")
Back to Journals » Journal of Pain Research » Volume 18
Analyzing Trends in the Pain Fellowship Match – A Survey of Program Directors
Authors Jueng J , Pritzlaff SG , Mehta N , Gulati A , Schatman ME , Wahezi SE, Day M, Durbhakula S, Pak DJ
Received 13 September 2024
Accepted for publication 29 April 2025
Published 7 May 2025 Volume 2025:18 Pages 2335—2341
DOI https://doi.org/10.2147/JPR.S496104
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ryan D'Souza
Jeremy Jueng,1 Scott G Pritzlaff,2 Neel Mehta,3 Amitabh Gulati,4 Michael E Schatman,5,6 Sayed Emal Wahezi,7 Miles Day,8 Shravani Durbhakula,9 Daniel J Pak3
1Department of Physical Medicine & Rehabilitation, Miami Miller School of Medicine, Miami, FL, USA; 2Department of Anesthesiology and Pain Medicine, University of California, Davis, Sacramento, CA, USA; 3Department of Anesthesiology, Weill Cornell Medicine, New York, NY, USA; 4Department of Anesthesiology and Critical Care, Memorial Sloan Kettering Cancer Center, New York, NY, USA; 5Department of Anesthesiology, Perioperative Care, and Pain Medicine, NYU Grossman School of Medicine, New York, NY, USA; 6Department of Population Health – Division of Medical Ethics, NYU Grossman School of Medicine, New York, NY, USA; 7Department of Physical Medicine & Rehabilitation, Montefiore Medical Center, Bronx, NY, USA; 8Department of Anesthesiology and Pain Medicine, Texas Tech University Health Sciences Center, Lubbock, TX, USA; 9Department of Anesthesiology, Vanderbilt University Medical Center, Nashville, TN, USA
Correspondence: Daniel J Pak, Department of Anesthesiology, Weill Cornell Medicine, 525 East 86 th St, New York, NY, 10065, USA, Email [email protected]
Introduction: Based on recent data, the pain fellowship match is decreasing in competitiveness. The most recent 2023– 2024 match cycle had the most unfilled positions and the highest match rate in the last five years. Although there has been some speculation about potential factors contributing to these trends, our study aimed to gather insight from pain fellowship program directors (PDs) nationwide to provide valuable perspectives on recent match trends.
Methods: We created an anonymous online survey, with questions regarding potential factors contributing to match trends over the last five years. Our survey was emailed to 115 program directors (PDs), and one follow-up Email was sent three weeks later to maximize responses.
Results: Surveys were completed by 25.2% (29/115) of PDs. Over the past five years, 82.8% of PDs (24/29) reported a decrease in applications to their program. For residency specialty of pain fellowship applicants, 100% of PDs (29/29) reported a decline in anesthesiology applicants. Most PDs reported an increase in applicants from PM&R (62.1%, 18/29), Neurology (69.0%, 20/29), and Emergency Medicine (93.1%, 27/29). For potential contributors to these trends, increasing compensation in primary residency specialty was the most significant perceived contributor, with a weighted average of 4.89/5. Decreasing pain reimbursement was the second strongest contributor, with a weighted average of 4.31/5.
Conclusion: Increasing compensation in primary residency specialty and declining pain reimbursements were the two most significant perceived contributors to the recent decline in interest in pain fellowship to resident trainees. Pain medicine is now attracting a more diverse applicant pool with a decrease in anesthesiology applicants and an increase in PM&R, Internal Medicine, Neurology, Emergency Medicine, and Psychiatry applicants. Future pain fellows’ increased variety of training backgrounds may present an opportunity to critically assess the current pain medicine curriculum to suit the needs of a more diverse cohort.
