")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Application of Multidisciplinary Rehabilitation Nursing in Patients with Brucellar Spondylitis and Its Effects on Pain, Inflammation, and Immune Function
Authors Zhang Y, Zuo X, Yang X, Li R, Wang H, Yu J, Yang X
Received 17 March 2025
Accepted for publication 19 June 2025
Published 2 July 2025 Volume 2025:18 Pages 3813—3826
DOI https://doi.org/10.2147/JMDH.S528741
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Ying Zhang,1 Xianhong Zuo,2 Xiao Yang,1 Rui Li,1 Huan Wang,1 Jiantao Yu,1 Xinming Yang1
1Department of Orthopedics, The First Affiliated Hospital of Hebei North University, Zhangjiakou, Hebei Province, 075000, People’s Republic of China; 2School of Nursing, Zhangjiakou University, Zhangjiakou, Hebei, 075000, People’s Republic of China
Correspondence: Xinming Yang, Email [email protected]
Objective: This study evaluated the effects of multidisciplinary rehabilitation nursing on postoperative outcomes in patients with brucellar spondylitis, focusing on pain, inflammation, immune function, emotional state, sleep quality, spinal mobility, adverse reactions, and patient satisfaction.
Methods: A retrospective analysis was conducted on 87 patients who underwent surgery for brucellar spondylitis between January 2020 and June 2024. Patients were divided into two groups: the Routine Group (n=43, receiving standard nursing care) and the Combined Group (n=44, receiving additional multidisciplinary rehabilitation nursing). Outcomes were assessed using the Visual Analog Scale (VAS), inflammatory markers (CRP, ESR, WBC), immune indicators (CD4+, CD8+, CD4+/CD8+), emotional scales (SAS, SDS), sleep quality (PSQI), spinal function (ODI), incidence of adverse reactions, and satisfaction (NSNS).
Results: The combined group exhibited significantly greater improvements than the routine group across most parameters. Postoperative pain (VAS) decreased more markedly at days 1 and 7. Inflammatory markers (CRP, ESR, WBC) and immune function (increased CD4+, CD4+/CD8+ and decreased CD8+) improved significantly by postoperative day 7, particularly in the combined group. Psychological status (SAS, SDS), sleep quality (PSQI), and spinal mobility (ODI) also improved more in the combined group. Adverse reaction rates were comparable between groups. However, patient satisfaction was significantly higher in the combined group (89.13%) than in the routine group (71.74%).
Conclusion: Multidisciplinary rehabilitation nursing, when integrated with conventional care, significantly improves pain control, inflammatory response, immune function, emotional well-being, sleep quality, and spinal mobility in patients with brucellar spondylitis, without increasing adverse events, and results in higher patient satisfaction.
Keywords: brucellar spondylitis, multidisciplinary rehabilitation nursing, effectiveness, pain, inflammation, immune function
Introduction
Brucellosis, a zoonotic chronic infectious disease caused by Brucella bacteria, is widely prevalent worldwide, particularly in regions where livestock farming is dominant.1,2 The clinical manifestations of brucellosis are diverse, including persistent fever, joint pain, fatigue, and excessive sweating. Among its complications, brucellar spondylitis is the most common and severe, causing significant morbidity.3 Brucellar spondylitis is characterized by inflammatory destruction of the vertebral body and intervertebral discs, leading to chronic back pain, restricted spinal movement, and in severe cases, spinal deformity and neurological impairment, which severely affect patients’ quality of life.4,5
Emerging evidence suggests that chronic brucellosis is frequently accompanied by neuropsychiatric manifestations, including depression, anxiety, autonomic nervous system dysfunction, and neuropathic pain due to central nervous system involvement.5,6 These neurological complications contribute significantly to the disease burden and are considered a major source of chronic pain, often surpassing the contribution from structural spinal lesions alone. Although the primary concentration of this study is brucellar spondylitis, multidisciplinary perioperative care, including psychological and neurorehabilitation strategies, was incorporated to address these broader systemic effects of chronic brucellosis, providing a more holistic assessment of patient outcomes.7 Given the high prevalence of neuropsychiatric symptoms and potential neuropathic pain in chronic brucellosis, pain management also included non-pharmacological strategies targeting central sensitization and emotional distress, such as mindfulness-based cognitive therapy and guided relaxation.8 These were aimed at modulating both physiological and psychological dimensions of pain, thereby enhancing analgesic effectiveness and patient quality of life.
Surgical intervention is an effective approach to mitigating severe pathological damage and restoring spinal function in brucellar spondylitis patients. However, due to the chronic inflammatory nature of the disease, postoperative recovery is often complex and accompanied by persistent pain, prolonged inflammation, immune dysfunction, increased psychological burden, and sleep disturbances.6,7 Therefore, optimizing perioperative nursing strategies is crucial to improving postoperative outcomes. Traditional perioperative nursing primarily focuses on basic care, wound management, and routine pain control, often neglecting the multisystem impact of brucellar spondylitis. This limitation results in slower postoperative recovery, reduced patient adherence to treatment, and lower satisfaction levels.8 In recent years, multidisciplinary rehabilitation nursing has been increasingly applied in perioperative management and has demonstrated significant advantages in the rehabilitation of chronic diseases and postoperative recovery.9–11 This model involves collaboration among multiple disciplines, including infectious disease specialists, rehabilitation medicine, psychology, nutrition, and nursing teams, to provide individualized, comprehensive rehabilitation interventions. Given the multifaceted challenges faced by brucellar spondylitis patients postoperatively, this study employs a retrospective analysis to evaluate the impact of multidisciplinary rehabilitation nursing on surgical patients. The findings aim to offer scientific insights and evidence for optimizing perioperative management in brucellar spondylitis.
