")
Back to Journals » Clinical Ophthalmology » Volume 18
Application of Negative Pressure by the Ocular Pressure Adjusting Pump to Provide a Sustained Reduction in IOP
Authors Ferguson TJ , Herndon LW, Terveen DC , Shah M, Samuelson TW, Yoo P, Berdahl JP
Received 5 September 2024
Accepted for publication 1 November 2024
Published 6 November 2024 Volume 2024:18 Pages 3171—3178
DOI https://doi.org/10.2147/OPTH.S492530
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Tanner J Ferguson,1 Leon W Herndon,2 Daniel C Terveen,1 Manjool Shah,3 Thomas W Samuelson,4 Paul Yoo,5 John P Berdahl1
1Vance Thompson Vision, Sioux Falls, SD, USA; 2Duke University, Durham, NC, USA; 3New York University Langone Health, New York, NY, USA; 4Minnesota Eye Consultants, Minneapolis, MN, USA; 5Balance Ophthalmics, Inc., Sioux Falls, SD, USA
Correspondence: Tanner J Ferguson, Vance Thompson Vision, 3101 W. 57th Street, Sioux Falls, SD, USA, Email [email protected]
Purpose: To evaluate the sustainability of IOP reduction with continuous negative pressure application over an extended duration with use of the Ocular Pressure Adjusting Pump.
Methods: Prospective, controlled, open-label, randomized, single site, pilot study. Subjects with primary open-angle glaucoma (OAG) were enrolled. One eye of each subject was randomized to receive negative pressure application; the fellow eye served as a control. The study eye negative pressure setting was programmed for 60% of the baseline IOP. Subjects wore the Ocular Pressure Adjusting Pump for 8 consecutive hours and IOP measurements occurred at 2-hour intervals for a total of 5 IOP measurements (08:00, 10:00, 12:00, 14:00, 16:00).
Results: Nine subjects successfully enrolled and completed the study. The mean programmed negative pressure setting was − 12.0 mmHg. At baseline, the mean IOP in the study eye was 21.4 ± 4.3 mmHg. The mean IOP reduction in the study eye at hours 0, 2, 4, 6, and 8 was 8.1 (37%), 6.4 (28%), 6.3 (29%), 7.3 (34%) and 6.7 (31%), respectively. All IOP measurements during negative pressure application were reduced from baseline. There were no serious adverse events.
Conclusion: The Ocular Pressure Adjusting Pump provides a sustained reduction in IOP while the device is worn with negative pressure applied with an IOP reduction exceeding 25% across 8 hours of continuous wear.
Keywords: negative pressure, ocular pressure adjusting pump, multi-pressure dial, open angle glaucoma
Introduction
Glaucoma is a leading cause of global blindness.1 Intraocular pressure (IOP) remains the only clinically-validated and modifiable risk factor associated with development and progression of glaucoma.2 Current treatment methods all target the reduction of IOP including topical ocular medications, laser procedures, and surgeries ranging from micro-invasive glaucoma procedures to traditional filtering procedures to facilitate an alternative drainage pathway.3,4 Although the glaucoma treatment landscape has undergone considerable advancement over the last decade, the currently available treatment options have limitations and risk factors and often require the clinician to weigh effectiveness versus safety. Currently, there is no treatment option available to reduce IOP which can be categorized as non-surgical or non-pharmacological.
The Ocular Pressure Adjusting Pump, or OPAP (FYSX™ Ocular Pressure Adjusting Pump, Balance Ophthalmics, Inc., USA) is a novel treatment device that consists of a pair of pressure-sensing goggles connected to a pressure-modulating pump.5–7 When the goggles are worn by a subject, negative pressure (or vacuum) is applied to create a localized decrease in atmospheric pressure contacting the eye, leading to a corresponding decrease in IOP. This mechanism of action is based on Pascal’s law, which states that when there is a change in pressure at any point in a confined fluid, there is an equal change throughout the fluid. The design of the Ocular Pressure Adjusting Pump allows for individualized and titratable negative pressure application to each eye. Multiple studies have been performed highlighting the safety and tolerability of the device.5–8
The Ocular Pressure Adjusting Pump was FDA approved in July 2024 and the IOP-lowering efficacy of the device has been well established by multiple previous studies;5,8 however, in prior work, the IOP measurements were not measured repeatedly throughout the treatment interval or involved a removal of the device to place specially designed goggles for IOP measurement during negative pressure application. Further, because no current tonometry methods allow for IOP measurements through the goggles during negative pressure application, a novel method of measurement was developed.
