")
Back to Journals » Journal of Pain Research » Volume 17
Analysis of Risk Factors Causing Adjacent Disc Degeneration After Percutaneous Kyphoplasty for Osteoporotic Vertebral Compression Fractures
Authors Song H, Wang A, Zang L , Wang T, Yuan S , Fan N, Du P
Received 11 July 2024
Accepted for publication 13 November 2024
Published 25 November 2024 Volume 2024:17 Pages 3985—3995
DOI https://doi.org/10.2147/JPR.S486668
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Krishnan Chakravarthy
He Song,* Aobo Wang,* Lei Zang, Tianyi Wang, Shuo Yuan, Ning Fan, Peng Du
Department of Orthopedics, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lei Zang, Department of Orthopedics, Beijing Chaoyang Hospital, Capital Medical University, 5 JingYuan Road, Shijingshan District, Beijing, 100043, People’s Republic of China, Tel +86-010-51718268, Email [email protected]
Purpose: Adjacent disc degeneration (ADD) is a common postoperative complication after percutaneous kyphoplasty (PKP). However, risk factors for ADD after PKP have not been reported. This study aimed to determine whether osteoporotic vertebral compression fracture (OVCF) following PKP is associated with a high risk for ADD and to identify the risk factors for ADD.
Patients and methods: Consecutive patients who underwent PKP at our center between January 2015 and January 2021 were retrospectively reviewed. The incidence of ADD was calculated and specific subgroups of ADD were identified. Demographic, clinical baseline, and radiologic data were analyzed using univariate and multivariate analyses to identify the risk factors associated with ADD.
Results: 130 eligible patients were included, and the incidence rate of ADD distinct from primary degeneration was 42.3%. Patients with OVCFs who underwent PKP had a high risk of developing ADD. The independent risk factors included the presence of intradiscal cement leakage (ICL; odds ratio [OR] 6.292; 95% confidence interval [CI] 2.588– 15.299; P < 0.001) and pre-operative cranial disc of the injured vertebrae degeneration (Pfirrmann grade ≥IV; OR 3.575; 95% CI 1.515– 8.438; P = 0.004).
Conclusion: Patients with OVCFs who underwent PKP were more likely to develop ADD, and most of the degenerated discs occurred in the vertebrae above the level of injury. ICL and pre-operative cranial disc of the injured vertebrae degeneration (Pfirrmann grade ≥IV) were independent risk factors for developing ADD in these patients.
Keywords: adjacent disc degeneration, percutaneous kyphoplasty, osteoporotic vertebral compression fracture, risk factors
Two Letters to the Editor have been received and published for this article
Introduction
Osteoporotic vertebral compression fracture (OVCF) is an important cause of disability in the elderly.1 About one-fifth of individuals aged >40 years will experience at least one vertebral fracture during their lifetime, and one-third of patients with compression fracture will suffer long-term pain or even disability.2,3 Conventional treatments of OVCFs include medications, bed rest, and bracing.4 However, previous studies have reported that conservative treatment failed in 35%–41% of OVCF cases.5 Therefore, percutaneous kyphoplasty (PKP), a minimally invasive surgical, is widely used for this type of fracture because of its rapid pain relief, partial vertebral height restoration, and wedge deformity reversion.
Despite its overall success, our team have reported that 44.2% of OVCF patients treated with PKP developed adjacent disc degeneration (ADD) that was distinguished from primary degeneration.6 Generally, Primary degeneration of intervertebral discs are characterized by degradation of the extracellular matrix and a reduction in the number of nucleus pulposus (NP) cells, and greater than 90% of people over the age of 50 present with degeneration of the intervertebral disc.7,8 However, bone cement accelerates this process by blocking the blood supply and increasing the axial stress of the adjacent disc after PKP.9,10 Although disc degeneration does not directly cause symptoms, it can significantly increase the stress on the endplate of the adjacent vertebrae and have a complex effect on the adjacent vertebrae.11,12 Moreover, PKP increased the risk of new-onset adjacent level fractures.13 The risk factors of these conditions include age, low body mass index (BMI), low bone mineral density (BMD), cement leakage to the disk space, thoracolumbar junction fracture, degree of vertebral height restoration, and sagittal imbalance.14
Currently, the effects of cement augmentation on discs adjacent to the fracture site is controversial. Theoretically, PKP-induced ADD is associated with thermal damage, mechanical effects, and blockage of the nutritional pathway.15–17 However, some studies found that the disc degeneration after PKP is a natural course rather than a complication of surgical intervention. In a long-term follow-up study, König et al reported that there was no ADD after PKP treatment of OVCF.18 Moreover, in their analysis of vertebral cement augmentation and its effects on sheep spine, Krebs et al showed that concerns regarding adjacent segment disc degeneration after PKP were unsubstantiated.19 However, several studies have argued an increased risk of ADD after PKP, with an incidence rate ranging from 34% to 52.6%.11,20 Most of these degenerations occur in the cranial disc.21 Considering the lack of comprehensive studies, the factors that affect ADD after PKP remain unknown.
