")
Back to Journals » International Journal of Women's Health » Volume 17
Association Between Depression Severity and Ovarian Cancer Among American Women: A Cross-Sectional Study
Authors Yang L , Zhang S, Li Y, Qian H, Xu W , Yu J
Received 1 February 2025
Accepted for publication 5 July 2025
Published 18 July 2025 Volume 2025:17 Pages 2145—2155
DOI https://doi.org/10.2147/IJWH.S520260
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Li Yang,1,* Shuang Zhang,1,* Yajun Li,2 Haiqing Qian,3 Wenting Xu,3 Jinfen Yu1
1Department of Obstetrics and Gynaecology, Zhangjiagang TCM Hospital Affiliated to Nanjing University of Chinese Medicine, Zhangjiagang, Jiangsu, People’s Republic of China; 2Department of Orthopedics, Zhangjiagang TCM Hospital Affiliated to Nanjing University of Chinese Medicine, Zhangjiagang, Jiangsu, People’s Republic of China; 3Department of Reproduction, Zhangjiagang TCM Hospital Affiliated to Nanjing University of Chinese Medicine, Zhangjiagang, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinfen Yu, Email [email protected] Wenting Xu, Email [email protected]
Objective: Inflammation is one of the main causes of ovarian cancer. Depression leads to an increase in pro-inflammatory cytokines, which in turn affects the progression and severity of cancer. There is a lack of research on the relationship between depression severity and ovarian cancer. This study aimed to explore the relationship between depression severity and ovarian cancer.
Methods: The study used data from seven cycles of the National Health and Nutrition Examination Survey (NHANES, 2005– 2018). Weighted multivariable logistic regression models were used to analyze the association between depression severity and ovarian cancer.
Results: A total of 14,843 women without cancer and 56 women only with ovarian cancer were included in this study. Weighted multivariable logistic regression models showed that severe depression was associated with ovarian cancer (unadjusted model, OR: 4.94, 95% CI: 1.14, 21.35, p < 0.05, p for trend: 0.1; partially adjusted model, OR: 6.10, 95% CI: 1.35, 27.51, p < 0.05, p for trend: 0.04; fully adjusted model, OR: 5.82, 95% CI: 1.19, 28.52, p < 0.05, p for trend: 0.05).
Conclusion: Severe depression was positively correlated with ovarian cancer. Longitudinal studies are necessary to explore causality.
Keywords: ovarian cancer, depression severity, cross-sectional study, NHANES, PHQ-9
Introduction
Ovarian cancer is a common gynecological malignant tumor and the risk of ovarian cancer death increases significantly after the age of 45.1 Ovarian cancer accounts for 2.5% of cancers in women and is the deadliest of gynecologic cancers.2 Ovarian cancer represents 1.0% of all new cancer cases in the United States.3 The rate of new cases of ovarian cancer was 10.2 per 100,000 women per year based on 2017–2021 cases, age-adjusted.3 Ovarian cancer is the fourteenth leading cause of cancer death in the United States.3 The earlier ovarian cancer is caught, the better chance a person has of surviving five years after being diagnosed.3 The global burden of ovarian cancer is still increasing, especially in less developed regions and the elderly.4 Moreover, the cost of the late stage is much higher than that of the early stage, increasing the physical and mental burden of patients.5,6 At present, the common treatments for ovarian cancer include surgery, chemotherapy, immunotherapy, targeted therapy and adjuvant therapy of traditional Chinese medicine (TCM).7–9 However, due to its high degree of malignancy, the survival rate cannot meet people’s expectations. Studies have shown that early menarche, late menopause, tobacco, family history of ovarian cancer and breast cancer, and Lynch syndrome increase women’s risk of ovarian cancer.10,11 It is well known that inflammation is one of the main causes of ovarian cancer.12 Women who consume more pro-inflammatory diets have a higher risk of ovarian cancer.13 Patients with a higher inflammation-related risk score(IRRS) before the diagnosis of ovarian cancer have a significantly higher mortality rate after diagnosis.14 The inflammatory response induced under physiological conditions may promote the development of epithelial ovarian cancer.15 Inflammation seems to have an impact on the occurrence, promotion, and progression of tumors.15 IL-6 is the main cytokine involved in the occurrence and development of epithelial ovarian cancer.15 The mechanism of action of anti-IL-6 in ovarian cancer is to inhibit the autocrine cytokine and chemokine networks in malignant cells.15