A recently published clinical trial evaluated the safety and effectiveness of negative pressure application for IOP reduction over a 90-day period, where IOP assessments were performed at Days 0, 30, 60, and 90. In this study, nearly 90% of eyes achieved an IOP reduction ≥20% and there was a 33.4% reduction in overall mean IOP from a baseline IOP of 19.4 ± 3.6 mmHg to 12.9 ± 3.2 mmHg on top of current medications.9 Collectively, these studies support the longitudinal IOP-lowering performance of the device. This present study aims to evaluate the sustained reduction in IOP throughout an extended duration of uninterrupted negative pressure application.
Methods
This prospective, fellow-eye controlled study was performed at a single site (Sioux Falls, SD). The study procedures were in accordance with the 1964 helsinki declaration and its later amendments or comparable ethical standard. All subjects included in the study provided informed consent prior to the beginning of the study. This study was designated as a non-significant risk clinical study and did not require clinical trial registration. This study was approved by the Advarra Institutional Review Board.
Inclusion Criteria
For this study, key inclusion criteria were subjects aged ≥22, a documented diagnosis of OAG in both eyes (OAG was inclusive of primary open-angle glaucoma and normal-tension glaucoma), periorbital anatomy that enabled a proper and secure, air-tight seal with the device in place and ability to tolerate IOP measurements with the device. Further, subjects had to have a screening IOP value ≥15 mmHg and ≤22 mmHg measured via Goldmann applanation tonometry in both eyes at the baseline visit with or without the use of IOP-lowering medication.
For exclusion criteria, subjects with the presence or history of an eye condition/disease that could limit evaluation of the study results or compromise patient safety were excluded. Subjects with macular degeneration, retinal detachment or other fundus findings that could limit visualization of the posterior segment in either eye were excluded. Subjects with eyelid edema, conjunctival chemosis, history of corneal transplant or history of allergy to any of the testing materials (eg, silicone) were excluded. Subjects with a history of a filtering procedure (eg, tube shunt or trabeculectomy) in either eye were also excluded. Subjects with narrow anterior chamber anatomy in either eye as visualized by gonioscopy with a Shaffer angle grade ≤2 in any of the four quadrants were also excluded.
Study Device
The Ocular Pressure Adjusting Pump is comprised of two components: pressure-sensing goggles and a programmable, pressure-modifying pump (Figure 1). The two components are connected via tubing that allows for control of each periorbital region with individualized tubing extending to each eye. This enables separate negative pressure control for each eye. Further, the OPAP goggles and pump are connected via a dual lumen tubing system through which both pressure-sensing and pressure delivery occur, for a closed-loop, instantaneous control of negative pressure.