Therefore, this study aimed to investigate whether PKP increases the risk of ADD distinct from primary degeneration and the risk factors associated with ADD.
Method
Study Subjects
Patients who underwent PKP in the orthopedics department of our hospital from January 2015 to January 2021 were selected. Osteoporosis was diagnosed by measuring the Hounsfield unit (HU) on computed tomography (CT): L1 ≤ 110 HU.22,23 The inclusion criteria were as follows: (1) age >55 years; (2) clinical findings and radiographic results confirming the presence of T5–L5 OVCFs; and (3) treatment with PKP. The exclusion criteria were as follows: (1) patients with a history of spine surgery; (2) patients with incomplete data or lost data within two years of follow-up; (3) multilevel PKP in initial surgery; and (4) pre-operative spinal tumor, infection, or deformity. The present study was approved by the institutional ethical review board of our hospital, and informed consent was waived because of its retrospective nature.
Diagnosis and Measurement of Disc Degeneration
Anteroposterior and lateral X-ray imaging of the spine, three-dimensional CT, and magnetic resonance imaging (MRI) were conducted. Spinal radiography or CT was performed within three days after PKP. All patients received regular outpatient follow-up including radiography, CT, and MRI, for at least two years. The occurrence of ADD was confirmed based on MRI. According to a previously validated protocol, the detailed criteria for post-operative ADD were as follows: (1) >10% loss of disc height or (2) new-onset Pfirrmann grade ≥ IV (Figure 1).6,11 Disc height was measured as the mean distance of the anterior, median, and posterior disc height on mid-sagittal MRI T2-weighted sequences. The degree of disc degeneration was graded according to the grading system proposed by Pfirrmann et al.24 The imaging data of all patients were measured by two surgeons, and the average value was considered as the final result. Then, the intra- and inter-reader correlation coefficients (intra-class correlation coefficients [ICCs]) were calculated.
 |
Figure 1 Illustrative case of a 79-year-old woman who developed ADD after PKP treatment for OVCF. Pre-operative CT (A). T2-weighted sequences showing OVCF (white arrows) at L1 and the height of the upper disc of L1 vertebra was 7.3mm (B). About 12 months after the initial PKP, intradiscal cement leakage (ICL) was observed in the superior disc (white arrows) on sagittal CT (C). More than 10% decrease of the height of upper disc of L1 (6.3mm) was observed on MRI T2-weighted sequences, whereas progression of degeneration was not detected in the control segments (D). |
As age increases, the elderly patient may experience primary disc degeneration. To distinguish primary degeneration, we also recorded the degeneration of the upper and lower discs of the adjacent non-traumatized vertebra (n+2 and n-2) as control segments. This is based on the assumption that adjacent segments have similar degeneration rates due to similar biomechanics, However, the biomechanical effects of PKP mainly concentrate on the discs adjacent to the fractured vertebra (n – 1 and n + 1).16 In this study, patients who developed ADD without control disc degeneration (CDD) were defined as the ADD group, and the other patients were defined as the control group (Figure 2).
 |
Figure 2 T2-weighted MR image of the sagittal plane. n – 1, upper disc of the fractured vertebra; n + 1, lower disc of the fractured vertebra; n – 2, upper disc of the cranial non-traumatized vertebra; n + 2, lower disc of the caudal non-traumatized vertebra. |
Surgical Methods
The PKP procedure was performed under local anesthesia with the patient in a prone position. The C-arm fluoroscopy system was used to visualize the anteroposterior image of the spine and to mark the pedicle location of the injured vertebra. Under the guidance of the fluoroscopy system, the puncture needle and inflatable balloon (Medtronic Sofamor Danek, Memphis, TN, USA) were introduced through the working channel into the injured vertebral body to create a cavity. Subsequently, the balloon was deflated and removed. Then, viscous polymethyl methacrylate (Mendec Spine Cement; Tecres SPA, Verona, Italy) was injected, and X-ray imaging was performed to ensure that there was no bone cement leakage. Patients remained on bed rest on the day of the procedure. On the following day, they were permitted to walk with orthotic support. Patients were routinely given anti-osteoporosis medications and non-steroidal anti-inflammatory drugs after surgery.
