postoperative cardiovascular surgery. A nomogram prediction model was constructed. Validation results from the training set (AUC 0.886) and the validation set (AUC 0.913) indicate that this model has potential application value for stratifying delirium risk in ICU patients in China, although further multicenter validation is required.
Materials and Methods
Study Design and Development Cohort
This trial is a prospective, single-center, observational study. All patients were treated by an ICU team with extensive clinical experience in accordance with relevant disease guidelines. This study included patients aged 18 years and older who had an ICU stay of 24 hours or more. Patients with a history of delirium, as well as pregnant or perinatal patients, were excluded from the study. Additionally, individuals with persistent coma (Glasgow Coma Scale score of 8 or lower) or deep sedation (Richmond Agitation-Sedation Scale score of −3 or lower) who could not be awakened for assessment were also excluded. Patients admitted to the intensive care unit of Yancheng Third People’s Hospital from January 2023 to June 2024 were continuously included. Based on the inclusion and exclusion criteria, a total of 641 patients were ultimately included. Using a simple random sampling method, the training set (n = 448) and the validation set (n = 193) were constructed in a ratio of 7:3. The delirium status of patients was evaluated by professionally trained doctors using the delirium assessment scale with high sensitivity and specificity: the Intensive Care Unit Confusion Assessment Method (CAM-ICU), which was administered three times a day (8 am, 4 pm, and 12 am) until the patient developed delirium or was discharged from the ICU.11 This study was reviewed and approved by the Medical Ethics Committee of Yancheng Third People’s Hospital (Ethics Approval: 2023–22), and was granted approval for obtaining participant authorization through oral informed consent. All study participants provided verbal consent to participate in the research before the study commenced. The researchers thoroughly explained the study’s purpose, procedures, and potential risks to the participants. After comprehensively understanding the relevant information, the participants voluntarily agreed to participate.
This research screened and identified the relevant risk factors for delirium through a systematic literature review. A standardized questionnaire was developed based on the evidence gathered. Clinical data from all patients were collected using the electronic medical record system of our hospital. The data extraction process was independently performed by two researchers who underwent unified training to ensure the reliability and consistency of data collection. Baseline data include age, sex, medical history (hypertension, diabetes, heart disease, stroke history), length of hospital stay, Acute Physiology And Chronic Health Evaluation II (APACHEII). Clinical data include emergency surgery, duration of mechanical ventilation, degree of coma (GCS score), metabolic acidosis (PH < 7.35), use of sedatives and analgesics, and disease classification (trauma, nervous system, cardiovascular surgery). Biological indicators: NLR (neutrophil/lymphocyte ratio), C-reactive protein (hs-CRP), white blood cell count (WBC), procalcitonin (PCT), blood urea nitrogen (BUN), creatinine (Cr), alanine aminotransferase (ALT), aspartate aminotransferase (AST), and blood lactate (Lac).
Statistical Analysis
Data were processed using SPSS version 27.0. All continuous data were subjected to the Shapiro–Wilk normality test (for samples < 1000). Normally distributed data were expressed as mean ± standard deviation, and independent samples t-test was used for inter-group comparisons, while paired samples t-test was employed for intra-group comparisons. For skewed distribution of continuous data, the Mann–Whitney U-test was utilized for inter-group comparisons. Categorical data were expressed as percentages, with the chi-square test applied for analysis; pairwise comparisons among multiple groups were corrected using the Bonferroni method, with the significance level α adjusted to the original α level divided by the number of comparisons. Logistic regression analysis was conducted to examine the factors influencing the occurrence of ICU delirium in patients. A nomogram model predicting the occurrence of ICU delirium was established using R language (version 4.1.0) along with the rms package. The caret package was employed to perform bootstrap methods to calculate the concordance index (C-index) for model validation. A decision curve was plotted with net benefit as the vertical axis and high-risk threshold as the horizontal axis to analyze the predictive value of the nomogram model for the occurrence of ICU delirium in patients. The receiver operating characteristic (ROC) curve was drawn to obtain the area under the curve (AUC), which was used to evaluate the predictive performance of the nomogram model for ICU delirium occurrence. An AUC < 0.50 indicates no predictive ability, 0.50 ≤ AUC < 0.70 indicates low predictive ability, 0.70 ≤ AUC < 0.90 indicates moderate predictive ability, and AUC ≥ 0.90 indicates high predictive ability; a P-value < 0.05 was considered statistically significant.
