")
Back to Journals » Journal of Inflammation Research » Volume 17
Assessing Functional Similarity of Biosimilar ABP 654 and Ustekinumab in Samples from Patients with Crohn’s Disease
Authors Foltz IN, Gaida K, Wong HY , Ng M , Busch M , Liu JL
Received 22 June 2024
Accepted for publication 5 November 2024
Published 7 December 2024 Volume 2024:17 Pages 10627—10640
DOI https://doi.org/10.2147/JIR.S478529
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Ian N Foltz,1 Kevin Gaida,2 Helen Y Wong,1 Michael Ng,1 Marijana Busch,1 Jennifer L Liu3
1Amgen Research, Department of Therapeutic Discovery, Amgen Inc., Burnaby, BC, V5A1V7, Canada; 2Research and Development, Amgen Inc., Thousand Oaks, CA, 91320, USA; 3Biosimilar Process Development, Amgen Inc., Thousand Oaks, CA, 91320, USA
Correspondence: Jennifer L Liu, Biosimilar Process Development, Amgen, Inc., One Amgen Center Dr, Thousand Oaks, CA, 91320, USA, Tel +1-805-447-2246, Email [email protected]
Purpose: ABP 654 is the first FDA-approved interchangeable biosimilar for ustekinumab reference product (RP). To support the totality of evidence (TOE), in vitro pharmacology studies were conducted in peripheral blood mononuclear cells (PBMCs) from healthy human donors and Crohn’s disease (CD) patients to evaluate IL-23 and IL-12 inhibition by ABP 654 and ustekinumab RP relevant to the mechanism of action of chronic inflammation.
Methods: ABP 654 and ustekinumab RP were assessed using inhibition of IL-23 and IL-12-mediated IFN-γ release, signal transducer and activator of transcription (STAT)3 and STAT4 phosphorylation, and IL-17 release. IFN-γ levels were determined using homogenous time-resolved fluorescence (HTRF). STAT3 and STAT4 phosphorylation were measured by flow cytometry. IL-17 was measured using a Cisbio IL-17 detection kit. IC50 values were calculated to assess the relative potency of ABP 654 and ustekinumab RP.
Results: ABP 654 and ustekinumab RP demonstrated similar inhibition and relative potency of IL-23 and IL-12-mediated IFN-γ release, and no difference in inhibition of IL-23/IL-12-mediated STAT3/STAT4 phosphorylation in healthy donor PBMCs, as evidenced by the overlapping standard deviation (SD). In CD PBMCs, ABP 654 and ustekinumab RP also showed no difference in IC50 values for inhibition of IL-23/IL-12-mediated STAT3/STAT4 phosphorylation. ABP 654 and ustekinumab RP showed no difference in IC50 values for IL-23-induced IL-17 release, in either healthy (ABP 654, 458.7± 110.8 pM; ustekinumab (EU), 514.6± 48.7 pM) or CD (ABP 654, 260.8± 88.5 pM; ustekinumab (EU), 256.9± 96.8 pM) donor cells with overlapping SD.
Conclusion: These studies demonstrated similar inhibition of IL-23 and IL-12 function by ABP 654 and ustekinumab RP in both healthy and CD PBMCs. Overall, these assays support the conclusion that ABP 654 and ustekinumab RP are functionally similar, thereby contributing to the TOE supporting a demonstration of biosimilarity.
Keywords: ABP 654, biosimilar pharmaceuticals, Crohn’s disease, interleukin-12, interleukin-23, interchangeable
Introduction
ABP 654 is the first FDA-approved biosimilar for ustekinumab reference product (RP) with interchangeable designation.1 ABP 654, similar to the ustekinumab RP, is approved to manage and treat moderate-to-severe plaque psoriasis in adults and pediatric patients, active psoriatic arthritis in adults and pediatric patients, moderate-to-severe active Crohn’s disease (CD) in adults, and moderate-to-severe active ulcerative colitis in adults.2,3 Both ABP 654 and ustekinumab RP are recombinant humanized immunoglobulin isotype class G subclass 1 kappa (IgG1κ) monoclonal antibodies, which bind with high specificity and affinity to the p40 protein subunit shared by both heterodimeric interleukin (IL)-23, composed of IL-12p40 and IL-23p19, and IL-12 cytokines, composed of IL-12p40 and IL-12p35.4 This binding prevents IL-23 and IL-12-mediated signaling and downstream biological functions by disrupting the interaction of these cytokines with a shared cell-surface receptor, IL-12Rβ1 (Interleukin 12 Receptor Subunit Beta 1).5
IL-23 and IL-12 are closely related and play important roles in inflammatory and immune responses. Binding of IL-23 and IL-12 to their receptors triggers the activation of the Janus kinase 2 (JAK2) and tyrosine kinase 2 (TYK2), leading to the phosphorylation of signal transducer and activator of transcription (STAT) 3 and STAT4 for IL-23 and IL-12 signaling respectively. The phosphorylated STAT3 and/or STAT4 proteins then translocate to the nucleus where they induce distinct transcriptional activities that include expression of the proinflammatory cytokine interferon gamma (IFN-γ) and other cytokines that promote the immune response against intracellular pathogens.6 IL-23 also acts through T cells, especially T helper 17 cells (Th17) and promotes the release of IL-17, which plays a key role in the pathophysiology of chronic inflammatory diseases.5,7 The dysregulation of the IL-23 and IL-12 signaling can be associated with excessive inflammation and autoimmune reactions. Binding of ustekinumab to the p40 subunit of IL-23 and IL-12 inhibits the interaction of these cytokines with their receptors, preventing the phosphorylation of downstream STAT signaling proteins and expression of IFN-γ.5