There is a strong correlation between emotion and health.16 With the increasing pressure of life and work, women’s mental health has been greatly affected. Depression is a common factor affecting women’s physical and mental health, and the prevalence rate among the elderly is 28.4%.17 Psychological and social stress can stimulate inflammatory signaling molecules.18 The inflammatory process plays an important role in the pathogenesis of depression.19 IL-6 has been consistently found to be elevated in patients with depression.19 The activation of the hypothalamic–pituitary–adrenal (HPA) axis in depression and the release of mediators during chronic stress suppress some non-specific and specific parts of the immune response, including NK cell activity, phagocytosis, production of inflammatory cytokines, and cytotoxic T cell activity, and may promote the occurrence and development of certain types of cancer.20 A study involving 698 patients with epithelial ovarian cancer showed that depression assessed 2–4 years before the diagnosis of ovarian cancer was associated with a slightly higher incidence rate of ovarian cancer (HR=1.30, 95% CI 1.05–1.60).21 A 24-year follow-up of the Baltimore Epidemiological Catchment Area sample showed that severe depression was associated with a higher overall cancer risk (HR: 1.9, 95% CI: 1.2, 3.0).22 The study on the relationship between depression and gynecological cancers in the NHANES database (2009–2018) showed a positive correlation between depression and ovarian cancer (n=48), but unfortunately, this study did not conduct a weighted analysis.23 It is worth exploring whether the severity of depression is closely related to the risk of ovarian cancer.
NHANES provides large-scale information on population, health, diet, laboratory, and physical conditions, providing a solid data foundation for studying the influencing factors of health issues. In addition, NHANES adopts a multi-stage probability sampling method to ensure the representativeness of the sample. The purpose of this study was to explore the relationship between depression severity and ovarian cancer in American women and to provide guidance for the prevention and treatment of ovarian cancer.
Materials and Methods
Study Design and Population
CDC’s National Center for Health Statistics (NCHS) conducts the National Health and Nutrition Examination Survey (NHANES).24 NHANES is a national survey that measures the health and nutrition of adults and children in the United States.24 NHANES is the only national health survey that includes health exams, laboratory tests, and dietary interviews for participants of all ages.24 After 1999, it became a continuity plan with approximately 5000 participants participating each year. All data in this study were from the NHANES database, including seven survey cycles from 2005 to 2018.
Among the initially extracted 70,190 participants, the exclusion criteria were as follows: (1) male participants (n=34,709); (2) did not answer the nine questions about depression assessment in the Patient Health Questionnaire (PHQ-9) and could not determine the specific range of their total score (n=17,004); (3) lack of cancer information (n=1062); (4) participants with ovarian cancer and other cancers or only other cancers (n=1685); and (5) lack of information on education, smoking, alcohol drinking, the routine place to go for healthcare, general health condition, health insurance, ever been pregnant, BMI, marital status, age at menarche (n=831).
Finally, 14,899 women were included in the study. A total of 14,843 women without cancer and 56 women only with ovarian cancer were included in this study. All participants signed informed consent forms.
Dependent Variable
Ovarian cancer was determined based on the medical conditions, where MCQ220 asked, “Have you ever been told by a doctor or other health professional that you had cancer or a malignancy of any kind?” and MCQ230A, MCQ230B, MCQ230C asked, “What kind of cancer was it?”. Participants who answered only ovarian cancer were categorized as the ovarian cancer group. If participants answered no on MCQ220, they were included in the population without ovarian cancer.
