")
Back to Journals » Clinical Ophthalmology » Volume 18
Artificial Intelligence in Uveitis: Innovations in Diagnosis and Therapeutic Strategies
Authors Murugan SRB, Sanjay S , Somanath A, Mahendradas P, Patil A, Kaur K, Gurnani B
Received 22 September 2024
Accepted for publication 6 December 2024
Published 14 December 2024 Volume 2024:18 Pages 3753—3766
DOI https://doi.org/10.2147/OPTH.S495307
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Siva Raman Bala Murugan,1 Srinivasan Sanjay,2 Anjana Somanath,3 Padmamalini Mahendradas,4 Aditya Patil,4 Kirandeep Kaur,5 Bharat Gurnani6
1Department of Uveitis and Ocular Inflammation Uveitis Clinic, Aravind Eye Hospital, Pondicherry, 605007, India; 2Department of Clinical Services, Singapore National Eye Centre, Third Hospital Ave, Singapore City, 168751, Singapore; 3Department of Uveitis and Ocular Inflammation, Aravind Eye Hospital, Madurai, Tamil Nadu; 4Department of Uveitis and Ocular Immunology, Narayana Nethralaya, Bangalore, Karnataka, 560010, India; 5Department of Cataract, Pediatric Ophthalmology and Strabismus, Gomabai Netralaya and Research Centre, Neemuch, Madhya Pradesh, 458441, India; 6Department of Cataract, Cornea and Refractive Surgery, Gomabai Netralaya and Research Centre, Neemuch, Madhya Pradesh, 458441, India
Correspondence: Siva Raman Bala Murugan, Consultant- Uveitis Services, Aravind Eye Hospital, Pondicherry, 605007, India, Email [email protected]
Abstract: In the dynamic field of ophthalmology, artificial intelligence (AI) is emerging as a transformative tool in managing complex conditions like uveitis. Characterized by diverse inflammatory responses, uveitis presents significant diagnostic and therapeutic challenges. This systematic review explores the role of AI in advancing diagnostic precision, optimizing therapeutic approaches, and improving patient outcomes in uveitis care. A comprehensive search of PubMed, Scopus, Google Scholar, Web of Science, and Embase identified over 10,000 articles using primary and secondary keywords related to AI and uveitis. Rigorous screening based on predefined criteria reduced the pool to 52 high-quality studies, categorized into six themes: diagnostic support algorithms, screening algorithms, standardization of Uveitis Nomenclature (SUN), AI applications in management, systemic implications of AI, and limitations with future directions. AI technologies, including machine learning (ML) and deep learning (DL), demonstrated proficiency in anterior chamber inflammation detection, vitreous haze grading, and screening for conditions like ocular toxoplasmosis. Despite these advancements, challenges such as dataset quality, algorithmic transparency, and ethical concerns persist. Future research should focus on developing robust, multimodal AI systems and fostering collaboration among academia and industry to ensure equitable, ethical, and effective AI applications. The integration of AI heralds a new era in uveitis management, emphasizing precision medicine and enhanced care delivery.
Keywords: artificial intelligence, uveitis management, machine learning, deep learning, optical coherence tomography, AI, ML, DL, OCT
Introduction
Artificial intelligence (AI) has become a cornerstone in modern medical practice, offering unprecedented opportunities for enhancing diagnostic accuracy and treatment efficacy across various disciplines.1 In ophthalmology, AI’s integration is particularly promising due to the field’s reliance on imaging and precise diagnostic criteria.2 Uveitis, an umbrella term for a group of inflammatory diseases affecting the uvea, presents significant diagnostic and therapeutic challenges due to its heterogeneity and complex etiologies.3 The application of AI in uveitis management represents a frontier for improving patient outcomes through advanced computational techniques. Historically, the diagnosis and management of uveitis have relied heavily on clinical expertise and a combination of imaging modalities, laboratory tests, and sometimes invasive procedures.4 The introduction of AI into this domain aims to streamline these processes, reduce diagnostic errors, and provide personalized treatment plans. AI technologies, including machine learning (ML) and deep learning (DL), have shown remarkable capabilities in image analysis, pattern recognition, and predictive modeling, which are critical in managing a multifaceted condition like uveitis.5 A major challenge in uveitis lies in the lack of standardized nomenclature and diagnostic criteria, as the condition encompasses a wide spectrum of inflammatory manifestations. AI algorithms have shown promise in addressing this gap by enabling automated categorization and diagnostic support through the Standardization of Uveitis Nomenclature (SUN) Working Group initiatives. These efforts leverage machine learning to standardize diagnostic protocols, ensuring consistency across clinical settings. Additionally, AI tools facilitate the identification of subtle inflammatory patterns that are often missed during conventional assessments, thereby improving diagnostic precision and aiding early intervention.6 The development of AI in healthcare can be traced back to the mid-20th century, with computational models initially focused on simulating human thought processes. The subsequent evolution of neural networks and the advent of DL algorithms in the 1990s significantly advanced AI’s potential applications in medicine.1 In ophthalmology, AI has predominantly been explored for retinal diseases such as diabetic retinopathy and age-related macular degeneration. However, its application in uveitis is gaining traction, driven by the need for more accurate diagnostic tools and efficient management strategies.7
Another critical gap in uveitis management is the variability in disease presentation and progression, which often complicates clinical decision-making. AI-driven diagnostic tools, such as automated grading systems for anterior chamber inflammation and vitreous haze, have demonstrated high accuracy in detecting subtle disease markers. These advancements allow clinicians to stratify patients more effectively and tailor interventions to individual needs, paving the way for precision medicine. Furthermore, AI-powered predictive models can forecast disease progression and treatment outcomes, enabling proactive management of this complex condition.1 Recent advancements in AI, particularly in natural language processing (NLP) and image processing, have opened new avenues for its application in uveitis. For instance, the Generative Pre-trained Transformer (GPT) models, developed by OpenAI, have demonstrated substantial proficiency in language understanding and healthcare diagnostics, achieving notable accuracy in medical licensing examinations and ophthalmic knowledge assessments.8 These models can process large volumes of clinical data, providing insights that can enhance decision-making and patient care. In uveitis, AI applications range from automated grading of inflammatory activity using optical coherence tomography (OCT) to developing screening algorithms for identifying ocular infections such as toxoplasmosis.4 Studies have shown that AI can achieve high accuracy in detecting anterior chamber inflammation and vitreous haze, which are critical indicators of uveitis activity. Moreover, AI-driven diagnostic support systems can assist clinicians in differentiating between various uveitis subtypes, potentially leading to more targeted and effective treatments.9 Despite these advancements, the implementation of AI in uveitis management faces several challenges. These include the need for high-quality, representative datasets, transparency in AI