Results
This study included a total of 1062 adult critically ill patients admitted to our hospital between January 2023 and June 2024. Based on the defined inclusion and exclusion criteria, 641 patients were ultimately selected to participate and completed the CAM-ICU assessment. Among these, 448 patients were allocated to the training set for model construction, while 193 patients formed the validation set. A comparison of the baseline data between the two patient groups indicated that the differences in baseline characteristics were not statistically significant (P > 0.05), demonstrating comparability. The specific patient screening process is illustrated in Figure 1, and the details of the baseline information are presented in Table 1.
 |
Table 1 Comparison of Baseline Information Between Training and Validation Sets |
 |
Figure 1 Research object flow chart. |
The Occurrence of Delirium in the ICU
The training set for this study comprised 448 patients, of whom 160 (35.71%) developed ICU delirium, while 288 (64.29%) did not. The results indicated that the GCS scores of patients in the delirium group were significantly lower than those in the non-delirium group (P < 0.05). Furthermore, significant differences were observed between the two groups regarding PCT levels, BUN concentrations, history of emergency surgery, use of sedatives, and the proportion of major cardiac vascular surgeries (P < 0.05). However, no statistically significant differences (P > 0.05) were found when comparing the two groups with respect to other baseline characteristics, as detailed in Table 2.
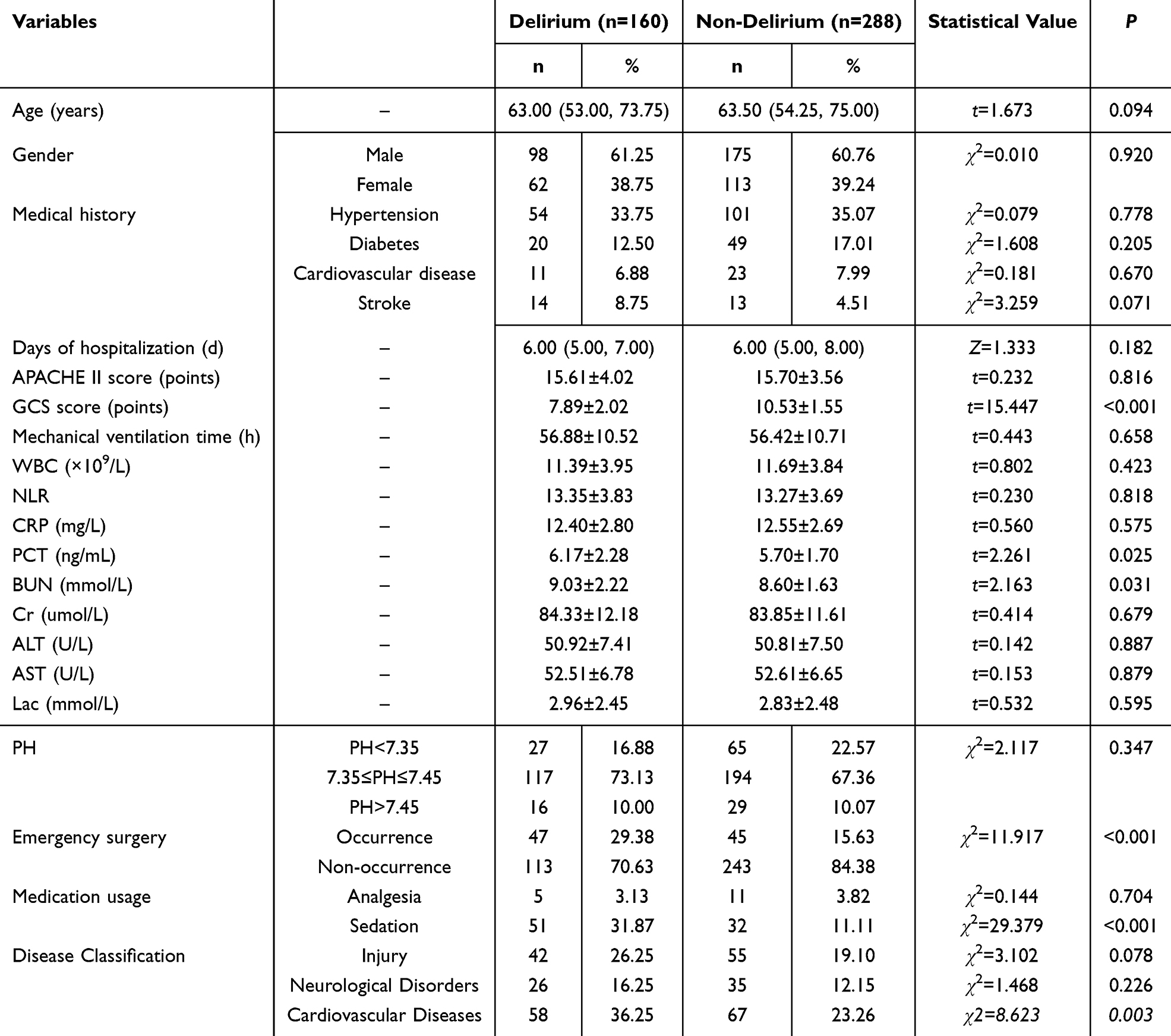 |
Table 2 Comparison of Baseline Information Between the Group That Developed ICU Delirium in the Training Set and the Group That Did Not Develop ICU Delirium |
Factors Influencing the Occurrence of ICU Delirium in Patients Tested by Regression Analysis
In this study, the GCS score, PCT, BUN, emergency surgery, use of sedative drugs, and disease classification related to cardiac macrovascular conditions were included as independent variables. The variable assignments are detailed in Table 3. The occurrence of ICU delirium was designated as the dependent variable, coded as 1 for occurrence and 0 for non-occurrence. The results of the logistic regression analysis indicated that a low GCS score, elevated BUN levels, the presence of emergency surgery, the use of sedative drugs, and the disease classification of cardiac macrovascular conditions were identified as risk factors for the development of ICU delirium (P < 0.05). The results of the multicollinearity analysis indicated that the tolerance values were all less than 1, and the variance inflation factor (VIF) values were all below 10, suggesting that there is no multicollinearity among the factors (Table 4).
 |
Table 3 Assignment of Independent Variables |
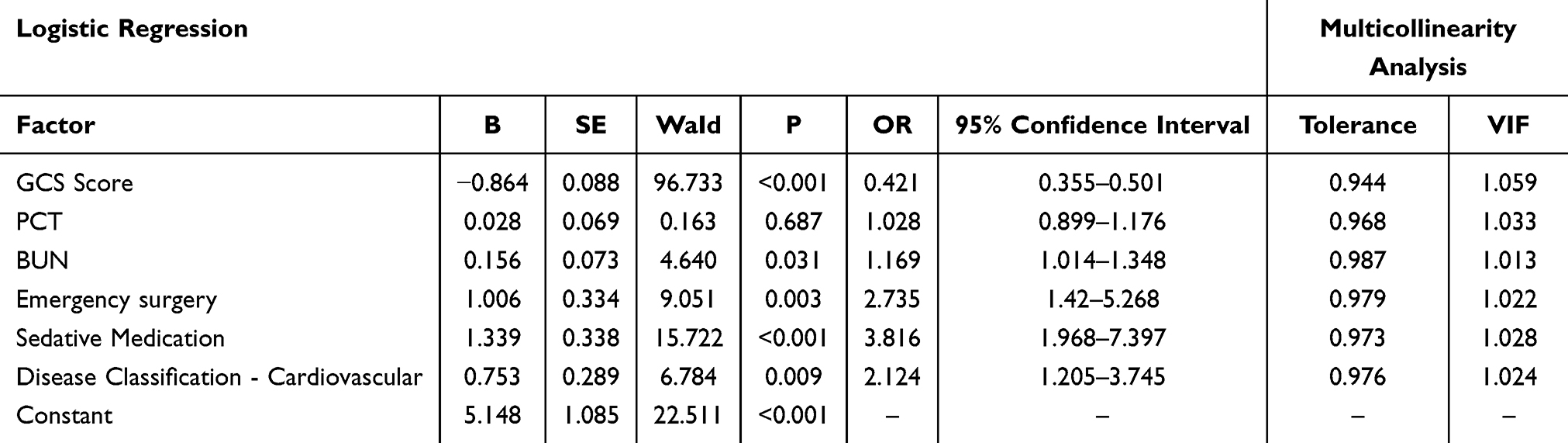 |
Table 4 Regression Analysis of Factors Influencing ICU Delirium in Patients |
