")
Back to Journals » Clinical Ophthalmology » Volume 18
Assessment of Tamarind Seed Polysaccharide (TSP) and Hyaluronic Acid (HA) Containing Ophthalmic Solution to Maintain Tear Osmolarity, Ocular Surface Temperature (OST) and Tear Production
Authors Alotaibi WM , Abusharha A, Pearce EI, Althomali M, Afsar T , Razak S
Received 27 August 2024
Accepted for publication 19 November 2024
Published 28 November 2024 Volume 2024:18 Pages 3503—3513
DOI https://doi.org/10.2147/OPTH.S493336
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Wafa M Alotaibi,1 Ali Abusharha,1 E Ian Pearce,2 Mohammed Althomali,1 Tayyaba Afsar,3 Suhail Razak3
1Department of Optometry, College of Applied Medical Sciences, King Saud University, Riyadh, 11433, Saudi Arabia; 2Glasgow Caledonian University, Glasgow, G4 0BA, UK; 3Department of Community Health Sciences, College of Applied Medical Sciences, King Saud University, Riyadh, 11433, Saudi Arabia
Correspondence: Suhail Razak, Department of Community Health Sciences, College of Applied Medical Sciences, King Saud University, 10219, Riyadh, 11433, Saudi Arabia, Email [email protected]
Background: The enhancement of ocular drug delivery is achieved by using biopolymer carriers in liquid ophthalmic preparations. Using natural polysaccharides to formulate ocular medications is attractive because they are economical and readily available. The primary goal of the study was to assess the safety and effectiveness of Tamarind seed polysaccharide (TSP)/Hyaluronic acid (HA) containing Rohto eye drops (TSP/HA drops) in alleviating the signs and symptoms of dry eye disease (DED) under dry environmental conditions using controlled environmental chamber (CEC).
Methods: 12 participants were subjected to harsh environmental conditions in a CEC with a relative humidity (RH) of 5% and an ambient temperature of 21°C. TSP/HA drops were used in the two treatment modalities, protection (drops instilled before exposure to the dry environment and relief (drops instilled after exposure to the dry environment. Before and after administering drops, patients undergo screening for ocular symptoms, tear osmolarity, ocular surface temperature (OST), and tear production using the ocular Surface Disease Index questionnaire (OSDI), OcuSense TearLab Osmometer, FLIR System ThermaCAM P620, and phenol red test (PRT) respectively. Tear production was calculated by the Tear Function Index test (TFI).
Results: Before (protection) and after (relief) exposure to the dry environment, TSP/HA resulted in a mean tear osmolarity of 296.0 mOsm/L and 292.0 mOsm/L, with no significant statistical difference. The presence of TSP/HA in both protection and relief modes led to an increase in tear production. TSP/HA drops did not significantly affect OST compared to the absence of TSP/HA drops at 5% RH. There was a significant increase in mean symptom score from 14 at 40% RH to 128 at 5% RH (p=0.003). A substantial reduction in symptoms was found in both protection (before exposure) (35) (p=0.003) and relief (after exposure) (50) (p=0.005) compared to when no drop was used.
Conclusion: It was apparent that using TSP/HA for protection was superior to relief for osmolarity and eye comfort. To optimise the therapeutic efficacy of TSP/HA, it is advisable to instruct patients to administer it before exposure to dry atmospheric conditions. The small sample size limits the ability to generalize the findings. Future studies should evaluate the tear supplement with a larger sample to improve statistical power.
Keywords: tamarind seed polysaccharide, TSP, hyaluronic acid, HA, tear function index test, dry eye disease, ocular symptoms, tear osmolarity, ocular surface temperature
Introduction
Individuals working in environments with low humidity often experience ocular symptoms, including itching, burning, and irritation. This occurs due to the reduced moisture in the air which can cause the eyes to become dry and uncomfortable These symptoms can be a significant source of discomfort and may affect productivity levels in the workplace.1–3 Many attempts have been made to control the relative humidity (RH) in indoor environments.4,5 Unfortunately, most of these environmental factors cannot be avoided. Despite the lack of sensory receptors specifically for humidity, symptoms of ocular discomfort have been commonly reported in dry air conditions.6 Dry eye disease (DED) pathogenesis involves cytotoxic inflammatory mediators, altered function of lacrimal glands and nerves, and metaplasia of the squamous epithelium of the conjunctiva. The corneal epithelium is damaged due to all of these factors.7
Eye drops are one of medical practice’s most regularly suggested dosage forms. However, they are often characterized by low bioavailability due to numerous eye barrier mechanisms. The strategies that enhance ocular drug delivery and advance bioavailability have become the main focus of investigations in the field of ophthalmic medicine advancement. The ocular drug bioavailability can be improved by extending retention time or enhancing the ocular permeability.8 The enhancement of ocular drug delivery is achieved by using biopolymer carriers in liquid ophthalmic preparations. Due to their many advantages, which include increasing the viscosity of the tear film, exhibiting bio-adhesive properties, and resisting drainage systems, they can prolong drug retention at the application site and improve the therapeutic effect.9,10 The use of natural polysaccharides for the