Materials and Methods
Basic Information
This study adopted a retrospective research design, analyzing the clinical data of patients with brucellar spondylitis who underwent surgical treatment in our hospital from January 2020 to June 2024. The study was approved by the Medical Ethics Committee of the First Affiliated Hospital of Hebei North University (Approval No. HLPW2413) and strictly adhered to the ethical guidelines of the Declaration of Helsinki. Informed consent to participate was obtained from all of the participants in the study. Patients were divided into a Routine Group (n=43, receiving conventional nursing care) and a Combined Group (n=44, receiving multidisciplinary rehabilitation nursing in addition to conventional care). No significant differences were observed in gender, age, body mass index (BMI), disease duration, surgical type, educational level, or comorbidities between the two groups (P>0.05), indicating comparability, as shown in Table 1. All patients underwent standardized surgical procedures performed by the same surgical team using consistent operative protocols, ensuring uniformity of intraoperative management across both groups.
 |

Inclusion and Exclusion Criteria
Inclusion Criteria: (1) Met the clinical diagnostic criteria for brucellar spondylitis12 and was confirmed by Brucella antibody testing, bacterial culture, and imaging examinations; (2) Age ≥18 years, no gender restriction; (3) First-time diagnosis of brucellar spondylitis and underwent surgical treatment in our hospital; (4) Preoperative imaging (X-ray, CT, or MRI) confirmed vertebral, intervertebral disc, or adjacent structural involvement, with varying degrees of spinal dysfunction; (5) No prior spinal surgery, and disease progression met the study criteria; (6) Stable condition, capable of tolerating surgery, and met perioperative management requirements; (7) Patients and their families provided informed consent and were willing to participate in follow-up and assessment.
Exclusion Criteria: (1) Severe cardiac, pulmonary, hepatic, or renal dysfunction, making surgery intolerable; (2) Presence of other spinal diseases such as spinal tuberculosis, degenerative spinal disorders, or bone tumors; (3) Presence of autoimmune diseases, such as systemic lupus erythematosus or rheumatoid arthritis; (4) Long-term use of immunosuppressants or corticosteroids, affecting immune function evaluation; (5) Presence of mental disorders or cognitive impairment, making cooperation with nursing interventions impossible; (6) Patients who did not complete follow-up or had missing clinical data postoperatively.
Methods
Routine Group
The Routine Group received standard perioperative nursing interventions, including preoperative preparation, intraoperative assistance, and postoperative basic nursing care, as detailed below: (1) Preoperative Nursing: ① Basic health education: Patients and their families were informed about the pathogenesis of brucellar spondylitis, surgical procedures, and postoperative recovery precautions to enhance understanding and cooperation. ② Preoperative examinations and preparation: Complete blood count, coagulation function tests, electrocardiogram, and imaging examinations were performed to confirm surgical eligibility. ③ Psychological intervention: Nursing staff conducted preoperative visits to alleviate patient anxiety and tension; if necessary, families were involved in supportive communication. ④ Nutritional assessment: Based on the patient’s nutritional status, dietary guidance was provided, such as increasing protein and calorie intake to support postoperative recovery. (2) Intraoperative Nursing: ① Positioning management: Patient positioning was adjusted according to surgical requirements to prevent pressure-related tissue damage. ② Intraoperative monitoring: Vital signs were closely monitored to ensure a safe and stable surgical process. ③ Surgical assistance: Nurses assisted the surgeon in optimizing surgical field exposure and maintaining a sterile environment. (3) Postoperative Nursing: ① Pain management: Conventional analgesic medications (eg, NSAIDs, opioids) were administered postoperatively, and patients were guided in basic relaxation techniques such as deep breathing exercises. ② Wound care: The surgical site was inspected daily for signs of infection, and sterile dressing changes were performed to prevent wound complications. ③ Basic functional rehabilitation: Patients were encouraged to engage in early mobilization, including turning in bed and passive limb movements within postoperative days 1–3, to promote circulation and prevent deep vein thrombosis. ④ Discharge guidance: Patients were provided with home care instructions, including medication adherence, appropriate physical activity, and scheduled follow-up visits.
Combined Group
The Combined Group received multidisciplinary rehabilitation nursing in addition to routine nursing care, covering preoperative, intraoperative, and postoperative phases. The specific interventions were as follows: (1) Preoperative Nursing: ① Multidisciplinary assessment: A joint evaluation of the patient’s overall condition was conducted by the surgery, rehabilitation, psychology, nursing, and nutrition departments, followed by the development of an individualized nursing plan. Preoperative screening was performed for high-risk factors (eg, chronic disease history, immunodeficiency) with targeted management. ② Preoperative rehabilitation training: One week before surgery, patients were guided in core muscle training to enhance spinal stability and reduce postoperative dysfunction. Progressive postural training was applied to help patients adapt to early postoperative mobilization. ③ Psychological intervention: Cognitive behavioral therapy (CBT)13 was used to help patients manage anxiety and depression, thereby improving postoperative rehabilitation confidence. Relaxation music or guided meditation was introduced preoperatively to enhance sleep quality. ④ Nutritional support: Patients were advised to consume a diet rich in protein, vitamins, and minerals to boost immunity. For malnourished patients, preoperative nutritional supplements or enteral nutrition support was considered. (2) Intraoperative Nursing: ① Precise anesthesia management: Collaboration with the anesthesia team was undertaken preoperatively to select the optimal anesthesia method and dosage based on the patient’s condition to minimize postoperative pain. ② Intraoperative protective measures: Pressure-relieving cushions were used to prevent intraoperative pressure ulcers. Hemodynamic monitoring was performed to prevent hypotension or hypoxemia from affecting postoperative recovery. (3) Postoperative Nursing: ① Pain management: A multimodal analgesia strategy was adopted, combining NSAIDs, local anesthesia, and physical pain relief techniques (eg, cold compress, transcutaneous electrical nerve stimulation [TENS]) to minimize opioid dependence. Psychological counseling (eg, mindfulness meditation training) and non-pharmacological interventions such as music therapy were integrated to improve pain tolerance. ② Inflammation control: Inflammatory markers were dynamically monitored postoperatively, and antibiotic regimens were adjusted according to disease progression. ③ Immune regulation: Postoperative nutritional management was reinforced, with encouragement of a high-protein, vitamin-rich diet to promote immune cell recovery. Early guidance and assistance in gentle rehabilitation exercises (eg, limb movements in bed) were provided to enhance immune function. ④ Sleep quality management: For patients experiencing postoperative insomnia, non-pharmacological interventions such as relaxation training, aromatherapy, and warm foot baths were offered. ⑤ Rehabilitation training: On postoperative day 1 (POD1), patients were guided by rehabilitation therapists to perform ankle pump exercises and lower limb movements to prevent thrombosis. On POD3, bedside standing training was encouraged, gradually increasing activity levels. On POD7, core muscle strengthening exercises were introduced based on recovery progress to optimize spinal function. ⑥ Discharge follow-up management: Upon discharge, a personalized rehabilitation plan covering diet, exercise, and psychological interventions was provided. Both groups underwent preoperative to postoperative discharge care, with outcomes assessed on POD7.