Construction of a Nomogram Model for the Prediction of the Occurrence of ICU Delirium
Based on the GCS score, BUN levels, emergency surgery, the use of sedative drugs, and disease classification related to the cardiovascular system, we established a nomogram model to predict the occurrence of ICU delirium, as illustrated in Figure 2A. Additionally, the bootstrap resampling method with 1000 repetitions was employed to validate the nomogram model’s predictive capability for ICU delirium occurrence. The calibration curve closely aligns with the straight-line Y = X, indicating good model calibration. The C-index value is 0.886, and the Hosmer-Lemeshow goodness-of-fit test yielded a statistic of 5.845, demonstrating strong discrimination ability of the model, as shown in Figure 2B. Furthermore, upon plotting the ROC curve, it was observed that the AUC of the nomogram model for predicting the risk of ICU delirium in patients was 0.886, which exceeds the threshold of 0.80, signifying a relatively high predictive value. The corresponding 95% confidence interval, P value, specificity, sensitivity, and Youden index for the AUC were 0.851–0.921, < 0.001, 0.906, 0.763, and 0.669, respectively, as presented in Figure 3A. The ROC curve analysis for the nomogram model performed using the validation set shows that the AUC value of the model for predicting the risk of ICU delirium in patients is 0.913 (> 0.90), indicating a high predictive value. Further analysis shows that the 95% confidence interval for the AUC of this model ranges from 0.869 to 0.957, with a P value of less than 0.001. The model has a specificity of 0.843 and a sensitivity of 0.878, resulting in a Youden index of 0.721. Detailed results are shown in Figure 3B. The decision curve is illustrated in Figure 4A, which shows that when the threshold probability ranges from 0.06 to 0.99, the net benefit is greater than 0, with the maximum net benefit being 0.316. This suggests that constructing a nomogram prediction model for the occurrence of ICU delirium in patients can provide substantial net benefits for clinical application. The decision curve is illustrated in Figure 4B, which shows that when the threshold probability ranges from 0.05 to 0.99, the net benefit is greater than 0, with a maximum net benefit of 0.331. This indicates that the development of a nomogram prediction model for ICU delirium in patients can provide substantial net benefits for clinical application.
 |
Figure 2 The nomogram model and calibration curve for predicting the occurrence of ICU delirium in patients. (A) Nomogram Model: Based on the values of predictive variables such as the GCS, BUN, emergency surgery, sedative drug usage, and cardiovascular status, scores can be obtained on the corresponding point axis (Points). By summing all the scores, the total score (Total Points) can be calculated, which allows for determining the corresponding risk value for ICU delirium on the risk axis (Risk of ICU delirium) at the bottom. (B) Calibration Curve: The curve labeled Apparent in the figure represents the performance of the original model, while Bias-corrected indicates the performance after overfitting correction using the Bootstrap method (1000 repetitions, sample size n=448). The Ideal curve represents the scenario where predictions are completely accurate. The mean absolute error (MAE) is 0.031. |