formulation of ocular medications is attractive because they are economical and readily available. Furthermore, they are non-toxic, possibly biodegradable, generally biocompatible, and can be modified chemically.11–13 Tamarind seed polysaccharide (TSP) is a mucoadhesive polymer extracted from tamarind kernels.14,15 TSP has been proven to improve the delivery and retention of ophthalmic solutions in the eye.16–19 A study has revealed that TSP 0.7% (w/vol) had a significant impact on the mean residence time of a variety of ophthalmic solutions when compared to other polymers like hyaluronic acid, hydroxyethyl cellulose and arabinogalactan.18 Hyaluronic acid (HA) is a natural polysaccharide that is present in the skin, connective tissues, umbilical cord, and the vitreous body of the eye. HA’s biocompatibility and muco-adhesiveness are its main advantages, along with its pseudo-plastic and viscoelastic behaviour used as a vehicle for ocular drug delivery.20,21 The use of HA for dry eye and ocular surface damage has been comprehensively acknowledged.22–24 Viscoelastic solutions, mainly those based on HA are plausibly useful in relieving signs of ocular burning, itching, and grittiness in patients with DED. Opthalmic solutions containing HA are more comfortable, cause less blurring, have longer residence time, provide superior hydration, and reduce surface friction. As a result, they are more effective in relieving DED symptoms.25 By encouraging corneal epithelium migration, adhesion, and proliferation, HA promotes the process of corneal wound healing.26,27 Patients with meibomian gland dysfunction recovered tear film stability after HA treatment.23 The mean tear breakup time (TBUT) significantly improved at 15, 30, and 60-minute time points after using HA compared to no HA.23 The efficacy of TSP has been examined among contact lens wearers with mild dry eyes. A previous study indicated TSP (Xioial, Farmigea, Pisa, Italy) treatment for sixty days resulted in notable improvement in tear stability, ocular comfort, tear production, and reduced ocular surface epithelial damage.28 In another study, TSP is effective in relieving dry eye symptoms and corneal damage.29 The mixture of hyaluronic acid and chitosan, hyaluronic acid, and TSP exhibits synergistic mucoadhesive properties.9,17,30
Numerous investigations have been directed at mucomimetic polysaccharides, but the greatest of them have been dedicated to the physical properties of these formulations and not their medical efficiency. These studies have found that TSP has mucoadhesive properties that can improve drug absorption and prolong drug elimination from the ocular surface.16 However, there are only an inadequate magnitude of publications that explore the influence of these preparations on tear film parameters ie, osmolarity, tear production, ocular discomfort, and ocular surface temperature. These studies did not evaluate the effectiveness of TSP in treating dry eyes caused by adverse environments or its interaction with tear film parameters. These studies could have been more informative if the authors had investigated the interrelationship between tear parameters and how TSP changes them to better understand the mechanism of TSP action. The current investigation aimed to study the response of tear film parameters to adverse dry environmental conditions and how these parameters are related to each other. This helps to gain insights into the mechanisms underlying changes caused by external factors. These investigations were performed using a technique to induce dry eye in healthy normal individuals. This method facilitates the testing of dry eye products on a well-controlled and rapid screening system. Additionally, we aim to establish a method for inducing dry eye in healthy individuals to create a well-controlled and efficient screening system for testing dry eye products.
Methods
Study Participants, Inclusion and Exclusion Criteria
In this investigation, twelve healthy male subjects with a mean age of 29 ± 4 years were selected. All human measures were executed following the ethical standards of the institution and the national committee accountable for human experimentation, as well as the Helsinki Declaration of 1975, revised in 2019.31 Approval for the study was obtained from the Glasgow Caledonian University Ethics Committee, Scotland, UK. (June 2021, GCU1321/34/A). All techniques were completely described to participants, and they provided written consent. All study procedures were carried out in a controlled environmental chamber (CEC). The CEC was designed and constructed by Weiss-Gallenkamp, (Loughborough, UK) in a tear film lab at the University of Glasgow Caledonian University. The CEC can produce any temperature between 5 and 35°C (± 2 °C) and relative humidity (RH) between 5 and 95% (± 3%). The room temperature was constant at both conditions at 21 °C.32
Inclusion criteria did not involve gender. However, all participants were male due to recruitment by individual contacts. A screening visit was piloted to estimate tear film and ocular surface integrity. Participants were selected if they met the following conditions ie normal tear secretion (Schirmer’s strip wetting length > 10 mm in 5 minutes) (Clement Clarke International Ltd (Wales, UK)) and a total symptoms score < 12 on the Ocular Surface Disease Index (OSDI) questionnaire.33 Subjects with a history of ocular surgery, ocular disease or who wear contact lenses were excluded from this study.