While ustekinumab RP and other biologics have transformed the treatment of chronic inflammatory disorders, their high costs have increased healthcare expenditure and been an impediment to their widespread use.8–10 A biosimilar is a biological product developed to resemble and perform with no clinically meaningful difference to the RP. The US Food and Drug Administration (FDA), European Medicines Agency, and other global health regulatory agencies have created rigorous scientific development and approval processes for biosimilars, ensuring biosimilars are highly similar to an approved RP. In the United States (US), the FDA is allowed to approve a biosimilar as an interchangeable biosimilar if it meets additional requirements outlined by law. In the US, savings to the healthcare system have been estimated to be $54 billion over a 10-year period.8
The scientific justification for use of biosimilars is being built on the totality of evidence (TOE), with a stepwise approach starting with extensive structural and functional characterization of the proposed biosimilar which serves as the foundation of biosimilar development program.11 While ustekinumab RP is manufactured in a murine myeloma (Sp2/0) cell line, and ABP 654 is manufactured in a glyco-engineered Chinese hamster ovary cell line, the amino acid sequence of ABP 654 is identical to that of the ustekinumab RP and the totality of the data so far demonstrates that ABP 654 is highly similar to ustekinumab RP.12 Comprehensive analytical characterization has shown that ABP 654 is similar to ustekinumab RP in terms of structure, function, purity, and potency.12 Additionally, no clinically meaningful difference was observed for pharmacokinetics (PK), safety, and immunogenicity in healthy volunteers.13 Currently, a clinical study (NCT04607980) comparing the efficacy, safety, and immunogenicity of ABP 654 and ustekinumab RP in patients with moderate-to-severe plaque psoriasis is ongoing. These studies were intended to further assess the functional similarity between ABP 654 and ustekinumab RP relevant to the mode of action (MOA) in both healthy and a disease model to support a demonstration of biosimilarity and generate additional substantive scientific justification for the extrapolation of ABP 654 to additional approved indications of ustekinumab RP. Specifically, in vitro pharmacology studies were conducted in peripheral blood mononuclear cells (PBMCs) from healthy human donors and/or patients with CD to compare the effect of ABP 654 and ustekinumab RP on IL-23-induced IFN-γ release, IL-12-induced IFN-γ release, IL-23-induced STAT3 signaling, IL-12-induced STAT4 signaling, and IL-23-induced IL-17 release.
Materials and Methods
All work was conducted following the associated good scientific practices according to Amgen Standard Operating Procedures. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Test Material
ABP 654 was prepared in the same dosage forms, presentations, and strengths as the RP. The RPs were separately sourced from the US and the European Union (EU) to allow for direct comparisons between ABP 654 and each of the RPs and between the two independently licensed RPs.
Peripheral Blood Mononuclear Cells (PBMCs)
PBMCs were isolated from donor cells. Cells from two healthy donors were purchased from Discovery Life Sciences, Huntsville, AL, and cells from two healthy donors were purchased from Astarte Biologics, Bothell, WA. Cells from four CD donors were purchased from Precision for Medicine, Carlsbad, CA. Due to limited amounts of cells not every donor was used for every assay. Vials of PBMCs were thawed in a water bath at 37°C in 5% CO2 for each experiment.
Detection of Homogenous Time Resolved Fluorescence
Detection of the cytokine of interest released was performed using a Europium Cryptate labelled antibody (donor molecule) and an allophycocyanin labelled antibody (acceptor molecule) that specifically targets and together binds to the cytokine in a sandwich assay format. The proximity of the antibodies triggers a fluorescence resonance energy transfer from the donor towards the acceptor molecule and causes the acceptor molecule to fluoresce at a specific wavelength of 665 nm. The signal intensity is captured with the Envision 2103 plate reader. The ratio of the acceptor (665 nm) and donor (615 nm) emission signals with the following formula:

Inhibition of IL-23-Induced IFN-γ Release/IL-12-Induced IFN-γ Release
PBMCs were isolated using Lymphoprep® (STEMCELL® Technologies, Vancouver, Canada) and frozen in 80% heat-inactivated fetal bovine serum (FBS) and 20% dimethyl sulfoxide (DMSO). Thawed PBMCs were cultured in medium consisting of RPMI 1640, supplemented with 10% FBS, 1X GlutaMAX, 1X non-essential amino acids (NEAA), 1 mm sodium pyruvate, 10 nM N-(2-hydroxyethyl)piperazine-N′-(2-ethanesulfonic acid) (HEPES), and 0.05 mm 2-mercaptoethanol. PBMCs were activated with plate-coated anti-cluster of differentiation 3 (anti-CD3; 43.5 nM in DPBS) and suspension anti-CD28 (22.7 nM) for 3 days at 37°C, 5% CO2. Cells were either combined with IL-18 (final concentration 2.0 nM) and IL-23 (final concentration of 0.088 nM) or IL-12 (final concentration 1.0 nM), pre-incubated with test materials with decreasing concentrations (for IL-23, 600 nM to 7.7 pM; for IL-12, 200 nM to 2.6 pM) and incubated at 37°C, 5% CO2 for 3 days. Cells were spun down at 400 x g for 5 minutes and assay was measured using an HTRF human IFN-γ detection kit (Cisbio) as above.