decision-making processes, and addressing ethical concerns related to data privacy and algorithmic biases.10 Future research should focus on improving AI model robustness, integrating multimodal data, and ensuring that AI tools are validated across diverse populations and clinical settings. Through enhanced data standardization and the incorporation of AI-driven precision medicine, clinicians can address current limitations in the management of uveitis, including variability in diagnosis, inefficiency in treatment workflows, and disparities in access to care. The potential of AI to revolutionize uveitis management is immense, promising more precise diagnostics, personalized treatment plans, and ultimately better patient outcomes.11 However, realizing this potential requires concerted efforts from researchers, clinicians, and industry stakeholders to address the existing limitations and ethical considerations. By harnessing the power of AI, we can pave the way for a new era in the diagnosis and treatment of uveitis, characterized by increased accuracy, efficiency, and equity in healthcare delivery.12 In the dynamic landscape of uveitis, the fusion of artificial intelligence (AI) with clinical correlation heralds a new era in the understanding and management of ocular diseases. The uniqueness of uveitis, characterized by its multifaceted inflammatory nature, emerges as a focal point for AI-driven advancements. This article navigates the intricate intersection where cutting-edge AI algorithms intersect with the complexities of uveitis, illuminating the transformative potential of machine learning, deep learning, and other AI methodologies in reshaping our approach to diagnosis and treatment in this challenging ocular pathology.13
Literature Review
To achieve a comprehensive understanding of the application of artificial intelligence (AI) in uveitis, a systematic search was conducted across multiple databases, including PubMed, Scopus, Google Scholar, Web of Science, and Embase. The search incorporated a broad range of terminologies and Boolean operators to ensure inclusivity of relevant studies. Primary keywords included “artificial intelligence”, “machine learning”, “deep learning”, “uveitis”, “ocular inflammation”, and their combinations using “AND” and “OR” commands. Secondary search terms such as “uveitic”, “posterior uveitis”, “anterior uveitis”, “intermediate uveitis”, “panuveitis”, and related phrases like “ocular AI diagnostics” and “AI-based screening in ophthalmology” were added to enhance specificity and coverage. The search strategy was further refined by including terms associated with disease manifestations and clinical features such as “retinal vasculitis”, “choroiditis”, “iridocyclitis”, and “scleritis”. Articles focused on AI applications in systemic diseases with ocular manifestations, such as “Behçet’s disease”, “sarcoidosis”, and “juvenile idiopathic arthritis”, were also included. Additionally, references to AI algorithms and tools like “neural networks”, “support vector machines”, “decision support systems”, and “predictive modeling” were explored. The initial screening identified over 10,000 articles. After applying language filters (non-English, Spanish, Portuguese) and excluding duplicates, non-human studies, and unrelated topics, 7,521 articles remained. A secondary screening based on titles and abstracts eliminated 6,754 irrelevant studies, leaving 767 articles for full-text review. Stringent inclusion criteria focused on studies published between 2008 and 2024, addressing AI’s diagnostic, prognostic, and therapeutic roles in uveitis. Ultimately, 52 articles were selected for thematic analysis.
The selected articles were categorized into six thematic areas: (1) diagnostic support algorithms, (2) screening algorithms, (3) standardization of Uveitis Nomenclature (SUN) using AI, (4) applications of AI in uveitis management, (5) systemic implications of AI in associated diseases, and (6) challenges, opportunities and future directions in AI-based uveitis research. Figure 1 provides a visual depiction of the literature review process, including detailed strategies for search refinement and article selection.
 |
Figure 1 Depicts the literature review strategy for artificial intelligence in uveitis. |
Detection Algorithms and Tools in Uveitis
Computational mathematic models which could predict results after sample-based training was first reported in 1950.14 Artificial intelligence showed more progress in the 1990s with the development of convolutional neural networks and deep learning [DL] models.15 Deep learning models can process images, written and spoken languages.16 The convergence of artificial intelligence (AI) and healthcare offers opportunities to enhance clinical decision-making and medical education. The increasing proficiency of AI in diagnosing various ocular conditions emphasizes its potential impact in the field of ophthalmology.17,18 Ophthalmology, by virtue of its image-based diagnosis, blends in for a marriage with AI. Ophthalmological AI algorithms have been applied mainly in diabetic retinopathy screening, age-related macular degeneration, retinopathy of prematurity, and corneal diseases,19 with diabetic retinopathy screening FDA-approved devices such as IDx-DR and EyeArt.20 Abellanas et al21 in their review of AI in uveitis noted that presently the performance of AI models were poor with limited datasets and a lack of validation studies and publicly available data and codes. Artificial intelligence could transform healthcare if it provides the treating clinical physicians accurate diagnosis, stratification of risk of progression and management protocols to allow for cost-effective care.22,23 Abellanas et al,21 in their review, included articles into 4 categories: diagnosis support algorithms, findings detection algorithms, screening algorithms, and Standardization of Uveitis Nomenclature (SUN) articles. The strengths include detection algorithms in uveitis leverage advanced deep learning (DL) models to process complex medical images and language data, enabling precise diagnosis and classification of ocular diseases. The integration of AI with ophthalmology has already shown success in related fields, such as diabetic retinopathy and age-related macular degeneration, demonstrating its potential for uveitis. The limitation include current AI models for uveitis are hindered by small, non-representative datasets, limiting their generalizability and robustness across diverse populations. The lack of publicly available datasets and validated studies impairs reproducibility and clinical trust in these algorithms.
Artificial Intelligence in Uveitis Education and Beyond: The Role of GPT Models
