")
Back to Journals » Clinical Ophthalmology » Volume 18
Assessment of Corneal Cross-Linking Effect on Progressive Keratoconus by Using the ABCD Grading System
Authors Alzahrani M, Alammari O, Binyamin A, Alsulami R, Hawsawi R
Received 22 January 2024
Accepted for publication 27 June 2024
Published 22 August 2024 Volume 2024:18 Pages 2349—2355
DOI https://doi.org/10.2147/OPTH.S460464
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mazen Alzahrani,1 Omer Alammari,2 Abdulelah Binyamin,3 Raed Alsulami,1 Rawan Hawsawi2
1Department of Anterior Segment, Jeddah Eye Hospital, Jeddah, Saudi Arabia; 2Department of Anterior Segment, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia; 3Department of Ophthalmology, King Fahad Armed Forces Hospital, Jeddah, Saudi Arabia
Correspondence: Mazen Alzahrani, Email [email protected]
Purpose: The aim of this study was to assess changes in corneal parameters 6 months after corneal cross-linking for progressive keratoconus, using the ABCD system.
Patients and Methods: This retrospective study was conducted at the King Khaled Eye Specialist Hospital (Riyadh, Saudi Arabia) between January 1 and July 30, 2022. This study included 16 eyes of 16 patients with keratoconus who underwent corneal cross-linking at the same hospital and were at least 18 years old. At least one preoperative (T0) and one postoperative examination was performed for each patient. Six months after the procedure (T1), patients underwent corneal tomography. The parameters A, B, C, and D were also evaluated. Other parameters monitored included maximal keratometry (Kmax) (K1 and K2), Belin/Ambrósio Enhanced Ectasia Display, and index vertical asymmetry. The progression of ectasia was identified by a consistent change in at least two parameters: steepening of the anterior corneal surface or the posterior corneal surface, thinning or an increase in the rate at which the corneal thickness changed from the periphery to the thinnest point, where the magnitude of the change was greater than the normal noise of the testing system.
Results: Among the patients, 68.8% were men. The patients’ average age was 25.8± 5 years. Throughout the 6-month postoperative follow-up, parameters A, B, and C exhibited substantial changes (P = 0.000 for parameters A, B, and C). Parameter A increased 6 months after surgery, whereas parameters B and C decreased. Preoperatively and 6 months after surgery, Kmax, K1, and Belin/Ambrosio-enhanced ectasia demonstrated substantial differences. However, parameter D, K2, and the average pachymetric progression index did not change significantly.
Conclusion: Anterior and posterior corneal curvatures and corneal thickness profiles can be useful for monitoring the progression of keratoconus and the success of the corneal cross-linking operation.
Keywords: corneal cross-linking, keratoconus, ABCD grading system, topography
Introduction
Keratoconus (KC) is a chronic ectatic cornea disorder that worsens over time and causes scarring, steepening, and uneven corneal curvature, which may impair vision.1 KC is a noninflammatory condition that develops early in infancy, peaking in symptoms between the ages of 14 years and 18 years. Patients frequently report deteriorating bilateral vision over time caused by increased astigmatism and myopia.2
However, based on international research conducted over 48 years, the frequency in the United States (US) is estimated to be 54.5 (0.05%) per 100,000 people. More recently, multiple studies have shown a higher incidence rate of KC, particularly in the Middle East and Saudi Arabia,3,4 and that it is more advanced at the time of diagnosis than in other countries throughout the world with cooler temperatures and less exposure to ultraviolet (UV) radiation.5,6 These are well-known risk factors, along with eye rubbing and atopy; however, the underlying etiology is thought to be complex.6
Fleischer rings, and Vogt striae are early slit-lamp microscopic features of KC. Corneal tomography devices such as the Pentacam (Oculus), which is used to assess posterior corneal protrusion and atypical distributions of the central thickness map or peripheral cornea, is essential for diagnosis and disease monitoring.7 The Amsler–Krumeich grading system is among the first and most popular KC grading systems. It is used to grade, based on central keratometry, scarring, and central corneal thickness.7