Independent Variable
The nine questions about depression assessment were from the Patient Health Questionnaire (PHQ-9) and questions were based on the nine DSM-IV signs and symptoms of depression. Each question was scored from “0” (not at all) to “3” (nearly every day). The diagnostic effectiveness of PHQ-9 was comparable to that of PRIME-MD used by original clinicians and was more efficient to use.25 Moreover, the PHQ-9 produced an index of the severity of depressive symptoms.25 The PHQ-9 score was divided into the following categories of increasing severity: None: 0–4points, Mild: 5–9points, Moderate: 10–14points, Moderately severe: 15–19points, and Severe: 20–27points.26
Covariates
In this study, covariates included age, race, education, marital status, poverty income ratio (PIR), age at menarche, ever been pregnant, smoking, alcohol drinking, general health condition, the routine place to go for healthcare, health insurance, and BMI.
The above covariates were derived from demographics, reproductive Health, hospital utilization and access to care, smoking, alcohol drinking, health insurance, and body measurement questionnaires of the NHANES database.
Smoking status was divided into three categories: never: smoked less than 100 cigarettes in life; former: smoked more than 100 cigarettes in life and smoke not at all now; now: smoked moth than 100 cigarettes in life and smoke some days or every day. The degree of alcohol drinking was divided into five categories: heavy:≥3 drinks per day for females; moderate:≥2 drinks per day for females; mild: not meat the above; former; never. The Poverty income ratio (PIR) was divided into two categories: <5; ≥5. BMI was divided into four categories: low weight: <18.5; normal weight: 18.5–25.0; overweight: 25.0–30.0; obesity: ≥30.0. Age at menarche was divided into three categories: <11; 11–16; >16. General health condition was divided into two categories: good; poor.
All the data of this study were available publicly on the NHANES website (https://wwwn.cdc.gov/nchs/nhanes/Default.aspx).
Statistical Analysis
The data of this study were from seven cycles (2005–2018) in the NHANES database. All analyses were weighted by one seventh of wtmec2yr. In the general data table, the continuous variables were represented by weighted mean (weighted standard error), and the categorical variables were represented by the weighted percentage. Weighted univariable and weighted multivariable logistic regression were used to analyze the association between depression severity and ovarian cancer. The results were expressed as OR (95% CI). This study established three logistic regression models to analyze the correlation between depression severity and ovarian cancer. Model 1 was a crude model. Model 2 was adjusted for variables found to be significant in the univariate logistic regression analysis and Clinically relevant, for example age at menarche. Model 3 was adjusted for age, race, marital status, poverty income ratio, age at menarche, education, BMI, ever been pregnant, smoking status, degree of alcohol drinking, general health condition, the routine place to go for healthcare, and health insurance. All statistical analyses were R software (version 4.2.2). A p-value < 0.05 was considered statistically significant.
Results
Weighted Characteristics of Participants
A total of 14,843 women without cancer and 56 women only with ovarian cancer were included in this study (Table 1). The weighted number of ovarian cancer patients was 311,166. There were significant differences in age, marital status, and PIR between women with ovarian cancer and women without cancer (p<0.0001, p<0.010, p<0.018) (Table 1).
 |
Table 1 Weighted Characteristics of Participants: NHANES 2005–2018 |
Weighted Univariable Analysis for the Prevalence of Ovarian Cancer
Univariable logistic regression analysis showed that increasing age was significantly associated with ovarian cancer (OR: 1.05, 95% CI: 1.03, 1.06) (Table 2). Mexican American was highly associated with ovarian cancer (OR: 2.71, 95% CI: 1.04, 7.06) (Table 2). Never married was highly associated with ovarian cancer (OR: 0.21, 95% CI: 0.06, 0.77) (Table 2). Severe depression was highly associated with ovarian cancer (OR: 4.94, 95% CI: 1.14, 21.35) (Table 2).