Natural language processing (NLP) models, such as the Generative Pre-trained Transformer (GPT) series developed by OpenAI, in San Francisco, CA, USA, have demonstrated significant potential in advancing language comprehension and healthcare diagnostics.24,25 GPT models are trained on a textual database, learning to generate coherent and contextually appropriate responses based on the abstract relationships between words (tokens) within the neural network.26 Previous research indicates that GPT-3.5 achieves an accuracy rate of over 50% on the United States Medical Licensing Examination (USMLE), approaching the 60% pass mark. Additionally, more than 90% of AI responses offer substantial insights, showcasing deductive reasoning beneficial for human learners.27 The capabilities of GPT models extend beyond general medical education; for instance, when tested with practice ophthalmic board questions, ChatGPT correctly answered 46% of them in January 2023.28 Subsequently, the GPT model has undergone an update from GPT-3.5 to GPT-4.0, indicating potential improvements in AI-enabled medical education. The new model exhibits enhanced contextual understanding, improved topic consistency, and significantly increased accuracy, demonstrated by its success on professional and academic assessments, transitioning from the 10th percentile to the 90th percentile on the Uniform Bar Exam.29 Recent studies utilizing the Basic and Clinical Science Course (BCSC) Self-Assessment Program for the Ophthalmic Knowledge Assessment Program (OKAP) examination reveal substantial advancements in recent ChatGPT iterations, matching the accuracy rate of human respondents.30 Nevertheless, the empirical examination of AI performance growth in GPT models, particularly in non-board style ophthalmology clinical cases, remains an area warranting further exploration. The strength include GPT-4.0, have shown substantial improvements in accuracy, contextual understanding, and topic consistency, making them valuable tools in medical education and diagnostic reasoning. The limitations, including the applicability of GPT models in non-board style ophthalmology clinical cases, remain underexplored, necessitating further empirical evaluation and validation.8
Diagnosis Supporting Algorithms
González-Lõpez et al31 in their retrospective review utilized a dataset of 3,674 individuals from Moorfields Eye Hospital and focused on anterior uveitis. This study proposed a Bayesian Belief Network algorithm for the differential diagnosis of the anterior uveitis etiology according to clinical characteristics and incidence.31 A similar AI model was used by Jamilloux et al for a dataset of 877 patients from a single university hospital in Lyon with a uveitis diagnosis.32 Mutawa and Alzuwawi, et al33 applied a dataset of 61 online published cases from a centre in Kuwait and proposed a Multilayer Rule-based Expert System (long-term memory, short-term memory, inference engine, and extra module for explanations) that assisted in the diagnosis of systemic and non-systemic diseases based on patient history and examination. Tugal-Tutkun et al34 utilized a dataset of 867 patients from multiple centres in Turkey, Israel, the United Kingdom, Tunisia, and India and focused on Bechet disease uveitis diagnosis based only on ocular findings characteristics. Classification and Regression Tree Analysis (CART) was used and it was based on the recursive-partitioning analysis method, to prospective data collected, with the high-scoring tree re-evaluated for clinical relevance. The strength is that diagnosis-supporting algorithms like Bayesian Belief Networks and Multilayer Rule-based Expert Systems have demonstrated the ability to enhance differential diagnosis accuracy in complex uveitis cases by incorporating diverse datasets and clinical characteristics. The limitation is that these algorithms rely heavily on limited datasets and specific populations, potentially restricting their generalizability and applicability across diverse clinical settings.33
Finding Detection Algorithms
Li et al used AI for identifying anterior chamber inflammation with time-domain anterior segment Carl Zeiss OCT scans.35 Sharma et al36 and Baghdasaryan et al37 used Image IQ (Cleveland, OH, USA) combined with ImagePro Plus (Media Cybernetics, Rockville, MD, USA) platform in B-scans and 3D reconstructions in spectral-domain (SD) OCT and Image J Particle Analysis algorithm (http://imagej.net/Particle_Analysis) in single b-scans of swept-source (SS) OCT respectively, to compare manual and automated cell counts with the clinical grading with anterior segment OCT. Passaglia et al38 compared computer scores against humans in vitreous haze grading, in retinal color fundus photos. The reported metric was 0.61 kappa agreement between National Institute of Health and Miami specialist vitreous haze grade and automated grading. The grading model was performed using MATLAB platform with no publicly available software and data.38 The strength of AI-based detection algorithms have shown significant potential in automating anterior chamber inflammation and vitreous haze grading, offering consistency and reducing human error compared to manual grading. The limitation is that these algorithms often rely on proprietary platforms and lack publicly available software and datasets, limiting their validation, reproducibility, and widespread adoption in clinical practice.38
Screening Algorithms
Parra et al39 utilized a dataset of 160 color fundus retinal images for training and evaluating a screening model from a Paraguayan hospital. The pre-processing process consisted of resizing the image, and the DL model applied was the ResNet18, which was pre-trained on the ImageNet dataset. A softmax layer replaced the final layer to classify images as healthy or with evidence of ocular toxoplasmosis.38 Parra et al40 used a trust-based methodology to evaluate deep learning models for automatic diagnosis of ocular toxoplasmosis from fundus images. This study delved the performance of DL models and decision rules, which could be interpretable to elicit trust from the medical community. They evaluated three different architectures:
- A Convoluted Neural Network (CNN) model with a few convolutional layers initialized with random weights.
- A VGG16 model pretrained on the Imagenet dataset.41
- A Resnet18 model pretrained on the Imagenet dataset.42
The obtained results suggested that predictions made by the most accurate deep learning might be harder to trust by experienced physicians. These findings agree with the existing literature, as it is known that healthcare workers often find it challenging to trust complex machine-learning models.43 Zhang et al44 included a dataset of 2,000 slit lamp photos from 478 Fuchs (FUS) patients and 474 non-Fuchs patients from the Affiliated Hospital of Chongqing Medical University, China. The pre-processing consisted of resizing and augmentations processes (random cropping, rotation, brightness change, and flips) and 7 different deep convolutional neural networks (DCNNs) to detect FUS. They concluded that the performance of the DCNNs was better than that of general ophthalmologists and could be of value in the diagnosis of FUS.44 The strength is that deep learning models, such as ResNet18 and DCNNs, demonstrate superior accuracy compared to general ophthalmologists in diagnosing conditions like ocular toxoplasmosis and Fuchs’ uveitis syndrome (FUS), showcasing their potential to enhance diagnostic precision. The limitation is that despite their accuracy, complex machine learning models often lack interpretability, leading to challenges in gaining trust from experienced clinicians, which may hinder their widespread clinical adoption.39
Standardization of Uveitis Nomenclature (SUN) and Classification Systems
Artificial intelligence has also been used in uveitis to process clinical data not directly obtained from images. Uvemaster is a mobile phone application that uses clinical data to obtain the most probable diagnosis.45 Recently, the SUN-working group used AI to define the criteria of 25 of the most common clinical uveitis diagnoses.46 The first step was to collect cases of each uveitic entity, the final database included a total of 5766 cases, with about 100–200 cases per entity.47 Those cases that obtained a 75% or greater consensus among the expert group to belong to a specific entity were selected for training the machine learning tool. The research team combined a training set of multiple approaches on a subset of the cases with a validation set of the performance of the criteria determined on a second subset of the cases. Overall, the AI system categorized over 90% within uveitic class.48,49 In 2021, the American Journal of Ophthalmology published articles50–71 which focused on the standardisation of uveitis from SUN working group. The articles applied machine-learning techniques to develop a multi-class classification in an American patient cohort through multinomial logistic regression with lasso regularization.48 This was the first initiative to standardize uveitis diagnosis using machine learning from the SUN group. Demographic data and bias assessment were not available in the articles, and the applied models and data were also not publicly available. Standardization of Uveitis Nomenclature working group correlation of AC inflammation by Sharma et al36 and Baghdasaryan37 or MATLAB (MathWorks, Natick, MA, USA) in high speed (HS) OCT has been reported.72
