")
Back to Journals » Journal of Inflammation Research » Volume 18
Aneurysm Wall Enhancement and Systemic Inflammation Jointly Contribute to Cognitive Dysfunction in Untreated Unruptured Intracranial Aneurysm Patients
Authors Wu XB, Luo B, Guo X, Liu CC, Liu YA, Ye JS, Fan SY, Li QJ, Wang SW
Received 1 February 2025
Accepted for publication 1 July 2025
Published 10 July 2025 Volume 2025:18 Pages 9045—9053
DOI https://doi.org/10.2147/JIR.S515856
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Adam Bachstetter
Xiao-Bing Wu,1,* Bin Luo,2,* Xin Guo,2,* Chi-Chen Liu,2 Yi-Ao Liu,2 Jie-Shun Ye,3 Shao-Yi Fan,4 Qing-Jian Li,5 Sheng-Wen Wang1
1Department of Neurosurgery, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China; 2Department of Neurosurgery, The Eighth Affiliated Hospital, Sun Yat-sen University, Shenzhen, People’s Republic of China; 3School of Civil Engineering and Transportation, South China University of Technology, Guangzhou, People’s Republic of China; 4Department of TCM, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, People’s Republic of China; 5Department of Oncology, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Sheng-Wen Wang, Department of Neurosurgery, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, No. 107, Yanjiang West Road, Guangzhou, Guangdong, 510120, People’s Republic of China, Email [email protected] Qing-Jian Li; Department of Oncology, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, No. 107, Yanjiang West Road, Guangzhou, Guangdong, 510120, People’s Republic of China, Email [email protected]
Background and Purpose: Peripheral inflammatory markers and aneurysm wall enhancement (AWE) on high-resolution vessel wall MRI (HR-VWI) may reflect inflammation in unruptured intracranial aneurysms (UIAs). We assessed cognitive function and its association with inflammatory markers in UIA patients.
Methods: The study included 120 consecutive patients with UIAs diagnosed between September 2018 and December 2023 and a control group of 27 healthy adults at our institution. Neuropsychological function in these patients was evaluated using the Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), Hamilton Anxiety Scale (HAMA), and Self-Rating Depression Scale (SDS). A MoCA score of < 23 was classified as cognitive decline, while scores of ≥ 23 indicated normal cognitive function. The peripheral blood inflammatory markers and radiological characteristics were compared between the patients with cognitive decline and those with normal cognitive function. The presence of AWE and white matter hyperintensities (WMH) in UIA was identified through HR-VWI.
Results: UIA patients demonstrated significantly poorer cognitive performance than controls, with lower MMSE (27.0 vs 29.0, P < 0.001) and MoCA scores (23.0 vs 25.0, P = 0.020). Patients with cognitive decline were older and exhibited elevated inflammatory markers (NLR, SII, hsCRP; all P < 0.05), along with higher rates of AWE and white matter hyperintensities (WMH) (both P < 0.001). Multivariate analysis identified AWE (OR = 5.33, 95% CI:1.82– 15.59), WMH (OR = 4.26, 95% CI:1.58– 11.49), and age (OR = 1.07, 95% CI:1.02– 1.12) as independent predictors of cognitive decline (all P ≤ 0.01). Moreover, the cognitive decline group also showed higher SDS and HAMA scores (P < 0.05), suggesting a correlation between emotional distress and cognitive impairment.
Conclusion: Untreated UIA patients exhibit cognitive decline associated with systemic inflammation (NLR, SII, hs-CRP). AWE, WMH and age are independent risk factors, suggesting vascular inflammation contributes to cognitive dysfunction.
Keywords: unruptured intracranial aneurysm, cognitive function, aneurysm wall enhancement, inflammation
Introduction
Unruptured intracranial aneurysms (UIAs), particularly the saccular type, are common brain vascular abnormalities found in about 3.2% of adults worldwide.1 While most UIAs cause no symptoms, their potential rupture can lead to subarachnoid hemorrhage (SAH) - a life-threatening condition often resulting in cognitive problems.2 Although cognitive issues after SAH are well-known, the possible cognitive effects of unruptured aneurysms have received little attention. One study using a composite inflammatory score-including white blood cell (WBC) counts-found that a higher score at midlife was associated with greater cognitive decline.3 This suggests that systemic inflammation may play a role in cognitive health. The neutrophil-to-lymphocyte ratio (NLR), a novel inflammatory indicator, has gained attention for its association with cognitive impairment. Elevated NLR has been reported in older adults with cognitive impairment4 and has been shown to predict an increased risk for dementia.5,6 Longitudinal studies with long-term follow-up have observed that inflammatory markers in peripheral blood correlate with cognitive decline and a 10-year cumulative incidence of cognitive impairment.7,8 These studies have revealed that circulating inflammatory markers are associated with cognitive impairment.