 |
Figure 1 Ocular Pressure Adjusting Pump (OPAP) The system creates a pressure-controlled environment in front of the eye. The system applies pressure in 1 mmHg increments to the front of the eye until sensors confirm that the target pressure has been achieved. |
This study included a specially adapted version of the OPAP goggles, known as the Excursion Ocular Pressure Adjusting Pump. The Excursion iteration of the device is identical to the standard version but is adapted with an access port on each side to facilitate IOP measurements while the device is active with negative pressure application. Moreover, the Excursion Ocular Pressure Adjusting Pump used in this study included an anesthetic port (Figure 2) established by a gasket in the lens of the goggles that allowed for application of topical anesthetic while maintaining the vacuum seal. This anesthetic port allowed for the instillation of topical anesthetic via a 27-gauge cannula prior to IOP measurements at each 2-hour interval. This device and the corresponding IOP measurement method have been described in detail by multiple previous studies validating the technique for IOP measurement.10–12
 |
Figure 2 The anesthetic port modification in the Excursion OPAP is shown in the nasal quadrant of the goggle lens, which allows instillation of topical anesthetic onto the surface of the cornea while maintaining a sealed environment. |
IOP Measurement Method
Because no current tonometry method allows IOP measurement through goggles and during negative pressure application, a novel method was developed for use with the device. This method of IOP measurement, also known as Excursion tonometry across the cornea relative to atmospheric pressure. This method of measurement was previously described in detail10–12 with favorable results consistent with the parameters of approved tonometry methods, supporting its use as a reliable method of IOP measurement. Excursion tonometry occurs with the Excursion adaptation of the Ocular Pressure Adjusting Pump, which include an access port on each side through which Excursion cartridges are placed to maintain the negative pressure environment while allowing a channel to contact the cornea. The Excursion cartridge consists of a silicone tube fitted with a latex Tono-Pen® cover. Upon proper fitting of the goggles and positioning of the cartridges, a Model 30™ pneumatonometer is employed to contact the corneal surface across the Tono-Pen® cover (which is positioned on the cornea) and obtain IOP measurements.
Study Design
Upon signing the informed consent, subjects were evaluated for eligibility and completed a battery of baseline testing to confirm their eligibility based on inclusion/exclusion criteria. The screening assessment included a manifest refraction, BCDVA (best-corrected distance visual acuity), slit lamp examination, gonioscopy and IOP measurement via Goldmann applanation tonometry (GAT). The screening IOP via GAT was used as the value for inclusion and had to be between ≤22 mmHg and ≥15 mmHg. Screening assessment also included a fitting to ensure that the subjects could comfortably wear the device while achieving a proper seal. All of this occurred on Visit 1.
Following Visit 1 and screening, treatment and control eye assignment occurred via a randomization sequence. Visit 2 occurred within 7 days of Visit 1 and was allowed to occur on the same day. Prior to beginning the study on Visit 2, IOP was also measured using pneumatonometry with the Model 30 (M30) pneumatonometer. The value obtained via pneumatonometry was used to determine the negative pressure (NP) setting for the duration of the study. For the treatment eye, an NP setting equal to 60% of the M30 value was used while the contralateral control eye was programmed to a negative pressure setting of 0 mmHg.
Following determination of the NP setting for the 8-hour wear period, subjects were re-fitted with the OPAP goggles to establish a secure seal prior to commencing the 8-hour period of uninterrupted negative pressure application. All subjects wore the Excursion OPAP for this study. After the Excursion goggles were placed on the subject, an IOP measurement via Excursion tonometry occurred prior to negative pressure application to serve as the baseline IOP measurement and the baseline value that was compared to IOP measurements obtained throughout the 8-hour wear period. After the baseline measurement, the device was programmed to the appropriate negative pressure settings for each eye and the study period was initiated.
During the study period, IOP measurements occurred immediately following initiation of negative pressure application and at 2-hour intervals for a total of up to 5 IOP measurements (08:00, 10:00, 12:00, 14:00, 16:00) across an 8-hour maximum treatment period. Across the 8-hour period, subjects were allowed to sit comfortably and maintained a seated position. Following the 8-hour period, an additional measurement was obtained immediately following cessation of negative pressure at the conclusion of the 8-hour study treatment.
Statistical Analysis
A repeated-measures ANOVA was performed to analyze the IOP data at each time point in the study eye. Post-hoc paired t-tests were performed with a Bonferroni correction to perform multiple comparisons between the IOP at baseline and at the various time points, including the time point immediately following the 8-hour study period. The mean and standard deviation are presented for continuous variables. A significance level of 0.05 was set.
Results
Efficacy
Ten subjects were enrolled into the study. One subject discontinued the device owing to a headache with the goggles after 45 minutes of wear. 9 subjects successfully completed the study and wore the device for the complete 8 hours without interruption. Of the 9 subjects, 6 were female and 3 were male. The average age was 67.1 ± 12.7 years (range 41–83).