Apart from clinical cells grading, Invernizzi et al73 correlated the aqueous signal intensity using the in-built software of the SS-OCT device, with the laser flare photometry measurements. It showed a positive correlation in active uveitis patients, but no correlation was found in the case of inactive uveitis patients.73 Nakayama et al13 in their review on AI in uveitis reported that the overall performance of AI models were poor, with limited datasets and a lack of validation studies and publicly available data and codes. They concluded that the AI held great promise to assist with the diagnosis and detection of ocular findings of uveitis, but further studies and large representative datasets were needed to guarantee generalizability and fairness. The strength is that the AI-driven initiatives by the SUN working group have significantly contributed to the standardization of uveitis diagnosis, achieving over 90% accuracy in categorizing cases within specific uveitic classes, showcasing AI’s potential to enhance clinical consistency and diagnostic precision. The limitation is that the lack of publicly available datasets and validation studies raises concerns about the generalizability and fairness of these AI models, limiting their applicability in diverse patient populations and real-world clinical settings.6
Application of Artificial Intelligence in Uveitis Management
Using anterior segment optical coherence tomography [AS-OCT], anterior segment cells are detected by the identification of hyperreflective spots.74–76 In a study by Agarwal et al, a good correlation for hyperreflective spot count between automated and manual methods was detected.72 There were no significant differences in mean values between the two methods except for grade 4. Similarly, an automated AI-based method to quantify inflammation in the AS was developed by Sorkhabi et al.74 They showed a significant correlation between clinical SUN grading and AI software-detected particle count and particle density. However, Ozer et al suggested that the iris pigment optical density measured at the pupillary margin of spectral-domain OCT could be a marker of Fuch’s heterochromic uveitis.75
According to the SUN working group, the quantification of vitreous inflammation is by the indirect ophthalmoscope. However, macular OCT scans help in measuring the vitreous inflammation. Terheyden et al have concluded that automated quantification of vitreous inflammation in uveitis is reliable.76 Three OCT scans will be sufficient to obtain a reliable automatic measurement of vitreous intensity. Passaglia et al have arrived at an algorithm where the vitreous haze grading provides a rapid, objective and reproducible method of grading vitreous inflammation.38 Keane et al generated an optical density ratio where the measurement of the vitreous signal intensity was then compared with that of the retinal pigment epithelium in OCT.77 These measurements showed a positive correlation with clinical vitreous haze scores. Choroidal vascularity index is a novel tool for assessing the clinical course in choroidal index. McKay et al identified and quantified inflammatory choriocapillaris lesions from automated swept-source OCT. They demonstrated a high degree of agreement with human graders in the determination of lesion area, spatial overlap, and reproducibility. Similarly, Chu et al detected choriocapillaris flow attenuation, with significantly larger areas of flow attenuation in patients with posterior uveitis than uveitis with no posterior involvement. Uveitic macula edema is a sequel of uveitis. Automated detection and quantification of macular edema caused by uveitis can be achieved, though intraocular inflammation could potentially obscure retinal structures. A deep learning method for localisation and quantification of fluid in the retina using OCT scans was done Schmidt et al and Moraes et al in neovascular age-related macular degeneration.78,79 Similar method can be used in quantification of fluid in uveitic macula edema. Ge L et al discussed the transformative role of Artificial Intelligence (AI) in enhancing systematic reviews (SRs) in health research. They highlighted how AI tools streamline processes like study screening, data extraction, and quality assessment, boosting efficiency and accuracy. Despite their promise, challenges such as bias, error propagation, and the need for human oversight remain. The authors emphasize that AI should complement human efforts rather than replace them, advocating for clear guidelines and further development to ensure reliability and rigor in SRs. The strength is that AI applications, such as automated methods using OCT for quantifying anterior segment and vitreous inflammation, demonstrate strong correlations with clinical grading systems, offering reproducible and objective assessments that enhance diagnostic precision. The limitation include despite these advancements, the reliance on automated algorithms faces challenges such as intraocular inflammation obscuring retinal structures and the potential for bias in AI systems, necessitating further validation across diverse clinical scenarios.80 Table 1 depicts the review of literature of application of artificial intelligence in uveitis.
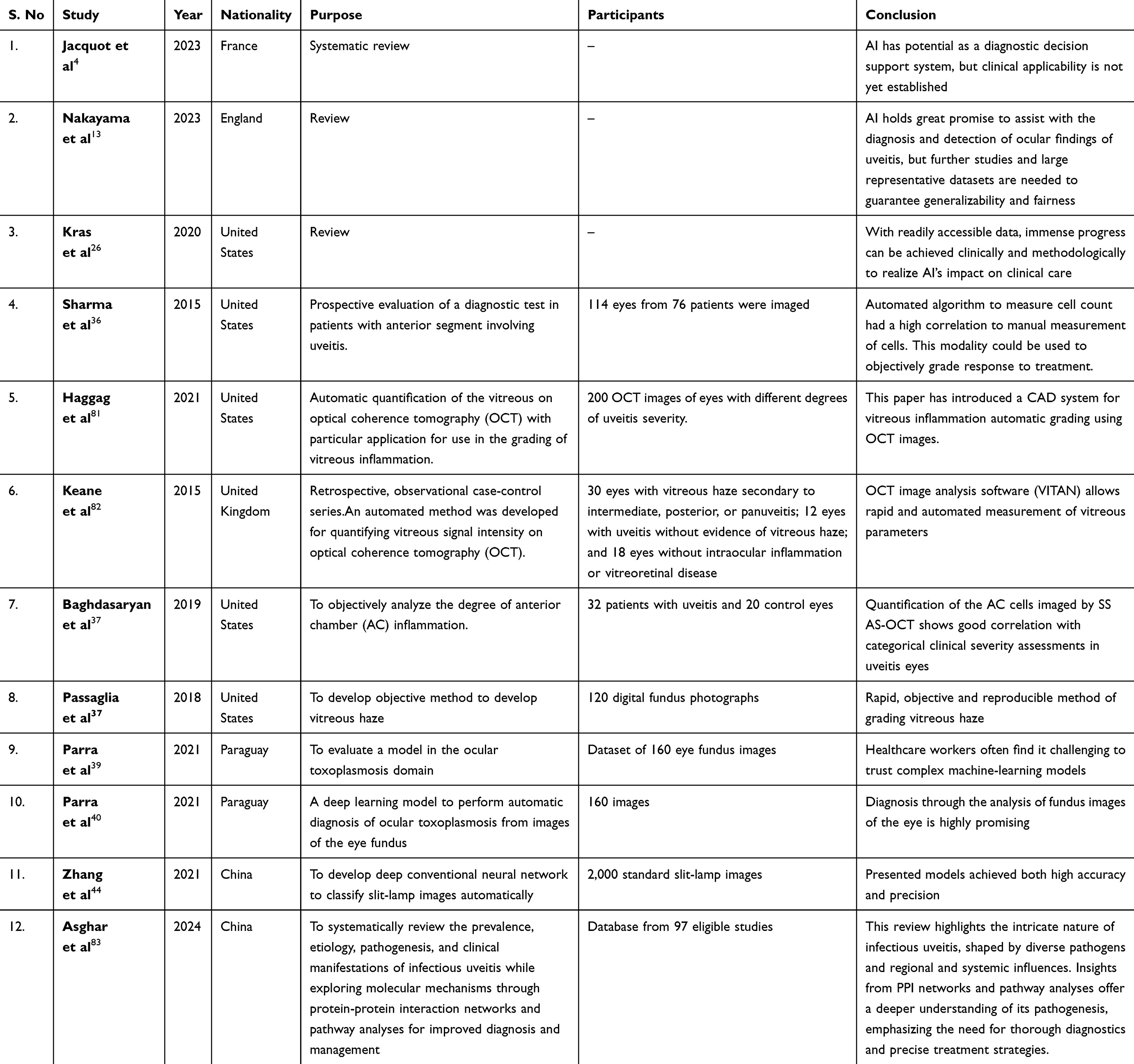 |
Table 1 Depicts the Review of Literature of Application of Artificial Intelligence in Uveitis |
Objective Grading of Inflammatory Indices
Inflammation in the anterior chamber (AC) can be objectively assessed and quantified with the help of AS-OCT along with automated AI algorithms. Clinically, the visibility of the AC cells depends on the cell size and cell type. Different cell types such as macrophages, lymphocytes, neutrophils, monocytes, and pigment granules may be present in the aqueous humor. Granulomatous inflammation is characterized by a predominance of macrophages, which are relatively larger in size and are readily visible clinically, whereas non-granulomatous cases predominantly have lymphocytes and plasma cells, which are smaller in size and consequently less visible on the slit-lamp. Using AS-OCT provides a more objective count of anterior chamber cellularity in inflammation, which not only correlates well with slit-lamp microscope grading but also detects cells missed on clinical examination.79 As there is poor inter-observer agreement when clinically grading intraocular inflammation,84 objective grading using AS-OCT may help produce standardized and reproducible quantification of inflammation. Good correlation has been established between clinical SUN grading of AC cells and objective grading of AC cells using OCT.74,81,84,85 Single-cell reflectivity on the OCT is also sufficiently sensitive to distinguish different cell types, making objective evaluation of inflammation even more useful towards diagnosing the underlying etiology.86 