")
Back to Journals » Journal of Asthma and Allergy » Volume 17
Assessment of Exercise Capacity in Patients Diagnosed with Moderate and Severe Bronchial Asthma: Preliminary Prospective Observational Study
Authors Bajer WA , Majewska-Pulsakowska M, Paprocka-Borowicz M, Wytrychowski K, Taradaj J , Ptaszkowski K
Received 30 May 2024
Accepted for publication 16 October 2024
Published 3 December 2024 Volume 2024:17 Pages 1247—1258
DOI https://doi.org/10.2147/JAA.S458717
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor David Price
Weronika Alicja Bajer,1 Marta Majewska-Pulsakowska,1 Małgorzata Paprocka-Borowicz,1 Krzysztof Wytrychowski,2 Jakub Taradaj,3 Kuba Ptaszkowski1
1Faculty of Health Sciences, Department of Physiotherapy, Wroclaw Medical University, Wroclaw, Lower Silesian Voivodeship, Poland; 2Faculty of Medicine, Clinical Department of Internal Medicine, Pneumology and Allergology, Wroclaw Medical University, Wroclaw, Lower Silesian Voivodeship, Poland; 3Institute of Physiotherapy and Health Sciences, Academy of Physical Education in Katowice, Katowice, Silesian Voivodeship, Poland
Correspondence: Weronika Alicja Bajer, Wroclaw Medical University, Chałubińskiego 3, 50-368 Wrocław, Wroclaw, Poland, Tel +48 71 784 28 15, Email [email protected]
Purpose: The main objective of the study was to assess exercise capacity and physical activity levels in patients with bronchial asthma compared to a control group without asthma, as well as to investigate how asthma severity affects the results of the 6MWT and physical activity as measured by the IPAQ questionnaire.
Patients and Methods: A total of 63 individuals were studied, divided into two groups: Group A, consisting of 33 individuals with bronchial asthma, and Group B, consisting of 30 individuals from the general population without bronchial asthma. In both groups, the following assessments were performed: The Six-Minute Walk Test (6MWT), The International Physical Activity Questionnaire (IPAQ) and the Borg rating of perceived exertion scale (the Borg RPE scale) ABB.
Results: It was demonstrated that patients with moderate asthma covered more distance during the 6MWT than patients diagnosed with severe asthma. The difference in metres covered between the two groups was statistically significant (p < 0.001), which could be observed during the walk test. The results indicate that a larger proportion of patients with asthma (76%) fall into the insufficient physical activity category compared to those without asthma (24%). Conversely, a higher percentage of non-asthmatic individuals (66.67%) report sufficient physical activity compared to asthmatic patients (33.33%)(P=0.005).
Conclusion: This study demonstrated that asthma severity significantly impacts exercise capacity, as shown by shorter distances covered in the 6-minute walk test (6MWT) among patients with severe asthma. While overall physical activity levels (measured by the IPAQ) were not significantly different between asthma and non-asthma groups, asthma patients exhibited significantly more sitting time, suggesting a more sedentary lifestyle.
Keywords: asthma, 6MWT, IPAQ
Introduction
According to the Global Strategy for Asthma Management and Prevention GINA 2022 (the GINA 2022 Report), bronchial asthma is a heterogeneous disease marked by chronic airway inflammation. The symptoms of this disease include wheezing, dyspnoea, chest tightness, and cough of variable frequency and severity.1
The pathomechanism of bronchial asthma is primarily chronic airway inflammation. Numerous cells and the mediators they produce are involved in this process, resulting in characteristic pathophysiological and pathomorphological changes.