Keywords: pain medicine, education, fellowship, medical training, chronic pain, multidisciplinary
Introduction
The landscape of pain fellowship recruitment has recently seen a significant shift in popularity. Since its inception in 1993, American College of Graduate Medical Education (ACGME) accredited pain medicine fellowships have rapidly expanded from 55 programs accepting anesthesiology residents only to 115 programs accepting residents of 7 different specialties now. Until the past few years, pain fellowship has traditionally been a competitive fellowship to match into with more applicants than spots offered.1 The popularity of pain fellowship may be attributable to an interest in nonopioid pharmacological and interventional therapies to combat the opioid crisis, an increase in the residency specialties eligible for pain fellowship, and/or increased compensation in comparison to primary residency specialty. However, recent National Resident Matching Program (NRMP) data suggest that the pain fellowship match is decreasing in competitiveness. From the 2018–2023 match cycles, there were an average of ~530 applicants (~421 submitting a rank list) for 366 positions offered per cycle. Despite an increase to 393 positions offered in the 2023–2024 cycle, there was a decrease to 446 applicants (359 submitting a rank list). For the 2023–2024 cycle, 30.4% (35/115) of ACGME accredited programs reported at least one unfilled position and 15.5% (61/393) of total available positions were initially unfilled compared to an average of 8.7% unfilled programs and 3.7% unfilled positions in cycles from 2018 to 2023.1 Concordant with these results, the percentage of initially matched applicants increased from 79.3% in the 2018–2019 cycle to 92.5% in the 2023–2024 cycle.1,2
The applicant pool has also shifted in the past several years. While fellowship matriculants have traditionally been primarily anesthesiology and physiatry trainees, there has been a recent increase in applicants from other specialties including emergency medicine, neurology, family medicine, and psychiatry. Between 2022 and 2023, anesthesia applicants to Pain Medicine fellowships decreased by 48.2%, contributing to over 61 unmatched positions and more than 35 unfilled programs for the 2024 matriculation year.2 Studies have speculated that this shift in the appeal of pain fellowship training may be primarily due to a strong general anesthesia job market and/or applicants’ concern regarding decreased compensation in pain medicine due to increased difficulties with insurance authorizations for interventional pain procedures and declining reimbursements.1 Another possible contributor to the decrease in popularity of pain fellowship could be the increase in North American Spine Society (NASS)-recognized Interventional Spine and Musculoskeletal Medicine (ISMM) fellowships. There are 60 spots available and per the NASS website, these fellowships focus on the clinical assessment and treatment of patients with spine and musculoskeletal conditions and are unique from ACGME Pain Medicine fellowships, which require training in inpatient acute pain management, palliative care, psychiatry, pediatric pain management, and intubation.3 These goals as stated may align more with applicants interested in practicing pain medicine, contributing to the decline in popularity of ACGME pain fellowships. To further elucidate and validate potential reasons behind these trends, we distributed an anonymous online survey to pain fellowship program directors regarding their insights on recruitment and the match.
Materials and Methods
The objective of our study was to obtain specifically program director insight into recent match trends to make recommendations about potential changes to the recruitment process and curriculum. Program directors were chosen since all are experts in pain fellowship recruitment as they are directly involved in the interview process and curriculum development. Data regarding past pain fellowship match cycles were obtained from the NRMP website. The NRMP is the official sponsor of matching cycles, so their website was chosen due to its authoritative and comprehensive dataset with no relevant data discarded. We used Google Forms to create an anonymous survey consisting of multiple-choice questions related to recent literature on match trends over the past 5 years.4–6 Authors who have published extensively on the topic of pain fellowship in light of recent match trends and regarded as experts in this domain were involved in the formulation and review of relevant questions to disseminate (authors SEW, SP, MD, AG, MS). These experts were also involved with data analysis and are authors on this manuscript. A full list of survey questions is included in the Supplementary Figure. We accessed the Association of Pain Program Directors directory and the AAMC pain fellowship program directory to identify program director Email addresses. Our survey was distributed to all 115 program directors of ACGME accredited pain fellowships. There were no sender errors when distributing the survey suggesting that all program director emails were correct. The initial Email to program directors requesting participation in the survey requested responses within 3 weeks. At the 3 week mark, a follow-up Email was sent to the same group of Email addresses to maximize response rate.