Counting of the AC cells on the OCT can be done either manually or using an automated cell counting program.74 Automated programs are faster and eliminate the risk of human errors in manual counting. There is good correlation between automated and manual methods of counting.82 Automated methods are also more sensitive than manual counting in higher grades of uveitis.85 Clinical grading of AC inflammation is challenging in cases with corneal edema such as endophthalmitis, corneal infections and post-operative uveitis. Objective grading using AS-OCT has been successfully used in such cases.85 The use of artificial intelligence (AI) takes objective evaluation of AC cells one step further. AI-based software has been used for automated segmentation of the anterior chamber and particle detection on AS-OCT scans.48 It relies on deep learning segmentation algorithms to accurately segment the AC in the scans, and a separate deep learning particle detection algorithm to count the number of hyperreflective spots. AI-based analysis has been found to be comparable, reproducible and independent of operator experience, thereby presenting clear advantages against SUN clinical grading.48
For evaluation of vitreous inflammation, clinical examination via indirect ophthalmoscopy and SUN grading of vitreous haze are the current gold standard. Although grading of vitreous haze is largely subjective, it can be evaluated objectively by measuring the vitreous signal intensity on macular OCT scans.87 Keane et al measured the vitreous signal intensity on OCT and compared it with the signal intensity of the retinal pigment epithelium, providing a VIT/RPE relative intensity ratio, which was significantly higher in uveitic eyes with known vitreous haze than in uveitic eyes without vitreous haze or healthy control eyes.87 The VIT/RPE relative intensity ratio showed significant, positive correlation with vitreous haze scores (r = 0.566) and good intergrader reproducibility (95% limit of agreement). An automated image-processing algorithm has been developed which objectively grades vitreous haze.87 The algorithm was compared against clinician’s vitreous haze grading and exact agreement between the algorithm and expert clinicians’ grades had a kappa value of 0.61. An AI-based computer-aided diagnostic (CAD) system has been developed by Haggag S. et al for grading of vitreous inflammation from macular OCT scans.86 The CAD system uses U-net convoluted neural networks for accurate segmentation of the OCT scans and machine learning classifiers to grade the vitreous inflammation. Their model has achieved an accuracy level of 86%, limited by the very high similarity in the vitreous appearance in different grades of inflammation.48,82 The strengths include that AI-based methods, such as automated segmentation and particle detection on AS-OCT and macular OCT, offer reproducible and operator-independent grading of inflammatory indices, improving objectivity and standardization in inflammation assessment. The limitation is that despite advancements, AI tools are constrained by challenges such as variability in inflammatory presentations, reliance on high-quality imaging datasets, and limited sensitivity in distinguishing subtle differences in inflammation grades.
Challenges and Opportunities for Artificial Intelligence in Uveitis
The field of AI is nascent and has multiple limitations on the following pointers. [a] The quality of the generated dataset in relation to the normative data applied to heterogeneous population is marked by high degree of variance. In particular, the data quality is subject to variance due to image specifications in addition to the atypicality of the clinical findings and the wide spectrum of the disease process per se. [b] The complex machine learning models lack transparency in making meaningful decision making process. The scientific rationale behind treatment recommendations based on the data at hand in the absence of missing links in the dataset needs an elegant scrutiny. [c] Currently there is a huge lacunae on the regulatory and ethical considerations on the validation, deployment and monitoring of the AI-based recommendations in uveitis to ensure data privacy and patient safety. [d] The patient demographics, disease prevalence and treatment practice pattern influence the ability to generalize the AI-based algorithms in real-time practice. The algorithmic errors due to biases involved in the training of the datasets can influence the output recommendations. In the absence of validation by diverse datasets, the fairness of AI generated data is questionable.
Incorporating Artificial Intelligence in Clinical Practice for Uveitis Management
While AI-driven advancements such as automated grading systems, diagnostic algorithms, and inflammatory index quantification tools demonstrate significant potential, their clinical utility hinges on seamless integration into everyday practice. For instance, AI-based grading of anterior chamber and vitreous inflammation could be integrated into electronic health records (EHR) systems, providing clinicians with real-time, objective data to guide treatment decisions. Furthermore, predictive algorithms for disease progression could enable proactive interventions tailored to individual patients, aligning with the principles of precision medicine. However, successful translation into practice requires addressing critical challenges. User-friendly interfaces and clinician training programs are essential to enhance adoption rates and build confidence in AI tools. Additionally, rigorous validation studies across diverse populations and clinical settings are imperative to ensure reliability, equity, and generalizability. Finally, interdisciplinary collaboration between AI developers, ophthalmologists, and healthcare policymakers is crucial to create ethical and regulatory frameworks, ensuring safe and effective deployment in patient care. By focusing on these pathways, AI technologies in uveitis management can move from research settings to becoming indispensable tools that enhance diagnostic accuracy, optimize therapeutic outcomes, and ultimately improve the quality of life for patients.
Future Directions
The researchers in artificial intelligence in uveitis hold promise in the following domains:
[a] The advancements in AI algorithms using convoluted neural networks and recurrent neural networks help in enhancing robustness and accuracy of AI models in uveitis. They help in integration of multimodal imaging, temporal dynamics of the data in addition to adapting to evolving disease patterns. [b] The collaborative efforts among academic institutions, industry partners are crucial to generate uveitis datasets on a large scale. This shall help in benchmarking the AI algorithms and cross-validate it before ready for clinical use in diverse setting. [c] The novel proteomic and genomic data can be integrated into AI-driven uveitis research. This shall enable the clinician to fathom novel pathophysiology and uniqueness in response to treatment. This shall guide in making precision molecular medicine a possibility using sequencing technologies and omics profiling to elucidate genetic variants, biomarkers and novel therapeutic targets in uveitis. [d] The remote assessment of disease activity and response to treatment, which is dynamic in nature, is feasible with telemedicine platforms and wearable devices. This AI-based telemedicine systems help to analyze on a real-time basis the visual acuity measurements, scoring of symptoms, quality of life indices and adherence to treatment as well. Focused treatment interventions can be done based on it to correct the healthcare disparities.