Inflammation plays a critical role in the formation, progression, and eventual rupture of UIAs.9,10 High-resolution vessel wall imaging (HR-VWI) has become a critical noninvasive imaging technique for assessing aneurysm wall stability in patients with UIA. Aneurysm wall enhancement observed on HR-VWI suggests active wall inflammation and aneurysm instability, marking it as a critical indicator of aneurysms at a higher risk of rupture.11–14 Our prior work found that UIAs with visible wall enhancement had higher NLR levels,15 but we do not yet know if these inflammatory changes relate to cognitive problems in UIA patients. This missing link could be clinically important. If cognitive issues in UIA patients connect to aneurysm instability and body-wide inflammation, it might change how we manage these patients. This study explored deficits in neuropsychological functioning, and their correlating factors in UIA patients, as well as the association between peripheral blood inflammatory indicators and cognitive impairment in these patients.
Materials and Methods
Patient Selection
We conducted a prospective study of otherwise healthy adults with untreated unruptured intracranial aneurysms (UIAs) at our institution between September 2018 and December 2023. Inclusion criteria were: (1) Age >18 years, (2) Minimum 9 years of compulsory education, (3) Diagnosis of saccular UIA confirmed by digital subtraction angiography or MRA, (4) Brain MRI confirming no intracranial hemorrhage. We excluded patients with a history of pneumonia, heart disease, autoimmune disease, hematological diseases, cancer, and chronic liver or kidney insufficiency. Patients with extracranial aneurysms or aneurysms in the cavernous sinus of the internal carotid artery were also excluded. Additionally, healthy adults (confirmed by MRA to have no IAs) were recruited as negative controls. This study was approved by the local institutional review board at our institution.
Laboratory Measurements
Laboratory parameters, including low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, high-sensitivity C-reactive protein, and white blood cell differential counts in peripheral blood, were conducted within 24 h after admission. The NLR, lymphocyte-to-monocyte ratio (LMR), and systemic immune-inflammation index (SII) were calculated as follows: NLR = neutrophil count/lymphocyte count, LMR = lymphocyte count/monocyte count, and SII = platelet count × neutrophil count/lymphocyte count.
Neuropsychological Examinations
In this study, neuropsychological function in UIA patients was evaluated using four key standardized tests before any surgical intervention: Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), Hamilton Anxiety Scale (HAMA), and Self-Rating Depression Scale (SDS). These tests were administered individually by two trained assessors before surgery. Each patient underwent these neuropsychological examinations. Each test assessed different dimensions of cognitive and emotional well-being. An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Objective cognitive performance was measured using MoCA and MMSE. MMSE is a 30-point performance-based screening tool widely used to detect cognitive changes. The MMSE evaluates cognitive domains such as attention, orientation, language, verbal memory, visuospatial, and executive function. MoCA is a screening tool designed to assess the same cognitive domains as the MMSE but with a stronger focus on detecting mild cognitive impairment (MCI). The Chinese translations of both the MoCA and MMSE have been previously validated for the population studied.16,17 A MoCA score of <23 maximized the sum of sensitivity and specificity for detecting MCI.18 In this study, MoCA < 23 was used to identify cognitive decline (cognitive decline group), whereas MoCA ≥ 23 indicated normal cognitive function (cognitive normal group). MoCA cutoff values of 23 were selected with reference to a Chinese population validation study, and sensitivity analyses were performed with internal data. Moreover, patients’ anxiety and depression were assessed using the Chinese version of the HAMA (a 14-item scale) and SDS (a 20-item scale).19
HR-VWI Examination
For each UIA patient, a gadolinium-enhanced brain HR-VWI scan was performed using a 3.0T MRI scanner at baseline. The post-contrast 2D/3D T1-weighted images were obtained 5 min after the administration of 0.1 mmol/kg gadopentetate glucosamine (Gd-DTPA, Hokuriku Pharmaceutical, China) injection. Detailed scanning parameters for these images are provided in Supplementary Material. The pattern of AWE was categorized into two groups based on the comparison of pre-contrast and post-contrast HR-VWI T1-weighted sequences: none AWE and AWE.20 Two readers who were blinded to the clinical data independently reviewed the HR-VWI T1-weighted images to identify the presence and pattern of AWE in saccular unruptured IAs. A third reader resolved disagreements. Cohen κ statistics were used to assess the interreader agreement. κ values >0.80 were regarded as excellent for the identification of AWE.15 White matter hyperintensities (WMH) of presumed vascular origin appear hyperintense on T2-weighted MRI sequences and isointense to mildly hypointense (but never as hypointense as CSF) on T1-weighted sequences.21
Statistical Analysis
Clinical and radiological characteristics, laboratory examinations, neuropsychological test results, and pattern medical history were thoroughly documented.