Protocol of Examination
Rohto Dry Eye Relief drops (purchased from Rohto Pharmaceutical Co, Osaka, Japan) containing a mixture of TSP and HA were used in the two treatment modalities, protection and relief. These drops were preferred for their unique composition, containing hyaluronic acid and tamarind seed polysaccharide biopolymer, mannitol, sodium phosphate monobasic monohydrate, sodium phosphate dibasic dodecahydrate, and purified water. Tear film parameters were examined 15 minutes after subjects were exposed to a 5% relative humidity (RH) environment. Then the eye drop was administered following the 15-minute exposure to evaluate whether the subjects experienced any relief (relief method). In the protection method, the eye drop was applied before exposure to the dry condition, and the tear film parameters were evaluated after a 15-minute of exposure to 5% relative humidity. The design of the protection and relief testing routine is more fully described in our previous examinations.34,35 Briefly, two appointments were conducted to carry out all the techniques to study tear parameters for the right eye during the two modalities. The subjects were divided into two groups. Group A was seen in protection and group B was seen in relief appointment. Each group was then crossed over so that Group A was tested in the relief method and Group B at protection at their next appointment.
Tear Film Parameters
Symptoms Assessment Using Ocular Surface Disease Index
Self-reporting of symptoms by patients has proven to be a reliable and repeatable tool to diagnose DED.36 Ocular symptoms of dry eye were evaluated using the Ocular Surface Disease Index (OSDI) developed by Allergan Inc (Irvine, California, USA).33 It is a twelve-item questionnaire providing an assessment of three major categories of symptoms. These categories include Ocular symptoms (soreness, grittiness, sensitivity to light, blurred, and poor vision) and vision function (driving at night, reading, working with computers, and watching TV), Environment-related symptoms (uncomfortable in air-conditioned rooms, in windy conditions, or dry places). The OSDI has a maximum score of 100 points. A patient with an OSDI score lower than 12 points is considered to have no ocular symptoms compatible with DED/ocular discomfort.
Infrared Thermography of Ocular Surface
Ocular surface temperature measurement (OST) was measured non-invasively using FLIR System ThermaCAM P620 (FLIR Systems, Surrey, UK).37 Infrared cameras record ocular temperature using emitted infrared radiation.38 The self-calibrating camera comes with a high-definition detector (focal plane array, 640×480 pixels) that is thermally sensitive to ±0.06°C and can detect temperatures ranging between −40 and + 500°C. Emissivity should be taken into consideration as the infrared thermometry technique calculates surface temperature by measuring the emitted radiation from the surface. A black body is considered the perfect emitter object with an emissivity of 1 (ε=1).39 It has been found that the anterior ocular surface has the same thermal properties as skin and water with an emissivity of 0.98 (ε = 0.98).40,41 The emissivity of the camera was set at 0.98. The temperature of the entire ocular surface, including both upper and lower eyelids, was continuously recorded at a frame rate of 30 hz for one minute. The camera data was transferred to a computer via Firewire cable, then and analysed using ThemaCAM Researcher Professional v2.9 software (FLIR Systems, Surrey, UK). The vertical distance from the pupil centre to the lower lid margin and the horizontal distance to the inner canthus were measured for each subject. The mean, maximum, and minimum temperatures were calculated for the area of interest on the ocular surface.42
Measurement of Tear Osmolarity
An OcuSence TearLab Osmometer was used to measure osmolarity using a technology of electrical impedance spectroscopy.43 A nano tear sample (50 nanolitres) is collected and analyzed using a single-use disposable chip. When the tear sample is collected, the collection pen provides visual and audio signals. The handheld pen is then placed in the stationary reader which analyses the sample by passing an electrical signal through the tear sample and displaying the osmolarity measurement. Values between 293 and 320 mOsm are the overlapping areas between normal and dry eye osmolarity.44 TFOS DEWS II reported that values of 308 mOsm/L or differences between eyes greater than 8 mOsm/L could be indicative of impaired ocular homeostasis (regarding DED).45
Tear Production Measurement Using Phenol Red Thread (PRT)
The tear film is mainly produced by the lacrimal gland.46 The mean tear flow of the normal tear film has been reported to be 1.03±0.39 µL/min, which refers to the measurement obtained using the fluorophotometric technique. This technique involves observing the decay of fluorescein concentration in the tear film for 30 minutes following the instillation of 1 μL of 2% fluorescein sodium into the lower fornix with a measuring, then scans are performed every 2 minutes. Then Tear Turnover Rate (TTR) is obtained from a defined formula described by Tomlinson et.al. The turnover in μL/min is then calculated.47 Tear flow in normal and dry eye patients has been extensively investigated to estimate tear production in normal and dry eye patients. The Phenol red thread test is used to measure residual tears in the lower conjunctival sac rather than the tear production that may allow a clinical differentiation of dry eye. The average absorption of tear by PRT is just 0.5 μL, therefore assessment of full tear production is unlikely to occur with PRT. PRT is a cotton thread impregnated with phenol red first suggested by Hamano for measurement of tear production.48 Phenol is a pH-sensitive indicator, that changes from yellow to red when it is inserted into the eye due to a change in the pH.49,50 The thread is inserted into the lower fornix for 15 seconds and the tear production is estimated by measuring the length of the red (wetted) part of the thread. The main advantage of PRT over other invasive techniques like Schirmer is that it is less invasive, resulting in less reflex tearing.