Radiological Analysis and Risk Factors for ADD Development
Patients’ perioperative baseline data on ADD risk factors (eg, age, sex, BMI, smoking history, diabetes mellitus, hyperlipidemia, time of injury before surgery, fracture location, cement volume, and follow-up period) were obtained from their medical records. In addition, radiologic data (eg, fracture type, fracture severity, presence of endplate cortical disruption, intravertebral cleft [IVC], intradiscal cement leakage [ICL], and BMD) were collected. Fracture types (wedge, biconcave, and crush) and fracture severity (mild, <25% reduction in vertebral height; moderate,25%-40% reduction in vertebral height; and severe, > 40% reduction in vertebral height) were classified according to the guidelines of Genant et al.25 The preoperative disc height in the risk factor analysis was calculated as the average height of the superior, median, and inferior disc heights (Figure 3A). The vertebral wedge angle was evaluated using lateral radiographs and defined as the angle between the superior and inferior endplates of the fractured vertebra. The segmental kyphotic angle was defined as the angle between the inferior endplate of the superior vertebra and the superior endplate of the inferior vertebra (Figure 3B). Endplate cortical disruption was defined as evident discontinuation of cortical hypointensity at the endplates and/or wall of the vertebral body on pre-operative sagittal CT and MRI (Figure 3C and D).26 IVC was defined as a well-demarcated, linear, or cystic hyperintensity similar to air on T1-weighted images and/or hyperintensity similar to cerebrospinal fluid on fat-saturated T2-weighted images (Figure 3E–G).27 ICL occurrence was assessed on post-operative CT of the treated area (Figure 3H). Furthermore, the pre-procedural BMD of all spinal levels was reviewed using the T-score, measured by dual-energy X-ray absorptiometry (GE Healthcare-LUNAR, Madison, WI, USA).
 |
Figure 3 Radiographic measurement of OVCFs. Points a and c represent the anteroinferior and posteroinferior margins of the superior vertebra, respectively. Points b and d represent the margins of the inferior vertebra. Meanwhile, points e and f are intersections of the extension lines of the midpoints of lines ac and bd to the superior vertebra (inferior endplate) and inferior vertebra (superior endplate), respectively (A). The segmental kyphotic (α) and vertebral wedge angles (β) were measured on the lateral radiograph (B). Endplate cortical disruption was indicated by white arrows in the pre-operative sagittal CT (C) and T2-weighted images (D). The white arrows indicate intravertebral cleft (IVC) identified by a gas-like density shown on pre-operative CT (E), hypointensity shown on pre-operative T1-weighted MR sequences (F), and hyperintensity shown on T2 short-tau inversion recovery MR images (G). Intradiscal leakage was indicated by white arrows in the post-operative radiographs (H). |
Statistical Analysis
All statistical analyses were performed using SPSS 25.0 (IBM, Armonk, NY, USA) software. Data are expressed as mean ± standard deviation or median (interquartile range), whereas count data are expressed as the number of cases and percentage. ICC was used to examine measurement reliability. The paired t test and McNemar–Bowker test were used to compare the pre-operative and post-operative results of each group. Univariate analyses including Student’s t test, Mann–Whitney U-test and chi-square test or Fisher’s exact test were performed to screen the potential risk factors for ADD. Variables with P < 0.05 in the univariate analyses were further included in the logistic regression models. Multivariate logistic regression was used to analyze the factors affecting ADD in patients with OVCF. Statistical significance was considered at P < 0.05.