The potency curves were generated with each data point as the mean of triplicate wells and the error bars representing the standard deviation and curves were generated using variable slope (4-parameter) curve fitting. All curves were constrained at the top and bottom asymptotes as well as by the hillslope to match the values for the plate control (on the same plate). For each constrained curve, the graphing software determined the IC50 value. The goodness-of-fit of the curve fit modeling was determined by the coefficient of determination. The percent (%) relative potency was calculated using the following formula:

In all assays, ABP 654 reference standard was prepared as the plate control and was used for relative potency calculations.
Inhibition of IL-23-Mediated STAT3 Phosphorylation/IL-12-Mediated STAT4 Phosphorylation
PBMCs were grown in medium consisting of Roswell Park Memorial Institute 1640 media (RPMI 1640) supplemented with 10% heat-inactivated (HI) FBS (1% HI FBS for IL-23 and IL-12 stimulations), 1X Penicillin-Streptomycin-Glutamine (PSG), and 25 mm HEPES. To generate activated T cells, the PBMC suspension (5 mL, 5×106 cells/mL) was incubated with 94 mL of prewarmed medium and 1 mL of phytohemagglutinin (PHA) for 5 days. Test materials were pre-incubated with either IL-23 or IL-12 for 30 minutes at room temperature, combined with cells and incubated at 37°C, 5% CO2 in a humidified incubator for 30 minutes, and then fixed/permeabilized. The final concentration was 10 ng/mL for IL-23 and 5 ng/mL for IL-12. The final concentration range for ABP 654 and ustekinumab RP (US and EU) was 100 nM to 5 pM in 3-fold dilutions. Alexa Fluor 647-conjugated anti-pY705 STAT3 antibody was used to detect phosphorylated STAT3, while phycoerythrin conjugated anti-pY693 STAT4 antibody was used to detect phosphorylated STAT4.
Analysis was performed on a BD LSRFortessa flow cytometer using BD FACSDiva™ software (version 9.0). The percent of cells expressing phosphorylated STAT3 (or STAT4) when treated with IL-23 (or IL-12) and ABP 654 or ustekinumab (US or EU) were normalized to the percent of cells expressing phosphorylated STAT3 (or STAT4) when treated with IL-23 (or IL-12) alone (control) and expressed as a percent of control (POC). Graphs were generated by plotting the concentration of ABP 654 and ustekinumab against the POC values for phosphorylated STAT levels. A curve was fit to the data points using the non-linear regression log (antagonist) versus response-variable slope (4-parameter) equation in GraphPad Prism using default settings to determine the half-maximal inhibitory concentration (IC50). Curves for the CD donors as well as ustekinumab RP Lot 3 in the healthy donor as part of the IL-23-mediated STAT3 phosphorylation assay were constrained at the bottom asymptotes. The goodness-of-fit of the curve fit modeling was automatically calculated by the software and determined by the r2 value.
Inhibition of IL-23-Mediated IL-17 Release
IL-23 was prepared at an optimized concentration (EC90) for each PBMC donor. PBMCs were cultured in X–VIVO® 15 serum-free hematopoietic cell medium supplemented with L-glutamine and transferrin. ABP 654 or ustekinumab dilution series were generated to give an 8-fold titration prepared in X–VIVO® 15 media (ranging from 600 nM to 36 pM final concentration). Equal volumes of IL-23 and antibody were combined and incubated at room temperature for at least 1 hour. PBMCs were thawed, washed 3 times, and incubated in DPBS containing 20% FBS at room temperature for 30 minutes. Cells were washed 3 times with X–VIVO® 15 media and counted. Cells were diluted 1:1 with CytoStim™ (at final dilution of 1:125) and seeded at optimal density for each PBMC donor. The IL-23 and antibody mixture was added to the same plate, and the cells were incubated for 3 days at 37°C, 5% CO2. Cells were spun down at 400 x g for 5 minutes and IL-17 was measured using the Cisbio IL-17 detection kit and read on the HTRF-compatible EnVision plate reader. HTRF ratio was then converted to IL-17 concentration using an IL-17 standard curve. A new standard curve was prepared for each replicate assay and the IL-17 concentration was calculated from the IL-17 standard curve prepared in the same assay. A standard titration was prepared to give a 2.1-fold titration (ranging from 3428 pM to 40 pM) and plotted by IL-17 concentration against HTRF ratio using GraphPad Prism’s simple linear regression analysis. Validity of the standard curve was determined by the goodness-of-fit r-squared value being greater or equal to 0.95. Concentration of IL-17 from HTRF was calculated with the following formula:

The potency curves were plotted by ABP 654 or ustekinumab (EU) concentration against IL-17 release with each data point as the mean of triplicate wells and the error bars representing the standard deviation. Curves were generated using GraphPad Prism software’s variable slope (4-parameter) curve fitting, where the four parameters are IC50, hillslope, bottom, and top plateau of the curve. Validity of dose-response curves was determined by goodness-of-fit r-square value being greater or equal to 0.95. The IC50 values for the dose-response of each test sample were calculated and compared. No outlier exclusion methods were used as there were no significant outliers present.