The main drawbacks of the Amsler–Krumeich grading system are its restricted corneal coverage and its ability to evaluate only the anterior corneal surface, eliminating any posterior corneal abnormalities. Optical coherence tomography (OCT) scanners can provide limbus-to-limbus coverage and scan the entire anterior region and the posterior corneal surfaces. The Belin ABCD keratoconus staging approach was created to use the thinnest areas of the cornea to identify any manifestation within the anterior and posterior curves of the cornea. Compared with earlier methods, which are restricted to the anterior corneal surface, the ABCD approach can detect progressive illness much sooner.8
The ABCD grading system divides KC into five stages, based on structural and functional alterations, by using tomographic measures and visual acuity. It gathers information on A (anterior radius of curvature), B (posterior curvature), C (corneal thickness), and D (corrected distance and visual acuity [BCVA]) in the 3.0 mm zone centered on the thinnest part of the cornea.8 This study used the ABCD approach to evaluate postoperative changes in corneal parameters 6 months after cross-linking (CXL) for progressive KC. Conducting a study in Saudi Arabia to assess the effectiveness of CXL in progressive keratoconus by using the ABCD grading system can fill a gap and provide regionally specific data. By offering regional perspectives in how local patients would respond, it could contribute to the development of locally adapted treatment protocols and improve clinical outcomes in patients with keratoconus.
Materials and Methods
Study Design, Period, and Area
From January 1, 2022, to July 30, 2022, this retrospective study was carried out at the King Khaled Eye Specialist Hospital (Riyadh, Saudi Arabia). This study included 16 eyes from 16 patients with KC who were at least 18 years old and had undergone corneal CXL at the same facility.
Study Population and Inclusion Criteria
Our study included 16 patients with progressive KC, aged 18 years or older, who underwent CXL and had at least 6 months of follow-up between the study’s start date (January 1, 2022) and end date (July 30, 2022).
Exclusion Criteria
Patients under the age of 18 years with corneal pachymetry less than 400 m, a history of ocular trauma or surgery, corneal scarring, and corneal diseases other than KC were excluded from the study.
Study Process, Operation, and Follow-Up Details
The surgeon who performed the CXL procedure was a cornea fellow with high level of expertise and training in corneal procedures. A cornea fellow is a qualified ophthalmologist who has gone through focused training in corneal and external diseases, including procedures such as CXL. The patients were managed, based on the progression of ectasia, which was identified by a consistent change in at least two of the following parameters: steepening of the anterior corneal surface, steepening of the posterior corneal surface, and thinning or an increase in the rate at which the corneal thickness changed from the periphery to the thinnest point, where the magnitude of the change was greater than the normal noise of the testing system.
The Dresden (standard) protocol using the Avedro machine involved the application of a riboflavin solution, specifically Vibex (0.1% riboflavin-5-phosphate and 20% dextran T-500; Avedro), administered at intervals of 1–5 minutes for a total soak time of 30 minutes, or until riboflavin was visible in the anterior chamber. Following this, the cornea was exposed to ultraviolet A (UVA) radiation at a wavelength of 370 nm with a specific intensity of 3 mW/cm² for 30 minutes. This corneal CXL method ensures the riboflavin adequately permeates the corneal stroma, allowing the UVA light to activate the riboflavin and facilitate cross-linking within the corneal collagen fibers. The entire procedure ensures efficient strengthening of the corneal structure through this standardized approach. In addition, the Pentacam diagnostic device (Oculus) was utilized for anterior segment imaging and cornea analysis. The Pentacam device was operated by the same person for all 16 cases.