Results
General Characteristics of Patients
One hundred and thirty patients, including 21 males and 109 females, with mean age of 72.59 ± 9.58 years, were included in this study. The mean BMI was 24.24 ± 4.64 kg/m2. In terms of fractures location, 10 (7.7%) fractures occurred in the thoracic vertebrae (T1–T9), 98 (75.4%) in the thoracolumbar vertebrae (T10–L2), and 22 (16.9%) in the lower lumbar vertebrae (L3–L5). The mean time of injury before surgery was seven days. The average follow-up period was 38.27 ± 13.87 months, and the overall incidence of ADD was 75.6%. After considering primary degeneration, the incidence of ADD was adjusted to 42.3% (Table 1). Inter- and intra-reader reproducibility were achieved, with intra-reader and inter-observer ICCs ranging from 0.874 to 0.906 and from 0.823 to 0.891, respectively.
 |
Table 1 Patients’ Information |
Progressions of ADD
Pre-operative adjacent disc height and Pfirrmann grade developed significantly during the follow-up period (P <0.05). However, no apparent progression (P < 0.05) of CDD (n + 2, n – 2) was observed, except for the decreased signal of post-operative n + 2 disc (P = 0.015). According to our criteria, a higher proportion (99/130) of cranial disc degeneration appeared in MRI scan than in caudal disc (Table 2).
 |
Table 2 Overall Progression of Disc Degenerations After PKP |
Risk Factor Analysis
In the univariate analysis of demographic and baseline clinical data (Table 3), no statistically significant differences were observed between the two groups. However, among the radiological variables (Table 4), the presence of endplate cortical disruption, IVC, ICL, and higher pre-operative Pfirrmann grade of the n – 1 intervertebral disc differed significantly between the groups. The variable assignment of multivariate logistic regression is presented in Table 4. The presence of ICL and pre-operative disc degeneration (Pfirrmann grade of n – 1 disc ≥IV) were independent risk factors of ADD in patients with OVCF (Table 5).
 |
Table 3 Univariate Analysis of Demographic and Baseline Clinical Data for ADD |
 |
Table 4 Univariate Analysis of Radiological Variables for ADD |
 |
Table 5 Multivariate Logistic Analysis for ADD |
Occurrence of Fractures
The influence of ADD on the prognosis of patients who underwent PKP was further analyzed. The results showed that 58 (44.6%) patients developed new vertebral fractures during the follow-up period: 26 (20.0%) patients with adjacent segment fractures (ASFs), 10 (7.7%) patients with control segment fractures (CSFs), and 22 (16.9%) patients with other segment fractures. In the ADD group, 21(38.2%) patients experienced ASF after developing ADD, whereas only four (7.3%) patients experienced CSF. The number of patients experiencing ASF is greater than that of patients experiencing CSF. Compared with the control group, the ADD group was more likely to progress to ASF (P=0.017, Figure 4).
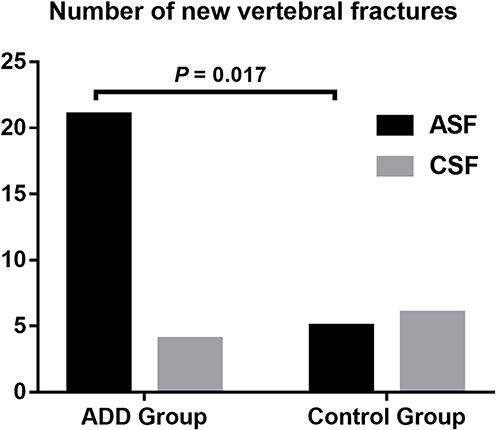 |
Figure 4 Histogram showing the number of ASFs and CSFs in the ADD and control groups. Abbreviations: ADD, adjacent disc degeneration; ASF, adjacent segment fracture; CSF, control segment fracture. |
Discussion
Although ADD after PKP has been described in previous studies, to the best of our knowledge, the present study is the first to determine whether such individuals have a higher risk of developing ADD and to identify its risk factors.6,11,28 This study revealed that the incidence of ADD was 42.3%, and most of these degenerations occurred in the cranial disc. Pre-operative disc height and disc signal developed significantly in patients who underwent PKP with OVCFs. The presence of ICL and pre-operative disc degeneration (Pfirrmann grade of n – 1 disc ≥IV) were the most important independent risk factors for ADD.