 |
Figure 3 ROC curve of the nomogram model predicting the risk of ICU delirium. (A) ROC curve of the training set: It demonstrates the ability of the nomogram model to distinguish whether patients will experience ICU delirium in the training dataset. The AUC is 0.886. (B) ROC curve of the validation set: It illustrates the ability of the nomogram model to differentiate whether patients will develop ICU delirium in the independent validation dataset. The AUC is 0.913. Notes: The horizontal axis of the figure represents 1 - Specificity, and the vertical axis represents Sensitivity. |
 |
Figure 4 Decision curve analysis (Training set and Validation set). (A) The x-axis represents the threshold probability, which serves as the cutoff for clinical intervention, while the y-axis displays the net benefit. Three distinct curves are presented: the solid line denotes the Nomogram model, the dashed line represents Intervene all (indicating intervention for all patients), and the dotted line signifies Intervene none (indicating no intervention). The gray shaded area, corresponding to a threshold probability range of 0.06 to 0.99, highlights the interval within which the model provides a positive net benefit that surpasses reference strategies. An arrow indicates the point of maximum net benefit, measured at 0.316. (B) The validation of the nomogram’s clinical utility was conducted in an independent cohort. The gray zone, which represents a threshold probability range of 0.05 to 0.99, delineates the decision-making ranges that are clinically useful. The arrow indicates the point of maximum net benefit, quantified as 0.331. |
Discussion
Currently, the assessment of ICU delirium primarily relies on various clinical scales. In this study, we found that the incidence of delirium in the training set was 35.71% using the CAM-ICU scale, which is largely consistent with the 35.2% reported by Cameron Green et al.12 However, the course of delirium exhibits considerable fluctuations; some patients may be in a non-delirious state at the time of evaluation by medical staff. Furthermore, the use of delirium screening instruments may be influenced by subjective factors or may overlook patients with low-activity delirium. Consequently, misdiagnoses and missed diagnoses are common.13 Early diagnosis and intervention are critical for reducing the duration, severity, and adverse outcomes associated with delirium.14 However, the underlying pathological mechanisms of delirium remain incompletely understood.