Conclusion
The integration of artificial intelligence (AI) into the field of uveitis management marks a significant milestone in modern ophthalmology, with the potential to redefine clinical practices by enhancing diagnostic precision, optimizing therapeutic strategies, and improving patient outcomes. By leveraging advanced AI algorithms, clinicians can detect subtle patterns, predict disease progression, and personalize treatment plans, paving the way for more effective and efficient care. Addressing the multifaceted challenges in uveitis requires a robust framework of interdisciplinary collaboration, global data-sharing initiatives, and strict adherence to ethical principles to ensure equity, transparency, and accountability in AI applications. Moreover, the evolving capabilities of AI offer promising opportunities to integrate precision medicine into routine clinical care, empowering clinicians to tailor interventions to individual patient profiles. This transformative approach not only elevates the standard of care but also fosters a proactive healthcare system that anticipates and mitigates potential complications. As AI technology continues to evolve, its successful implementation in uveitis care heralds a new era of innovation, collaboration, and hope for the global patient community, underscoring the limitless potential of AI to revolutionize healthcare and improve lives.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No external support, either public or private, was received for the conduct of this study.
Disclosure
The authors declare that they have no competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Krishnan G, Singh S, Pathania M, et al. Artificial intelligence in clinical medicine: catalyzing a sustainable global healthcare paradigm. Front Artif Intell. 2023;6:1227091. doi:10.3389/frai.2023.1227091
2. Li Z, Wang L, Wu X, et al. Artificial intelligence in ophthalmology: the path to the real-world clinic. Cell Rep Med. 2023;4(7):101095. doi:10.1016/j.xcrm.2023.101095
3. Lee RW, Nicholson LB, Sen HN, et al. Autoimmune and autoinflammatory mechanisms in uveitis. Semin Immunopathol. 2014;36(5):581–594. doi:10.1007/s00281-014-0433-9
4. Jacquot R, Sève P, Jackson TL, Wang T, Duclos A, Diagnosis S-SD. Classification, and Assessment of the Underlying Etiology of Uveitis by Artificial Intelligence: a Systematic Review. J Clin Med. 2023;12(11):3746. doi:10.3390/jcm12113746
5. Pinto-Coelho L. How Artificial Intelligence Is Shaping Medical Imaging Technology: a Survey of Innovations and Applications. Bioengineering. 2023;10(12):1435. doi:10.3390/bioengineering10121435
6. Jabs DA, Nussenblatt RB, Rosenbaum JT; Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data Results of the First International Workshop. Am J Ophthalmol. 2005;140(3):509–516. doi:10.1016/j.ajo.2005.03.057
7. Popescu Patoni SI, Muşat AAM, Patoni C, et al. Artificial intelligence in ophthalmology. Rom. J Ophthalmol. 2023;67(3):207–213. doi:10.22336/rjo.2023.37
8. Jiao C, Edupuganti NR, Patel PA, Bui T, Sheth VE. the Artificial Intelligence Performance Growth in Ophthalmic Knowledge. Cureus. 2023;15(9):e45700. doi:10.7759/cureus.45700
9. Liu X, Kale AU, Ometto G, et al. OCT Assisted Quantification of Vitreous Inflammation in Uveitis. Transl Vis Sci Technol. 2022;11(1):3. doi:10.1167/tvst.11.1.3
10. Iqbal J, Cortés Jaimes DC, Makineni P, et al. Reimagining Healthcare: unleashing the Power of Artificial Intelligence in Medicine. Cureus. 2023;15(9):e44658. doi:10.7759/cureus.44658
11. Soenksen LR, Ma Y, Zeng C, et al. Integrated multimodal artificial intelligence framework for healthcare applications. NPJ Digit Med. 2022;5(1):149. doi:10.1038/s41746-022-00689-4
12. Yelne S, Chaudhary M, Dod K, Sayyad A, Sharma R. Harnessing the Power of AI: a Comprehensive Review of Its Impact and Challenges in Nursing Science and Healthcare. Cureus. 2023;15(11):e49252. doi:10.7759/cureus.49252
13. Nakayama LF, Ribeiro LZ, Dychiao RG, et al. Artificial intelligence in uveitis: a comprehensive review. Surv Ophthalmol. 2023;68(4):669–677. doi:10.1016/j.survophthal.2023.02.007
14. Turing AM. I.—computing machinery and intelligence. Mind. 1950;LIX(236):433–460. doi:10.1093/mind/lix.236.433
15. Muthukrishnan N, Maleki F, Ovens K, Reinhold C, Forghani B, Forghani R. Brief history of artificial intelligence. Neuroimaging Clin N Am. 2020;30(4):393–399. doi:10.1016/j.nic.2020.07.004
16. Esteva A, Robicquet A, Ramsundar B, et al. A guide to deep learning in healthcare. Nat Med. 2019;25(1):24–29. doi:10.1038/s41591-
17. Ting DSW, Cheung CY, Lim G, et al. Development and Validation of a Deep Learning System for Diabetic Retinopathy and Related Eye Diseases Using Retinal Images From Multiethnic Populations With Diabetes. JAMA. 2017;318(22):2211–2223. doi:10.1001/jama.2017.18152
18. Obermeyer Z, Emanuel EJ. Predicting the Future - Big Data Machine Learning, and Clinical Medicine. N Engl J Med. 2016;375(13):1216–1219. doi:10.1056/NEJMp1606181
19. Kras A, Celi LA, Miller JB. Accelerating ophthalmic artificial intelligence research: the role of an open access data repository. Curr Opin Ophthalmol. 2020;31(5):337–350. doi:10.1097/ICU.0000000000000678
20. Grzybowski A, Brona P, Lim G, et al. Artificial intelligence for diabetic retinopathy screening: a review. Eye. 2020;34(3):451–460. doi:10.1038/s41433-019-0566-0
21. Abellanas M, Elena MJ, Keane PA, Balaskas K, Grewal DS, Carreño E. Artificial Intelligence and Imaging Processing in Optical Coherence Tomography and Digital Images in Uveitis. Ocul Immunol Inflamm. 2022;30(3):675–681. doi:10.1080/09273948.2022.2054433
22. Liu X, Faes L, Kale AU, et al. A comparison of deep learning performance against health-care professionals in detecting diseases from medical imaging: a systematic review and meta-analysis. Lancet Dig Health. 2019;1(6):e271–97. doi:10.1016/S2589-7500(19)30123-2
23. Abràmoff MD, Lavin PT, Birch M, Shah N, Folk JC . Pivotal trial of an autonomous AI-based diagnostic system for detection of diabetic retinopathy in primary care offices. npj Digital Medicine. 2018;1:
24. Sallam M. ChatGPT Utility in Healthcare Education, Research, and Practice: systematic Review on the Promising Perspectives and Valid Concerns. Healthcare. 2023;11(6):887. doi:10.3390/healthcare11060887
25. Yang LWY, Ng WY, Foo LL, et al. Deep learning-based natural language processing in ophthalmology: applications, challenges and future directions. Curr Opin Ophthalmol. 2021;32(5):397–405. doi:10.1097/ICU.0000000000000789