Results
The in vitro pharmacological activity of ABP 654 was compared to that of ustekinumab (US) and ustekinumab (EU) in biological functional similarity assessments. A subset of the assays evaluated as well as previously published analytical and functional studies,12,13 demonstrate similarity of ustekinumab RP sourced from the US and EU.
ABP 654 and Ustekinumab RP Exhibit Similar Inhibition of IL-23-Induced IFN-γ Release in Healthy Donor Cells
Inhibition of IL-23-induced IFN-γ release was assessed across three runs of one lot each of ABP 654, ustekinumab (US), and ustekinumab (EU) in PBMCs from a leukopak of a healthy donor. ABP 654, ustekinumab (US), and ustekinumab (EU) showed similar blocking of IL-23-mediated IFN-γ release in the presence of IL-18 in PBMCs from healthy donor (Figure 1A). Percent (%) relative potency values were similar between the pairs of antibodies tested, ranging between 80% and 120% of the plate control (Figure 1B). In head-to-head comparisons calculated based on triplicate measurements, the average % relative potency values when compared to each other were 102% for ABP 654 and 100% for ustekinumab (EU), 89.5% for ABP 654 and 90.5% for ustekinumab (US), and 89.2% for ustekinumab (EU) and 98.8% for ustekinumab (US). ABP 654 inhibited IL-23-induced IFN-γ release with a mean IC50 of 2.11 pM ± 2.03 pM; ustekinumab (EU) inhibited IL-23-induced IFN-γ release with a mean IC50 of 2.68 pM ± 2.98 pM; and ustekinumab (US) inhibited IL-23-induced IFN-γ release with a mean IC50 of 2.07 pM ± 1.59 pM. The overlapping standard deviations from the IC50 values indicate no difference among the products (Table 1).
 |
Table 1 IC50 Values from ABP 654, Ustekinumab (EU), and Ustekinumab (US) Inhibition of IL-23-Induced IFN-γ Release Assay Using Cells from Healthy Donor |
 |
Figure 1 Similarity in inhibition of IL-23-induced IFN-γ release of ABP 654 versus ustekinumab (EU), ABP 654 versus ustekinumab (US), and ustekinumab (EU) versus ustekinumab (US) in healthy donor cells shown by (A) dose-dependent concentration-response curves depicted as the mean of 3 replicates ± standard deviation; and (B) relative potency of binding. Each bar of the graph represents the mean of 3 replicate experiments ± standard deviation and the test samples were run in pairs. Abbreviations: EU, European Union; IL, interleukin; IFN-γ, interferon gamma; US, United States. |
ABP 654 and Ustekinumab RP Exhibit Similar Inhibition of IL-12-Induced IFN-γ Release in Healthy Donor Cells
Inhibition of IL-12-induced IFN-γ release was assessed across at least three runs of one lot each of ABP 654, ustekinumab (US), and ustekinumab (EU) in PBMCs from a healthy donor leukopak. ABP 654, ustekinumab (US), and ustekinumab (EU) showed similar blocking of IL-12-mediated IFN-γ release in PBMCs from healthy donor (Figure 2A). Percent (%) relative potency values were similar between the pairs of antibodies tested, ranging between 80% and 120% of the plate control (Figure 2B). In head-to-head comparisons, calculated based on triplicate measurements, the average % relative potency values when compared to each other were 100.4% for ABP 654 and 89.7% for ustekinumab (EU), 92.7% for ABP 654 and 89.4% for ustekinumab (US), and 109.2% for ustekinumab (EU) and 107.8% for ustekinumab (US). ABP 654 inhibited IL-12-induced IFN-γ release with a mean IC50 of 1.04 pM ± 0.65 pM; ustekinumab (EU) inhibited IL-12-induced IFN-γ release with a mean IC50 of 1.09 pM ± 0.50 pM; and ustekinumab (US) inhibited IL-12-induced IFN-γ release with a mean IC50 of 1.10 pM ± 0.75 pM. The overlapping standard deviations from the IC50 values indicate no difference among the products (Table 2).
 |
Table 2 IC50 Values from ABP 654, Ustekinumab (EU), and Ustekinumab (US) Inhibition of IL-12-Induced IFN-γ Release Assay Using Cells from Healthy Donor |
 |
Figure 2 Similarity in inhibition of IL-12-induced IFN-γ release of ABP 654 versus ustekinumab (EU), ABP 654 versus ustekinumab (US), and ustekinumab (EU) versus ustekinumab (US) in healthy donor cells shown by (A) dose-dependent concentration-response curves depicted as the mean of 3 replicates ± standard deviation; and (B) relative potency of binding, each bar of the graph represents the mean of 3 replicate experiments ± standard deviation and the test samples were run in pairs. Abbreviations: EU, European Union; IL, interleukin; IFN-γ, interferon gamma; US, United States. |
ABP 654 and Ustekinumab RP Exhibit Similar Inhibition of IL-23-Mediated STAT3 Phosphorylation in Healthy and CD Donor Cells
ABP 654, ustekinumab (US), and ustekinumab (EU) were tested for their ability to inhibit IL-23-induced STAT3 phosphorylation in cells from a healthy human donor. Three different lots of each test article were evaluated. ABP 654 and ustekinumab RP showed similar inhibition of IL-23-induced STAT3 with overlapping dose-response curves in PBMCs from a healthy donor (Figure 3A). ABP 654 inhibited STAT3 phosphorylation in activated T cells with a mean IC50 of 3.4 nM ± 0.6 nM; ustekinumab (US) inhibited STAT3 phosphorylation with a mean IC50 of 3.9 nM ± 0.3 nM; and ustekinumab (EU) inhibited STAT4 phosphorylation with a mean IC50 of 3.5 nM ± 0.3 nM. The overlapping standard deviations from the relative potency and IC50 values indicate that there was no difference among the products (Figure 3B, Supplemental Table 1).