Consistent with literature, our study revealed that disc degeneration may have a negative impact on the prognosis of patients after PKP. Although several studies have shown no direct correlation between ADD and pain symptoms of patients, the present study found that patients with ADD had a higher incidence of ASF compared to those without.11,20 There are two main reasons for this finding. First, disc degeneration reduces its ability to absorb mechanical stress. Second, decreased disc height can lead to increased kyphosis, resulting in stress concentration.29 When an axial load is applied to the spine, the NP generates hydrostatic pressure, which radiates the load to the annulus fibrosus to counteract the compressive load on the center of the endplate. However, intervertebral disc degeneration will significantly increase the stress on the endplate of the adjacent vertebral body, which can lead to fractures.3,12 Therefore, it is important to explore whether PKP increases the risk of developing ADD in patients with OVCFs.
In the present study, 42.3% of adjacent intervertebral discs experienced degeneration distinct from the primary process after PKP treatment of OVCFs. Consistent with our results, Wu et al concluded that cementing procedures accelerated disc degeneration adjacent to the fractured vertebra based on a modified Pfirrmann grading system.30 Despite disc degeneration being observed in the final images, their study did not observe a reduction in disc height, which may be related to the different measurement of intervertebral disc height and shorter follow-up time. However, some scholars believe that PKP has no effect on ADD. Noriega et al conducted MR diffusion-weighted imaging on patients receiving PVP for OVCF; they found that PVP could prevent disc degeneration and that bone cement did not affect vertebral blood supply.31 However, we believe that PKP had adverse effects on adjacent discs. According to a previous study, bone cement can damage adjacent discs and high temperatures during the formation of exothermic cement can accelerate their degeneration.32 Animal models demonstrated that the inhibition of each endplate pathway with cement injection may block the nutritional route of the endplate and that severe inhibition of the nutritional pathway of the endplate may result in intervertebral disc degeneration.33 Additionally, a finite element study found that rigid cement augmentation resulted in elevated pressure in the NP.34 Recently, another study revealed that bone cement can induce disc degeneration by downregulating connective tissue growth factor through the Hippo/YAP pathway.35 Given these findings, ADD may be attributed to the combined effects of biomechanical and metabolic factors associated with PKP.
We first found that pre-operative disc degeneration (Pfirrmann grade of n – 1 disc ≥IV) is a risk factor for post-operative ADD, and many previous literatures supported this conclusion. In their retrospective study, Wang et al found that decreased of pre-operative disc height increases the risk of developing radiographic adjacent segment degeneration, with disc degeneration being the most common type.6 Furthermore, Kim et al reported that pre-existing disc degeneration increases the risk of radiologic adjacent segment degeneration after lumbar fusion.36 A finite element study also showed that the presence of ADD before surgery increases adjacent segment motions, leading to adjacent segment disc disease.37 The degeneration of the intervertebral disc, an important structure connecting the fractured and adjacent vertebra, is closely related to the creep deformation of the fractured and adjacent vertebra, new fractures, and aggravation of segment kyphosis, which can lead to further disc degeneration.38,39
In the present study, most degenerated discs occurred above the injured vertebrae. We believe that this is because the upper endplate is relatively fragile and endplate cortical disruption and ICL mostly occur in cranial discs. ICL is a crucial trigger for ADD.40 The main reasons are as follows: First, ICL can directly harm regular disc structures, resulting increased intradiscal pressure.41 Second, the direct interaction of cement with the internal environment of the intervertebral disc triggers various biochemical responses in disc cells, including apoptosis induction and proliferation inhibition.42 Consistent with our results, Wu et al and Shen et al found that the quantity of cement leaking into the disc space is positively correlated with the progression rate of disc degeneration.28,30 Therefore, surgeons should reduce the risk of ICL by estimating of a suitable threshold of injected cement meticulously expanding the balloon and filling with cement, and performing detailed intraoperative fluoroscopy to further lower the risk of ADD.43
This study has several limitations. First, it is a retrospective in nature and was conducted in a single center, which may have led to selection bias. Further validation with prospective multicenter studies is required. Second, we did not investigate ADD combined with clinical symptoms because most patients had no obvious clinical symptoms. Therefore, we could not draw a clear relationship between radiographic and clinical ADD in patients with OVCFs treated with PKP. Third, the evaluation of primary disc degeneration was based on the assumption that the control discs (n + 2 and n - 2) were less affected by PKP, since single-level intervention did not alter the range of motion of the index spinal unit. Although our results showed that pre-operative degeneration progressed more in adjacent discs than in control discs, these findings still need to be verified by further studies.