26. GPT-4; 2023. Availabe from: https://openai.com/research/gpt-4.
27. Kung TH, Cheatham M, Medenilla A, et al. Performance of ChatGPT on USMLE: potential for AI-assisted medical education using large language models. PLOS Digit Health. 2023;2(2):e0000198. doi:10.1371/journal.pdig.0000198
28. Mihalache A, Popovic MM, Muni RH. Performance of an Artificial Intelligence Chatbot in Ophthalmic Knowledge Assessment. JAMA Ophthalmol. 2023;141(6):589–597. doi:10.1001/jamaophthalmol.2023.1144
29. GPT-4 technical report. OpenAI OpenAI. arXiv. 2023.
30. Cai LZ, Shaheen A, Jin A, et al. Performance of Generative Large Language Models on Ophthalmology Board-Style Questions. Am. J Ophthalmol. 2023;254:141–149. doi:10.1016/j.ajo.2023.05.024
31. González-López JJ, García-Aparicio ÁM, Sánchez-Ponce D, et al. Development and validation of a Bayesian network for the differential diagnosis of anterior uveitis. Eye. 2016;30(6):865–872. doi:10.1038/eye.2016.64
32. Jamilloux Y, Romain-Scelle N, Rabilloud M, et al. Development and validation of a Bayesian network for supporting the etiological diagnosis of uveitis. J Clin Med Res. 2021;10(15). doi:10.3390/jcm10153398
33. Mutawa AM, Alzuwawi MA. Multilayered rule-based expert system for diagnosing uveitis. Artif Intell Med. 2019;99:101691. doi:10.1016/j.artmed.2019.06.007
34. Tugal-Tutkun I, Onal S, Stanford M, et al. An algorithm for the diagnosis of behçet disease uveitis in adults. Ocul Immunol Inflamm. 2021;29(6):1154–1163. doi:10.1080/09273948.2020.1736310
35. Li Y, Lowder C, Zhang X, Huang D. Anterior chamber cell grading by optical coherence tomography. Invest Ophthalmol Vis Sci. 2013;54(1):258–265. doi:10.1167/iovs.12-10477
36. Sharma S, Lowder CY, Vasanji A, Baynes K, Kaiser PK, Srivastava SK. Automated analysis of anterior chamber inflammation by spectral-domain optical coherence tomography. Ophthalmology. 2015;122(7):1464–1470. doi:10.1016/j.ophtha.2015.02.032
37. Baghdasaryan E, Tepelus TC, Marion KM, et al. Analysis of ocular inflammation in anterior chamber-involving uveitis using swept-source anterior segment OCT. Int Ophthalmol. 2019;39(8):1793–1801. doi:10.1007/s10792-
38. Passaglia CL, Arvaneh T, Greenberg E, Richards D, Madow B. Automated method of grading vitreous haze in patients with uveitis for clinical trials. Transl Vis Sci Technol. 2018;7(2):10. doi:10.1167/tvst.7.2.10
39. Parra R, Ojeda V, Vázquez Noguera JL, et al. Automatic Diagnosis of Ocular Toxoplasmosis from Fundus Images with Residual Neural Networks. Stud Health Technol Inform. 2021;281:173–177. PMID: 34042728. doi:10.3233/SHTI210143
40. Parra R, Ojeda V, Vázquez Noguera JL, et al. A trust-based methodology to evaluate deep learning models for automatic diagnosis of ocular toxoplasmosis from fundus images. Diagnostics. 2021;11(11). doi:10.3390/diagnostics11111951
41. Simonyan K, Zisserman A. Very Deep Convolutional Networks for Large-Scale Image Recognition. arXiv. 2014;
42. He K, Zhang X, Ren S, Sun J Deep Residual Learning for Image Recognition. In
43. Stiglic G, Kocbek P, Fijacko N, et al. Interpretability of machine learning based prediction models in healthcare. Wiley Interdiscip Rev Data Min Knowl Discov. 2020;10:e1379.
44. Zhang W, Chen Z, Zhang H, et al. Detection of Fuchs’ uveitis syndrome from slit-lamp images using deep convolutional neural networks in a Chinese population. Front Cell Dev Biol. 2021;9. doi:10.3389/fcell.2021.684522
45. Gegundez-Fernandez JA, Fernandez-Vigo JI, Diaz-Valle D, et al. Uvemaster: a mobile app-based decision support system for the differential diagnosis of uveitis. Invest Ophthalmol Vis Sci. 2017;58(10):3931–3939. doi:10.1167/iovs.17-21493
46. Trusko B, Thorne J, Jabs D, et al. The standardization of uveitis nomenclature (SUN) project. Development of a clinical evidence base utilizing informatics tools and techniques. Methods Inf Med. 2013;52(3):259–65,S1–6. doi:10.3414/ME12-01-0063
47. Jabs DA, Dick A, Doucette JT, et al. Interobserver agreement among uveitis experts on uveitic diagnoses: the standardization of uveitis nomenclature experience. Am J Ophthalmol. 2018;186:19–24. doi:10.1016/j.ajo.2017.10.028
48. Van Gelder RN, Sen HN, Tufail A, Lee AY. Here comes the SUN (Part 2): standardization of uveitis nomenclature for disease classification criteria. Am J Ophthalmol. 2021;228:A2–A6. doi:10.1016/j.ajo.2021.05.006
49. Standardization of Uveitis Nomenclature Working G. Development of classification criteria for the uveitides. Am J Ophthalmol. 2021;228:96–105. doi:10.1016/j.ajo.2021.03.061
50. Standardization of Uveitis Nomenclature (SUN) Working Group. Classification criteria for acute posterior multifocal placoid pigment epitheliopathy. Am J Ophthalmol. 2021;228:174–181. doi:10.1016/j.ajo.2021.03.056
51. Standardization of Uveitis Nomenclature (SUN) Working Group. Classification criteria for Behçet disease uveitis. Am J Ophthalmol. 2021;228:80–88. doi:10.1016/j.ajo.2021.03.058
52. Standardization of Uveitis Nomenclature (SUN) Working Group. Classification criteria for birdshot chorioretinitis. Am J Ophthalmol. 2021;228:65–71. doi:10.1016/j.ajo.2021.03.059
53. Standardization of Uveitis Nomenclature (SUN) Working Group. Classification criteria for Cytomegalovirus anterior uveitis. Am J Ophthalmol. 2021;228:89–95. doi:10.1016/j.ajo.2021.03.060
54. Standardization of Uveitis Nomenclature (SUN) Working Group. Classification criteria for Fuchs uveitis syndrome. Am J Ophthalmol. 2021;228:262–267. doi:10.1016/j.ajo.2021.03.052
55. Standardization of Uveitis Nomenclature (SUN) Working Group. Classification criteria for herpes simplex virus anterior uveitis. Am J Ophthalmol. 2021;228:231–236. doi:10.1016/j.ajo.2021.03.053
56. Standardization of Uveitis Nomenclature (SUN) Working Group. Classification criteria for intermediate uveitis, non-pars planitis type. Am J Ophthalmol. 2021;228:159–164. doi:10.1016/j.ajo.2021.03.054
57. Standardization of Uveitis Nomenclature (SUN) Working Group. Classification criteria for juvenile idiopathic arthritis-associated chronic anterior uveitis. Am J Ophthalmol. 2021;228:192–197. doi:10.1016/j.ajo.2021.03.055