Statistical Validation
The data was analyzed statistically using PASW Statistics version 18 (IBM corporation, Somers, NY, USA). A Kolmogorov–Smirnov test was applied to measure normality. Normally distributed data were evaluated using repeated measures ANOVA followed by Tukey’s post-hoc test. Data that were not normally distributed were compared using Friedman test followed by a post-hoc Wilcoxon rank-sum test. Correlation between parameters was tested using Pearson’s correlation for normally distributed data, and Spearman’s rho test was applied for data that did not follow a normal distribution. Tear osmolarity, PRT and ocular surface temperature data were normally distributed, whereas OSDI scores were not parametric data. All data of tear production measured at 5% RH using PRT (Equation 1) was corrected using the formula obtained from the slope of the line and intercept.

Results
The study compared tear film parameters under two different relative humidity (RH) conditions (40% and 5%) and evaluated the effects of TSP/HA instillation for protection and relief during exposure to 5% RH. The mean and standard deviation values of various measurements are shown in Table 1.
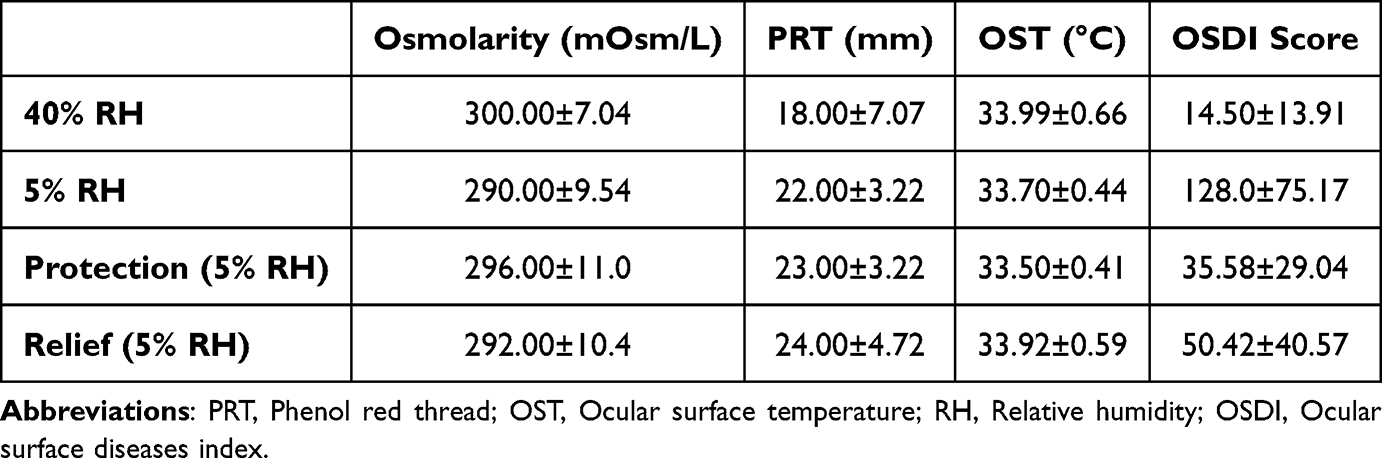 |
Table 1 The Mean and Standard Deviation of Tear Parameters Were Measured at 40% RH, 5% RH, Protection, and Relief |
Osmolarity
The mean tear film osmolarity decreases from 300.0 mOsm/L at 40% RH to 290.0 mOsm/L at 5% RH. However, the drop in tear film osmolarity observed during exposure to 5% RH was not significantly different (p=0.055) (Figure 1). Under 5% humidity condition the mean osmolarity remained unchanged with the use of TSP/HA drops measuring 296.0 0 mOsm/L (protection method) and 292.0 0 mOsm/L (relief method).
 |
Figure 1 The graph illustrates the reduction in tear osmolarity during exposure to a dry environment (p=0.055) (n=12). At the protection visit, the instillation of TSP/HA drops maintained tear osmolarity at the same level observed at 40%. Abbreviation: RH, Relative humidity. |
Measurement of Tear Production
The mean Phenol Red Thread (PRT) wetting length was 18.00 mm at 40% RH compared with 22.0 mm under desiccating conditions (5% RH) (Figure 2). An increase in tear production was observed when TSP/HA was instilled in both protection and relief modes. In protection, the mean wetting length was 23.00±3.00 mm, while in the relief method, the tear production increased to 24.00±5.00 mm. However, although a repeated measured ANOVA showed statistical differences in tear production (P=0.013), a post-hoc pairwise test (Tukey’s) showed no statistical differences between the measurements. This statistical anomaly could be due to the relatively small sample size.
 |
Figure 2 Box plot PRT wetting showed no significant change in tear production during exposure to dry conditions (5%). The mean wetting length was increased post-instillation of TSP/HA in protection and relief modes, but the increase did not reach significance compared with both 40 and 5% RH when no TSP/HA was used (n=12). Abbreviation: RH, Relative humidity. |
Validity of Tear Film Production Measurements
The pilot study was performed to validate tear production measurement by PRT under 40 and 5% RH. The results showed reduced wetting length for all strip tests at 5% RH. The reduction was statically significant for PRT (p=0.002) (Figure 3). A linear regression test was applied to estimate how to convert the PRT values observed at 5% RH to the corresponding true value that would be seen at 40% RH.