After the procedure, the cornea was cleaned with a balanced salt solution before a silicone hydrogel bandage contact lens was placed. Topical corticosteroids were administered postoperatively for 1–4 months, depending on the level of corneal haze. Each patient underwent at least one preoperative (T0) and postoperative examination. Six months after surgery (T1), the patient underwent scans. Patients underwent corneal tomography and slit-lamp examinations at the follow-up visit. In addition, visual acuity was examined before and after implementing the procedure. The quality of scans taken with the Pentacam device (Oculus) was assessed on a variety of aspects. First, we checked for good focusing and correct positioning with regard to the center of the cornea. We also checked Placido rings alignment with Scheimpflug image quality to confirm that the images were correctly captured. Furthermore, we checked the images for any artifacts or distortion, which may likely affect the accuracy of measurements. Scans that did not meet these criteria were repeated in order to ensure the collection of high-quality data for analysis.
Parameters Used
Parameters A, B, C, and D were examined during the postoperative follow-up. Maximal keratometry (Kmax), (K1 and K2), BADD, and visual acuity (IVA) were other tracked metrics.
Statistical Analysis
The entire dataset was entered into Microsoft Office Excel tables and analyzed using SPSS version 24. The Shapiro–Wilk’s test was used to determine normality. The paired sample t-test was used to compare two time points (T0 and T1) to examine the difference in corneal parameters before and after the corneal CXL procedure. Statistical significance was defined as a P value of 0.05 or less.
Ethical Approval
The King Khaled Eye Specialist Hospital Institutional Review Board permitted us to gather data and authorized this study (reference number RD/26001/IRB/0213-23). Informed consent was obtained from all participants involved in the study. The study was conducted in accordance with the ethical principles that have their origin in and comply with the Declaration of Helsinki.
Results
The study included 16 eyes of 16 participants, 68.8% of whom were men. The patients’ average age was 25.8± 5 years. Table 1 presents the results pertaining to parameters A, B, C, and D. Throughout the 6-month postoperative follow-up, parameters A, B, and C exhibited statistically significant changes (P ≤ 0.001 for parameters A, B, and C). Parameter A increased 6 months after surgery, whereas parameters B and C decreased. However, parameter D did not show a statistically significant change (P = 0.751).
 |
Table 1 ABC Grading Scale Before Corneal Cross-Linking and 6 Months Postoperatively, and the Paired Sample t-Test Comparison Between T0 and T1 |
The minimum preoperative values of parameters A, B, C, and D were 5.3, 3.8, 366.0, and 0.60, respectively. The minimum values 6 months postoperatively were 5.2, 3.7, 367, and 0.60, respectively.
Before the operation, the mean values and their corresponding 95% confidence intervals (CIs) of parameters A, B, C, and D were 6.4 (95% CI, 6.0–9.8), 4.7 (95% CI, 4.5–5.0), 439 (95% CI, 420–458), and 0.83 (95% CI, 0.77–0.88), respectively. The mean values and their corresponding 95% CIs for the same parameters 6 months postoperatively were 6.5 (95% CI, 6.1–6.9), 4.6 (95% CI, 4.4–4.9), 435 (95% CI, 414.3–457.2), and 0.83 (95% CI, 0.77–0.90), respectively (Tables 1 and 2).
 |
Table 2 Descriptive Data of the Parameters Preoperatively and 6 Months Postoperatively |
Table 3 displays the findings with reference to keratometric and tomographic indices values. Preoperatively and 6 months after surgery, the Kmax, K1, and Belin/Ambrosio enhanced ectasia total were each substantially different. The maximum values of these parameters preoperatively were 47.3, 38.4, and 4.8, respectively, and the mean of these values and their corresponding 95% CIs preoperatively were 59.6 (95% CI, 54.5–65.3), 48.5 (95% CI, 44.2–53), and 10.9 (95% CI, 8.7–13.1), respectively (Tables 2 and 3). The mean values and their corresponding 95% CIs 6 months postoperatively were 58.8 (95% CI, 54–63.5), 46.7 (95% CI, 43.6–49.7), and 11.5 (95% CI, 9.1–14.9), respectively (Table 2). However, K2 and the average pachymetric progression index did not change significantly. Figure 1 shows the relationships between all variables preoperatively and 6 months postoperatively.