Results
We received 29 responses to our survey for a response rate of 25.2% (29/115). Over the past 5 years, 82.8% of PDs (24/29) reported a decrease in the number of applications to their program (Figure 1). For the number of interviewed applicants ranked at their program, 55.2% (16/29) of PDs reported no change, while 34.5% (10/29) reported an increase, and only 10.3% (3/29) reported a decrease (Figure 2). Similarly, 48.3% (14/29) of PDs reported minimal change in the rank of the last matched applicant to their program. In comparison, 44.8% (13/29) of PDs reported having to go down further down their rank order list for their last matched applicant. Only 6.9% (2/29) of PDs reported going further up their rank order list for their last matched applicant (Figure 3).
 |
Figure 1 Over the last 5 years, what trends have you noticed in the number of pain fellowship applications? |
 |
Figure 2 Over the last 5 years, what patterns have you noticed in the number of interviewed applicants who are ranked at your institution for the Match? |
 |
Figure 3 Over the last 5 years, which of the following is true regarding your match list? |
For residency specialty of pain fellowship applicants, 100% of PDs (29/29) reported a decrease in anesthesiology applicants (Figure 4). Most PDs reported an increase in applicants from PM&R (62.1%, 18/29), Neurology (69.0%, 20/29), and Emergency Medicine (93.1%, 27/29) (Figure 4). For matched applicants, most PDs reported a decrease in anesthesiology residents (65.5%, 19/29), while most PDs reported an increase in matched PM&R (65.5%, 19/29) and Emergency Medicine (65.5%, 19/29) residents (Figure 5).
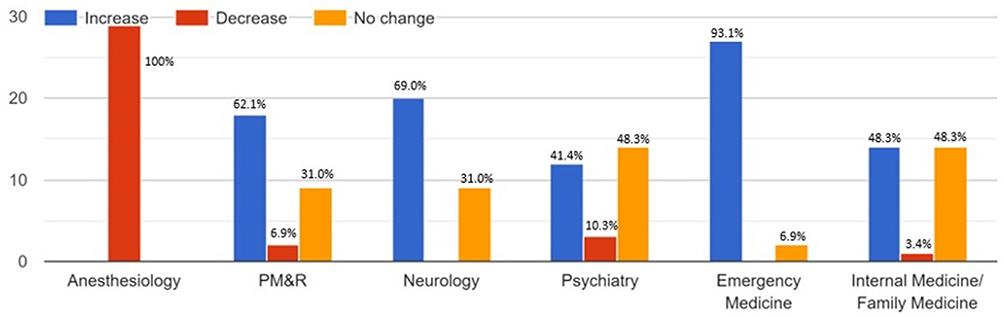 |
Figure 4 Over the last 5 years, what trend have you noticed in the number of applicants from the following residency specialties (Anesthesia, PM&R, Neurology, Psychiatry, Emergency Medicine, IM/FM)? |
 |
Figure 5 Over the last 5 years, what trend have you noticed in the number of MATCHED applicants from the following residency specialties (Anesthesiology, PM&R, Neurology, Psychiatry, Emergency Medicine, IM/FM)? |
In terms of potential contributors to these trends, increasing compensation in primary residency specialty was the most significant perceived contributor with a weighted average of 4.89/5 (5 was most significant and 1 was least significant) (Figure 6). Decreasing pain reimbursement was the second most significant contributor, with a weighted average of 4.31/5 (Figure 6). Other factors assessed were too many new fellowship programs (2.86/5), advanced practice provider encroachment (2.69/5), virtual interview format (3.34/5), and lack of interest in pain medicine (2.90/5) (Figure 6).
 |
Figure 6 Given the increase in the number of unmatched fellowship positions from 2018, please rank the following factors as potential contributors to this trend on a scale of 1 to 5 (5 is most significant, 1 is least significant). |
Discussion
Since receiving accreditation by the Accreditation Council of Graduate Medical Education (ACGME) in 1993, the number of Pain Medicine fellowships has expanded from 55 to 115 programs.7,8 With an increase in demand for fellowship-trained pain medicine physicians over the past 30 years, Pain Medicine fellowship has traditionally been recognized as a competitive subspecialty. However, recent match data and this survey suggest a recent decline in the appeal and competitiveness of the specialty. This survey-based study provides valuable insight from PDs regarding recent pain fellowship match trends and potential contributing factors.