Our study identified risk factors associated with ICU delirium through univariate and logistic regression analyses. It was found that a lower GCS score and higher BUN levels within 24 hours of ICU admission, along with emergency surgery, the use of sedative drugs, and postoperative heart and large vessel conditions, were significant risk factors for the development of ICU delirium in patients (P < 0.05). The GCS score serves as an indicator of the level of consciousness in patients admitted to the ICU for various reasons. The findings indicated a negative correlation between GCS scores and the occurrence of ICU delirium, consistent with the meta-analysis summary by Zaal et al,9 which reported that lower GCS scores are associated with a higher risk of developing delirium. Consequently, medical staff in the ICU should closely monitor changes in consciousness levels within the first 24 hours after patient admission. For patients exhibiting severe consciousness disorders, vigilance against delirium is essential. Early prevention and intervention should be prioritized to enhance patient prognosis. BUN, a product of protein catabolism, tends to increase during stress responses in critically ill patients due to heightened catabolism. This metabolic waste can penetrate the blood-brain barrier, leading to neurotoxicity, neuronal invasion, altered consciousness levels, and subsequent delirium.15–17 Our study results indicate that BUN levels in patients who developed delirium were significantly higher than those in patients who did not, establishing it as an independent risk factor for delirium in ICU patients. Clinically, attention should be focused on critically ill patients with elevated BUN levels, and efforts should be made to actively treat the underlying disease and any acute kidney injury to reduce BUN concentration and prevent delirium. The PAD guidelines indicate that emergency surgery is a non-modifiable risk factor, with substantial evidence linking it to the occurrence of delirium.18 Research has demonstrated that delirium is more frequently associated with emergency surgeries compared to elective procedures.19 This increased risk can be attributed to the stress responses elicited by emergency surgeries, which elevate the levels of inflammatory mediators in the body. Such changes can compromise the integrity of the blood-brain barrier, resulting in central nervous system damage and the subsequent onset of delirium.20,21
The 2018 Chinese Adult ICU Analgesia and Sedation Treatment Guidelines indicate that sedation in critically ill patients can alleviate anxiety, prevent resistance to therapeutic interventions, reduce oxygen consumption and associated damage, and facilitate a healthier recovery.22 Notably, the delirium group utilized a greater quantity of sedative medications compared to the non-delirium group. Regression analysis revealed that the incidence of delirium among ICU patients receiving sedative drugs was 3.816 times higher than that of patients not receiving such medications. Salluh et al23 also demonstrated that the administration of the sedative midazolam was significantly associated with delirium (P = 0.009), and excessive sedation was independently linked to delirium, increased ICU mortality, and prolonged hospital stays.24 The use of sedative drugs represents a modifiable factor; therefore, effective management and application of these medications in clinical practice are crucial. This is particularly important for patients on mechanical ventilation, where daily interruptions of sedation and the maintenance of mild sedation should be prioritized.18,25–27
In recent years, brain injuries occurring during the postoperative recovery period of patients undergoing cardiac great vessel surgery have become increasingly common, drawing significant attention from medical professionals. The incidence of delirium in this population exceeds 50%.28–30 Both deep hypothermic circulatory arrest and prolonged extracorporeal circulation time during cardiac surgery can induce neurological inflammatory responses. Additionally, low perfusion and cerebral oxygenation disrupt brain tissue metabolism, potentially leading to brain dysfunction, cognitive alterations, and delirium symptoms in high-risk populations.31–33 To reduce the incidence of postoperative delirium, it is essential not only to implement effective body temperature management, control the duration of cardiopulmonary bypass, and monitor cerebral blood flow, but also to minimize physical restraints in the intensive care unit following surgery. Encouraging early mobilization and improving patients’ sleep quality while adjusting their circadian rhythms can help alleviate negative emotions such as anxiety and tension.34,35 Recent studies have emphasized the potential impact of infectious diseases on the pathological mechanisms of delirium. An