Etiotropic Therapy Protocol
All patients received standardized etiotropic therapy prior to surgical intervention, consistent with national and WHO guidelines for the treatment of brucellosis. The primary regimen included doxycycline (100 mg orally, twice daily) and rifampicin (600–900 mg orally, once daily) for a minimum duration of 6 weeks. In cases presenting with severe or refractory symptoms, streptomycin (1 g intramuscularly, once daily for 2–3 weeks) was added during the initial phase of treatment. The mean duration of preoperative etiotropic therapy was 6.5 ± 1.2 weeks, with no significant differences between the Routine and Combined groups. Surgical intervention was considered only after patients completed at least 6 weeks of antibiotic therapy and showed radiological evidence of structural instability, persistent neurological deficits, or failure of conservative management despite microbiological improvement. Postoperatively, all patients continued oral doxycycline and rifampicin for an additional 6 weeks to reduce the risk of recurrence. Antibiotic regimens were consistent across both groups.
Observation Indicators
Pain Assessment
Postoperative pain control followed a standardized multimodal analgesia protocol for both groups. Non-steroidal anti-inflammatory drugs (NSAIDs; eg, celecoxib 200 mg/day) were the first-line agents. In cases of severe pain, opioids such as tramadol (50–100 mg orally, every 6–8 hours) were used judiciously for short-term relief. The Combined Group also received adjunctive therapies including TENS and psychological pain modulation techniques. All pain regimens were adjusted based on individual pain severity, VAS scores, and tolerability. Pain levels were assessed preoperatively, on POD1, and POD7 using the Visual Analog Scale (VAS) (Cronbach’s α coefficient = 0.896, validity = 0.843).14 The VAS ranges from 0 to 10, with higher scores indicating more severe pain.
Inflammatory Marker Levels
On preoperative day and POD7, 4 mL of fasting venous blood was collected from the elbow vein. After centrifugation or anticoagulation processing: C-reactive protein (CRP) was measured by immunoturbidimetry. Erythrocyte sedimentation rate (ESR) was determined using Westergren’s method. White blood cell count (WBC) was analyzed using a fully automated hematology analyzer.
Immune Function Indicators
To enhance the reliability of immune function assessments, CD4+ and CD8+ T lymphocyte subsets were quantified both in relative percentages (%) and absolute counts (cells/µL) using flow cytometry. This approach allowed for a more accurate analysis of postoperative immune status. Antibiotic therapy was taken into account when interpreting these immune indices, as Brucella-targeted antimicrobials may influence lymphocyte subset distribution. On preoperative day and POD7, 4 mL of fasting venous blood was collected from the elbow vein and preserved in heparinized anticoagulant tubes. Flow cytometry (FCM) was used to detect peripheral blood T lymphocyte subsets (CD4+ and CD8+ levels), and the CD4+/CD8+ ratio was calculated.
Negative Emotional State
On preoperative day and POD7, anxiety and depression were assessed using: Self-Rating Anxiety Scale (SAS) (Cronbach’s α = 0.857, validity = 0.825); Self-Rating Depression Scale (SDS) (Cronbach’s α = 0.876, validity = 0.841).15 Both scales have a total score of 100 points, with cutoff scores of 50 for SAS and 53 for SDS, where higher scores indicate more severe negative emotions.
Sleep Quality Assessment
Psychological disturbances and sleep disorders observed in some patients were primarily attributed to chronic pain, limited mobility, and long-term disease burden rather than acute brucella intoxication. All patients had completed the full recommended course of etiotropic therapy prior to surgery, and none showed signs of ongoing active systemic infection at the time of psychological evaluation. Thus, mood and sleep disturbances were considered secondary to chronic dysfunction and addressed accordingly with rehabilitation and supportive care. On preoperative day and POD7, sleep quality was evaluated using the Pittsburgh Sleep Quality Index (PSQI) (Cronbach’s α = 0.846, validity = 0.819).16 The total PSQI score ranges from 0 to 21, with higher scores indicating poorer sleep quality.
Spinal Mobility Function
On preoperative day and POD7, spinal mobility dysfunction was assessed using the Oswestry Disability Index (ODI) (Cronbach’s α = 0.863, validity = 0.840).17 The questionnaire includes 10 items, each scored from 0 to 5. ODI score (%) = (actual score / 50) × 100%, with higher percentages indicating more severe spinal mobility dysfunction.
Incidence of Adverse Reactions
Adverse events occurring during hospitalization (eg, pressure injuries, deep vein thrombosis [DVT], bleeding, infection, and nerve damage) were recorded by medical staff.