At baseline, the mean IOP in the study eye was 21.4 ± 4.3 mmHg. The mean programmed negative pressure setting was −12.0 mmHg. Across the 8-hour study duration with negative pressure application, the mean IOP in the study eye was 14.4 ± 2.6 mmHg, representing a 32% (7.0 mmHg) reduction from baseline. Following the 8-hour study period and cessation of negative pressure, the mean IOP in the study eye was 23.1 ± 3.5 mmHg (P=0.71). The mean IOP in the study eye at hours 0, 2, 4, 6, and 8 was 13.3 ± 3.6, 15.0 ± 2.8, 15.1 ± 3.4, 14.1 ± 5.2 and 14.7 ± 4.4 mmHg, respectively. The percent IOP reduction values at hours 0, 2, 4, 6 and 8 were 38% (8.1, P<0.01), 30% (6.4, P<0.01), 29% (6.3, P<0.01), 34% (7.3, P<0.01) and 31% (6.7, P<0.01). All IOP measurements with negative pressure application in the study eye represented a reduction in IOP from baseline.
In the control eye, the mean IOP at baseline was 20.4 ± 3.6 mmHg. The control eye was programmed to 0 mmHg throughout the entire study. At hours 0, 2, 4, 6 and 8, the mean IOP via Excursion tonometry in the control eye was 17.6 ± 3.0 (P<0.05), 19.3 ± 2.8 (P>0.9), 20.8 ± 3.6 (P>0.9), 19.4 ± 4.3 (P>0.9) and 20.1 ± 4.1 (P>0.9) mmHg, respectively. Across the entire study period, the mean IOP in the control eye was 19.5 ± 3.6 mmHg. Following the 8-hour study period, the mean IOP in the control eye was 22.9 ± 4.4 mmHg (P=0.12). The IOP outcomes are shown below in Figure 3. Table 1 shows the percent reduction in IOP for both the study and control eyes by time point.
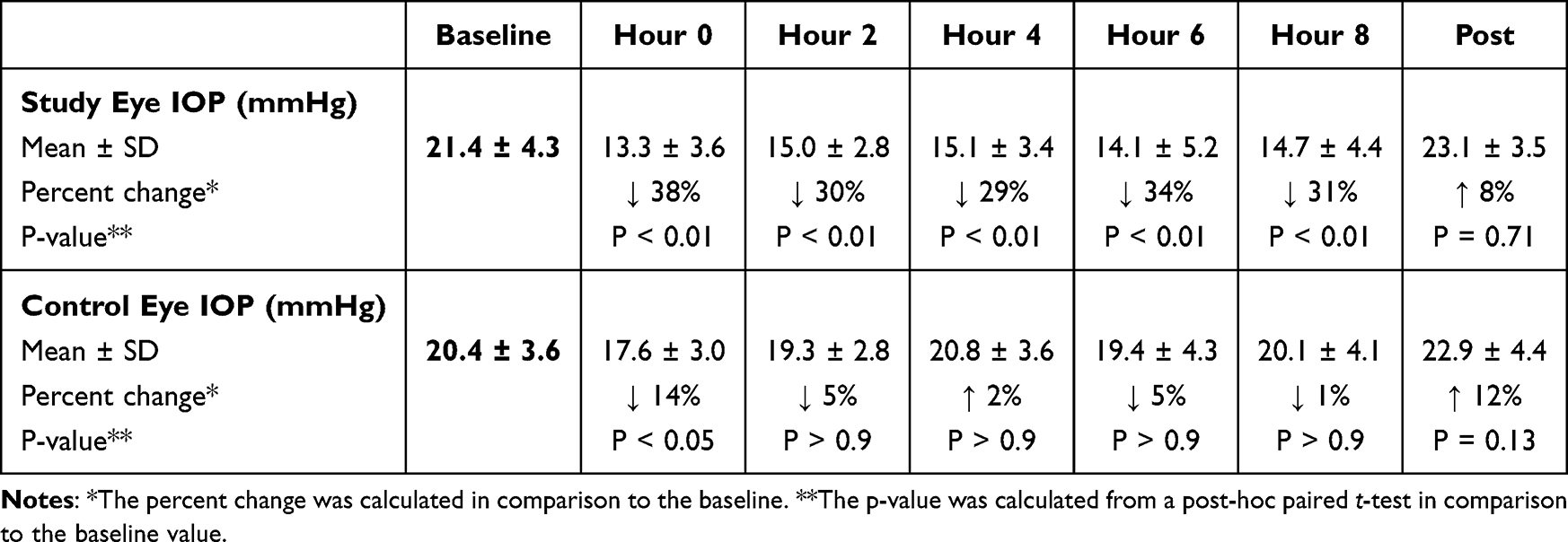 |
Table 1 Mean IOP Measurements at Various Time Points in the Study and Control Eye. The Percent Change from Baseline and the p-value Comparing the Value to Baseline in Shown for All Time Points Following the Baseline Measurement |
 |
Figure 3 The mean IOP in the study and control eye is shown at each time point including at baseline and across 8 hours of continuous, uninterrupted negative pressure application. |
Safety
There were no serious adverse events in the study. There were two minor adverse events that occurred. One subject proceeded through screening but was only able to wear the device for 45 minutes due to a headache. The headache resolved promptly and without intervention after removal of the device, and the subject was subsequently exited from the study. At the slit lamp examination following the 8-hour wear session, a corneal abrasion was identified in another subject that was attributed to the repeated IOP measurements. The corneal abrasion responded to topical therapy and resolved without sequelae by the follow-up examination two days later. There was no associated loss of BCDVA in any patient.
Discussion