 |
Table 3 The Preoperative and 6-Month Postoperative Values of the Keratometric and Tomographic Indices |
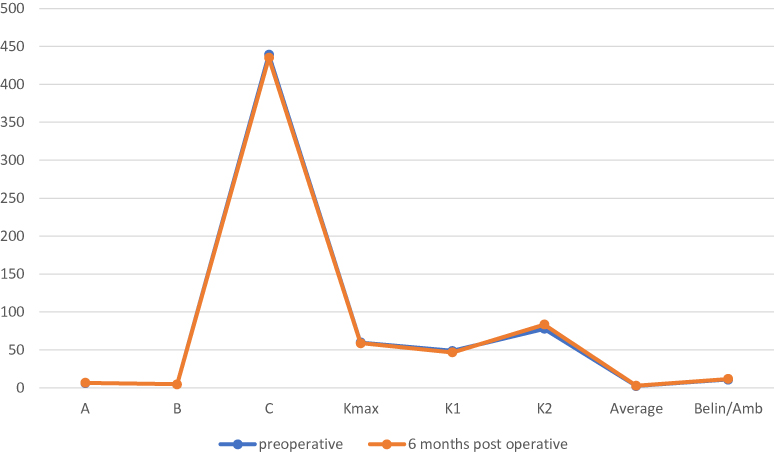 |
Figure 1 Different parameters preoperatively and 6 months postoperatively. |
Discussion
The Global Consensus on Keratoconus and Ectatic Diseases states that there is no precise definition of corneal ectasia progression.9 Several techniques have been discussed to assess corneal ectasia advancement or track CXL effectiveness. Although many more recent techniques use complicated keratometric indices to characterize progression, earlier systems relied solely on serial topographic analyses to describe progression.9–11 Kmax is the most commonly utilized metric for ectatic progression detection and monitoring, as well as for assessing the effectiveness of CXL. However, studies have revealed that Kmax does not accurately indicate the severity of ectasia, and ectatic progression can occur, even without a change in the Kmax.12
In our study, we found that throughout the 6-month postoperative follow-up, parameters A, B, and C exhibited statistically significant changes (P ≤ 0.001 for parameters A, B, and C). Parameter A increased 6 months after surgery, whereas parameters B and C decreased. However, parameter D did not have a statistically significant change (P = 0.751). This finding was different from the findings of a previous study by Saglik and Isik in 2019,13 in which they found that the average value for parameter A decreased by an average of 0.19 ± 0.56 (P = 0.014) and the average value for parameter C increased by average of 0.13± 0.34 (P = 0.004).13 This finding could be justified for different reasons, including the difference in the follow-up period, which was longer in the aforementioned study by Saglik and Isik study (12 months) than in our study in which the patients were followed-up for 6 months only. Other possible reasons include differences in patients’ baseline demographic characteristics, CXL protocols, and difference in baseline keratoconus severity.
In 2016, Belin and Duncan14 proposed a staging scheme that considered KC modifications and closely resembled the previously used Amsler–Krumeich classification system. By including information on the anterior and posterior corneal surfaces, corneal thickness in its final analysis, and KC classification, the ABCD grading system can reflect anatomical and functional corneal alterations.15
In this study, C, which measures thinnest location values, initially decreased after CXL. Over time, parameter A increased from the baseline value. According to Bardan et al, parameter C significantly increased (parameter C increased at all visits, compared with the baseline), but parameter A significantly decreased over the first post-CXL year.12
Six months after CXL, the current investigation revealed an opposite shift in parameter C, which stabilized and returned to the preoperative values. These findings are corroborated by earlier research examining corneal thickness following CXL; some of these investigations found that both parameters stabilized 6 months after treatment.16,17
Compared to the findings of our study, Considerable parameter A regression was found 1 year after CXL.12,13,18 Parameter B did not significantly change postoperatively, according to Bardan et al.12 Our study’s findings are different because parameter A showed a modest decline 6 months after surgery.12 Future research on the potential effects of various CXL techniques and riboflavin solutions on the ABCD grading system will be helpful. The ABCD grading method has been shown to be effective in additional treatment procedures such as intracorneal ring implantation and evaluating CXL efficacy.19
Our investigation found alterations in the corneal indices, keratometries of progression, and the ABCD grading system. Kmax decreased 6 months after surgery, which is a finding in other studies.16,18,20 In previous studies, researchers have observed changes in corneal curvature after the conventional CXL procedure. Wittig-Silva et al21 found a flattening of 1.03 D in the Kmax value over a 3-year period, with a sample size of 100. Hashemi et al22 reported a flattening of 0.16 D over a 5-year period, with a sample size of 40. Chow et al23 reported a flattening of 1.6 D over a 1-year period, with a sample size of 38.