Conclusion
Patients with OVCFs who undergo PKP are more likely to develop ADD, and its progression is distinct from primary degeneration. Furthermore, ICL and pre-operative disc degeneration (Pfirrmann grade of n – 1 disc ≥IV) are independent risk factors for ADD. Prospective multicenter studies are needed to further validate our findings.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
The research conducted has been performed in accordance with the Declaration of Helsinki. Approval for the study was obtained from the ethics committees of the Beijing Chaoyang Hospital (2022-KE-15). Informed consent to this study was waived because of this was a retrospective study, which was also approved by the institutional ethical review board. All patient data were anonymized and kept strictly confidential after completion of collection, and the manuscript did not contain any private information that could identify the patient.
Funding
There is no funding that supported this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ballane G, Cauley JA, Luckey MM, El-Hajj Fuleihan G. Worldwide prevalence and incidence of osteoporotic vertebral fractures. Osteoporos Int. 2017;28(5):1531–1542. doi:10.1007/s00198-017-3909-3
2. Wang L, Yu W, Yin X, et al. Prevalence of Osteoporosis and Fracture in China: the China Osteoporosis Prevalence Study. JAMA Netw Open. 2021;4(8):e2121106. doi:10.1001/jamanetworkopen.2021.21106
3. Rahmani MS, Takahashi S, Hoshino M, et al. The degeneration of adjacent intervertebral discs negatively influence union rate of osteoporotic vertebral fracture: a multicenter cohort study. J Orthop Sci. 2018;23(4):627–634. doi:10.1016/j.jos.2018.03.008
4. Lee HM, Park SY, Lee SH, Suh SW, Hong JY. Comparative analysis of clinical outcomes in patients with osteoporotic vertebral compression fractures (OVCFs): conservative treatment versus balloon kyphoplasty. Spine J off J North Am Spine Soc. 2012;12(11):998–1005. doi:10.1016/j.spinee.2012.08.024
5. Zhang J, He X, Fan Y, Du J, Hao D. Risk factors for conservative treatment failure in acute osteoporotic vertebral compression fractures (OVCFs). Arch Osteoporos. 2019;14(1):24. doi:10.1007/s11657-019-0563-8
6. Wang T, Si F, Zang L, et al. Radiographic adjacent segment degeneration and risk factors for osteoporotic vertebral compression fractures treated with percutaneous kyphoplasty. Int Orthop. 2022;46(11):2619–2628. doi:10.1007/s00264-022-05510-1
7. Sun K, Yan C, Dai X, et al. Catalytic Nanodots‐Driven Pyroptosis Suppression in Nucleus Pulposus for Antioxidant Intervention of Intervertebral Disc Degeneration. Adv Mater. 2024;36(19):2313248. doi:10.1002/adma.202313248
8. Krut Z, Pelled G, Gazit D, Gazit Z. Stem Cells and Exosomes: new Therapies for Intervertebral Disc Degeneration. Cells. 2021;10(9):2241. doi:10.3390/cells10092241
9. Farooq N, Park JC, Pollintine P, Annesley-Williams DJ, Dolan P. Can Vertebroplasty Restore Normal Load-Bearing to Fractured Vertebrae? Spine. 2005;30(15):1723–1730. doi:10.1097/01.brs.0000171906.01906.07
10. Feng Z, Chen L, Hu X, Yang G, Chen Z, Wang Y. Vertebral Augmentation can Induce Early Signs of Degeneration in the Adjacent Intervertebral Disc: evidence from a Rabbit Model. Spine. 2018;43(20):E1195–E1203. doi:10.1097/BRS.0000000000002666
11. Qian J, Yang H, Jing J, et al. The Early Stage Adjacent Disc Degeneration after Percutaneous Vertebroplasty and Kyphoplasty in The Treatment of Osteoporotic VCFs. PLoS One. 2012;7(10):e46323. doi:10.1371/journal.pone.0046323
12. Holm S, Holm AK, Ekström L, Karladani A, Hansson T. Experimental Disc Degeneration Due to Endplate Injury. J Spinal Disord Tech. 2004;17(1):64–71. doi:10.1097/00024720-200402000-00012
13. Trout AT, Kallmes DF, Kaufmann TJ. New fractures after vertebroplasty: adjacent fractures occur significantly sooner. AJNR Am J Neuroradiol. 2006;27(1):217–223.