First, we compared clinical, radiological, and laboratory data, along with neuropsychological examination results, between UIA patients and healthy controls. Then, the data were further analyzed by comparing UIA patients within two subgroups: those experiencing cognitive (MoCA < 23) and those with normal cognitive function (MoCA ≥ 23). Multivariate logistic regression with a backward elimination method was used to identify independent risk factors for cognitive decline in UIA patients. Variables with P < 0.05 in the univariate analysis were included in the regression model to adjust for potential confounding factors. Correlation analysis was conducted to examine the associations between anxiety (HAMA), depression (SDS), and cognitive function (MoCA) in UIA patients. We also assessed the associations between laboratory findings (such as NLR, LMR, and SII), neuropsychological results, and different patterns of AWE in UIA patients. Statistical analysis was performed using SPSS 22.0 software. Continuous variables were analyzed using Student’s t-test or Mann–Whitney U-test, depending on data distribution. Categorical variables were evaluated using Fisher’s exact test or chi-square test. Two-tailed P values of <0.05 were considered statistically significant.
Results
Clinical Characteristics
During the 4-year study period, 179 consecutive patients with 198 IAs were identified. Among them, 120 UIA patients met the inclusion criteria and were included in the study after applying the exclusion criteria. Additionally, 27 healthy adults were recruited as controls. The mean age of the UIA patients was 58.6 ± 11.5 years, with 50 (41.7%) being men. Table 1 presents the clinical characteristics of both the UIA patients and healthy adults. Thirty-six (30%) UIAs showed AWE, and The interreader agreement for the identification of AWE was excellent, with κ = 0.92. Statistical analyses revealed no significant differences in clinical data between the UIA patients and healthy controls.
 |
Table 1 Characteristics of Patients with UIA and Healthy Adults |
UIA Patients Have Decreased Cognitive Function and Abnormal Expression of Inflammatory Markers
The MMSE and MoCA scores were significantly lower in the UIA than in the healthy adults (MMSE, 27.0 vs 29.0, P < 0.001; MoCA, 23.0 vs 25.0, P = 0.020). The NEUT, NLR, and SII were significantly higher in the patients (P < 0.001) than in the healthy adults, whereas the LYM and LMR were significantly lower (P < 0.001) (Table 1).
AWE, WMH and Older Age as Independent Predictors of Cognitive Decline
Patients with cognitive decline were older and exhibited elevated inflammatory markers (NLR, SII, hsCRP; all P < 0.05), along with higher rates of AWE and white matter hyperintensities (WMH) (both P < 0.001) (Table 2). The SDS scores were also higher in the cognitive decline group than in the cognitively normal group. Backward multiple logistic regression analysis revealed that AWE (OR:5.33, 95% CI:1.82–15.59, P = 0.002), WMH (OR:4.26, 95% CI:1.58–11.49, P = 0.004), and older age (OR:1.07, 95% CI:1.02–1.12, P = 0.010) were independently associated with cognitive decline (Table 3).
 |
Table 2 Factors Associated with Cognitive Decline in Patients with UIA |
 |
Table 3 Multiple Logistic Regression Analysis for Cognitive Decline in Patients with Unruptured Intracranial Aneurysm |
Negative Linear Correlation Between MoCA and HAMA and SDS
The median SDS scores were significantly higher in the cognitive decline group than in the cognitively normal group (34.0 vs 31.0, P = 0.014). Additionally, the median HAMA scores in the cognitive decline group was higher than in the cognitively normal group (8.0 vs 7.0), but the difference did not reach statistical significance (P = 0.059) (Table 2).