analysis by Ertekin et al on hospitalized COVID-19 patients found that advanced age (OR=1.15), hypertension (OR=6.7), and oxygen therapy (OR=7.0) are independent predictors of delirium. This overlaps with the findings of our study, which identified elevated BUN (OR=1.17) and emergency surgery (OR=2.74) as predictors—both indicating the effects of metabolic stress and systemic inflammatory response on neurological function. However, this study also reported that diabetes significantly increases the risk of anxiety (OR=13.95), whereas our study did not observe an association between blood glucose indicators and delirium. This suggests that the driving factors for delirium may differ across various disease contexts, warranting future exploration of their applicability in infected populations.36
This study constructed a nomogram to assess the risk of ICU delirium based on five identified risk factor variables, effectively visualizing complex clinical data. This tool offers convenient and rapid guidance for predicting the risk of delirium in patients entering the ICU within 24 hours. Targeted interventions and management strategies can be implemented for high-risk patients to mitigate the occurrence of delirium, which is worthy of clinical promotion and application. To enhance practical implementation, we recommend integrating the nomogram into ICU electronic information systems for real-time risk assessment. Furthermore, developing a mobile application that alerts physicians when high-risk scores are detected could facilitate early intervention and personalized management strategies. Additionally, the ROC curve and calibration curve of the model were drawn, revealing an AUC of 0.886 in the training set, which exceeds the threshold of 0.80. The model demonstrated a sensitivity of 76.3% and a specificity of 90.6%. The calibration curve indicates a high degree of fit, with a C-index value of 0.886, signifying that the prediction model exhibits good discrimination and calibration. Furthermore, the AUC of the prediction model in the validation set is 0.913, surpassing 0.90, with a sensitivity of 84.3% and a specificity of 87.8%. These results suggest that the prediction model developed in this study possesses a notable degree of repeatability and extrapolability. Compared to the widely used PRE-DELIRIC (AUC = 0.83) and E-PRE-DELIRIC (AUC = 0.85) models, our prediction model exhibited a slightly superior discriminative ability, achieving an AUC of 0.886 in the training set and 0.913 in the validation set. Furthermore, while the PRE-DELIRIC models consider variables such as age, infection, and the use of sedatives, our model integrates BUN and emergency surgery, which may better reflect the specific clinical characteristics of Chinese ICU patients.
This research, a single-center prospective study, has yielded preliminary results in identifying risk factors for delirium; however, it is not without certain limitations. Our study was conducted at a single center, which may limit the generalizability of the findings due to the lack of external validation. Future research should prioritize multicenter validation across diverse geographic and clinical settings to enhance external applicability. Secondly, while significant risk factors have been analyzed, the complexity of delirium pathogenesis suggests that some risk factors may remain unexplored. This gap necessitates further investigation. Moreover, potential unmeasured confounders, such as variations in sedation protocols, nursing interventions, and ICU environments, may also affect the incidence of delirium. These factors should be considered in future studies to improve the robustness of the models used. Additionally, the effectiveness and applicability of the prediction model require validation through multi-center, large-sample clinical trials to ensure its stability and reliability across diverse medical settings. To enhance the model’s predictive accuracy and clinical utility, it is essential to adjust and optimize the included variables and pursue in-depth research to improve the identification of delirium and the reliability of clinical applications.
Conclusion
In this study, we developed and validated a prediction model and nomogram for delirium in ICU patients, demonstrating high predictive efficacy and significant clinical value for early warning. A comparative analysis with established models, such as PRE-DELIRIC and E-PRE-DELIRIC, demonstrates improved applicability in Chinese cohorts. This is achieved through the incorporation of population-specific predictors and a simplified operational workflow for bedside risk assessment, which does not require specialized tools. It is essential for medical staff to thoroughly evaluate patients with high-risk factors for delirium and to implement targeted interventions and treatments as early as possible.