Satisfaction Assessment
At the end of the intervention, nursing satisfaction was assessed using the Newcastle Nursing Service Satisfaction Scale (NSNS) (Cronbach’s α = 0.852, validity = 0.834).18 The scale consists of 19 items, scored using a 5-point Likert scale, with higher scores indicating greater satisfaction. Score categories: Very satisfied (≥76 points); Satisfied (57–75 points); Neutral (38–56 points); Dissatisfied (<38 points). Total satisfaction rate (%) = (very satisfied cases + satisfied cases) / total cases × 100%.
Statistical Analysis
All data were analyzed using SPSS 22.0 software. Categorical variables were expressed as n (%) and analyzed using the χ²-test. Continuous variables were expressed as ( ) and compared between groups using the independent sample t-test. Within-group comparisons were analyzed using the paired t-test. Repeated measures analysis of variance (ANOVA) was used for comparisons across multiple time points. In addition to between-group comparisons, paired t-test was conducted to assess pre- and postoperative changes within each group, thereby enabling clearer interpretation of treatment effects, including in the routine group. A P-value <0.05 was considered statistically significant.
) and compared between groups using the independent sample t-test. Within-group comparisons were analyzed using the paired t-test. Repeated measures analysis of variance (ANOVA) was used for comparisons across multiple time points. In addition to between-group comparisons, paired t-test was conducted to assess pre- and postoperative changes within each group, thereby enabling clearer interpretation of treatment effects, including in the routine group. A P-value <0.05 was considered statistically significant.
Results
Comparison of Pain Levels
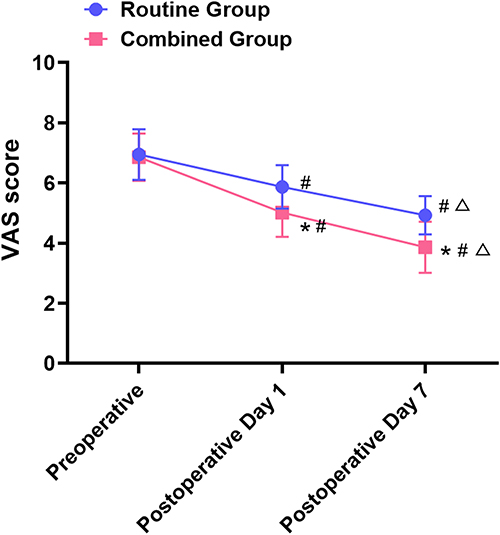
There were significant differences in group effects (F=9.736), time effects (F=12.458), and interaction effects (F=10.561) of VAS scores between the two groups (P<0.05). Within-group comparisons: VAS scores on postoperative day 1 (POD1) and postoperative day 7 (POD7) were significantly lower than preoperative scores in both groups, and POD7 scores were significantly lower than POD1 scores (P<0.05). In the routine group, these reductions from baseline were statistically significant (P<0.05), confirming the effectiveness of conventional care alone; however, the combined group exhibited a significantly greater reduction at each time point (P<0.05), highlighting the added value of the multidisciplinary approach. Between-group comparisons: No significant difference was observed in preoperative VAS scores between the two groups (P>0.05), but the Combined Group had significantly lower VAS scores at POD1 and POD7 than the Routine Group (P<0.05), as shown in Figure 1.

Comparison of Inflammatory Marker Levels
At POD7, CRP, ESR, and WBC levels in both groups were significantly lower than preoperative levels, with a more pronounced decrease in the Combined Group compared to the Routine Group (P<0.05), as shown in Figure 2.
 |
Figure 2 Comparison of inflammatory marker levels ( Notes: Compared with the Routine Group at the same time point, *P<0.05; compared with preoperative levels within the same group, #P<0.05. |

Comparison of Immune Function Indicators
At POD7, CD4+ and CD4+/CD8+ levels were higher, while CD8+ levels were lower than preoperative values in both groups, with a more significant change observed in the Combined Group compared to the Routine Group (P<0.05), as shown in Figure 3.
 |
Figure 3 Comparison of immune function indicators ( Notes: Compared with the Routine Group at the same time point, *P<0.05; compared with preoperative levels within the same group, #P<0.05. |

Comparison of Negative Emotional States
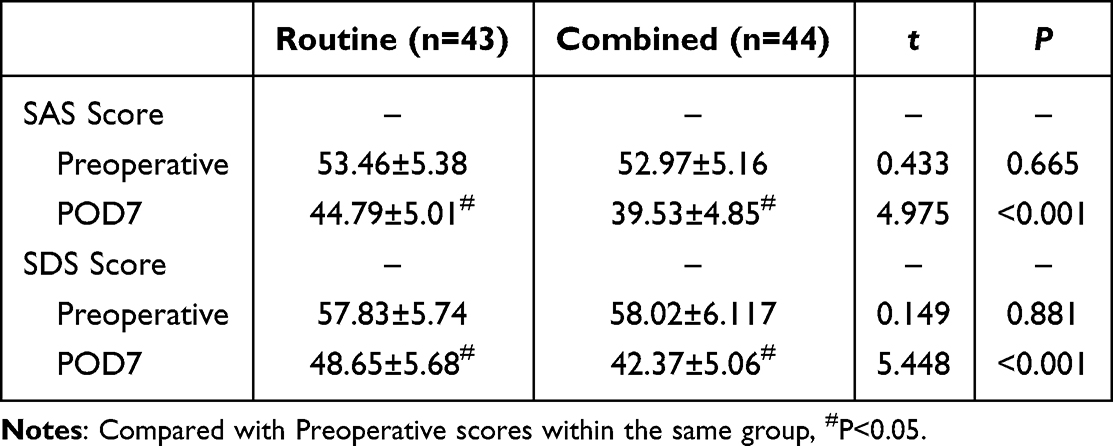
At POD7, SAS and SDS scores in both groups were significantly lower than preoperative values, with the Combined Group showing a greater reduction compared to the Routine Group (P<0.05), as shown in Table 2.