 |
Figure 3 Relative humidity (RH) affects the measurement of phenol red threads (PRT). A significant reduction in wetting length of the PRT (p=0.002) was found as subjects (n=7) were observed in 5% RH. |
Measurement of Ocular Surface Temperature (OST)
The mean ocular surface temperature at 40% RH was 33.99 °C and decreased to 33.70 °C after exposure at 5% RH (Figure 4). However, the change in RH did not cause a significant change in OST. The use of TSP/HA did not significantly alter OST compared to when no TSP/HA was used at 5% RH.
 |
Figure 4 The ocular surface temperature was measured at 40% and 5% RH without using TSP/HA tear supplement (Control) and following the instillation of TSP/HA either before (protection) or after (relief) exposure to a desiccating environment (n=12). No significant difference was observed in any of the observations. |
Measurement of Ocular Discomfort
A box plot showing the ocular discomfort score is presented in Figure 5. There was a significant increase in mean symptom score from 14 at 40% RH to 128 at 5% RH (p=0.003). A significant reduction in symptoms was found in both protection (before exposure) (35) (p=0.003) and relief (after exposure) (50) (p=0.005) compared to when no drop was used. However, no significant difference was seen between protection and relief (p= 0.12).
 |
Figure 5 A box plot showing ocular discomfort (visual analogue scale) experienced by subjects at 40 and 5% RH (Control) and when TSP/HA was used before (protection) and after (relief) exposure to 5% RH (n=12). A significant reduction in discomfort results was observed with the use of TSP/HA both before exposure (protection) and following exposure (relief). Pairwise significant differences are indicated by (*). Abbreviation: RH, Relative humidity. |
Discussion
In dry environments or areas with low humidity levels, individuals often report suffering from dryness in the eyes, nose, and skin. This can be noticeable as an itchy or scratchy sensation in the eyes, a feeling of congestion in the nose, and flaky or tight skin. These indications are usually initiated by a lack of moisture in the air, which can lead to dehydration of the mucous membranes and skin.1–3 Numerous efforts have been commenced to improve the quality of the indoor working environment.3,4 At times the surrounding atmosphere cannot be improved making avoidance of exposure to adverse climate conditions hard. Therefore, the tear film and ocular surface should be secure against these adverse environments. It has been found that ocular comfort is enhanced significantly as office humidity increases.4 The dry eye drops containing TSP/HA, which are presently available in the market, have been used in this investigation. The manufacturer has likely conducted related studies before launching the prescription. However, our study aims to provide independent and comprehensive insights that complement and potentially expand the existing literature. Our examination underscores the value of our independent analysis, which meaningfully contributes to the discourse on safety and effectiveness. For this purpose, the response of tear film parameters to adverse dry environmental conditions and the interrelationship between these parameters were investigated. Moreover, this helps to gain insights into the mechanisms underlying changes caused by external factors. These investigations were performed using a technique to induce dry eye in healthy normal individuals. This method facilitates the testing of dry eye products on a well-controlled and rapid screening system. Additionally, we aim to establish a method for inducing dry eye in healthy individuals to create a well-controlled and efficient screening system for testing dry eye products.
The efficiency of TSP/HA drops having properties of mucomimetic polymers was assessed in treating tear film disruption caused by a dry environment using two distinct usage modalities: “protection” when used before exposure to dry conditions and “relief” when used after exposure. Exposure to low humidity was shown to unfavourably disturb all tear film parameters except ocular surface temperature and tear osmolarity. A distinguished decline in tear osmolarity was detected when the participants were exposed to a dry environment. These alterations in tear parameters led to augmented ocular discomfort and dry eye symptoms in a desiccating environment. Previous studies have validated that hyaluronan polysaccharide helps to retain moisture in vitro by generating a sponge-like structure that traps water.5 Using TSP/HA before exposure (protection) may have allowed more time for an aqueous layer to integrate well with hyaluronan polysaccharide and enhance its capability to control the evaporation rate of tear film. Under dry conditions Therefore, in addition to mucomimetic properties, hyaluronic acid improves water-retention properties and can reduce evaporation.6 Tear hyperosmolarity is mainly induced by a reduction in tear volume that may result from either excessive evaporation or low lacrimal flow.7,8 At 5% RH a marked reduction in tear osmolarity (but not statistically significant, p=0.055) was observed. This effect was not seen when TSP/HA was used before exposure to a dry environment (protection).