Further analysis using linear regression models demonstrated that both HAMA and SDS scores were negatively correlated with the MoCA scores (R = 0.279, P = 0.002; R = 0.356, P < 0.001, respectively) (Figure 1).
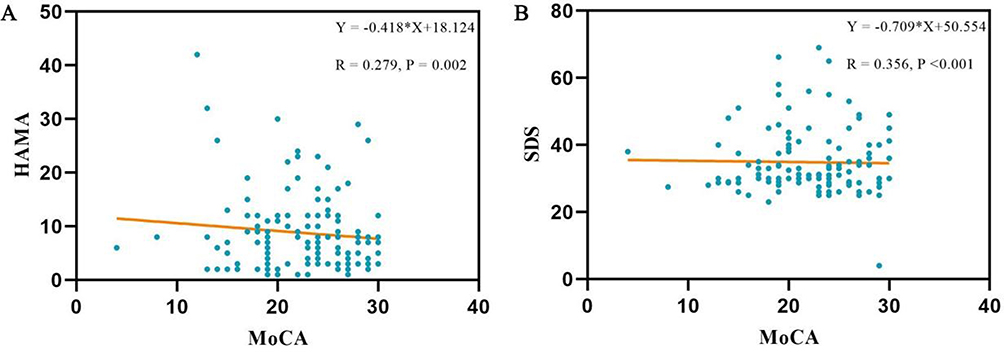 |
Figure 1 Correlation analysis was conducted to examine the associations between MoCA and (A) anxiety (HAMA), (B) depression (SDS) in UIA patients. |
Laboratory Examination and Neuropsychological Examinations in UIA Patients with AWE
NLR and SII expression significantly decreased across the three groups: UIA patients with AWE had the highest levels, followed by UIA patients without AWE and healthy controls (NLR, 2.31 vs 1.82 vs 0.81, P < 0.001; SII, 559.96 vs 429.40 vs 185.7, P < 0.001) (Figure 2). Additionally, LMR, inversely related to NLR and SII, significantly increased across the groups: UIA patients with AWE had the lowest LMR, followed by UIA patients without AWE, and the healthy controls exhibited the highest LMR (3.47 vs 4.35 vs 5.69, P < 0.001) (Figure 2).
 |
Figure 2 Comparison of circulating inflammatory indicators (NLR, SII and LMR) and neuropsychological function (MMSE, MoCA, HAMA and SDS) in UIA patients with enhancement, without enhancement, and healthy control. (A) NLR. (B) SII. (C) LMR. (D) MMSE. (E) MoCA. (F) HAMA. (G) SDS. ****P < 0.0001, ***P < 0.001,*P < 0.05. |
The MoCA scores were significantly lower in the UIA patients with AWE than in the UIA patients without AWE (19 vs 24, P < 0.001). The MMSE scores were the highest in the UIA patients with AWE, followed by UIA patients without AWE and healthy controls (24 vs 27 vs 29, P < 0.001) (Figure 2).
Discussion
Our study demonstrates three principal findings in untreated saccular UIA patients: (1) Significant cognitive impairment correlated with both local (AWE) and systemic (NLR/SII/hsCRP) inflammatory markers; (2) AWE, WMH and age emerged as independent risk factors for cognitive decline; (3) Emotional distress (depression/anxiety) showed strong association with cognitive dysfunction, potentially mediated by shared inflammatory pathways.