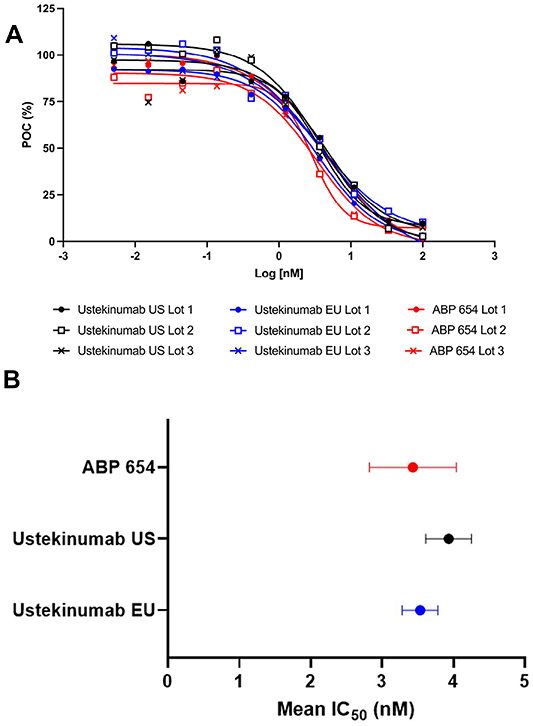 |
Figure 3 Similarity in inhibition of IL-23-mediated STAT3 phosphorylation of three lots each of ustekinumab (US), ustekinumab (EU), and ABP 654 in healthy donor cells shown by (A) overlapping dose-response curves for all 9 lots expressed as POC; and (B) mean IC50 values for 3 lots of ABP 654, ustekinumab US, or ustekinumab EU, error bars represent the standard deviation. Abbreviations: EU, European Union; IC50, half maximal inhibitory concentration; IL, interleukin; POC, percent of control; STAT3, signal transducer and activator of transcription 3; US, United States. |
For the CD donor cells, ABP 654 and ustekinumab (EU) were compared for their ability to inhibit IL-23-induced STAT3. Ustekinumab (US) was not tested as it was found similar to ustekinumab (EU) in its ability to inhibit IL-23-induced STAT3 phosphorylation in cells from healthy human donors. Assay results in PBMCs from three different CD donor cells showed that ABP 654 and ustekinumab (EU) exhibited similar inhibition of IL-23-induced STAT3 phosphorylation (Figure 4A). In the PBMCs from three CD donors, ABP 654 and ustekinumab (EU) showed similar IC50 for the inhibition of IL-23-induced STAT3 phosphorylation in activated T cells (Figure 4B, Table 3).
 |
Table 3 ABP 654 and Ustekinumab (EU) IC50 Values for Inhibition of IL-23-Induced STAT3 Phosphorylation in CD Donor Cells |
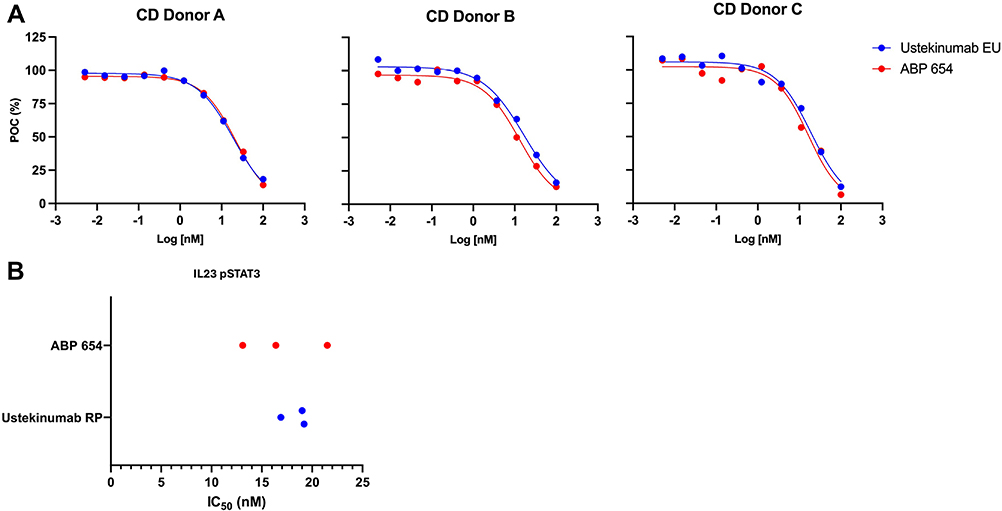 |
Figure 4 Similarity in inhibition of IL-23-mediated STAT3 phosphorylation using ustekinumab (EU) and ABP 654 in cells from three different CD donors shown by (A) overlapping dose-response curves; and (B) IC50 values. Abbreviations: CD, Crohn’s disease; EU, European Union; IC50, half-maximal inhibitory concentration; IL, interleukin; POC, percent of control; RP, reference product; STAT3, signal transducer and activator of transcription 3. |
ABP 654 and Ustekinumab RP Exhibit Similar Inhibition of IL-12-Mediated STAT4 Phosphorylation in Healthy and CD Donor Cells
ABP 654, ustekinumab (US), and ustekinumab (EU) were tested for their ability to inhibit IL-12-induced STAT4 phosphorylation in cells from a healthy human donor. Three different lots of each test article were evaluated. ABP 654, ustekinumab (US), and ustekinumab (EU) showed similar inhibition of IL-12-induced STAT4 with overlapping dose-response curves in PBMCs from healthy donor cells (Figure 5A). ABP 654 inhibited STAT4 phosphorylation in activated T cells with a mean IC50 of 1.5 nM ± 0.5 nM; ustekinumab (US) inhibited STAT4 phosphorylation with a mean IC50 of 2.2 nM ± 0.5 nM; and ustekinumab (EU) inhibited STAT4 phosphorylation with a mean IC50 of 2 nM ± 0.4 nM. The overlapping standard deviations from the relative potency and IC50 values indicate no difference among the products (Figure 5B, Supplemental Table 2).