The causes of asthma development are divided into two groups: those that cause the development of the disease and those that trigger its symptoms. These usually include individual factors (genetic predisposition) and environmental factors that emerge later in the course of the disease. The pathomechanisms responsible for the development and severity of asthma symptoms are complex and interact with each other. Individual factors include genetic factors, obesity and gender. Conversely, environmental factors include allergens, infections, occupational factors, tobacco smoke, outdoor and indoor air pollution, and diet.2
Assessing the severity of bronchial asthma is a major step in the overall assessment of an asthmatic patient. According to previous GINA reports, it was recommended to analyse asthma severity before starting treatment. A previous assessment of asthma severity led to asthma being diagnosed as ‘severe’ before treatment. Pharmacotherapy and general recommendations usually lead to significant control of symptoms or complete resolution.3 Hence, the GINA 2022 report recommends that asthma severity be assessed retrospectively based on the treatment required to control symptoms and exacerbations. Assessment can be performed after a few months of taking NSAIDs and when treatment has decreased over several months or years. The severity of the disease is not constant; it changes over months and years. According to GINA 2022 experts, there are three degrees of asthma severity:
• mild asthma – well controlled with Step 1 and Step 2 treatment, use of bronchodilators on demand, low doses of inhaled corticosteroids (ICS) or leukotriene modifier or chromones;
• moderate asthma – well controlled with Step 3 treatment, use of low-dose ICS in combination with a long-acting β2-agonist (LABA);
• severe asthma – use of Step 4 and Step 5 treatment.1
Asthma significantly affects the patient’s social functioning, physical activity and playing sports. Typical symptoms of asthma include an exacerbation of respiratory symptoms after intense exercise. At the same time, the level of physical activity is a fundamental parameter for assessing the level of disease control. The effect of intense exercise in asthmatic patients is a temporary increase in airway resistance. Post-exercise dyspnoea occurs in 50–80% of patients. Post-exercise bronchospasm is related to the inflammatory process underlying asthma and can affect the severity of asthma. Patients’ subconscious fear of the occurrence and severity of post-exercise symptoms leads them to limit their physical activity. This has an adverse effect on overall health and respiratory efficiency. Regular exercise in asthmatic patients improves overall health and ventilation rates and enables patients to breathe more freely. Poor weather is one of the leading causes of dyspnoea during exercise. Physical activity in cold air during freezing weather is a potent stimulus that activates the airways and causes dyspnoea. Air pollution with pollen, exhaust fumes, and tobacco smoke also has an adverse effect on the patient’s respiratory system. An important way to prevent dyspnoea is to treat asthma properly. Control of this disease is achieved through appropriate pharmacological treatment and physiotherapeutic measures.4
Physical endurance is the ability to perform prolonged physical exertion involving large muscle groups without significant disruption to homeostasis or rapidly increasing fatigue. Endurance affects the level of physical activity and determines the body’s potential to perform efforts involving large muscle groups. It can be assessed using an exercise test on a cycle ergometer, a treadmill, or an ergospirometer.5
The main objective of the study was to assess exercise capacity and physical activity levels in patients with bronchial asthma compared to a control group without asthma, as well as to investigate how asthma severity affects the results of the 6MWT and physical activity as measured by the IPAQ questionnaire.
Specific Aims:
- Assessing differences in exercise capacity between patients with moderate and severe asthma and those without asthma, as measured by the 6MWT. “Research Hypothesis: Patients with asthma, particularly those with severe asthma, will walk shorter distances in the 6MWT compared to individuals without asthma”.
- Investigating differences in physical activity levels (measured by the IPAQ questionnaire) between patients with asthma and a control group without asthma. “Research Hypothesis: Patients with asthma will demonstrate lower total physical activity levels compared to individuals without asthma”. Analyzing the relationship between the distance covered in the 6MWT, the IPAQ score, and the probability of asthma occurrence, while accounting for additional variables such as gender, age, weight, height, and BMI.
Research Hypothesis: The distance covered in the 6MWT and the IPAQ score will be negatively correlated with the probability of asthma, meaning that greater distances and higher IPAQ scores will be associated with a lower probability of asthma.
Materials and Methods
Ethical Considerations
The study was approved by the Ethics Committee of Wroclaw Medical University (approval no. KB – 568/2018). This study was entered in the ISRCTN registry – ISRCTN10887245. The study lasted from October 2018 to February 2019, which was 5 months.
The study was conducted in accordance with the Good Clinical Practice Guidelines and the Declaration of Helsinki. Each person was briefed and instructed on the conduct of the experiment before signing the consent to participate. All study participants were informed of the possibility of discontinuing their participation in the project in the case of health problems or for other reasons.