Less attention has been paid to the cognitive function state in UIA patients. This study revealed that cognitive function declined in the UIA patients compared with healthy adults, which was consistent with the results of previous studies.22,23 In addition, this study showed that the level of peripheral blood inflammatory markers (NLR/SII/hsCRP) was significantly higher in the UIA patients than in the healthy adults. Previous studies have also reported that the level of circulating inflammatory markers correlated with cognitive decline,7,8 elevated NLR status was associated with increased risk of cognitive impairment in Chinese community-dwelling older adults.24 Moreover, the increased levels of NLR were strongly associated with the post-stroke cognitive impairment.25 Popularity of NLR/SII as a routine blood test, was suitable for promotion in primary hospitals, while HR-VWI is costly and in most cases can only be done in large hospitals. According to studies, AWE was not only a manifestation of local inflammation of UIA26–28 but also was strongly correlated with blood inflammatory chemokines in the aneurysm sac.29 By contrast, it was reported that serum IL-1β and IL-1.ra levels was correlated with AWE.30 Moreover, in our previous study, NLR was higher in UIA patients with AWE than in those without.15 The elevated levels of circulating inflammatory markers may have caused cognitive decline in the UIA patients. In addition, AWE, reflecting local and systemic inflammatory states, was found to be an independent predictor of cognitive decline in UIA patients. Thus, inflammation plays a crucial role in cognitive decline in UIA patients.
UIAs are known to be a significant cause of anxiety and depression. Chinese patients with untreated UIA tend to develop depression and anxiety and have reduced quality of life in the short term after diagnosis.16,31 Furthermore, in the early stages of Alzheimer’s disease, anxiety and depression often occur at the same time following cognitive impairment due to coping difficulties.32 In this study, SDS and HAMA scores of the UIA patients were higher in the cognitive decline group than in the cognitively normal group. In addition, a linear negative correlation was observed between SDS, HAMA, and MoCA scores. A possible common factor in this phenomenon is inflammation, as inflammatory processes have been implicated in the pathophysiology of depression.33
Advanced age and WMH emerged as an independent risk factor for cognitive decline in our study. While cognitive deterioration and WMH naturally occurs with aging,21,34 our findings suggest this process may be accelerated in UIA patients through blood-brain barrier (BBB) dysfunction and cerebral white matter integrity decreasing. Specifically, age-related BBB permeability changes appear critical, mediated by an imbalance between elevated pro-inflammatory factors and reduced anti-inflammatory mediators.
The significant association between cognitive decline and both aneurysm wall enhancement (AWE) and systemic inflammatory markers in UIA patients may have important therapeutic implications. While current management primarily relies on endovascular interventions - chosen based on availability, patient factors, and surgeon expertise35 - our findings highlight the need to investigate how different treatment approaches might influence postoperative cognitive outcomes.
This study has several limitations. First, data for this retrospective study were collected from a single center with a relatively small sample size. This might have led to selection bias. Although the control group size was limited, post-hoc analysis confirmed our key findings remained significant (P < 0.01) when comparing UIA subgroups (AWE+/AWE-) to controls. Second, not all inflammatory indicators were associated with cognitive decline, possibly because of variations in the sensitivities of each index and the relatively small sample size. Third, all study participants were Chinese, and differences across races may influence cognitive function outcomes. Finally, HAMA and SDS are self-assessed screening tools, which may have led to somewhat subjective results.
Conclusions
In this study, patients with untreated UIAs had poorer cognitive function, which was correlated with their levels of peripheral blood inflammatory markers (ie, NLR, SII, and hs-CRP). AWE, WMH and older age were independent risk factors for cognitive decline in these patients. Inflammation played a vital role in cognitive decline in these patients with untreated UIA. However, the underlying mechanism needs further investigation.
Data Sharing Statement
The data supporting the funding of this study are available from the corresponding author upon request.
Ethics Declaration
The studies involving human participants were reviewed and approved by Sun Yat-sen Memorial Hospital. The patients/participants provided their written informed consent to participate in this study. This study adhered to the principles outlined in the revised Declaration of Helsinki from 2013.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China project (81901339), the National Natural Science Foundation of China project (82203086), the Guangdong Basic and Applied Basic Research Foundation, project (2023A1515010916) and the Shenzhen Futian District Public Health Research Project (FTWS2021015).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Thompson BG, Brown RD, Amin-Hanjani S, et al. Guidelines for the management of patients with unruptured intracranial aneurysms: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2015;46(8):2368–2400. doi:10.1161/STR.0000000000000070
2. Reijmer YD, van den Heerik MS, Heinen R, et al. Microstructural white matter abnormalities and cognitive impairment after aneurysmal subarachnoid hemorrhage. Stroke. 2018;49(9):2040–2045. doi:10.1161/STROKEAHA.118.021622
3. Walker KA, Gottesman RF, Wu A, et al. Systemic inflammation during midlife and cognitive change over 20 years: the ARIC Study. Neurology. 2019;92(11):e1256–e1267. doi:10.1212/WNL.0000000000007094
4. Liu JH, Zhang YJ, Ma QH, Sun HP, Xu Y, Pan CW. Elevated blood neutrophil to lymphocyte ratio in older adults with cognitive impairment. Arch Gerontol Geriatr. 2020;88:104041. doi:10.1016/j.archger.2020.104041
5. Ramos-Cejudo J, Johnson AD, Beiser A, et al. The neutrophil to lymphocyte ratio is associated with the risk of subsequent dementia in the Framingham heart study. Front Aging Neurosci. 2021;13:773984.