 |
Figure 5 Similarity in inhibition of IL-12-mediated STAT4 phosphorylation of three lots each of ustekinumab (US), ustekinumab (EU), and ABP 654 in healthy donor cells shown by (A) overlapping dose-response curves for all 9 lots expressed as POC; and (B) mean IC50 values for 3 lots of ABP 654, ustekinumab US, or ustekinumab EU, error bars represent the standard deviation. Abbreviations: EU, European Union; IC50, half-maximal inhibitory concentration; IL, interleukin; POC, percent of control; STAT4, signal transducer and activator of transcription 4; US, United States. |
For the CD donor cells, ABP 654 and ustekinumab (EU) were compared for their ability to inhibit IL-12-induced STAT4. Ustekinumab (US) was not tested as it was found similar to ustekinumab (EU) in its ability to inhibit IL-12-induced STAT4 phosphorylation in cells from healthy human donors. Assay results in PBMCs from three different CD donor cells showed that ABP 654 and ustekinumab (EU) exhibited similar inhibition of IL-12-induced STAT4 phosphorylation (Figure 6A). In the PBMCs from three CD donors, ABP 654 and ustekinumab (EU) showed similar IC50 for the inhibition of IL-12-induced STAT4 phosphorylation in activated T cells (Figure 6B; Table 4).
 |
Table 4 ABP 654 and Ustekinumab (EU) IC50 Values for Inhibition of IL-12-Induced STAT4 Phosphorylation in CD Donor Cells |
 |
Figure 6 Similarity in inhibition of IL-12-mediated STAT4 phosphorylation using ustekinumab (EU) and ABP 654 in cells from three different CD donors showing (A) overlapping dose-response curves; and (B) IC50 values. Abbreviations: CD, Crohn’s Disease; EU, European Union; IC50, half-maximal inhibitory concentration; IL, interleukin; POC, percent of control; RP, reference product; STAT4, signal transducer and activator of transcription 4. |
ABP 654 and Ustekinumab RP Exhibit Similar Inhibition of IL-23-Induced IL-17 Release in Healthy and CD Donor Cells
Three independent experiments were run for each of the two healthy donors and for three CD donors to determine the similarity of ABP 654 and ustekinumab RP in the neutralization of IL-23-induced IL-17 release assay. ABP 654 and ustekinumab (EU) showed similar inhibition of IL-23-induced IL-17 release in PBMCs from healthy (Figure 7A) and CD (Figure 7B) donors’ cells. In the two healthy donors, ABP 654 inhibited IL-23-induced IL-17 release with a mean IC50 of 458.7 pM ± 110.8 pM; and ustekinumab (EU) inhibited IL-23-induced IL-17 release with a mean IC50 of 514.6 pM ± 48.7 pM. In the three CD donors, ABP 654 inhibited IL-23-induced IL-17 release with a mean IC50 of 260.8 pM ± 88.5 pM; and ustekinumab (EU) inhibited IL-23-induced IL-17 release with a mean IC50 of 256.9 pM ± 96.8 pM. The IC50 values were determined and considered similar for both healthy donor cells and CD donor cells. The overlapping standard deviations from the IC50 values indicate no difference among the products (Figure 7, Table 5).
 |
Table 5 IC50 Values from ABP 654 and Ustekinumab (EU) Inhibition of IL-23-Induced IL-17 Release Assay Using Cells from Healthy and CD Donors |
 |
Figure 7 Similarity in inhibition of IL-23-induced IL-17 release in cells from 3 independent experiments shown by mean IC50 values with error bars representing the standard deviation in (A) healthy donors; and (B) CD donors. Abbreviations: CD, Crohn’s disease; EU, European Union; IC50, half-maximal inhibitory concentration; IL, interleukin. |
Discussion
The comprehensive non-clinical strategy of in vitro pharmacologic assessments presented here demonstrates similarity of functional activity of ABP 654 as compared to RP in blocking various IL-12 and IL-23 activities, important in mediating their anti-inflammatory actions.5 These results complement prior comprehensive analytical testing results that demonstrated similarity with regard to physicochemical and biological properties, including structure, function, purity, and potency,12 with additional in vitro pharmacological comparisons of IL-23-induced STAT3 signaling, IL-12-induced STAT4 signaling, IL-23-induced IFN-γ release, IL-12-induced IFN-γ release, and IL-23-induced IL-17 release of ABP 654 as compared to RP in cells from both healthy volunteers and patients with CD. The results provide additional scientific support for extrapolation based on the functional similarity of ABP 654 and ustekinumab RP in the primary MOA underlying all indications for which ustekinumab has been approved.