Over the past 5 years, most PDs (82.8%) reported a decrease in the number of applicants to their program which was concordant with recent NRMP data.2 Additionally, 34.5% of PDs reported the need to rank more applicants, whereas 10.5% indicated a decrease in the number of ranked applicants. Similarly, 44.8% of PDs reported having to go down further down their rank order list for their last matched applicant, while only 6.9% of PDs reported going further up their rank order list for their last matched applicant. These data suggest that PDs have recently needed to interview more applicants in order to fill their matched pain fellow classes, suggesting a greater struggle to find suitable candidates for their programs.
Overall, PDs felt that factors related to income, with both increasing compensation in general anesthesia and decreasing pain reimbursement, represent the most significant contributors to the recent decrease in appeal of pain medicine fellowship to anesthesia residents. Based on MGMA data, median salary for pain medicine was $494,488 in 2021 and $518,715 in 2024, representing an increase of $24,227 (4.9%). On the other hand, median anesthesia salary was $462,917 in 2021 and $515,767 in 2024, representing an increase of $52,850 (11.9%). Median PM&R salary was $313,183 in 2021 and $333,808 in 2024 representing an increase of $20,625 (6.7%). Other specialties applying to pain fellowship had an increase in salary from 2021 to 2024 of Emergency Medicine (3.2%), Internal Medicine (10.5%), Psychiatry (16.2%), and Neurology (10.4%).9 These data demonstrate that the absolute median salary for general anesthesia has increased over the years to essentially match the absolute median salary of pain medicine in 2024. Additional data for the strong general anesthesia market include an increase in unfilled anesthesia fellowship positions. From 2018 to 2022 cardiothoracic anesthesia fellowship had ~359 applicants per cycle compared to 313 in the 2023 cycle.10 From 2018 to 2023, critical care anesthesia had ~212 applicants per cycle compared to 189 in the 2024 cycle.11 Thus, the additional year of pain medicine fellowship for a similar salary as general anesthesia may make pain medicine less attractive to anesthesiology residents. The median salary for pain medicine remains higher than the median salary for other specialties such as PM&R, Emergency Medicine, Internal Medicine, Psychiatry, and Neurology which may explain the increase in applicants from these fields. Non-anesthesiology applicants may also recognize decreased anesthesiology applications as an opportunity for matriculation in pain medicine that did not exist when anesthesia was more robustly represented in the applicant pool. Of note, lack of interest in pain medicine was only the 4th most significant contributor out of 6, suggesting persistent interest in the field.
The primary specialty of Pain is becoming more diverse, as 100% of PDs reported a decrease in anesthesiology applicants and a majority reported an increase in PM&R (62.1%), Neurology (69.0%), and Emergency Medicine (93.1%) applicants. These trends coincide with AAMC data: 351 applicants from Anesthesiology in 2019–2020 compared to 193 in 2023–2024 representing a decrease of 45.0%. There were 101 applicants from PM&R in 2019–2020 compared to 134 in 2023–2024, representing an increase of 32.7%. In 2019–2020, there were only 10 applicants from Emergency Medicine compared to 29 in 2023–2024,1 representing an increase of 190%. Most PDs also reported a decrease in matched anesthesiology residents (65.5%) while also indicating an increase in matched PM&R (65.5%) and Emergency Medicine residents (65.5%). The authors surmise that potential factors contributing to the increase of matched PM&R and Emergency Medicine residents include the increase in compensation for pain medicine compared to primary residency specialty and desire to practice a more procedural-based and/or outpatient-based specialty.12 Based on our data, PDs did not consider factors such as too many new ACGME pain fellowships, advanced practice provider encroachment, and lack of interest in pain medicine as representing significant contributors which decreased anesthesiology application. Overall, these data suggest strong interest in pain medicine from non-anesthesiology specialties and that pain medicine is likely to become more heterogeneous should these trends continue. Growth in non-accredited spine/sports, radiology, and NASS fellowships provide other pathways to pain treatments without an ACGME pain medicine fellowship, further adding to an increasingly diverse group of pain medicine practitioners.