Ethical Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Scientific Research Program of Clinical College of Jiangsu Vocational College of Medicine 20209113.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Stollings JL, Kotfis K, Chanques G, Pun BT, Pandharipande PP, Ely EW. Delirium in critical illness: clinical manifestations, outcomes, and management. Intensive Care Med. 2021;47(10):1089–1103. doi:10.1007/s00134-021-06503-1
2. Krewulak KD, Stelfox HT, Leigh JP, Ely EW, Fiest KM. Incidence and prevalence of delirium subtypes in an adult ICU: a systematic review and meta-analysis. Crit Care Med. 2018;46(12):2029–2035. doi:10.1097/CCM.0000000000003402
3. Szendi I. Delirium: a common complication of severe pathological conditions. Orv Hetil. 2014;155(48):1895–1901. doi:10.1556/OH.2014.30049
4. Mart MF, Williams Roberson S, Salas B, Pandharipande PP, Ely EW. Prevention and management of delirium in the intensive care unit. Semin Respir Crit Care Med. 2021;42(1):112–126. doi:10.1055/s-0040-1710572
5. Teng J, Qin H, Guo W, Liu J, Sun J, Zhang Z. Effectiveness of sleep interventions to reduce delirium in critically ill patients: a systematic review and meta-analysis. J Crit Care. 2023;78:154342. doi:10.1016/j.jcrc.2023.154342
6. van den Boogaard M, Pickkers P, Slooter AJ, et al. Development and validation of PRE-DELIRIC (PREdiction of DELIRium in ICu patients) delirium prediction model for intensive care patients: observational multicentre study. BMJ. 2012;344:e420. doi:10.1136/bmj.e420
7. Wassenaar A, van den Boogaard M, van Achterberg T, et al. Multinational development and validation of an early prediction model for delirium in ICU patients. Intensive Care Med. 2015;41(6):1048–1056. doi:10.1007/s00134-015-3777-2
8. Ouimet S, Kavanagh BP, Gottfried SB, Skrobik Y. Incidence, risk factors and consequences of ICU delirium. Intensive Care Med. 2007;33(1):66–73. doi:10.1007/s00134-006-0399-8
9. Zaal IJ, Devlin JW, Peelen LM, Slooter AJ. A systematic review of risk factors for delirium in the ICU. Crit Care Med. 2015;43(1):40–47. doi:10.1097/CCM.0000000000000625
10. Khan BA, Perkins AJ, Prasad NK, et al. Biomarkers of delirium duration and delirium severity in the ICU. Crit Care Med. 2020;48(3):353–361. doi:10.1097/CCM.0000000000004139
11. Moss SJ, Hee Lee C, Doig CJ, Whalen-Browne L, Stelfox HT, Fiest KM. Delirium diagnosis without a gold standard: evaluating diagnostic accuracy of combined delirium assessment tools. PLoS One. 2022;17(4):e0267110. doi:10.1371/journal.pone.0267110
12. Green C, Bonavia W, Toh C, Tiruvoipati R. Prediction of ICU delirium: validation of current delirium predictive models in routine clinical practice. Crit Care Med. 2019;47(3):428–435. doi:10.1097/CCM.0000000000003577
13. van Eijk MM, van den Boogaard M, van Marum RJ, et al. Routine use of the confusion assessment method for the intensive care unit: a multicenter study. Am J Respir Crit Care Med. 2011;184(3):340–344. doi:10.1164/rccm.201101-0065OC
14. Cherak SJ, Soo A, Brown KN, Ely EW, Stelfox HT, Fiest KM. Development and validation of delirium prediction model for critically ill adults parameterized to ICU admission acuity. PLoS One. 2020;15(8):e0237639. doi:10.1371/journal.pone.0237639
15. Liu M, Liang Y, Chigurupati S, et al. Acute kidney injury leads to inflammation and functional changes in the brain. J Am Soc Nephrol. 2008;19(7):1360–1370. doi:10.1681/ASN.2007080901
16. Wan Y, Wu J, Ni L, et al. Prognosis analysis of patients with mental disorders with COVID-19: a single-center retrospective study. Aging. 2020;12(12):11238–11244. doi:10.18632/aging.103371
17. Pang H, Kumar S, Ely EW, Gezalian MM, Lahiri S. Acute kidney injury-associated delirium: a review of clinical and pathophysiological mechanisms. Crit Care. 2022;26(1):258. doi:10.1186/s13054-022-04131-9
18. Devlin JW, Skrobik Y, Gélinas C, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46(9):e825–e873. doi:10.1097/CCM.0000000000003299
19. Koebrugge B, van Wensen RJ, Bosscha K, Dautzenberg PL, Koning OH. Delirium after emergency/elective open and endovascular aortoiliac surgery at a surgical ward with a high-standard delirium care protocol. Vascular. 2010;18(5):279–287. doi:10.2310/6670.2010.00052
20. Cortese GP, Burger C. Neuroinflammatory challenges compromise neuronal function in the aging brain: postoperative cognitive delirium and Alzheimer’s disease. Behav Brain Res. 2017;322(Pt B):269–279. doi:10.1016/j.bbr.2016.08.027
21. Djaiani G. Cerebral oximetry and postoperative delirium after cardiac surgery - a reply. Anaesthesia. 2018;73(5):648–649. doi:10.1111/anae.14287
22. SOCCMCM A. Guidelines for analgesia and sedation treatment in intensive care unit of Chinese adults. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2018;30(6):497–514. doi:10.3760/cma.j.issn.2095-4352.2018.06.001
23. Salluh JI, Soares M, Teles JM, et al. Delirium epidemiology in critical care (DECCA): an international study. Crit Care. 2010;14(6):R210. doi:10.1186/cc9333
24. Rasulo FA, Badenes R, Longhitano Y, et al. Excessive sedation as a risk factor for delirium: a comparison between two cohorts of ARDS critically ill patients with and without COVID-19. Life. 2022;12(12). doi:10.3390/life12122031.