6. van der Willik KD, Fani L, Rizopoulos D, et al. Balance between innate versus adaptive immune system and the risk of dementia: a population-based cohort study. J Neuroinflammation. 2019;16(1):68. doi:10.1186/s12974-019-1454-z
7. Schubert CR, Fischer ME, Pinto AA, et al. Inflammation, metabolic dysregulation and environmental neurotoxins and risk of cognitive decline and impairment in midlife. Neurol Sci. 2023;44(1):149–157. doi:10.1007/s10072-022-06386-0
8. Xu Y, Yang Y, Chen X, et al. NLRP3 inflammasome in cognitive impairment and pharmacological properties of its inhibitors. Transl Neurodegener. 2023;12(1):49. doi:10.1186/s40035-023-00381-x
9. Turjman AS, Turjman F, Edelman ER. Role of fluid dynamics and inflammation in intracranial aneurysm formation. Circulation. 2014;129:373–382. doi:10.1161/CIRCULATIONAHA.113.001444
10. Liu Q, Zhang Y, Yang J, et al. The relationship of morphological-hemodynamic characteristics, inflammation, and remodeling of aneurysm wall in unruptured intracranial aneurysms. Transl Stroke Res. 2022;13:88–99. doi:10.1007/s12975-021-00917-1
11. Hashimoto Y, Matsushige T, Kawano R, et al. Segmentation of aneurysm wall enhancement in evolving unruptured intracranial aneurysms. J Neurosurg. 2021;136(2):449–455. doi:10.3171/2021.2.JNS2114
12. Wu XB, Wu YT, Guo XX, et al. Circular RNA hsa_circ_0007990 as a blood biomarker for unruptured intracranial aneurysm with aneurysm wall enhancement. Front Immunol. 2022;13:1061592. doi:10.3389/fimmu.2022.1061592
13. Yang CY, Wen L, Cui C, et al. A prospective follow-up study on risk factors to predict the progression of unruptured intracranial aneurysms on enhanced HR-MRI. Acad Radiol. 2023;30(7):1247–1256. doi:10.1016/j.acra.2022.10.014
14. Bae H, Suh SI, Yoon WK, Roh H, Kim C, Kwon TH. Correlation of aneurysmal wall enhancement of unruptured intracranial aneurysms on high-resolution vessel-wall imaging with clinical indices and surgical findings. Neurosurgery. 2021;89(3):420–427. doi:10.1093/neuros/nyab178
15. Wu XB, Zhong JL, Wang SW, et al. Neutrophil-to-lymphocyte ratio is associated with circumferential wall enhancement of unruptured intracranial aneurysm. Front Neurol. 2022;13:879882. doi:10.3389/fneur.2022.879882
16. Roalf DR, Moore TM, Mechanic-Hamilton D, et al. Bridging cognitive screening tests in neurologic disorders: a crosswalk between the Short Montreal Cognitive Assessment and Mini-mental State Examination. Alzheimers Dement. 2017;13(8):947–952. doi:10.1016/j.jalz.2017.01.015
17. Li C, Hong Y, Yang X, et al. The use of subjective cognitive complaints for detecting mild cognitive impairment in older adults across cultural and linguistic groups: a comparison of the cognitive function instrument to the Montreal Cognitive Assessment. Alzheimers Dement. 2023;19(5):1764–1774. doi:10.1002/alz.12804
18. Islam N, Hashem R, Gad M, et al. Accuracy of the Montreal Cognitive Assessment tool for detecting mild cognitive impairment: a systematic review and meta-analysis. Alzheimers Dement. 2023;19(7):3235–3243. doi:10.1002/alz.13040
19. Liu J, Duan W, Xiao Z, Wu Y. The effectiveness of online group mindfulness-based cognitive therapy for outpatients with depression in China. J Affect Disord. 2024;351:387–391. doi:10.1016/j.jad.2024.01.223
20. van der Kamp LT, Edjlali M, Naggara O, et al. Gadolinium-enhanced intracranial aneurysm wall imaging and risk of aneurysm growth and rupture: a multicenter longitudinal cohort study. Eur Radiol. 2024;34(7):4610–4618. doi:10.1007/s00330-023-10388-7