Given the shifting background training of pain fellows, it may be worthwhile to reassess the current curricula of pain medicine fellowships. Contemporary literature describes that many pain fellowship programs perceive weakness in psychological, radiological, and procedural education with required supplemental education from pain societies and industry, much of which is not overseen or standardized by the ACGME, potentially creating disparities in training and bias.5,6,13 A more heterogeneous pain fellow pool may complicate these concerns as individual programs may struggle to understand and address perceived weaknesses to fit the needs of a more diverse class of trainees.5 Furthermore, supplemental education from pain societies and industry are valuable tools which Pain fellowships rely on to supplement education; however, these programs will likely need revision to accommodate the learning styles of the non-anesthesiologists for which they were not designed. The authors submit that all of these challenges result in discrepancies of fellow education due to the lack of standardization and limited oversight from the ACGME.14–16 We hope that the ACGME sees the current state of Pain medicine fellowship challenges as an opportunity to intervene and improve the state of Pain education. With the recent increase in diversity of training backgrounds of pain fellows, we propose a need for more standardization in training and possible overhaul of the curriculum, which has been proposed by several authors.4,6,17
Limitations/Future Directions
This is a descriptive study with an objective of identifying potential factors contributing to recent match trends and providing recommendations for future pain fellowship recruitment practices and curriculum development. This is not a study that aims to establish causality about specific factors contributing to recent match trends, although additional studies could be conducted to better deduce causality for these match trends. Survey research, generally, is subject to response and sampling biases. The responses to our survey represent the opinions of only 29/115 (25.2%) of pain fellowship program directors, and the possibility that our results captured a sample of only PDs who were most motivated to elicit changes in pain medicine education cannot be ruled out. Future studies could attempt to elicit higher percentages of responses, perhaps by extending the study period and encouraging those slow to respond. Exploring the perspectives of trainees could also provide meaningful insight to validate our findings. Additionally, because our survey was anonymous and requested no identifying information, we were unable to determine the proportion of responses that came from academic versus community-based program directors. Further work could analyze whether the large shift in pain fellowship appeal also corresponded with the types of programs to which residents applied. Finally, NRMP data indicate that the 2023–2024 match cycle was the first cycle with a large decrease in number of applicants. Future studies could assess match data for longer periods of time to determine whether the 2023–2024 cycle was an anomaly or the continuation of a trend. Future match data could also be analyzed when compensation changes for each specialty to determine whether this remains the most significant contributor.
Conclusion
Although historically considered a competitive fellowship into which to match, pain fellowship has recently decreased in appeal as demonstrated by a large decrease in applicants and an increase in unfilled positions. Based on our results, PDs felt that compensation in general anesthesia residency and declining pain procedure reimbursements were the two most significant perceived contributors to the recent decline in anesthesiology resident appeal for pain medicine fellowship. Though pain fellowship interest remains high amongst non-anesthesiology pain fellowship eligible trainees, it is not enough to adequately fill the current spots available given a rising increased unmatched rate in several consecutive years. Earlier education and recruitment for pain medicine in medical school or residency could increase exposure and cultivate applicants for the future match cycles. Finally, given the continued need for chronic pain practitioners across the country and the imminently increasing heterogeneity of specialists in our field, it is time to revise the pain fellowship curriculum to adapt accordingly.
Ethics
This study was reviewed by the University of Miami Human Research Subject Office Institutional Review Board and determined to meet criteria for an exemption. Informed consent was obtained from the study participants at the beginning of the survey. Subject were informed that the survey was completely anonymous, results would not be linked to participants, and participation was voluntary. They were informed that results would only be used for future presentations and/or publications. Guidelines in the Declaration of Helsinki were followed when conducting this study.
Disclosure
Dr Scott G Pritzlaff reports personal fees from SPR Therapeutics and Nalu Medical; royalties from Wolter Kluwer; grants from Medtronic, Abbott, Biotronik, and Nevro, outside the submitted work. Dr Amitabh Gulati is a consultant for Medtronic, AIS healthcare, SPR therapeutics, Hinge health, Nalu Medical, Neurovasis, Smart ms3, Tersera Medical, and Edenos, outside the submitted work. Dr Michael E Schatman is a senior medical advisor for Apurano Pharma, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Christiansen S, Pritzlaff S, Escobar A, Kohan L. A sudden shift for pain medicine fellowships – a recount of the 2024 match. Interv Pain Med. 2024;3(2):100404. doi:10.1016/j.inpm.2024.100404
2. National Resident Matching Program. NRMP results and data specialties matching service, 2024 appointment year. 2024. Available from: https://www.nrmp.org/wp-content/uploads/2024/02/2024-SMS-Results-Data-1.pdf.