Study Material
This observational study was conducted at EuroMediCare (Wrocław, Poland) and the Healthcare Centre in Święta Katarzyna (Święta Katarzyna, Poland). A total of 74 individuals were initially assessed for eligibility based on the inclusion and exclusion criteria of the study. Eleven individuals were excluded for not meeting the study criteria. A total of 63 individuals were studied, divided into two groups: Group A, consisting of 33 individuals with bronchial asthma, and Group B, consisting of 30 individuals from the general population without bronchial asthma (Figure 1) from the local area. Similar sociodemographic characteristics formed the basis for including the A participants in the B group. Patients in the A group were qualified for the study based on spirometry findings and bronchial asthma criteria by specialists in allergology and pulmonology. Conditions for inclusion in the B group were the absence of diagnosed bronchial asthma, patient consent and good health on the day of the study. Exclusion criteria for both groups included untreated and uncontrolled hypertension; orthopaedic devices; exercise intolerance; risk factors for exercise; cardiac arrhythmia in the form of atrial fibrillation; unstable coronary artery disease; a history of myocardial infarction within the past month and other cardiac or neurological disorders preventing 6MWT, preventing exercise; and lack of consent from the participant.
 |
Figure 1 Flowchart of Study Design. |
Research Methods
Clinical Measurements
Before the study, each participant was informed how the study was to be conducted, its objectives and methods, and gave written consent.
The protocol for each study included an interview, instruction on the purpose of the measurements and the study procedures. For patients in the A and B groups, the visit protocol included three assessments:
1. A subjective assessment of exertion according to the Borg rating of perceived exertion (RPE) scale;
2. Exercise capacity assessments using the 6MWT;
3. Assessments of physical activity levels using the IPAQ.
Procedures
The Borg RPE Scale
The 12-point Borg RPE scale is used to assess the intensity and severity of dyspnoea. The Borg RPE scale assessed perceived exertion before and after the walk test in both groups.
The Six-Minute Walk Test (6MWT)
Each patient rested for approximately ten minutes before starting the test. Discontinuation of chronic medication was not recommended before the test. Patients with bronchial asthma take the recommended and prescribed medications by their attending physician. Before the 6MWT, the patient was allowed to take their medication, and there was no restriction against it. At least two hours before the walk test, the patient could not engage in vigorous and prolonged physical activity. The walk test in the A and B group lasted six minutes. For both groups, the walkway was 20 meters long and was marked every 3 meters. The ends of the walkway were also defined (start and turnaround point during the walk). Each patient walked individually, at a leisurely and convenient pace, along the empty walkway’s flat and level surface. During the A, the distance covered by the patient and the severity of perceived exertion according to the Borg RPE scale were assessed before and after the walk test. Blood pressure, heart rate and saturation were measured in each participant before and after the test. Heart rate, blood pressure and saturation were taken again five minutes after the test.
The International Physical Activity Questionnaire (IPAQ)
The IPAQ – short form – contained seven questions that referred to all types of physical activity as a component of daily life, work and leisure during the past week. Patients were asked to factor in activities carried out at work, in and around the house, moving from place to place and in leisure time devoted to recreation, exercise or sport. Information was collected from the respondents on the time spent on intensive and moderate physical activity and the time spent sitting and walking in the last seven days. Activities lasting more than ten minutes without interruption were taken into account. The questionnaire specifically inquired about the time spent in vigorous physical activity, moderate physical activity, walking, and sitting, with only activities lasting at least 10 minutes continuously being included in the analysis. Physical activity levels were reported in terms of metabolic equivalents (METs), which allowed for the classification of participants into one of three categories: high (1500–3000 MET-min/week), moderate (600–1500 MET-min/week), or low (<600 MET-min/week).
Statistical Analysis
Sample size analysis. We have conducted the sample size estimation based on the available data from our unit’s database before the study commenced. Specifically, we analyzed how the IPAQ (International Physical Activity Questionnaire) scores differed between two groups. The means and standard deviations of IPAQ results in both groups were used in the analysis for estimating the sample size.
In the study group, the mean IPAQ score was 681.3 (SD = 180), while in the control group, the mean IPAQ score was 844.09 (SD = 220). The estimated sample size was calculated using a two-sample unpaired-means test (unpaired t-test). The alpha level was set at 0.05, and the power of the test was set at 0.8. Additionally, we assumed no correlation between the evaluated variables and adopted a two-sided null hypothesis. Based on these parameters, the estimated sample size was determined to be 30 participants in each group.
Statistical analysis. Arithmetic means, medians, standard deviations, range of variation (extreme values), lower quartile, and upper quartile were calculated for measurable variables. In the case of qualitative variables, their frequency (%) was calculated. Qualitative variables were compared between the groups using the chi-squared test. All studied quantitative variables were verified using the Shapiro–Wilk test to determine distribution type. Comparison of the results of quantitative variables between groups was performed using the Mann–Whitney U-test or the t-test for independent samples, depending on whether the conditions were met. In addition, a post test (Dunn’s test) was carried out.