14. Takahara K, Kamimura M, Moriya H, et al. Risk factors of adjacent vertebral collapse after percutaneous vertebroplasty for osteoporotic vertebral fracture in postmenopausal women. BMC Musculoskelet Disord. 2016;17(1):12. doi:10.1186/s12891-016-0887-0
15. Hutton WC, Murakami H, Li J, et al. The Effect of Blocking a Nutritional Pathway to the Intervertebral Disc in the Dog Model. J Spinal Disord Tech. 2004;17(1):53–63. doi:10.1097/00024720-200402000-00011
16. Rohlmann A, Zander T, Bergmann G. Spinal loads after osteoporotic vertebral fractures treated by vertebroplasty or kyphoplasty. Eur Spine J. 2006;15(8):1255–1264. doi:10.1007/s00586-005-0018-3
17. Kobayashi N, Togawa D, Fujishiro T, et al. Histological and radiographic evaluation of polymethylmethacrylate with two different concentrations of barium sulfate in a sheep vertebroplasty model. J Biomed Mater Res A. 2005;75(1):123–127. doi:10.1002/jbm.a.30388
18. König MA, Panzer S, Schulz J, Bierschneider M, Boszczyk BM. Magnetic resonance imaging changes of intervertebral discs after kyphoplasty. Eur Spine J. 2015;24(4):724–733. doi:10.1007/s00586-014-3244-8
19. Krebs J, Ferguson SJ, Goss BG, Stauffer E, Ettinger L, Aebli N. Effect of vertebral cement augmentation with polymethylmethacrylate on intervertebral disc and bone tissue. J Biomed Mater Res B. 2012;100(3):660–667. doi:10.1002/jbm.b.31990
20. Marie-Hardy L, Barut N, Sari Ali H, Khalifé M, Pascal-Moussellard H. Evaluation of disc degeneration adjacent to AOspine A fractures: pre- and post-operative MRI analysis. SICOT-J. 2020;6:33. doi:10.1051/sicotj/2020032
21. Collinet A, Charles YP, Ntilikina Y, Tuzin N, Steib JP. Analysis of intervertebral discs adjacent to thoracolumbar A3 fractures treated by percutaneous instrumentation and kyphoplasty. Orthop Traumatol Surg Res OTSR. 2020;106(6):1221–1226. doi:10.1016/j.otsr.2020.05.006
22. Luo Y, Jiang T, Guo H, Lv F, Hu Y, Zhang L. Osteoporotic vertebral compression fracture accompanied with thoracolumbar fascial injury: risk factors and the association with residual pain after percutaneous vertebroplasty. BMC Musculoskelet Disord. 2022;23(1):343. doi:10.1186/s12891-022-05308-7
23. Zou D, Li W, Deng C, Du G, Xu N. The use of CT Hounsfield unit values to identify the undiagnosed spinal osteoporosis in patients with lumbar degenerative diseases. Eur Spine J. 2019;28(8):1758–1766. doi:10.1007/s00586-018-5776-9
24. Pfirrmann CWA, Metzdorf A, Zanetti M, Hodler J, Boos N. Magnetic Resonance Classification of Lumbar Intervertebral Disc Degeneration. Spine. 2001;26(17):1873–1878. doi:10.1097/00007632-200109010-00011
25. Genant HK, Wu CY, Van Kuijk C, Nevitt MC. Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res. 2009;8(9):1137–1148. doi:10.1002/jbmr.5650080915
26. Wang G, Yang H, Chen K. Osteoporotic vertebral compression fractures with an intravertebral cleft treated by percutaneous balloon kyphoplasty. J Bone Joint Surg Br. 2010;92(11):1553–1557. doi:10.1302/0301-620X.92B11.24671
27. Nieuwenhuijse MJ, Van Rijswijk CSP, Van Erkel AR, Dijkstra SPD. The Intravertebral Cleft in Painful Long-Standing Osteoporotic Vertebral Compression Fractures Treated With Percutaneous Vertebroplasty: diagnostic Assessment and Clinical Significance. Spine. 2012;37(11):974–981. doi:10.1097/BRS.0b013e318238bf22
28. Shen M, Niu J, Zhou H, Meng Q, Gan M, Yang H. Adjacent disc height reduction and clinical outcome after intradiscal cement leakage. Int J Spine Surg. 2016;10:34. doi:10.14444/3034
29. Tao W, Biao W, Xingmei C, et al. Predictive Factors for Adjacent Vertebral Fractures After Percutaneous Kyphoplasty in Patients With Osteoporotic Vertebral Compression Fracture. Pain Physician. 2022;25(5):E725–E732.