The present study had limitations, including its small sample size and short follow-up time. Numerous studies15,24 have demonstrated the importance of long-term follow-up to obtain precise postoperative results because corneal cross-linking can alter the cornea several years after treatment. Future studies with larger sample sizes are needed to verify the study findings further and increase the reliability of the study findings.
Further studies with extended follow-up periods and larger samples need to be conducted in order to validate and understand the long-term effects of CXL. In addition, comparative research in quality of life assessment and CXL techniques, and subgroup analysis to optimize treatment for different demographic groups are needed.
Conclusions
When the corneal thickness profiles and the anterior and posterior curvatures of the cornea are combined, they provide a good indication of KC severity. This can help track the development of KC and the effectiveness of corneal CXL.
Abbreviations
A, anterior radius of curvature; B, posterior curvature; C, corneal thickness; BCVA, corrected distance and visual acuity; CXL, cross-linking; K1, flat keratometry; K2, steep keratometry; KC, keratoconus; Kmax, maximal keratometry; OCT, optical coherence tomography; UV, ultraviolet.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gokul A, Patel DV, McGhee CN. Dr John Nottingham’s 1854 landmark treatise on conical cornea considered in the context of the current knowledge of keratoconus. Cornea. 2016;35(5):673–678. doi:10.1097/ICO.0000000000000801
2. Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42(4):297–319. doi:10.1016/S0039-6257(97)00119-7
3. Assiri AA, Yousuf BI, Quantock AJ, Murphy PJ. Incidence and severity of keratoconus in Asir province, Saudi Arabia. Br J Ophthalmol. 2005;89(11):1403–1406. doi:10.1136/bjo.2005.074955
4. Kennedy RH, Bourne WM, Dyer JA. A 48-year clinical and epidemiologic study of keratoconus. Am J Ophthalmol. 1986;101(3):267–273. doi:10.1016/0002-9394(86)90817-2
5. Belin MW, Kundu G, Shetty N, Gupta K, Mullick R, Thakur P. ABCD: a new classification for keratoconus. Indian J Ophthalmol. 2020;68(12):2831–2834. doi:10.4103/ijo.IJO_2078_20
6. Krachmer JH, Feder RS, Belin MW. Keratoconus and related noninflammatory corneal thinning disorders. Surv Ophthalmol. 1984;28(4):293–322. doi:10.1016/0039-6257(84)90094-8
7. Randleman JB, Dupps WJ Jr, Santhiago MR, et al. Screening for keratoconus and related ectatic corneal disorders. Cornea. 2015;34(8):e20–e22. doi:10.1097/ICO.0000000000000500
8. Gomes JA, Tan D, Rapuano CJ, et al. Global consensus on keratoconus and ectatic diseases. Cornea. 2015;34(4):359–369. doi:10.1097/ICO.0000000000000408
9. Kanellopoulos AJ, Asimellis G. Revisiting keratoconus diagnosis and progression classification based on evaluation of corneal asymmetry indices, derived from Scheimpflug imaging in keratoconic and suspect cases. Clin Ophthalmol. 2013;7:1539–1548. doi:10.2147/OPTH.S44741
10. O’Brart DP, Chan E, Samaras K, Patel P, Shah SP. A randomised, prospective study to investigate the efficacy of riboflavin/ultraviolet A (370 nm) corneal collagen cross-linkage to halt the progression of keratoconus. Brit J Ophthalmol. 2011;95(11):1519–1524. doi:10.1136/bjo.2010.196493