Furthermore, Spearman’s rank correlation coefficient for quantitative variables was applied.
The level of α = 0.05 was used for all comparisons. This study also used logistic regression to assess the influence of various independent variables on the dependent variable, which was the presence of asthma (coded as a binary variable: 0 – no asthma, 1 – asthma present). The logistic regression analysis utilized the maximum likelihood estimation (MLE) method. The model included 63 observations and 7 independent variables, including gender, age, weight, height, BMI, 6MWT test result, and the IPAQ questionnaire result. Sample size analysis and statistical analysis were performed in Statistica 13 (TIBCO Software Inc, Santa Clara; USA).
Results
A group of 63 individuals was studied. The A group consisted of 33 individuals, 16 women and 17 men, and the B group consisted of 30 individuals, 16 women and 14 men (Table 1).
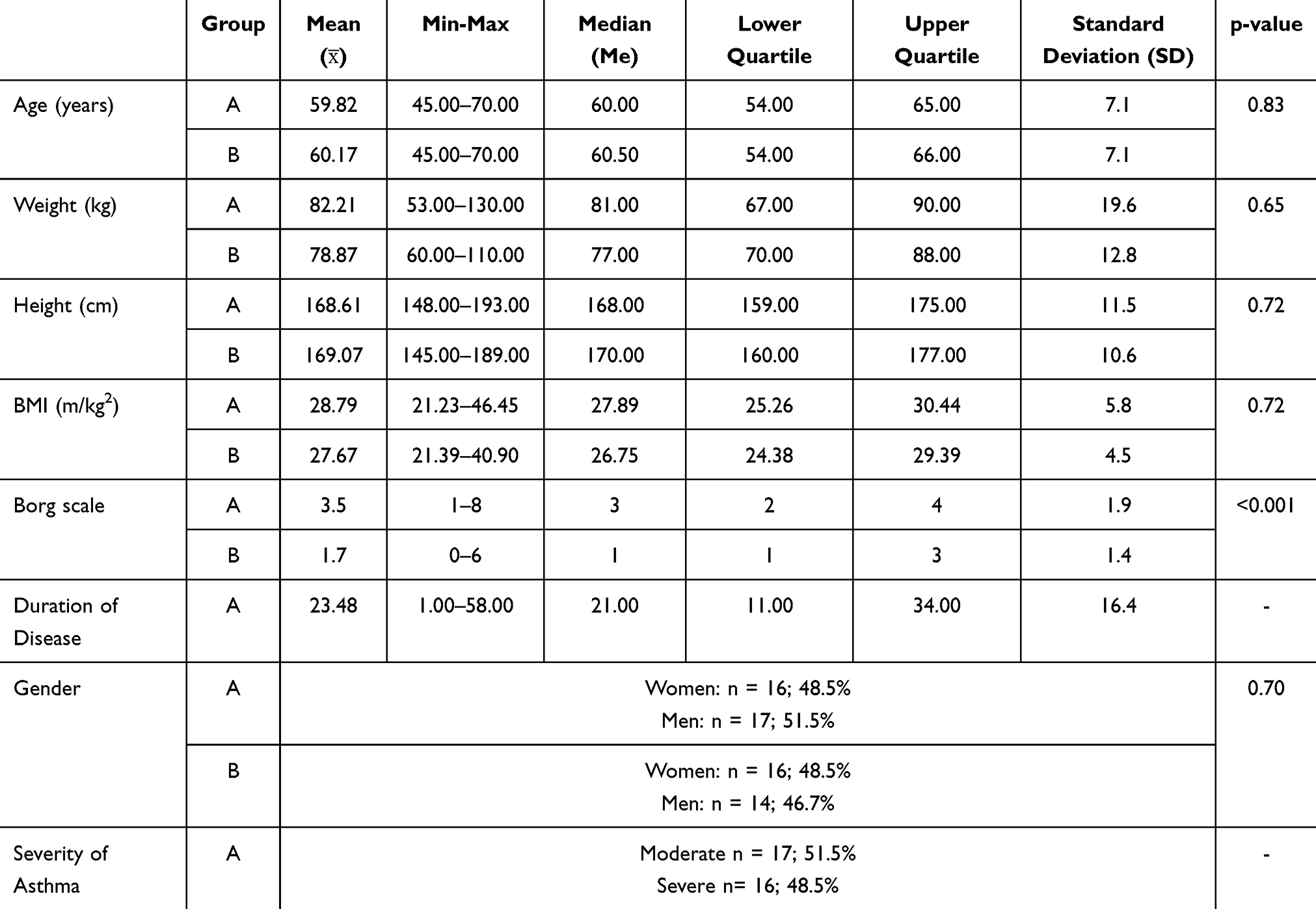 |
Table 1 Characteristics of the Study and Control Groups |
Statistical analysis began by comparing the groups studied in terms of demographic and anthropometric characteristics. No significant statistical differences were found, indicating homogeneity (Table 1).