21. Wardlaw JM, Smith EE, Biessels GJ, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013;12(8):822–838. doi:10.1016/S1474-4422(13)70124-8
22. Su SH, Xu W, Hai J, et al. Cognitive function, depression, anxiety and quality of life in Chinese patients with untreated unruptured intracranial aneurysms. J Clin Neurosci. 2014;21(10):1734–1739. doi:10.1016/j.jocn.2013.12.032
23. Bonares MJ, de Oliveira Manoel AL, Macdonald RL, Schweizer TA. Behavioral profile of unruptured intracranial aneurysms: a systematic review. Ann Clin Transl Neurol. 2014;1(3):220–232. doi:10.1002/acn3.41
24. Wang X, Wang B, Du X, et al. Associations between neutrophil-lymphocyte ratio and risk of cognitive impairment among Chinese older adults. BMC Geriatr. 2025;25(1):114. doi:10.1186/s12877-025-05763-6
25. Mao FL, He X, Huang XL, Cheng YM, Qin FL, Wang YQ. Predictive value of lymphocyte-associated inflammation index in post-stroke cognitive impairment: a systematic review and meta-analysis. Front Neurol. 2025;15:1469152. doi:10.3389/fneur.2024.1469152
26. Dinia L, Vert C, Gramegna LL, et al. Wall enhancement as a biomarker of intracranial aneurysm instability: a histo-radiological study. Acta Neurochir. 2023;165(10):2783–2791. doi:10.1007/s00701-023-05739-8
27. Zhong W, Su W, Li T, et al. Aneurysm wall enhancement in unruptured intracranial aneurysms: a histopathological evaluation. J Am Heart Assoc. 2021;10(2):e018633. doi:10.1161/JAHA.120.018633
28. Quan K, Song J, Yang Z, et al. Validation of wall enhancement as a new imaging biomarker of unruptured cerebral aneurysm. Stroke. 2019;50(6):1570–1573. doi:10.1161/STROKEAHA.118.024195
29. Swiatek VM, Neyazi B, Roa JA, et al. Aneurysm wall enhancement is associated with decreased intrasaccular IL-10 and morphological features of instability. Neurosurgery. 2021;89(4):664–671. doi:10.1093/neuros/nyab249
30. Liu Q, Zhang Y, Zhu C, et al. Serum IL-1, pyroptosis and intracranial aneurysm wall enhancement: analysis integrating radiology, serum cytokines and histology. Front Cardiovasc Med. 2022;9:818789. doi:10.3389/fcvm.2022.818789
31. Ignacio KHD, Pascual JSG, Factor SJV, Khu KJO. A meta-analysis on the prevalence of anxiety and depression in patients with unruptured intracranial aneurysms: exposing critical treatment gaps. Neurosurg Rev. 2022;45(3):2077–2085. doi:10.1007/s10143-022-01768-6
32. Botto R, Callai N, Cermelli A, Causarano L, Rainero I. Anxiety and depression in Alzheimer’s disease: a systematic review of pathogenetic mechanisms and relation to cognitive decline. Neurol Sci. 2022;43(7):4107–4124. doi:10.1007/s10072-022-06068-x
33. Beurel E, Toups M, Nemeroff CB. The bidirectional relationship of depression and inflammation: double trouble. Neuron. 2020;107(2):234–256. doi:10.1016/j.neuron.2020.06.002
34. Jost Z, Kujach S. Understanding cognitive decline in aging: mechanisms and mitigation strategies—a narrative review. Clin Interv Aging. 2025;20:459–469. doi:10.2147/CIA.S510670
35. de Liyis BG, Surya SC, Tini K. Effectivity and safety of endovascular coiling versus microsurgical clipping for aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis. Clin Neurol Neurosurg. 2024;236:108058. doi:10.1016/j.clineuro.2023.108058
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.