The production of tears via the lacrimal gland does not necessarily correlate with environmental humidity. Instead, we highlight the importance of considering environmental factors that might indirectly influence tear production, such as air quality or indoor conditions. It has been noted that the lacrimal gland does not dynamically adjust tear production in response to changes in environmental humidity (particularly the basal tears).9 Tear production is primarily regulated by various factors, such as reflexes triggered by ocular surface irritation, emotional stimuli, and neural signals.10 The term Tear Production widely used in tear film studies is commonly used to refer to the overall amount and availability of tears rather than the production of tears by the lacrimal gland. This is performed by inserting a strip or thread into the lower fornix and measuring the wetting length while measuring the tears produced by the lacrimal gland, a technology such as a fluorophotometer that helps to estimate the tear production and turnover rate. The data on tear production showed that tear volume was not significantly affected at low RH when TSP/HA was used for protection and relief. In dry environments, the eye often responds to increased tear evaporation with a reflex tearing. While reflex tearing increases tear volume temporarily, it does not necessarily improve tear film quality or the homeostatic status of the ocular surface. This could explain the temporary increase in tear film volume after exposure to adverse environmental conditions. Moreover, the tear evaporation rate with TSP/HA in protection was significantly lower than when no TSP/HA was used. Barabino et al observed similar findings and reported that patients who underwent treatment with HA and TSP showed significant improvement in the OSDI score, reduced BUT and the extent of injury assessed by corneal and conjunctival staining. However Non-significant changes were recorded for the Schirmer test.11 Reflex tears typically have a different composition compared to the baseline tears that normally stabilize the tear film. In very dry environments, this type of tear production may be inefficient for maintaining a stable tear film, leading to continued symptoms of discomfort, dryness, and irritation. As production and evaporation of tear film were protected, it would be expected that no changes may happen to ocular surface homeostatic condition and therefore tear osmolarity. That explains the ability of TSP/HA in the protection method to maintain tear osmolarity during exposure to 5% RH at the same level as that seen at 40% RH. This study found that the instillation of TSP/HA using both treatment techniques improved ocular comfort and resulted in a significant reduction in total ocular discomfort score. The enhancement in ocular comfort could have resulted from the improvement in NITBUT and tear evaporation observed following the use of TSP/HA.12 This is in agreement with various previous studies showing a subjective benefit in the relief of symptoms of dry eye after using tear supplements containing TSP.13–15 These studies found that the instillation of TSP/HA using both treatment techniques improved ocular comfort and resulted in a significant reduction in total ocular discomfort score.
Although the small sample size may limit the ability to generalize the findings to a larger population, the result of the current study found significant changes in various parameters. However, in future investigations, it would be useful to evaluate the effect of the tear supplement with a larger sample size which may increase the statistical power of the analysis.
Study Limitation
The study was performed in controlled short-term environmental conditions with less number of participants. Several questions remain to be answered regarding the protection of tear film and the homeostasis status of the ocular surface under prolonged exposure to an adverse dry environment. A further study could assess the efficiency of tear film supplements among individuals who spend a long time in some workplaces characterized by low humidity such as aeroplane cabins or high-tech device factories, where the RH is less than 5%.
Conclusion
The application of TSP/HA eye drops resulted in a noticeable enhancement of the tear film parameters in dry environmental surroundings. The two treatment methods were found to be effective in addressing the issue. However, it was discovered that the use of TSP/HA for protective purposes provided greater benefits in terms of osmolarity and eye comfort compared to its use for relief. As a result, it is suggested that patients use TSP/HA on a preventive basis before being exposed to dry conditions, for instance, during commercial air travel, to achieve the utmost benefits.
Data Sharing Statement
All the relevant data has been provided in the manuscript. Datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval
The Glasgow Caledonian University Ethics Committee, Scotland, UK, approved the study (GCU1321/34/A). All subjects signed a consent form explaining the study procedures and requirements.
Acknowledgments
The authors extended their appreciation to the Researchers Supporting project number (RSPD2024R653), as King Saud University, Riyadh Saudi Arabia, for funding this project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The project was funded by the Researcher supporting project number (RSPD2024R653), King Saud University, Riyadh, Saudi Arabia.
Disclosure
The authors affirm that they have no competing interests.