Ustekinumab is approved to manage and treat the inflammatory diseases of plaque psoriasis, psoriatic arthritis, CD, and ulcerative colitis.2,3 IL-12 and IL-23 both participate in immune responses that are characterized as pro-inflammatory. Dysregulation of IL-12 and IL-23 pathways is known to contribute to the chronic inflammation mediated by T-helper type 1 (Th1) and Th17 immune responses associated with many inflammatory diseases.5 The MOA of ustekinumab is to bind to the p40 subunit of IL-23 and IL-12, blocking the cytokines’ interaction with their receptors and preventing the phosphorylation of STAT-signaling proteins and expression of the proinflammatory cytokines, IFN-γ and IL-17.5 To demonstrate that ABP 654 is able to neutralize IL-23- and IL-12-mediated signaling activity similarly to the RP, ABP 654 and ustekinumab RP were tested in multiple different side-by-side experiments.
IL-23 signaling is mediated through intracellular phosphorylation of STAT3 proteins. Similar inhibition was observed with ABP 654 and ustekinumab RP of IL-23-mediated STAT3 phosphorylation in healthy and CD donor cells, with overlapping standard deviations for all the lots tested. Since ABP 654 and ustekinumab RP bind to the common p40 subunit of IL-12 and IL-23, inhibition to IL-12-mediated signaling was also examined. ABP 654 and ustekinumab RP exhibit similar inhibition of IL-12-mediated STAT4 phosphorylation in healthy and CD donor cells with overlapping standard deviation for all the lots tested.
Both IL-23 and IL-12 play crucial roles in activating cells to elicit IFN-γ release.14,15 Examining the neutralization of IL-23-induced IFN-γ release, the % relative potency for ABP 654 as compared with ustekinumab RP was similar in each of the pairwise comparison assays performed. Similar to IL-23, IL-12 is also known to increase IFN-γ release, and, in our assays measuring the neutralization of IL-12-induced IFN-γ release, ABP 654 exhibited similar % relative potency as compared with ustekinumab RP in each of the pairwise comparison assays performed.
IL-23 also has the ability to stimulate IL-17 production and expression, and IL-17-producing T cell numbers in gut mucosa have been found to be higher in patients with CD than in healthy controls, and some of these cells also secrete IFN-γ.16 ABP 654 was determined to be functionally similar to ustekinumab RP based on results that demonstrate similarity of blocking of IL-23-induced IL-17 release in PBMC from multiple healthy and CD donors.
ABP 654 has previously been shown to be identical to ustekinumab RP in amino acid sequence and chemical modifications. Size and charge variants for ABP 654 and ustekinumab RP were also considered similar, despite minor differences that were deemed not clinically meaningful. Initial comparative assessments of their anti-inflammatory action in human embryonic kidney (HEK) cells, including inhibition of IL-23-mediated signaling, inhibition of IL-12-mediated signaling, IL-23 receptor-ligand binding, and IL-12 receptor-ligand binding were also found to be similar.12 PK equivalency and no clinical meaningful differences in safety were demonstrated between ABP 654 and ustekinumab RP in healthy volunteers.13 These previously published analytical and functional studies,12 clinical PK studies,13 as well as functional studies as reported in this manuscript also established ustekinumab RP bridging between US- and EU-sourced products and support the use of ustekinumab sourced from either region in further studies.
Conclusions
In summary, these nonclinical pharmacology data support the conclusion that ABP 654 and ustekinumab RP exert similar anti-inflammatory actions in vitro in both healthy and CD donor cells. These results of functional similarity in addition to the previously reported evidence of their structural similarities, functional similarities in other in vitro and in vivo systems,12 as well as evidence of no clinically meaningful differences in PK, safety, and immunogenicity in healthy volunteers,13 and efficacy and safety in subjects with plaque psoriasis (manuscript in review),17,18 are key data that form the TOE for similarity. This work adds to the TOE supporting the conclusion of similarity and the scientific rationale for ABP 654 as an FDA-approved biosimilar to ustekinumab across all indications of chronic inflammation (plaque psoriasis, psoriatic arthritis, CD, ulcerative colitis) for which ustekinumab is approved. Approved biosimilars offer healthcare professionals and patients more choices for treatment, enabling access to more affordable treatment options for some patients.19
Ethics Approval and Informed Consent
All human specimens were collected via Amgen Human Tissue Science Center study specifications under site-specific Institutional Review Board or Ethics Board approval with appropriate informed consent in compliance with all applicable laws and regulations. In all cases, materials obtained were surplus to standard clinical practice and standards of care. Patient identity and Protected Health Information/identifying information were redacted from tissues and clinical data prior to submission to Amgen. Human tissue specimens were obtained from the following institutions: Precision for Medicine, Bethesda, MD, USA.