 |

Comparison of Sleep Quality and Spinal Mobility Function
At POD7, PSQI and ODI scores in both groups were significantly lower than preoperative values, with a greater reduction in the Combined Group compared to the Routine Group (P<0.05), as shown in Table 3.
 |
Table 3 Comparison of Sleep Quality and Spinal Mobility Function ( |

Comparison of Adverse Reactions
The incidence of adverse reactions did not differ significantly between the Combined Group and the Routine Group (13.64% vs 16.28%, P>0.05), as shown in Table 4.
 |
Table 4 Comparison of Adverse Reactions [n (%)] |
Comparison of Satisfaction Levels
Among 43 patients in the Routine Group, 11 were very satisfied, 20 were satisfied, 9 were neutral, and 3 were dissatisfied. Among 44 patients in the Combined Group, 19 were very satisfied, 21 were satisfied, 3 were neutral, and 1 was dissatisfied. The satisfaction rate in the Combined Group was significantly higher than that in the Routine Group (90.91% vs 72.09%, P<0.05), as shown in Figure 4.
 |
Figure 4 Comparison of satisfaction levels [n (%)]. Notes: Compared with the Routine Group, *P<0.05. |
Discussion
Effect of Multidisciplinary Rehabilitation Nursing on Postoperative Pain
Postoperative pain not only affects patient comfort but may also lead to anxiety, depression, and resistance to rehabilitation training, thereby delaying functional recovery. Therefore, pain management should not only focus on pain relief itself but also consider its impact on overall rehabilitation. The results of this study showed that VAS scores at postoperative day 1 (POD1) and postoperative day 7 (POD7) were significantly lower in the Combined Group compared to the Routine Group (P<0.05), indicating the superiority of multidisciplinary rehabilitation nursing in postoperative pain management. This finding is consistent with previous studies,19 which suggest that while single-mode analgesia may alleviate acute postoperative pain, its long-term efficacy is often insufficient. In contrast, a comprehensive analgesic strategy that integrates psychological interventions and rehabilitation training can effectively shorten the duration of postoperative pain and enhance pain tolerance. In this study, the Combined Group adopted a multimodal analgesia strategy, incorporating pharmacological analgesia, physical analgesia, and psychological analgesia, which enabled multilayered pain management and improved analgesic effectiveness. Moreover, Chen et al20 found that patients with higher preoperative anxiety levels often reported higher postoperative pain scores, possibly due to heightened pain perception caused by anxiety. In this study, preoperative pain expectation education and anxiety interventions were implemented in the Combined Group, which helped patients develop more rational psychological expectations about postoperative pain, thus reducing actual pain perception postoperatively. Additionally, rehabilitation training played a crucial role in pain relief. Early postoperative bedside limb exercises and progressive standing training not only enhanced local blood circulation and accelerated pain mediator metabolism but also prevented muscle stiffness and joint contracture caused by prolonged inactivity, thereby reducing pain levels in patients.
Effect of Multidisciplinary Rehabilitation Nursing on Inflammation Control and Immune Function
Persistent postoperative inflammation can delay tissue repair and increase the risk of infections and complications.21 At the same time, patients with brucellar spondylitis often exhibit immune dysfunction, and prolonged postoperative inflammation can further weaken immune function, reducing the body’s resistance to infection.22 The results of this study showed that at POD7, CRP, ESR, WBC, and CD8+ levels were significantly lower in the Combined Group compared to the Routine Group, while CD4+ and CD4+/CD8+ ratio were significantly higher (P<0.05), indicating that multidisciplinary rehabilitation nursing not only effectively controlled inflammation but also improved immune function, thereby enhancing overall resistance. The underlying mechanisms of these effects may be attributed to the comprehensive intervention strategies used in the Combined Group. First, dynamic monitoring of inflammatory and immune function markers allowed for individualized adjustment of anti-inflammatory and immune support strategies, ensuring precise and optimized treatment. This personalized management prevented the risks associated with both overuse and underuse of antibiotics, thereby enhancing targeted anti-inflammatory therapy. Additionally, nutritional interventions were reinforced in the Combined Group, with dietary plans enriched in proteins, vitamins, Omega-3 fatty acids, glutamine, and trace elements (zinc, selenium). These nutrients have been shown to enhance anti-inflammatory capacity, accelerate inflammation resolution, and promote immune cell recovery. Furthermore, enhanced nutritional support and immune-focused interventions, such as a high-protein diet and early mobilization, coincided with statistically significant improvements in CD4+, CD4+/CD8+ ratios, and reductions in inflammatory markers (CRP, ESR, WBC; all P<0.05), indicating a measurable physiological impact. Additionally, the implementation of multimodal analgesia combined with non-pharmacological strategies (eg, TENS, cold compresses, mindfulness) directly contributed to superior pain control postoperatively (VAS score reduction). Finally, personalized discharge planning and follow-up played a role in improving overall nursing satisfaction scores, with a higher total satisfaction rate in the Combined Group. These findings collectively demonstrate that each major component of the multidisciplinary rehabilitation nursing program exerted a distinct and statistically verifiable influence on the recovery trajectory. Moreover, the role of moderate exercise in inflammation control and immune activation has gained increasing attention. Yao et al23 demonstrated that early rehabilitation training could enhance T-cell proliferation, improve macrophage phagocytic activity, and reduce postoperative inflammatory cytokine accumulation, thereby lowering infection risks. In this study, patients in the Combined Group initiated bedside mobility on POD1 and gradually progressed to standing and walking exercises on POD3-5, effectively preventing postoperative immunosuppression caused by prolonged bed rest, and thereby enhancing the body’s immune defense capabilities.