The Table 2 presents the descriptive statistics for the IPAQ (International Physical Activity Questionnaire) scores and the 6-Minute Walk Test (6MWT) distances in patients with moderate and severe asthma. The following metrics are reported: mean (), minimum and maximum values, median (Me), lower quartile, upper quartile, standard deviation (SD), and the associated p-value.
 |
Table 2 Comparison of Results in Patients with Moderate and Severe Asthma During 6MWT |
IPAQ Scores: Patients with moderate asthma had an average IPAQ score of 970.91 MET-min/week, with a range from 219 to 2794 MET-min/week. The median was 638.40. Patients with severe asthma had a significantly lower mean IPAQ score of 445.43 MET-min/week, ranging from 99 to 918 MET-min/week. The median was 438.00, the p-value of 0.149 indicates that the difference in IPAQ scores between the moderate and severe asthma groups was not statistically significant.
Six-Minute Walk Test (6MWT) Distances: Patients with moderate asthma had an average 6MWT distance of 401.71 meters, ranging from 270 to 527 meters. The median distance was 380 meters, Patients with severe asthma had a significantly shorter mean 6MWT distance of 277.94 meters, ranging from 180 to 390 meters. The median was 280 meters. The p-value of <0.001 indicates a statistically significant difference in the 6MWT distances between the moderate and severe asthma groups, with patients with severe asthma demonstrating reduced exercise capacity.
The Figure 2 illustrates the distribution of patients across different categories of physical activity (IPAQ) in relation to their asthma status. The contingency table shows the counts and corresponding percentages of patients in three IPAQ categories: Insufficient, Sufficient, and High, stratified by asthma status (1 = Asthma, 0 = No Asthma). The results indicate that a larger proportion of patients with asthma (76%) fall into the insufficient physical activity category compared to those without asthma (24%). Conversely, a higher percentage of non-asthmatic individuals (66.67%) report sufficient physical activity compared to asthmatic patients (33.33%). The Chi-square test revealed a statistically significant association between asthma status and physical activity levels (p = 0.005), suggesting a meaningful difference in physical activity profiles between the two groups.
 |
Figure 2 Distribution of IPAQ Physical Activity Categories by Asthma Status with Chi-Square Test Results”. |
The Figure 3 presents a comparison of several variables between Group A (asthma) and Group B (control group without asthma) using box plots for each variable. The p-values from the Mann–Whitney U-test are displayed for each comparison.
 |
Figure 3 Boxplot Analysis of IPAQ (Vigorous activity, Moderate activity, Walking, Sitting, Total physical activity) and 6MWT: Group A (Asthma) vs Group B (Control)”. |
The median total physical activity (IPAQ_total) appears slightly lower in Group A compared to Group B, but the difference is not statistically significant (p = 0.25).
Group B (control group) shows a higher median distance covered during the 6-Minute Walk Test (6MWT) compared to Group A, suggesting better exercise capacity in the control group. Although the difference is noticeable (p = 0.061).
There is no significant difference between Group A and Group B in terms of vigorous physical activity levels. The p-value (0.865) indicates no meaningful difference between the groups.
Group B shows a slightly higher median level of moderate physical activity compared to Group A, but this difference does not reach statistical significance (p = 0.076).
There is a noticeable but non-significant difference between the two groups in terms of walking activity, with Group B showing slightly higher median walking levels compared to Group A (p = 0.082).
The most significant difference between Group A and Group B is observed in sitting time. Group A (asthma) reports significantly higher sitting time compared to Group B (p = 0.002), suggesting that patients with asthma spend more time sitting.