References
1. Wolkoff P, Nojgaard JK, Troiano P, Piccoli B. Eye complaints in the office environment: precorneal tear film integrity influenced by eye blinking efficiency. Occup Environ Med. 2005;62(1):4–12. doi:10.1136/oem.2004.016030
2. Wolkoff P. “Healthy” eye in office-like environments. Environ Int. 2008;34(8):1204–1214. doi:10.1016/j.envint.2008.04.005
3. Nagda NL, Hodgson M. Low relative humidity and aircraft cabin air quality. Indoor Air. 2001;11(3):200–214. doi:10.1034/j.1600-0668.2001.011003200.x
4. Reinikainen LM, Jaakkola JJK, Heinonen OP. The effect of air humidification on different symptoms in office workers—an epidemiologic study. Environ Int. 1991;17(4):243–250. doi:10.1016/0160-4120(91)90009-F
5. Reinikainen LM, Sc D, Tech OS. The effect of air humidification on symptoms and perception of indoor air quality in office workers: a six-period cross-over trial. Arch Environ Health. 1992;47(1):8–15. doi:10.1080/00039896.1992.9935938
6. Wolkoff P, Kjaergaard SK. The dichotomy of relative humidity on indoor air quality. Environ Int. 2007;33(6):850–857. doi:10.1016/j.envint.2007.04.004
7. Pflugfelder SC, de Paiva CS. The pathophysiology of dry eye disease: what we know and future directions for research. Ophthalmology. 2017;124(11):S4–S13. doi:10.1016/j.ophtha.2017.07.010
8. Irimia T, Ghica MV, Popa L, Anuţa V, Arsene A-L, Dinu-Pîrvu C-E. Strategies for improving ocular drug bioavailability and corneal wound healing with chitosan-based delivery systems. Polymers. 2018;10(11):1221. doi:10.3390/polym10111221
9. Račić A, Krajišnik D. Biopolymers in mucoadhesive eye drops for treatment of dry eye and allergic conditions: application and perspectives. Pharmaceutics. 2023;15(2):470. doi:10.3390/pharmaceutics15020470
10. Račić A, Čalija B, Milić J, Milašinović N, Krajišnik D. Technology: development of polysaccharide-based mucoadhesive ophthalmic lubricating vehicles: the effect of different polymers on physicochemical properties and functionality. J Drug Deliv Sci Technol. 2019;49:50–57. doi:10.1016/j.jddst.2018.10.034
11. Dubashynskaya N, Poshina D, Raik S, Urtti A, Skorik YA. Polysaccharides in ocular drug delivery. Pharmaceutics. 2019;12(1):22. doi:10.3390/pharmaceutics12010022
12. Berezin A, Lomkova E, Skorik YA. Chitosan conjugates with biologically active compounds: design strategies, properties, and targeted drug delivery. Russ Chem Bull. 2012;61:781–795. doi:10.1007/s11172-012-0109-3
13. Tiwari S. Bahadur PJIjobm: modified hyaluronic acid based materials for biomedical applications. Int J Biol Macromol. 2019;121:556–571. doi:10.1016/j.ijbiomac.2018.10.049
14. Avachat AM, Shrotriya SN. Tamarind seed polysaccharide in novel drug delivery and biomedical applications. Polysaccharide Based Biomater. 2022;13:445.
15. de Castro MA, Prata WM, Cunha AS. Tamarind seed polysaccharide (TSP) uses in ophthalmic drug delivery. Revista de Ciências Farmacêuticas Básica e Aplicada. 2022;43:1–10.
16. Uccello-Barretta G, Nazzi S, Balzano F, Sansò M. A nuclear magnetic resonance approach to the comparison of mucoadhesive properties of polysaccharides for ophthalmic uses. Int J Pharm. 2011;406(1–2):78–83. doi:10.1016/j.ijpharm.2010.12.032
17. Uccello-Barretta G, Nazzi S, Zambito Y, Di Colo G, Balzano F, Sansò M. Synergistic interaction between TS-polysaccharide and hyaluronic acid: implications in the formulation of eye drops. Int J Pharm. 2010;395(1–2):122–131. doi:10.1016/j.ijpharm.2010.05.031
18. Di Colo G, Zambito Y, Zaino C, Sansò M. Selected polysaccharides at comparison for their mucoadhesiveness and effect on precorneal residence of different drugs in the rabbit model. Drug Dev Ind Pharm. 2009;35(8):941–949. doi:10.1080/03639040802713460
19. Lehr CM, Lee YH, Lee VHL. Improved ocular penetration of gentamicin by mucoadhesive polymer polycarbophil in the pigmented rabbit. Invest Ophthalmol Vis Sci. 1994;35(6):2809–2814.
20. Zhang X, Wei D, Xu Y, Zhu Q. Hyaluronic acid in ocular drug delivery. Carbohydr Polym. 2021;264:118006. doi:10.1016/j.carbpol.2021.118006
21. Marinho A, Nunes C, Reis S. Hyaluronic acid: a key ingredient in the therapy of inflammation. Biomolecules. 2021;11(10):1518. doi:10.3390/biom11101518
22. Aragona P, Di Stefano G, Ferreri F, Spinella R, Stilo A. Sodium hyaluronate eye drops of different osmolarity for the treatment of dry eye in Sjogren’s syndrome patients. Br J Ophthalmol. 2002;86(8):879–884. doi:10.1136/bjo.86.8.879
23. Prabhasawat P, Tesavibul N, Kasetsuwan N. Performance profile of sodium hyaluronate in patients with lipid tear deficiency: randomised, double-blind, controlled, exploratory study. Br J Ophthalmol. 2007;91(1):47–50. doi:10.1136/bjo.2006.097691
24. Johnson ME, Murphy PJ, Boulton M. Effectiveness of sodium hyaluronate eyedrops in the treatment of dry eye. Graefes Arch Clin Exp Ophthalmol. 2006;244(1):109–112. doi:10.1007/s00417-005-0028-1
25. Arshinoff SA, Hofmann I, Nae H. Surgery R: role of rheology in tears and artificial tears. J Cataract Refract Surg. 2021;47(5):655–661.