Effect of Multidisciplinary Rehabilitation Nursing on Psychological State and Sleep Quality
Postoperative pain, hospitalization environment changes, and uncertainty about the disease may contribute to anxiety, depression, and sleep disturbances.24 This study found that at POD7, SAS, SDS, and PSQI scores were significantly lower in the Combined Group compared to the Routine Group (P<0.05), indicating that multidisciplinary rehabilitation nursing had a positive impact on alleviating negative emotions and improving sleep quality. This finding is consistent with the results of Zhang et al,25 who reported that patients receiving CBT and mindfulness training postoperatively exhibited significantly lower anxiety and depression scores, along with notable improvements in sleep quality. In this study, CBT and progressive relaxation training were introduced preoperatively to help patients develop accurate perceptions of postoperative pain and recovery processes. Postoperatively, mindfulness training, meditation therapy, and family involvement were encouraged to enhance patients’ sense of security and confidence in recovery. Furthermore, sleep quality improvement was closely associated with precise pain management. Studies26 have shown that postoperative pain can disrupt sleep architecture, while sleep deprivation exacerbates pain perception, creating a vicious cycle. The precise analgesia strategy in the Combined Group effectively minimized pain-related insomnia, while psychological interventions reduced anxiety-induced sleep difficulties, ultimately leading to significant improvements in postoperative sleep quality.
Effect of Multidisciplinary Rehabilitation Nursing on Postoperative Functional Recovery
Restoring spinal function after surgery is a primary rehabilitation goal for patients with brucellar spondylitis.27 The results of this study showed that at postoperative day 7 (POD7), the reduction in ODI scores was significantly greater in the Combined Group than in the Routine Group (P<0.05), indicating that this model is more effective in promoting postoperative functional recovery. Several studies28,29 have confirmed that early rehabilitation training can significantly improve postoperative functional outcomes and reduce the risk of long-term disability. In this study, the Combined Group initiated core muscle training preoperatively to enhance spinal stability and establish a solid foundation for postoperative recovery. Postoperatively, the group received early individualized rehabilitation training, including bedside activities, progressive walking exercises, and balance training, to accelerate functional recovery. Notably, psychological interventions also played a key role in functional recovery. Shi et al30 found that postoperative patients who received psychological interventions exhibited greater adherence to rehabilitation training and faster functional recovery compared to those who did not receive such interventions. In this study, CBT, mindfulness meditation, and family support systems were integrated into the Combined Group’s rehabilitation process, enhancing patient engagement and encouraging active participation in recovery, ultimately leading to improved spinal function.
Effect of Multidisciplinary Rehabilitation Nursing on Patient Satisfaction
Patient satisfaction is not only an indicator of nursing quality but also directly affects the rehabilitation experience and treatment adherence. The results of this study showed that patient satisfaction was significantly higher in the Combined Group than in the Routine Group (P<0.05), demonstrating that multidisciplinary rehabilitation nursing is more effective in improving patient satisfaction. This finding aligns with the study by Xu et al,31 which identified personalized nursing, rehabilitation effectiveness, and psychological support as key determinants of patient satisfaction. The Combined Group’s nursing model enhanced care precision through individualized nursing plans. For instance, patients underwent preoperative assessments to develop personalized strategies, including pain management, nutritional support, and rehabilitation training, which were dynamically adjusted postoperatively based on patient progress, making the nursing approach more scientific and flexible. Postoperative pain control is another key factor influencing nursing satisfaction. The Combined Group’s use of a multimodal analgesia strategy resulted in more effective pain relief, reducing the negative impact of pain on sleep, mood, and rehabilitation adherence, thereby improving patients’ overall perception of nursing care. Additionally, psychological interventions and sleep management optimizations played crucial roles in enhancing satisfaction. Preoperatively, CBT helped patients develop a clear understanding of surgery and recovery, reducing anxiety and improving psychological adaptability. Postoperatively, mindfulness training, music therapy, and sleep environment optimization improved emotional stability, making the overall recovery experience more comfortable. The statistically significant group, time, and interaction effects found in repeated measures ANOVA support the conclusion that the multidisciplinary approach produced superior outcomes compared to routine care alone. Notably, preoperative psychological interventions such as CBT and music-guided relaxation were closely associated with significant reductions in postoperative anxiety and depression scores (SAS and SDS), suggesting their direct contribution to improved emotional resilience. Similarly, preoperative core muscle training and progressive rehabilitation exercises initiated as early as POD1 were strongly linked to greater functional recovery as evidenced by significantly lower ODI scores. Furthermore, the multidisciplinary collaborative nursing model fostered stronger communication among healthcare teams, enhancing the systematic and professional nature of nursing care. This approach provided comprehensive care support,32 allowing patients to gain a clearer understanding of their recovery process, which in turn increased their trust in the nursing team and overall healthcare system.