30. Wu T, Han X, Tian W, Wang L, Wang C. Effect of Percutaneous Kyphoplasty on the progression of intervertebral disc degeneration: a retrospective cohort study. J Orthop Surg. 2023;18(1):172. doi:10.1186/s13018-023-03627-6
31. Natarajan RN, Andersson GBJ. Lumbar disc degeneration is an equally important risk factor as lumbar fusion for causing adjacent segment disc disease. J Orthop Res. 2017;35(1):123–130. doi:10.1002/jor.23283
32. Belkoff SM, Molloy S. Temperature measurement during polymerization of polymethylmethacrylate cement used for vertebroplasty. Spine. 2003;28(14):1555–1559. doi:10.1097/01.BRS.0000076829.54235.9F
33. Yin S, Du H, Zhao W, et al. Inhibition of both endplate nutritional pathways results in intervertebral disc degeneration in a goat model. J Orthop Surg. 2019;14(1):138. doi:10.1186/s13018-019-1188-8
34. Keller TS, Kosmopoulos V, Lieberman IH. Vertebroplasty and Kyphoplasty Affect Vertebral Motion Segment Stiffness and Stress Distributions: a Microstructural Finite-Element Study. Spine. 2005;30(11):1258–1265. doi:10.1097/01.brs.0000163882.27413.01
35. Ge J, Yang H, Chen Y, Yan Q, Wu C, Zou J. PMMA Bone Cement Acts on the Hippo/YAP Pathway To Regulate CTGF and Induce Intervertebral Disc Degeneration. ACS Biomater Sci Eng. 2019;5(7):3293–3302. doi:10.1021/acsbiomaterials.9b00146
36. Kim JY, Ryu DS, Paik HK, et al. Paraspinal muscle, facet joint, and disc problems: risk factors for adjacent segment degeneration after lumbar fusion. Spine J. 2016;16(7):867–875. doi:10.1016/j.spinee.2016.03.010
37. Raj PP. Intervertebral Disc: anatomy-Physiology-Pathophysiology-Treatment. Pain Pract. 2008;8(1):18–44. doi:10.1111/j.1533-2500.2007.00171.x
38. Lu X, Yang J, Zhu Z, et al. Changes of the adjacent discs and vertebrae in patients with osteoporotic vertebral compression fractures treated with or without bone cement augmentation. Spine J. 2020;20(7):1048–1055. doi:10.1016/j.spinee.2020.02.012
39. Lu X, Zhu Z, Pan J, et al. Traumatic vertebra and endplate fractures promote adjacent disc degeneration: evidence from a clinical MR follow-up study. Skeletal Radiol. 2022;51(5):1017–1026. doi:10.1007/s00256-021-03846-0
40. Mao H, Geng D, Zhu X, et al. Intervertebral disc degeneration induced by intradiscal poly(methyl methacrylate) leakage after spine augmentation in an in vivo rabbit model. Acta Biomater. 2014;10(7):3059–3067. doi:10.1016/j.actbio.2014.03.008
41. Baroud G, Nemes J, Heini P, Steffen T. Load shift of the intervertebral disc after a vertebroplasty: a finite-element study. Eur Spine J. 2003;12(4):421–426. doi:10.1007/s00586-002-0512-9
42. Dahl OE, Garvik LJ, Lyberg T. Toxic effects of methylmethacrylate monomer on leukocytes and endothelial cells in vitro. Acta Orthop Scand. 1994;65(2):147–153. doi:10.3109/17453679408995423
43. Luo J, Daines L, Charalambous A, Adams MA, Annesley-Williams DJ, Dolan P. Vertebroplasty: only Small Cement Volumes Are Required to Normalize Stress Distributions on the Vertebral Bodies. Spine. 2009;34(26):2865–2873. doi:10.1097/BRS.0b013e3181b4ea1e
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.