The current IOP-lowering treatment options for glaucoma include medications, laser procedures, implantable devices, and a variety of filtering procedures.3 Even with the emergence and introduction of numerous novel medical and surgical options, many patients do not achieve an adequate reduction in IOP and demonstrate progression of disease despite having an apparent “controlled” IOP value.13 Furthermore, it is difficult to lower IOP further on patients who are already on medications or have IOPs in the low teens. This is particularly true in patients with normal-tension and severe open-angle glaucoma, two subsets of glaucoma in which the current range of treatments such as lasers, medications and MIGS procedures have diminished IOP-lowering effect.14,15 Traditional, filtering surgical options offer favorable IOP-lowering results but have an increased risk profile and high rate of failure.16 The Ocular Pressure Adjusting Pump is a promising new treatment option that has shown consistent IOP-lowering results across multiple studies and would represent the first non-pharmacologic, non-procedural option for reduction of IOP.
The safety profile of the Ocular Pressure Adjusting Pump has been extensively studied in multiple, prior studies including a recently published multicenter clinical trial.5,7,9,17 In addition, a prior study by Shafer et al18 assessed the impact of negative pressure application on both IOP and retrobulbar pressure (RBP) in cadaver subjects. In this study, across multiple test runs, there was no detectable change in RBP, showing that negative pressure application with the device does not lead to changes in pressure behind the eye. Additionally, there has been interest in using OCT angiography (OCT-A) to deepen our understanding of glaucoma and the alterations in the retinal microvasculature with pressure changes and glaucomatous damage.19 In a recent study by Kamalipour et al, the effects of short-term IOP reduction on the retinal microvasculature were evaluated by measuring capillary density.20 In this study, using OCT-A, they identified a dose-dependent increase in the retinal microcirculation during IOP reduction with the Ocular Pressure Adjusting Pump.
A multitude of studies have also highlighted the IOP-lowering efficacy of the Ocular Pressure Adjusting Pump; however, for each of these studies, the IOP was not measured repeatedly throughout the treatment interval or involved a suction break to place specially adapted goggles for IOP measurement. This study is the first to obtain IOP measurements throughout an extended duration of wear and the results support the sustained IOP reduction and absence of tachyphylaxis with the device. In this study, the IOP reduction at hour 0 (37%) was similar to the IOP reduction achieved at hours 6 (34%) and 8 (31%), demonstrating that the IOP reduction is sustained throughout the duration of wear. At each time point, the IOP reduction in the study eye exceeded 25% with the IOP reduction at hours 0, 6 and 8 all exceeding 30%. These results are consistent with two mathematical modeling studies that predicted a sustained reduction in pressure and decreased strain at the optic nerve head with the Ocular Pressure Adjusting Pump.21,22 Further, consistent with prior work23 evaluating the device, every IOP measurement in this study with negative pressure application demonstrated a reduction in IOP.