Limitations and Future Directions
Although this study demonstrated that multidisciplinary rehabilitation nursing effectively improved postoperative pain management, inflammation control, immune function, psychological state, sleep quality, spinal function recovery, and patient satisfaction in brucellar spondylitis patients, some limitations must be acknowledged:
(1) Limited Sample Size: The relatively small sample size, despite strict inclusion and exclusion criteria, may introduce statistical bias, and the generalizability of findings requires further validation. (2) Short Follow-up Period: This study focused on short-term outcomes (within POD7) and did not assess long-term rehabilitation progress or recurrence rates. Future research should incorporate extended follow-up periods to evaluate the long-term effects of this nursing model. (3) Single-center Retrospective Study: This study was conducted at a single institution, potentially limiting its applicability to other hospitals with different nursing standards. Future research should conduct multicenter, large-sample prospective randomized controlled trials (RCTs) to improve reliability and clinical applicability. (4) Complexity of Intervention Factors: Multidisciplinary rehabilitation nursing integrates pain management, inflammation control, psychological intervention, and rehabilitation training, making it challenging to isolate the independent contributions of each factor. Future studies should employ multivariate analyses or stratified studies to determine the specific impact of each intervention component. (5) One notable limitation of this study is the relatively short follow-up period, with outcomes assessed only up to postoperative day 7. While this timeframe allowed for the evaluation of early postoperative recovery in terms of pain, inflammation, immune function, psychological state, and mobility, it is insufficient for determining the long-term efficacy and sustainability of the multidisciplinary rehabilitation nursing approach. Evaluating long-term outcomes, such as recurrence rates, functional independence, and quality of life, requires extended follow-up, ideally ranging from three to six months or longer. Future prospective studies incorporating long-term follow-up will be essential to validate these preliminary findings and to provide a more comprehensive assessment of patient prognosis and the enduring impact of multidisciplinary interventions. (6) Patient Adherence Variability: Rehabilitation outcomes depend heavily on patient adherence, and individual differences in engagement with rehabilitation training, psychological interventions, and sleep management may affect results. Future research could incorporate behavioral studies to optimize adherence strategies. Compared to routine nursing, multidisciplinary rehabilitation nursing more effectively alleviates postoperative pain, reduces inflammation, enhances immune function, improves psychological well-being and sleep quality, and promotes spinal function recovery, ultimately improving patients’ quality of life. By integrating precise assessments, individualized nursing plans, multimodal pain management, inflammation control, early rehabilitation training, and psychological interventions, this approach enables comprehensive postoperative recovery management, increasing patient adherence and satisfaction. Future research should further refine nursing protocols, extend follow-up periods, and conduct large-scale, multicenter studies to confirm the long-term effectiveness of multidisciplinary rehabilitation nursing and optimize nursing interventions for postoperative management of brucellar spondylitis.
Funding
Hebei Medical Science Research Project (20200504, 20241026); 2024 Zhangjiakou City Level Science and Technology Plan Project (2421133D).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rudolf I, Kejíková R, Kosoy M, et al. Brucella microti and rodent-borne brucellosis: a neglected public health threat. Zoonoses Public Health. 2025;72(1):1–8. doi:10.1111/zph.13188
2. Meletis E, Sakhaee E, Kostoulas P. Bayesian true prevalence estimation of brucellosis in sheep, goats, cattle and camels in southeast regions of Iran. Zoonoses Public Health. 2024;71(2):170–177. doi:10.1111/zph.13095
3. Wu P, Zhang Y-J, Guo H-B, et al. [values of apparent diffusion coefficient and fractional anisotropy in the diagnosis of brucella spondylitis]. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2020;42(2):154–163. Danish. doi:10.3881/j.issn.1000-503X.11300
4. Çiftdoğan DY, Aslan S. Osteoarticular involvement of brucellosis in pediatric patients: clinical and laboratory characteristics. Turk J Pediatr. 2020;62(2):199–207. doi:10.24953/turkjped.2020.02.005
5. Lu YP, Qiu W-Q, Zhang T, et al. Epidemiology and laboratory testing of brucella spondylitis. Sci Rep. 2024;14(1):26345. doi:10.1038/s41598-024-77391-w
6. Jiang D, Ma L, Wang X, et al. Comparison of two surgical interventions for lumbar brucella spondylitis in adults: a retrospective analysis. Sci Rep. 2023;13(1):16684. doi:10.1038/s41598-023-43812-5
7. Zhang Y, Zhao C, Chen J, et al. Beneficial influence of single-stage posterior surgery for the treatment of lumbar brucella spondylitis combined with spondylolisthesis. Sci Rep. 2022;12(1):19459. doi:10.1038/s41598-022-24223-4
8. Baron-Epel O, Obeid S, Kababya D, et al. A health promotion perspective for the control and prevention of brucellosis (Brucella melitensis); Israel as a case study. PLoS Negl Trop Dis. 2022;16(9):e0010816. doi:10.1371/journal.pntd.0010816
9. Wang TL. [Accelerating the transformation from anesthesia clinic to comprehensive anesthesia and multi-disciplinary evaluation, consultation, pre-rehabilitation and follow-up center in outpatient under aged society]. Zhonghua Yi Xue Za Zhi. 2023;103(41):3229–3231. Danish. doi:10.3760/cma.j.cn112137-20230609-00983
10. Lian B, Yu PF, Yang B, et al. [Management of radiation-induced intestinal injury: from multi-disciplinary team team to holistic integrative management]. Zhonghua Wei Chang Wai Ke Za Zhi. 2023;26(10):922–928. Hawaiian. doi:10.3760/cma.j.cn441530-20230709-00241