The univariate logistic regression analysis was performed to evaluate the relationship between several independent variables and the presence of asthma (Table 3). The results showed that the variables 6-Minute Walk Test (6MWT) and Borg scale were significantly associated with the likelihood of asthma, while other variables such as gender, age, weight, height, BMI, and IPAQ_total did not demonstrate statistically significant associations. 6MWT (Coefficient = −0.0054, p = 0.048, 95% CI: −0.0107 to −0.0001) was negatively associated with asthma, indicating that for each additional meter walked, the odds of having asthma decrease. Borg scale (Coefficient = 0.7055, p = 0.002, 95% CI: 0.2673 to 1.1436) showed a significant positive association with asthma. Higher perceived exertion on the Borg scale was related to an increased likelihood of asthma, indicating that patients with asthma experience higher levels of exertion during physical activity.
 |
Table 3 Logistic Regression Analysis Predicting Asthma Presence |
Other variables, including gender (p = 0.701), age (p = 0.842), weight (p = 0.426), height (p = 0.867), BMI (p = 0.394), and IPAQ_total (p = 0.861), were not statistically significant predictors of asthma in this model.
Discussion
This study has described the difference in physical activity and exercise capacity between patients with moderate bronchial asthma and those with severe asthma, compared with a sex- and age-matched control population.
We have demonstrated that patients with asthma show reduced exercise capacity scores compared to controls. Our results also show that patients diagnosed with severe asthma have reduced physical capacity compared to both the control group and patients with moderate asthma. Cordova-Rivera et al also demonstrated this in their study. Bronchial asthma is a chronic disease that significantly impacts patients’ quality of life. Currently, asthma management is limited to drug treatment, primarily with steroids, aimed at Bling symptoms and bronchial inflammation, while other therapeutic approaches to Bling asthma have been neglected. According to reports by Polish and international researchers, pulmonary rehabilitation in asthmatic patients reduces symptoms, improves quality of life and reduces the number of medicines taken.6,7
According to Bruurs et al, breathing exercises, exercises for strengthening respiratory muscles, physical exercises and physiotherapeutic techniques that help clear the airways, improve quality of life and physical parameters, and reduce symptoms and medication intake.8
In patients with chronic lung disease, the quality of life may be impaired by an inability to achieve satisfactory physical activity levels. This was demonstrated by Cordova-Rivera et al. They found that severe asthma was associated with lower levels of physical activity. Higher activity levels and less sedentary lifestyles were associated with better exercise capacity, asthma B and reduced systemic inflammation. Cordova-Riviera et al concluded that interventions in the form of increased walking and reduced sitting time had an impact on improving exercise capacity and patients achieving higher levels of physical activity.9
Complex interactions between biomechanics, physiology and psychological mechanisms influence activity limitation. According to Ford et al, there is a clear relationship between reduced physical activity and quality of life in patients. Severe asthma is associated with a more than twofold risk of reduced physical activity, negatively affecting professional and daily activities.10 Our findings from the 6MWT in asthmatic patients demonstrate unequivocally that patients with severe asthma covered a shorter distance (277.94 m) than patients with moderate asthma (401.71 m). Physical activity should be distinguished from exercise capacity, defined as the maximum amount of physical exertion a patient can endure. Exercise capacity is related to the patient’s vital signs. In asthmatics, it is usually determined by spirometry. A involving asthma patients found that patients with lower spirometry scores (severe asthma) covered a shorter distance during the 6MWT than patients with higher spirometry scores (moderate asthma). According to François Vermeulen et al, exercise capacity among asthmatics can be improved by regular exercise and a well-balanced diet.11
Our findings show that the BMI was not dependent on spirometry results, as patients with severe asthma had similar BMI values to patients with moderate asthma. In recent years, many researchers have drawn attention to the problem of symptom control in asthma, as demonstrated by Pedersen et al. According to them, the classification of asthma severity based solely on a subjective assessment of symptom frequency based on St George’s Respiratory Questionnaire (SRGQ) and spirometry results does not take into account many important aspects for the patient. First, it does not determine functional physical activity; insight into it can be obtained from screening tests, eg the 6MWT, to confirm subjective physical activity with an objective score during the test.12
The application and use of the 6MWT was presented by Agarwala et al. The walk test assesses exercise tolerance, qualification for rehabilitation, and the appropriate level of load applied during exercise. It is also used to evaluate the effectiveness of improvement. The 6MWT is a simple way to assess exercise tolerance, adaptation to daily life activities and the effectiveness of treatment and prognosis. The 6MWT has become a popular method for assessing exercise capacity in clinical practice.13 An assessment of exercise capacity in patients from the study and control groups carried out during our research showed that the average score during the 6MWT for patients in the study group was 341.7 m and 396.5 m for patients in the control group. It was also demonstrated that the higher the severity of asthma, the lower the distance covered during the 6MWT. The average distance for patients with moderate asthma was 401.71 m and for those with severe asthma – 277.94 m.