58. Standardization of Uveitis Nomenclature (SUN) Working Group. Classification criteria for multifocal choroiditis with panuveitis. Am J Ophthalmol. 2021;228:152–158. doi:10.1016/j.ajo.2021.03.043
59. Standardization of Uveitis Nomenclature (SUN) Working Group. Classification criteria for multiple evanescent white dot syndrome. Am J Ophthalmol. 2021;228:198–204. doi:10.1016/j.ajo.2021.03.050
60. Standardization of Uveitis Nomenclature (SUN) Working Group. Classification criteria for multiple sclerosis-associated intermediate uveitis. Am J Ophthalmol. 2021;228:72–79. doi:10.1016/j.ajo.2021.03.044
61. Standardization of Uveitis Nomenclature (SUN) Working Group. Classification criteria for pars planitis. Am J Ophthalmol. 2021;228:268–274. doi:10.1016/j.ajo.2021.03.045
62. Standardization of Uveitis Nomenclature (SUN) Working GroupClassification criteria for punctate inner choroiditis. Am J Ophthalmol. 2021;228:275–280. doi:10.1016/j.ajo.2021.03.046
63. Standardization of Uveitis Nomenclature (SUN) Working GroupClassification criteria for sarcoidosis-associated uveitis. Am J Ophthalmol. 2021;228:220–230. doi:10.1016/j.ajo.2021.03.047
64. Standardization of Uveitis Nomenclature (SUN) Working GroupClassification criteria for serpiginous choroiditis. Am J Ophthalmol. 2021;228:126–133. doi:10.1016/j.ajo.2021.03.038
65. Standardization of Uveitis Nomenclature (SUN) Working GroupClassification criteria for spondyloarthritis/HLA-B27-associated anterior uveitis. Am J Ophthalmol. 2021;228:117–125. doi:10.1016/j.ajo.2021.03.049
66. Standardization of Uveitis Nomenclature (SUN) Working GroupClassification criteria for sympathetic ophthalmia. Am J Ophthalmol. 2021;228:212–219. doi:10.1016/j.ajo.2021.03.048
67. Standardization of Uveitis Nomenclature (SUN) Working GroupClassification criteria for syphilitic uveitis. Am J Ophthalmol. 2021;228:182–191. doi:10.1016/j.ajo.2021.03.039
68. Standardization of Uveitis Nomenclature (SUN) Working GroupClassification criteria for tubercular uveitis. Am J Ophthalmol. 2021;228:142–151. doi:10.1016/j.ajo.2021.03.040
69. Standardization of Uveitis Nomenclature (SUN) Working GroupClassification criteria for tubulointerstitial nephritis with uveitis syndrome. Am J Ophthalmol. 2021;228:255–261. doi:10.1016/j.ajo.2021.03.041
70. Standardization of Uveitis Nomenclature (SUN) Working GroupClassification criteria for varicella zoster virus anterior uveitis. Am J Ophthalmol. 2021;228:165–173. doi:10.1016/j.ajo.2021.03.037
71. Standardization of Uveitis Nomenclature (SUN) Working GroupClassification criteria for Vogt-Koyanagi-Harada disease. Am J Ophthalmol. 2021;228:205–211. doi:10.1016/j.ajo.2021.03.036
72. Agarwal A, Ashok Kumar D, Jacob S, et al. High-speed optical coherence tomography for imaging anterior chamber inflammatory reaction in uveitis: clinical correlation and grading. Am J Ophthalmol. 2009;147(3):413–6e3. doi:10.1016/j.ajo.2008.09.024
73. Invernizzi A, Marchi S, Aldigeri R, et al. Objective quantification of anterior chamber inflammation: measuring cells and flare by anterior segment optical coherence tomography. Ophthalmology. 2017;124(11):1670–1677. doi:10.1016/j.Ophtha.2017.05.013
74. Sorkhabi MA, Potapenko IO, Ilginis T, Alberti M, Cabrerizo J. Assessment of Anterior Uveitis through Anterior-Segment Optical Coherence Tomography and Artificial Intelligence-Based Image Analyses. Transl Vis Sci Technol. 2022;11:7. doi:10.1167/tvst.11.4.7
75. Ozer MD, Kebapci F, Batur M, Seven E, Tekin S. In vivo analysis and comparison of anterior segment structures of both eyes in unilateral Fuchs’ uveitis syndrome. Graefes Arch Clin Exp Ophthalmol Albrecht Von Graefes Arch Klin Exp Ophthalmol. 2019;257:1489–1498. doi:10.1007/s00417-019-04351-w
76. Terheyden JH, Ometto G, Montesano G, et al. Automated quantification of posterior vitreous inflammation: optical coherence tomography scan number requirements. Sci Rep. 2021;11:3271. doi:10.1038/s41598-021-82786-026
77. Keane PA, Karampelas M, Sim DA, et al. Objective measurement of vitreous inflammation using optical coherence tomography. Ophthalmology. 2014;121:1706–1714. doi:10.1016/j.ophtha.2014.03.006
78. Moraes G, Fu DJ, Wilson M, et al. Quantitative Analysis of OCT for Neovascular Age-Related Macular Degeneration Using Deep Learning. Ophthalmology. 2020;128:693–705.
79. Schmidt-Erfurth U, Vogl W-D, Jampol LM, Bogunović H. Application of Automated Quantification of Fluid Volumes to Anti–VEGF Therapy of Neovascular Age-Related Macular Degeneration. Ophthalmology.
80. Ge L, Agrawal R, Singer M, et al. Leveraging artificial intelligence to enhance systematic reviews in health research: advanced tools and challenges. Syst Rev. 2024;13(1):269. doi:10.1186/s13643-024-02682-2
81. Rose-Nussbaumer J, Li Y, Lin P, et al. Aqueous cell differentiation in anterior uveitis using Fourier-domain optical coherence tomography. Invest Ophthalmol Vis Sci. 2015;56(3):1430–1436. doi:10.1167/IOVS.14-15118
82. Development of Classification Criteria for the Uveitides. Am J Ophthalmol. 2021;228:96–105. doi:10.1016/J.AJO.2021.03.061
83. Asghar MA, Tang S, Wong LP, Yang P, Zhao Q. “Infectious uveitis: a comprehensive systematic review of emerging trends and molecular pathogenesis using network analysis”. J Ophthalmic Inflamm Infect. 2024;14(1):60. doi:10.1186/s12348-024-00444-8
84. Kempen JH, Ganesh SK, Sangwan VS, Rathinam SR. Interobserver agreement in grading activity and site of inflammation in eyes of patients with uveitis. Am J Ophthalmol. 2008;146(6). doi:10.1016/J.AJO.2008.06.004
85. Igbre AO, Rico MC, Garg SJ. High-speed optical coherence tomography as a reliable adjuvant tool to grade ocular anterior chamber inflammation. Retina. 2014;34(3):504–508. doi:10.1097/IAE.0B013E31829F73BD
86. Haggag S, Khalifa F, Abdeltawab H, et al. An Automated CAD System for Accurate Grading of Uveitis Using Optical Coherence Tomography Images. Sensors (Basel). 2021;21(16). doi:10.3390/S21165457
87. Keane PA, Balaskas K, Sim DA, et al. Automated analysis of vitreous inflammation using spectral-domain optical coherence tomography. Transl Vis Sci Technol. 2015;4:4.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.