11. Liu XZ, Wu AW. [Role of multidisciplinary cooperation in the diagnosis and treatment of pelvic floor disorder disease]. Zhonghua Wei Chang Wai Ke Za Zhi. 2021;24(4):306–309. Hawaiian. doi:10.3760/cma.j.cn.441530-20210107-00006
12. Wu N, Zhang Y, Yu YS. Pedro Pons’ sign of brucellar spondylitis. Rev Soc Bras Med Trop. 2020;53:e20190561. doi:10.1590/0037-8682-0561-2019
13. Golovacheva VA, Golovacheva AA, Fateeva TG, et al. [Cognitive behavioral therapy in the treatment of patients with chronic migraine and concomitant chronic insomnia: a prospective, randomized trial]. Zh Nevrol Psikhiatr Im S S Korsakova. 2024;124(5. Vyp. 2):110–117. Hungarian. doi:10.17116/jnevro2024124052110
14. Lu JS, Qian BP, Qiu Y, et al. [The best preferable sagittal vertical axis for the ankylosis spondylitis with thoracolumbar kyphosis following one-level pedicle subtraction osteotomy under different cervical range of motion]. Zhonghua Yi Xue Za Zhi. 2025;105(1):48–55. Danish. doi:10.3760/cma.j.cn112137-20240730-01753
15. He TT, Zhang XH, Kong XL, et al. [Effect of virtual reality video-based pre-discharge psychological intervention on the post-discharge emotions of patients with deep facial burns: a prospective randomized controlled study]. Zhonghua Shao Shang Za Zhi. 2021;37(1):70–75. Danish. doi:10.3760/cma.j.cn501120-20191226-00473
16. Yang YP, Ding YY, Wang YY, et al. [Effects of preoperative quetiapine on postoperative delirium and sleep quality in elderly orthopaedic patients]. Zhonghua Yi Xue Za Zhi. 2023;103(41):3252–3257. Danish. doi:10.3760/cma.j.cn112137-20230719-00029
17. Guo Y, Wan WT, Bian HM, et al. [Occurrence and risk factors of adjacent segment degeneration after early extreme lateral interbody fusion]. Zhonghua Yi Xue Za Zhi. 2025;105(9):681–687. Danish. doi:10.3760/cma.j.cn112137-20240821-01931
18. Yin H. Enhanced recovery after surgery (ERAS) in postoperative lung cancer patients: a novel perioperative strategy for preventing venous thromboembolism and improving quality of life. Tohoku J Exp Med. 2024;262(3):201–209. doi:10.1620/tjem.2023.J105
19. Lin JH, Zhang YW, Mao QJ, et al. [Clinical practice of minimally invasive daytime hepatectomy based on enhanced recovery after surgery whole-process management scheme]. Zhonghua Wai Ke Za Zhi. 2025;63(4):331–337. Hawaiian. doi:10.3760/cma.j.cn112139-20241031-00481
20. Chen MT, Yu HJ, Yang LJ, et al. [Efficacy of early interdisciplinary palliative care based on WARM model in non-small-cell lung cancer]. Zhonghua Yi Xue Za Zhi. 2021;101(45):3736–3741. Danish. doi:10.3760/cma.j.cn112137-20210607-01298
21. Khaidarova Y, Kurmanova G, Nurgaliyeva G, et al. What could lead to the production of anti-rheumatoid antibodies in patients with brucellosis spondylodiscitis: possible causes. Med J Islam Repub Iran. 2024;38:89. doi:10.47176/mjiri.38.89
22. Senevirathne A, Hewawaduge C, Lee JH. Live vaccine consisting of attenuated Salmonella secreting and delivering brucella ribosomal protein L7/L12 induces humoral and cellular immune responses and protects mice against virulent brucella abortus 544 challenge. Vet Res. 2020;51(1):6. doi:10.1186/s13567-020-0735-y
23. Yao YM, Zhang H. [Rehabilitation strategy for the improvement of long-term outcomes of patients after sepsis]. Zhonghua Shao Shang Yu Chuang Mian Xiu Fu Za Zhi. 2022;38(3):201–206. Danish. doi:10.3760/cma.j.cn501120-20211004-00344
24. Chao JY, Xiong KP, Zhuang S, et al. [Relationship between emotional apathy and motor symptoms, sleep and cognitive function in patients with early Parkinson’s disease]. Zhonghua Yi Xue Za Zhi. 2021;101(35):2792–2797. Danish. doi:10.3760/cma.j.cn112137-20210130-00286
25. Zhang Y, Zhang H, Zhang Y, et al. Effect of MBSR, DBT and CBT on the hypertension patients with depression/anxiety: protocol of a systematic review and Bayesian network meta-analysis. PLoS One. 2023;18(2):e0281469. doi:10.1371/journal.pone.0281469
26. Liu HL, Song YN, Wang XX, et al. [Effects of whole-course multimodal analgesia on postoperative pain and rapid recovery in elderly patients with urological tumors]. Zhonghua Yi Xue Za Zhi. 2023;103(41):3245–3251. Danish. doi:10.3760/cma.j.cn112137-20230725-00089
27. Kou XS, She W, Ma G-F, et al. [One-stage posterior debridement and spinal internal fixation for the treatment of lumbar Brucellar spondylitis]. Zhongguo Gu Shang. 2024;37(8):764–771. Danish. doi:10.12200/j.issn.1003-0034.20230255
28. Agranovich NV, Muskhadzhieva RM, Sivolapova MS, et al. [The effectiveness of the use of non-drug treatment complexes and their impact on quality of life indicators, the psychosomatic status of patients with residual brucellosis with lesions of the musculoskeletal system]. Vopr Kurortol Fizioter Lech Fiz Kult. 2022;99(5):28–36. Polish. doi:10.17116/kurort20229905128
29. Tschopp R, GebreGiorgis A, Abdulkadir O, et al. Risk factors for brucellosis and knowledge-attitude practice among pastoralists in Afar and Somali regions of Ethiopia. Prev Vet Med. 2022;199:105557. doi:10.1016/j.prevetmed.2021.105557
30. Shi WZ, Chen HY, Wang F. [Comprehensive intervention combined with cognitive psychological care based on quality chain for patients with benign prostatic hyperplasia]. Zhonghua Nan Ke Xue. 2024;30(4):331–335. Basque
31. Xu J, Xie Y, Yuan D, et al. [Feasibility and safety study of building a friendly management model for elderly critically ill patients based on geriatric intensive care unit: a prospective controlled study]. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024;36(8):867–870. Dutch. doi:10.3760/cma.j.cn121430-20240109-00024
32. Zhong WZ. [Chinese expert consensus on the multidisciplinary team diagnosis and treatment of lung cancer]. Zhonghua Zhong Liu Za Zhi. 2020;42(10):817–828. Polish. doi:10.3760/cma.j.cn112152-20200812-00731
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Temporal Changes in Ankle Joint Pathology, Pain and Secondary Osteoporosis in Collagen-Induced Arthritis Rats
Liu Q, Nan N, Li W, Dong M, Pu W, Liu Y, Zhao J, Hao H
Journal of Inflammation Research 2024, 17:9795-9804
Published Date: 26 November 2024