This study is not without limitations. This was a single-center, open-label study with a relatively small sample size. There was an increase in IOP following the 8-hour study period in the study eye; however, the increase in IOP was not statistically different (P=0.7) from baseline and was <10% different in comparison to baseline and nearly all of the IOP measurements with application of negative pressure were >30% reduction from baseline. In this study, IOP measurements were obtained with the Excursion test method, a newly developed form of IOP measurement designed specifically for the OPAP. However, the precision and accuracy of Excursion tonometry has been validated with multiple studies.10–12 Further, the recently published clinical trial evaluating the Ocular Pressure Adjusting Pump included both GAT and Excursion tonometry and the mean difference between the two methods was <1 mmHg, highlighting the favorable agreement between the two methods of tonometry.9
Conclusion
The results of this study demonstrate that the IOP reduction conferred by the Ocular Pressure Adjusting Pump is sustained while the device is worn with active negative pressure with an IOP reduction exceeding 25% across 8 hours of continuous wear. Further, the safety profile of this study is consistent with prior work evaluating the device with an absence of IOP spikes following wear of the device. As the first non-surgical, non-pharmacologic option for IOP reduction, the OPAP holds promise as a potential new treatment option for patients with glaucoma.
Funding
This study was sponsored by Balance Ophthalmics, Inc.
Disclosure
Drs. Ferguson, Herndon, Terveen, Samuelson and Yoo are consultants for Balance Ophthalmics. Dr. Shah reports consulting fees from AbbVie, Alcon, Glaukos, ONL Therapeutics, Nova, Elios, and Bausch and Lomb, outside the submitted work. Dr. Berdahl is the founder and owner of Balance Ophthalmics. The authors report no other conflicts of interest in this work.
References
1. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
2. Heijl A, Leske MC, Bengtsson B, et al. Reduction of intraocular pressure and glaucoma progression: results from the early manifest glaucoma trial. Arch Ophthalmol. 2002;120(10):1268–1279. doi:10.1001/archopht.120.10.1268
3. Conlon R, Saheb H, Ahmed IIK. Glaucoma treatment trends: a review. Can J Ophthalmol. 2017;52(1):114–124. doi:10.1016/j.jcjo.2016.07.013
4. Lavia C, Dallorto L, Maule M, Ceccarelli M, Fea AM. Minimally-invasive glaucoma surgeries (MIGS) for open angle glaucoma: a systematic review and meta-analysis. PLoS One. 2017;12(8):e0183142. doi:10.1371/journal.pone.0183142
5. Swan RJ, Ferguson TJ, Shah M, et al. Evaluation of the IOP-lowering effect of a multi-pressure dial at different negative pressure settings. Trans Vision Sci Technol. 2020;9(12):19. doi:10.1167/tvst.9.12.19
6. Samuelson TW, Ferguson TJ, Radcliffe NM, et al. 8 hrs safety evaluation of a multi-pressure dial in eyes with glaucoma: prospective, open-label, randomized study. Clin Ophthalmol. 2019;13:1947–1953. doi:10.2147/OPTH.S217736
7. Ferguson TJ, Radcliffe NM, Van Tassel SH, et al. Overnight safety evaluation of a multi-pressure dial in eyes with glaucoma: prospective, open-label, randomized study. Clin Ophthalmol. 2020;14:2739–2746. doi:10.2147/OPTH.S256891
8. Goldberg JL, Jiminez-Roman J, Hernandez-Oteyza A, Quiroz-Mercado H. Short-term evaluation of negative pressure applied by the multi-pressure dial system to lower nocturnal IOP: a prospective, controlled, intra-subject study. Ophthalmol Ther. 2021;10(2):349–358. doi:10.1007/s40123-021-00343-4