Marcon et al showed in their study that patients with mild asthma covered a distance 17.1 m shorter in the 6MWT than patients in the control group. The authors also noted that patients with asthma are less active than healthy individuals. Their study also found that male gender, younger age, lower BMI and better asthma control were associated with covering more walking distance.14 Coelho et al reported that asthma patients covered a distance of 521.1 m in the 6MWT, while controls covered 529.8 m. The researchers proved that there is a correlation between the quality of life, the distance covered during the 6MWT and the occurrence of depression. Patients who had been diagnosed with or had symptoms of depression showed lower quality of life and covered a shorter distance in the walk test compared to healthy patients.15
The analysis of the IPAQ conducted in our study showed that patients with asthma scored lower in moderate activity, vigorous activity and walking than patients in the control group. This difference was statistically significant. The insufficient physical activity category included 57.58% of patients in the study group and 20% of patients in the control group. The sufficient physical activity category included 33.33% of patients with asthma and 73.33% of healthy controls. The high physical activity category consisted of 9.09% of patients in the study group and 6.67% of patients in the control group. Much higher results were reported by Ziętkowski et al but with a similar ratio between patient groups. The insufficient physical activity category included 49% of patients in the study group and 7% of those in the control group. The sufficient physical activity category consisted of 10% of patients diagnosed with asthma and 8% of healthy controls. The high physical activity category comprised 41% of patients in the study group and 85% in the control group. The authors also indicated that the physical activity level of patients diagnosed with asthma decreased significantly as the extent of disease control declined. More than half of patients with uncontrolled asthma had insufficient levels of physical activity. It was also shown that patients reported less physical activity as spirometry results deteriorated.16
According to Shi et al, it is advisable for patients diagnosed with asthma to be physically active. Regular physical activity reduces the incidence of dyspnoea, has a tangible impact on better disease control, reduces the incidence of hospitalisation and shortens the length of hospital stay. Regular exercise contributes to psychological well-being and improves patients’ quality of life.17
Patients diagnosed with asthma were advised against physical activity for many years. Currently, appropriate therapeutic management enables the patient to engage in regular exercise, improving respiratory and cardiovascular efficiency. Physical activity reduces the risk of asthma attacks and disease symptoms. Correct asthma management involves the ability to use medication, appropriate sports adapted to the age and severity of the disease, and the conditions under which exercise is performed.18,19
Study Limitations
Our study has some limitations. Firstly, a one-off therapeutic intervention is used in the study. The MRC scale and the Borg RPE scale are subjective. The exercise capacity assessment in patients with bronchial asthma is influenced by the exacerbation of the disease, which was not taken into account when examining the patients. The physical activity assessment did not address musculoskeletal conditions, which may negatively affect activity levels and sitting time during the day or interact with some dependent outcomes. This is a future area of research.
Conclusion
This study demonstrated that asthma severity significantly impacts exercise capacity, as shown by shorter distances covered in the 6-minute walk test (6MWT) among patients with severe asthma. While overall physical activity levels (measured by the IPAQ) were not significantly different between asthma and non-asthma groups, asthma patients exhibited significantly more sitting time, suggesting a more sedentary lifestyle.
The regression analysis revealed a significant association between Borg scale scores and asthma, indicating that patients with asthma perceive higher levels of exertion during physical activity. This may contribute to lower participation in physical activity, despite their similar total physical activity scores compared to controls.
Although increased physical activity was associated with better performance in the 6MWT, it remains uncertain whether promoting physical activity will lead to long-term improvements in asthma patients’ exercise capacity. Further research is needed to explore the long-term effects of physical activity interventions and to better understand the factors influencing exertion and exercise tolerance in asthma patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. GINA committee. Global Strategy For Asthma Management and Prevention 2022 Update. Glob Initiat Asthma. 2022;225. Available from: http://www.ginasthma.org.
2. Kuruvilla ME, Vanijcharoenkarn K, Shih JA, Lee FEH. Epidemiology and risk factors for asthma. Respir Med. 2019;149(November 2018):16–22. doi:10.1016/j.rmed.2019.01.014
3. Diagnosis of Diseases of Chronic Airflow Limitation: Asthma COPD and Asthma-COPD Overlap Syndrome (ACOS) Based on the Global Strategy for Asthma Management and Prevention and the Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease. 2014 The Global Initiative for Asthma and The Global Initiative for Chronic. 2014. Available from: www.ginasthma.orgwww.goldcopd.org.