Acknowledgments
Medical writing assistance was provided by Jennifer L. Fogel, PhD (Amgen Inc.), under the direction of Sonya G. Lehto, PhD (Amgen Inc.). Editing support was provided by Innovation Communications Group, New York, NY (on behalf of Amgen Inc.).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
All studies in this manuscript were funded by Amgen, Inc.
Disclosure
INF, KG, HYW, MN, JL are employees and stockholders of Amgen, Inc. MB is a an employee of Amgen, Inc. The authors report no other conflicts of interest in this work.
References
1. US Food & Drug Administration. FDA approves interchangeable biosimilar for multiple inflammatory diseases. 2023. Available from: https://www.fda.gov/news-events/press-announcements/fda-approves-interchangeable-biosimilar-multiple-inflammatory-diseases.
2. STELARA® (ustekinumab) [Prescribing Information]. Horsham, PA: Janssen Pharmaceuticals; 2009.
3. WEZLANA™ (ustekinumab-auub) [Prescribing Information]. Thousand Oaks, CA: Amgen Inc.; 2023.
4. Floss DM, Moll JM, Scheller J. IL-12 and IL-23-close relatives with structural homologies but distinct immunological functions. Cells. 2020;9(10):2184. doi:10.3390/cells9102184
5. Benson JM, Peritt D, Scallon BJ, et al. Discovery and mechanism of ustekinumab: a human monoclonal antibody targeting interleukin-12 and interleukin-23 for treatment of immune-mediated disorders. MAbs. 2011;3(6):535–545. doi:10.4161/mabs.3.6.17815
6. Moschen AR, Tilg H, Raine T. IL-12, IL-23 and IL-17 in IBD: immunobiology and therapeutic targeting. Nat Rev Gastroenterol Hepatol. 2019;16(3):185–196. doi:10.1038/s41575-018-0084-8
7. Pastor-Fernández G, Mariblanca IR, Navarro MN. Decoding IL-23 signaling cascade for new therapeutic opportunities. Cells. 2020;9(9):2044. doi:10.3390/cells9092044
8. Mulcahy AW, Hlavka JP, Case SR. Biosimilar cost savings in the United States: initial experience and future potential. Rand Health Q. 2018;7(4):3.
9. Baumgart DC, Misery L, Naeyaert S, Taylor PC. Biological therapies in immune-mediated inflammatory diseases: can biosimilars reduce access inequities? Front Pharmacol. 2019;10:279. doi:10.3389/fphar.2019.00279
10. Kim H, Alten R, Avedano L, et al. The future of biosimilars: maximizing benefits across immune-mediated inflammatory diseases. Drugs. 2020;80(2):99–113. doi:10.1007/s40265-020-01256-5
11. US Department of Health and Human Services Food and Drug Administration. Scientific considerations in demonstrating biosimilarity to a reference product. Guidance for Industry. April 2015. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/scientific-considerations-demonstrating-biosimilarity-reference-product.
12. Cantin G, Liu Q, Shah B, et al. Analytical and functional similarity of the biosimilar candidate ABP 654 to Ustekinumab reference product. Drugs R D. 2023;23(4):421–438. doi:10.1007/s40268-023-00441-7
13. Chow V, Mytych DT, Das S, Franklin J. Pharmacokinetic similarity of ABP 654, an ustekinumab biosimilar candidate: results from a randomized, double-blind study in healthy subjects. Clin Pharmacol Drug Dev. 2023;12(9):863–873. doi:10.1002/cpdd.1301
14. van de Wetering D, de Paus RA, van Dissel JT, van de Vosse E. IL-23 modulates CD56+/CD3- NK cell and CD56+/CD3+ NK-like T cell function differentially from IL-12. Int Immunol. 2009;21(2):145–153. doi:10.1093/intimm/dxn132
15. Ullrich KA, Schulze LL, Paap EM, Müller TM, Neurath MF, Zundler S. Immunology of IL-12: an update on functional activities and implications for disease. EXCLI J. 2020;19:1563–1589. doi:10.17179/excli2020-3104
16. Annunziato F, Cosmi L, Santarlasci V, et al. Phenotypic and functional features of human Th17 cells. J Exp Med. 2007;204(8):1849–1861. doi:10.1084/jem.20070663
17. Blauvelt A, Papp K, Trivedi M, et al. Efficacy and safety of the biosimilar candidate ABP 654 in the treatment of moderate-to-severe plaque psoriasis: results from a phase 3, multicenter, randomized, double-blinded study. EADV. 2023.
18. Chow V, Mytych DT, Blauvelt A, et al. P1081 Pharmacokinetics and immunogenicity of the ustekinumab biosimilar candidate ABP 654 in patients with moderate-to-severe plaque psoriasis. J Crohn’s Colitis. 2024;18(Supplement_1):i1943. doi:10.1093/ecco-jcc/jjad212.1211
19. Sheridan M, Massich M, Ashourian N. Biosimilars: from Production to Patient. J Infus Nurs. 2024;47(1):19–29. PMID: 38211611; PMCID: PMC10786443. doi:10.1097/NAN.0000000000000528
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.