11. Choi JA, Kim MS. Progression of keratoconus by longitudinal assessment with corneal topography. Invest Ophthalmol Vis Sci. 2012;53(2):927–935. doi:10.1167/iovs.11-8118
12. Bardan AS, Kubrak-Kisza M, Kisza KJ, Nanavaty MA. Impact of classifying keratoconus location based on keratometry or pachymetry on progression parameters. Clin Exp Optom. 2020;103(3):312–319. doi:10.1111/cxo.12927
13. Saglik A, Isik MU. Progression Analysis with ABCD grading system following corneal collagen cross-linking in keratoconus. Beyoglu Eye J. 2019;4(3):156–162. doi:10.14744/bej.2019.49469
14. Belin MW, Duncan JK. Keratoconus: the ABCD grading system. Klin Monbl Augenheilkd. 2016;233(6):701–707. doi:10.1055/s-0042-100626
15. Kasumovic SS, Pavljasevic S, Dacic-Lepara S, Jankov M. The results of corneal cross-linking in the treatment of keratoconus. Med Arch. 2013;67(5):372–373.
16. Zarei-Ghanavati S, Khakshour H, Vejdani M, Ghooshkhanei H, Vejdani A. Evaluation of changes in visual acuity, contrast sensitivity and aberrations in patients with keratoconus after corneal collagen cross-linking. J Ophthalmic Vis Res. 2017;12(3):260–264. doi:10.4103/jovr.jovr_30_16
17. Zhang X, Sun L, Chen Y, Li M, Tian M, Zhou X. One-year outcomes of pachymetry and epithelium thicknesses after accelerated (45 mw/cm(2)) transepithelial corneal collagen cross-linking for keratoconus patients. Sci Rep. 2016;6:32692. doi:10.1038/srep32692
18. Kasai K, Kato N, Konomi K, Shinzawa M, Shimazaki J. Flattening effect of corneal cross-linking depends on the preoperative severity of keratoconus. Medicine (Baltimore). 2017;96(40):e8160. doi:10.1097/MD.0000000000008160
19. Sedaghat MR, Momeni-Moghaddam H, Belin MW, et al. Anatomical and visual effects of the MyoRing implantation measured by the ABCD keratoconus grading system. Eye Contact Lens. 2020;46(1):52–56. doi:10.1097/ICL.0000000000000595
20. Kymionis GD, Grentzelos MA, Liakopoulos DA, et al. Long-term follow-up of corneal collagen cross-linking for keratoconus--The Cretan Study. Cornea. 2014;33(10):1071–1079. doi:10.1097/ICO.0000000000000248
21. Wittig-Silva C, Chan E, Islam FM, Wu T, Whiting M, Snibson GR. A randomized, controlled trial of corneal collagen cross-linking in progressive keratoconus: three-year results. Ophthalmology. 2014;121(4):812–821. doi:10.1016/j.ophtha.2013.10.028
22. Hashemi H, Seyedian MA, Miraftab M, Fotouhi A, Asgari S. Corneal collagen cross-linking with riboflavin and ultraviolet a irradiation for keratoconus: long-term results. Ophthalmology. 2013;120(8):1515–1520. doi:10.1016/j.ophtha.2013.01.012
23. Chow VW, Chan TC, Yu M, Wong VW, Jhanji V. One-year outcomes of conventional and accelerated collagen crosslinking in progressive keratoconus. Sci Rep. 2015;5:14425. doi:10.1038/srep14425
24. Noor IH, Seiler TG, Noor K, Seiler T. Continued long-term flattening after corneal cross-linking for keratoconus. J Refract Surg. 2018;34(8):567–570. doi:10.3928/1081597X-20180607-01
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.