4. Parsons JP, Hallstrand TS, Mastronarde JG, et al. An official American Thoracic Society clinical practice guideline: exercise-induced bronchoconstriction. Atsjournals.org. 2013;187(9):1016–1027. doi:10.1164/rccm.201303-0437ST
5. Bull FC, Al-Ansari SS, Biddle S, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54(24):1451–1462. doi:10.1136/bjsports-2020-102955
6. Majewski M, Dabrowska G, Pawik M, Rozek K. Evaluation of a home-based pulmonary rehabilitation program for older females suffering from bronchial asthma. Adv Clin Exp Med. 2015;24(6):1079–1083. doi:10.17219/ACEM/31679
7. Miller RL, Grayson MH, Strothman K. Advances in asthma: new understandings of asthma’s natural history, risk factors, underlying mechanisms, and clinical management. J Allergy Clin Immunol. 2021;148(6):1430–1441. doi:10.1016/J.JACI.2021.10.001
8. Bruurs MLJ, Van Der Giessen LJ, Moed H. The effectiveness of physiotherapy in patients with asthma: a systematic review of the literature. Respir Med. 2013;107(4):483–494. doi:10.1016/J.RMED.2012.12.017
9. Cordova-rivera L, Hons B, Gibson PG, Gardiner PA. Physical activity and exercise capacity in severe asthma: key clinical associations participant selection. J Allergy Clin Immunol in Pract. 2018;1–9. doi:10.1016/j.jaip.2017.09.022
10. Ford ES, Mannino DM, Redd SC, Moriarty DG, Mokdad AH. Determinants of quality of life among people with asthma: findings from the behavioral risk factor surveillance system. J Asthma. 2004;41(3):327–336. doi:10.1081/JAS-120026090
11. Vermeulen F, Garcia G, Ninane V, Laveneziana P. Activity limitation and exertional dyspnea in adult asthmatic patients: what do we know? Respir Med. 2016;117:122–130. doi:10.1016/j.rmed.2016.06.003
12. Knag Pedersen S, Ustrup AS, Baarnes CB, Suppli Ulrik C. Usefulness of mannitol challenge testing for diagnosing asthma in everyday clinical practice. J Asthma. 2020;57(6):663–669. doi:10.1080/02770903.2019.1600144
13. Agarwala P, Salzman SH. Six-minute walk test: clinical role, technique, coding, and reimbursement. Chest. 2020;157(3):603. doi:10.1016/J.CHEST.2019.10.014
14. Marcon A, Girardi P, Ferrari M, et al. Mild asthma and chronic bronchitis seem to influence functional exercise capacity: a multi-case control study. Int Arch Allergy Immunol. 2013;161(2):181–188. doi:10.1159/000345137
15. Coelho CM, Campos LA, Pereira FO, et al. Objectively measured daily-life physical activity of moderate-to-severe Brazilian asthmatic women in comparison to healthy controls: a cross-sectional study. J Asthma. 2018;55(1):73–78. doi:10.1080/02770903.2017.1306547
16. Ziętkowski Z, Skiepko R, Skiepko U, Perkowska M, Bodzenta-łukaszyk A. Ocena poziomu i rodzaju aktywności fizycznej pacjentów z astmą [The evaluation of level and type of physical activity in patient with asthma]. Alergoprofil. 2013;9(2):26–31. Polish.
17. Shi S, Huang H, Zheng R, et al. Can long-term regular physical activity improve health outcomes among adults with asthma—evidence from a systematic review and Bayesian meta-analysis. Ann Transl Med. 2022;10(6):338. doi:10.21037/ATM-22-1170
18. McLoughlin RF, Clark VL, Urroz PD, Gibson PG, McDonald VM. Increasing physical activity in severe asthma: a systematic review and meta-analysis. Eur Respir J. 2022;60(6):2200546. doi:10.1183/13993003.00546-2022
19. Freitas PD, Silva AG, Ferreira PG, et al. Exercise improves physical activity and comorbidities in obese adults with asthma. Med Sci Sports Exerc. 2018;50(7):1367–1376. doi:10.1249/MSS.0000000000001574
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.