26. Gomes J, Amankwah R, Powell-Richards A, Dua H. Sodium hyaluronate (hyaluronic acid) promotes migration of human corneal epithelial cells in vitro. Br J Ophthalmol. 2004;88(6):821–825. doi:10.1136/bjo.2003.027573
27. Nishida T, Nakamura M, Mishima H, Otori T. Hyaluronan stimulates corneal epithelial migration. Exp Eye Res. 1991;53(6):753–758. doi:10.1016/0014-4835(91)90110-Z
28. Versura P, Profazio V, Balducci N, Campos EC. Efficacy of two-month treatment with Xiloial eyedrops for discomfort from disposable soft contact lenses. Clin Ophthalmol. 2010;4:1035–1041. doi:10.2147/OPTH.S10448
29. Rolando M, Valente C. Establishing the tolerability and performance of tamarind seed polysaccharide (TSP) in treating dry eye syndrome: results of a clinical study. BMC Ophthalmol. 2007;7(1):5. doi:10.1186/1471-2415-7-5
30. Wadhwa S, Paliwal R, Paliwal SR, Vyas SP. Hyaluronic acid modified chitosan nanoparticles for effective management of glaucoma: development, characterization, and evaluation. J Drug Targeting. 2010;18(4):292–302. doi:10.3109/10611860903450023
31. Shrestha B, Dunn L. The declaration of Helsinki on medical research involving human subjects: a review of seventh revision. J Nepal Health Res Counc. 2019;17(4):548–552.
32. Madden LC, Tomlinson A, Simmons PA. Effect of humidity variations in a controlled environment chamber on tear evaporation after dry eye therapy. Eye Contact Lens. 2013;39(2):169–174. doi:10.1097/ICL.0b013e318283dfc6
33. Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the ocular surface disease index. Arch Ophthalmol. 2000;118(5):615–621. doi:10.1001/archopht.118.5.615
34. Abusharha A, Pearce IE, Afsar T, Razak S. Evaluation of therapeutic capability of emustil drops against tear film complications under dry environmental conditions in healthy individuals. Medicina. 2023;59(7):1298. doi:10.3390/medicina59071298
35. Abusharha A, Pearce IE, Afsar T, Alsaqr A, Fagehi R, Razak S. Evaluation of different treatment modalities on the efficacy of hydroxypropyl Guar (HP-Guar) formulation on tear film stability (TFS) in subjects exposed to adverse environmental conditions. BMC Ophthalmol. 2023;23(1):226. doi:10.1186/s12886-023-02977-3
36. Nichols KK, Nichols JJ, Mitchell GL. The reliability and validity of McMonnies dry eye index. Cornea. 2004;23(4):365. doi:10.1097/00003226-200405000-00010
37. Abusharha AA, Pearce EI. The effect of low humidity on the human tear film. Cornea. 2012;32(4):429–434. doi:10.1097/ICO.0b013e31826671ab
38. Morgan PB, Soh MP, Efron N, Tullo AB. Potential applications of ocular thermography. Optom Vis Sci. 1993;70(7):568–576. doi:10.1097/00006324-199307000-00008
39. Tan JH, Ng EYK, Acharya UR, Chee C. Infrared thermography on ocular surface temperature: a review. Infrared Phys Technol. 2009;52(4):97–108. doi:10.1016/j.infrared.2009.05.002
40. Steketee J. Spectral emissivity of skin and pericardium. Phys Med Biol. 1973;18:686. doi:10.1088/0031-9155/18/5/307
41. Rysa P, Sarvaranta J. Corneal temperature in man and rabbit. Observations made using an infra-red camera and a cold chamber. Acta Ophthalmol. 1974;52(6):810–816. doi:10.1111/j.1755-3768.1974.tb01117.x
42. Purslow C: Dynamic ocular thermography: [PhD thesis]. Birmingham: Aston University; 2005.
43. Tomlinson A, McCann LC, Pearce EI. Comparison of human tear film osmolarity measured by electrical impedance and freezing point depression techniques. Cornea. 2010;29(9):1036–1041. doi:10.1097/ICO.0b013e3181cd9a1d
44. Tomlinson A, Khanal S, Ramaesh K, Diaper C, McFadyen A. Tear film osmolarity: determination of a referent for dry eye diagnosis. Invest Ophthalmol Vis Sci. 2006;47(10):4309–4315. doi:10.1167/iovs.05-1504
45. Winebrake J, Drinkwater O, Brissette A. The TFOS dry eye workshop II: key updates. Ophthalmic Pearls. 2017.
46. Dartt DA. Dysfunctional neural regulation of lacrimal gland secretion and its role in the pathogenesis of dry eye syndromes. Ocular Surf. 2004;2(2):76–91. doi:10.1016/S1542-0124(12)70146-5
47. Tomlinson A, Doane MG, McFadyen A. Inputs and outputs of the lacrimal system: review of production and evaporative loss. Ocul Surf. 2009;7(4):186–198.
48. Hamano H, Hori M, Hamano T, et al. A new method for measuring tears. CLAO J. 1983;9(3):281–289.
49. Sakamoto R, Bennett ES, Henry VA, et al. The phenol red thread tear test: a cross-cultural study. Invest Ophthalmol Vis Sci. 1993;34(13):3510–3514.
50. Abusharha A, Pearce EI, Afsar T, Razak S. Protecting tear-film stability under adverse environmental conditions using a mucomimetic with a non-Newtonian viscosity agent. Medicina. 2023;59(10):1862. doi:10.3390/medicina59101862
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.