9. Samuelson TW, Ferguson TJ, Brubaker JW, et al. Negative pressure application via a multi-pressure dial to lower IOP in patients with suspected glaucoma or open-angle glaucoma. J Glaucoma. 2023;32:708–720. doi:10.1097/IJG.0000000000002231
10. Ferguson TJ, Knier CG, Chowdhury UR, et al. Intraocular pressure measurement with pneumatonometry and a tonometer tip cover. Ophthalmol Ther. 2020;9:127–137. doi:10.1007/s40123-020-00235-z
11. Brambilla E, Ferguson TJ, Chu N, Ammar D, Yoo P. Intraocular pressure measurement with pneumatonometry and a tonometer tip cover during negative pressure application. OPTH. 2022;16:1289–1300. doi:10.2147/OPTH.S359605
12. Chu N, Brambilla E, Yoo P, Ferguson TJ. Evaluation of negative pressure transfer through tissue in a benchtop cornea and eyelid model. Ophthalmol Eye Dis. 2020;12:251584142097140. doi:10.1177/2515841420971406
13. Leske MC, Heijl A, Hussein M, Bengtsson B, Hyman L, Komaroff E. Factors for glaucoma progression and the effect of treatment: the early manifest glaucoma trial. Arch Ophthalmol. 2003;121(1):48–56. doi:10.1001/archopht.121.1.48
14. De Moraes CG. Natural history of normal-tension glaucoma with (very) low intraocular pressure. Ophthalmology. 2019;126(8):1117–1118. doi:10.1016/j.ophtha.2019.02.003
15. Lee JWY, Chan PP, Zhang X, Chen LJ, Jonas JB. Latest developments in normal-pressure glaucoma: diagnosis, epidemiology, genetics, etiology, causes and mechanisms to management. Asia Pac J Ophthalmol. 2019;8(6):457–468. doi:10.1097/01.APO.0000605096.48529.9c
16. Gedde SJ, Herndon LW, Brandt JD, et al. Postoperative complications in the tube versus trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153(5):804–814.e1. doi:10.1016/j.ajo.2011.10.024
17. Thompson VM, Ferguson TJ, Ahmed IIK, et al. Short-term safety evaluation of a multi-pressure dial: a prospective, open-label, non-randomized study. Ophthalmol Ther. 2019;8(2):279–287. doi:10.1007/s40123-019-0181-y
18. Shafer B, Ferguson TJ, Chu N, Brambilla E, Yoo P. The Effect of Periocular Negative Pressure Application on Intraocular and Retrobulbar Pressure in Human Cadaver Eyes. Ophthalmol Ther. 2022;11(1):365–376. doi:10.1007/s40123-021-00442-2
19. WuDunn D, Takusagawa HL, Sit AJ, et al. OCT angiography for the diagnosis of glaucoma: a report by the American Academy of Ophthalmology. Ophthalmology. 2021;128(8):1222–1235. doi:10.1016/j.ophtha.2020.12.027
20. Kamalipour A, Moghimi S, Inpirom VR, Mahmoudinezhad G, Weinreb RN. Multi-pressure dial goggle effects on circumpapillary structure and microvasculature in glaucoma patients. Ophthalmol Glaucoma. 2022;5(6):572–580. doi:10.1016/j.ogla.2022.05.004
21. Safa BN, Bleeker A, Berdahl JP, Ethier CR. The effects of negative periocular pressure on biomechanics of the optic nerve head and cornea: a computational modeling study. Trans Vision Sci Technol. 2023;12(2):5. doi:10.1167/tvst.12.2.5
22. Ethier CR, Yoo P, Berdahl JP. The effects of negative periocular pressure on intraocular pressure. Exp Eye Res. 2020;191:107928. doi:10.1016/j.exer.2020.107928
23. Peters KS, Brambilla E, Ferguson T, Kramer B, Terveen D, Berdahl J. Manometric intraocular pressure reduction with negative pressure using ocular pressure adjusting pump goggles. Ophthalmol Glaucoma. 2024;S2589419624001777. doi:10.1016/j.ogla.2024.09.005
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.