25. Delaney A, Hammond N, Litton E. Preventing delirium in the intensive care unit. JAMA. 2018;319(7):659–660. doi:10.1001/jama.2018.0159
26. Olsen HT, Nedergaard HK, Strøm T, et al. Nonsedation or light sedation in critically ill, mechanically ventilated patients. N Engl J Med. 2020;382(12):1103–1111. doi:10.1056/NEJMoa1906759
27. Pearson SD, Patel BK. Evolving targets for sedation during mechanical ventilation. Curr Opin Crit Care. 2020;26(1):47–52. doi:10.1097/MCC.0000000000000687
28. Chaud German, Belén Simon, Filippa Pablo, et al. Is the risk of delirium reduced in minimal invasive cardiac surgery. J Cardiol Cardiovasc Ther. 2019;13(1):555879.
29. Pagad S, Somagutta MR, May V, et al. Delirium in cardiac intensive care unit. Cureus. 2020;12(8):e10096. doi:10.7759/cureus.10096
30. Faisal H, Farhat S, Grewal NK, Masud FN. ICU delirium in cardiac patients. Methodist DeBakey Cardiovasc J. 2023;19(4):74.
31. O’Neal JB, Billings FT 4th, Liu X, et al. Risk factors for delirium after cardiac surgery: a historical cohort study outlining the influence of cardiopulmonary bypass. Can J Anaesth. 2017;64(11):1129–1137. doi:10.1007/s12630-017-0938-5
32. Motshabi-Chakane P, Mogane P, Moutlana J, et al. Contemporary neuroprotection strategies during cardiac surgery: state of the art review. Int J Environ Res Public Health. 2021;18(23):12747. doi:10.3390/ijerph182312747
33. Kowalska K, Klimiec E, Weglarczyk K, et al. Reduced ex vivo release of pro-inflammatory cytokines and elevated plasma interleukin-6 are inflammatory signatures of post-stroke delirium. J Neuroinflammation. 2018;15(1):111. doi:10.1186/s12974-018-1156-y
34. Wang J, Ren D, Liu Y, Wang Y, Zhang B, Xiao Q. Effects of early mobilization on the prognosis of critically ill patients: a systematic review and meta-analysis. Int J Nurs Stud. 2020;110:103708. doi:10.1016/j.ijnurstu.2020.103708
35. Lu Y, Li YW, Wang L, et al. Promoting sleep and circadian health may prevent postoperative delirium: a systematic review and meta-analysis of randomized clinical trials. Sleep Med Rev. 2019;48:101207. doi:10.1016/j.smrv.2019.08.001
36. Ertekin H, Kettaş E, Şa K. Psychiatric conditions and delirium in hospitalized patients with COVID-19 during the pandemic. Fam Pract Palliat Care. 2024;9(2):54–59. doi:10.22391/fppc.1404419
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Nomogram for Predicting 28-Day Mortality on Admission in Elderly Patients with Severe Community-Acquired Pneumonia
Song Y, Wang X, Lang K, Wei T, Luo J, Song Y, Yang D
Journal of Inflammation Research 2022, 15:4149-4158
Published Date: 21 July 2022
Tracking Epidemiological Characteristics and Risk Factors of Multi-Drug Resistant Bacteria in Intensive Care Units
Wu C, Lu J, Ruan L, Yao J
Infection and Drug Resistance 2023, 16:1499-1509
Published Date: 15 March 2023
Establishment and Validation of a Nomogram Prediction Model for the Severe Acute Pancreatitis
Li B, Wu W, Liu A, Feng L, Li B, Mei Y, Tan L, Zhang C, Tian Y
Journal of Inflammation Research 2023, 16:2831-2843
Published Date: 8 July 2023
Development and Validation Nomogram for Predicting the Survival of Patients with Thrombocytopenia in Intensive Care Units
Jiang ZH, Zhang GH, Xia JM, Lv SJ
Risk Management and Healthcare Policy 2023, 16:1287-1295
Published Date: 17 July 2023
Dynamic Nomogram for Subsyndromal Delirium in Adult Intensive Care Unit: A Prospective Cohort Study
Cheng J, Lao Y, Chen X, Qiao X, Sui W, Gong X, Zhuang Y
Neuropsychiatric Disease and Treatment 2023, 19:2535-2548
Published Date: 22 November 2023