3. NASS. Match opportunities. 2024. Available from: https://www.spine.org/Portals/0/Assets/Downloads/Education/Match-Opportunities.pdf.
4. Wahezi SE, Hunter CW, Ahadian FM, Argoff CE, Schatman ME. Predicting the collapse of pain medicine using the economic recession of 2008 as a comparator: lessons remain unlearned. J Pain Res. 2024;17:2341–2344. doi:10.2147/jpr.S471143
5. Wahezi SE, Emerick TD, Caparó M, et al. The current state of training in pain medicine fellowships: an association of pain program directors (appd) survey of program directors. Pain Pract. 2024. doi:10.1111/papr.13373
6. Wahezi SE, Caparo M, Naeimi T, Kohan L. Fellowship education in a new era of pain medicine: concerns and commentary for change. Pain Med. 2024;25(1):3–4. doi:10.1093/pm/pnad116
7. AAMC. Pain medicine (multidisciplinary). 2024.
8. ACGME. ACGME program requirements for graduate medical education in pain medicine ACGME. 2022.
9. MGMA. 2024 provider compensation data report. 2024. Available from: https://www.mgma.com/data-report-provider-comp-2024.
10. SF Match. Adult cardiothoracic anesthesiology fellowship match. 2024. Available from: https://sfmatch.org/specialty/adult-cardiothoracic-anesthesiology-fellowship/Statistics.
11. SF Match. Critical care anesthesiology fellowship match. 2024. Available from: https://sfmatch.org/specialty/critical-care-anesthesiology-fellowship/Statistics.
12. Wahezi SE, Naeimi T, Caparo M, et al. Trainee insight into pain fellowship programs: a critical evaluation of the current educational system by the appd. Pain Physician. 2024;27(5):E627–e636.
13. Pritzlaff SG, Goree JH, Hagedorn JM, et al. Pain education and knowledge (peak) consensus guidelines for neuromodulation: a proposal for standardization in fellowship and training programs. J Pain Res. 2023;16:3101–3117. doi:10.2147/jpr.S424589
14. Abd-Elsayed A, Abdallah R, Falowski S, et al. Development of an educational curriculum for spinal cord stimulation. Neuromodulation. 2020;23(5):555–561. doi:10.1111/ner.13142
15. Pak DJ, Gruber J, Deer T, et al. Spinal cord stimulator education during pain fellowship: unmet training needs and factors that impact future practice. Reg Anesth Pain Med. 2019;44(3):407–414. doi:10.1136/rapm-2018-100065
16. Durbhakula S, Toy S, Acosta CA, et al. Needs-based novel digital curriculum for the neuromodulation training deficit: pain rounds. Reg Anesth Pain Med. 2023;48(8):414–419. doi:10.1136/rapm-2023-104480
17. Wahezi SE, Caparo M, Naeimi T, Kohan L. The importance of interventional pain research in academic settings: a call for change to fortify our future. A message from the association of pain program directors (appd). Pain Med. 2023;24(12):1293–1295. doi:10.1093/pm/pnad099
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Multimodal and Interdisciplinary Interventions for the Treatment of Localized Provoked Vulvodynia: A Scoping Review of the Literature from 2010 to 2023
Rains A, Bajzak K, Miller ME, Swab M, Logan GS, Jackman VA, Gustafson DL
International Journal of Women's Health 2024, 16:55-94
Published Date: 15 January 2024
Artificial Intelligence and Pain Medicine: An Introduction
Hagedorn JM, George TK, Aiyer R, Schmidt K, Halamka J, D'Souza RS
Journal of Pain Research 2024, 17:509-518
Published Date: 2 February 2024
An Integrative Review of Opioid Stewardship: Optimizing Patient Care and Safety with a Multidisciplinary Approach
Adams N, Ott CA, Mullen CJ, Wang Y
Nursing: Research and Reviews 2024, 14:173-200
Published Date: 29 August 2024