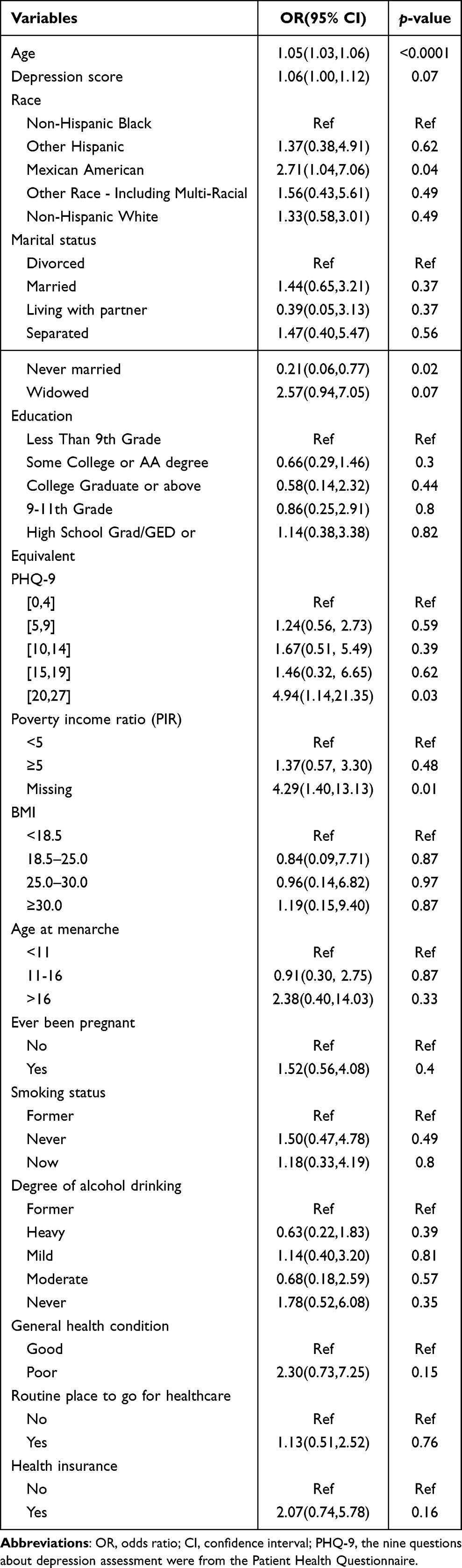 |
Table 2 Univariable Analysis for the Prevalence of Ovarian Cancer (Weighted) |
Association Between Depression Severity and Ovarian Cancer
Table 3 presented weighted multivariable logistic regression models between depression severity and ovarian cancer. Model 1 was not adjusted, and the results showed that severe depression was associated with ovarian cancer (OR: 4.94, 95% CI: 1.14, 21.35, p < 0.05, p for trend: 0.1). Model 2 was adjusted for age, race, marital status, PIR, age at menarche. Severe depression was positively correlated with ovarian cancer (OR: 6.10, 95% CI: 1.35, 27.51, p < 0.05, p for trend: 0.04). Model 3 was adjusted for age, race, marital status, PIR, age at menarche, education, BMI, ever been pregnant, smoking status, degree of alcohol drinking, general health condition, the routine place to go for healthcare, and health insurance. Severe depression was positively correlated with ovarian cancer (OR: 5.82, 95% CI: 1.19, 28.52, p < 0.05, p for trend: 0.05).
 |
Table 3 Association Between Depression Severity and Ovarian Cancer in the Database From NHANES 2005–2018 (Weighted) |
Discussion
This study found the relationship between depression severity and ovarian cancer by analyzing the nutrition and health data of the American population summarized in the NHANES database from 2005 to 2018. The results showed that severe depression was positively correlated with ovarian cancer in unadjusted, partially adjusted and fully adjusted models. However, the fully adjusted model indicated that there was no linear trend between them.
Depression is a global public health problem that plagues more than 300 million people.27 It is estimated that major depression costs Australia up to A$12 billion per year.28 Depression is often not diagnosed and treated effectively due to inadequate mental health resources, stigma, etc., resulting in a relatively low incidence.27 It is estimated that more than 75% of depressed people in low- and middle-income countries do not receive treatment.29 Depression is a risk factor for mortality, and major depression is closely related to greater mortality.30 Major depression is a serious mental illness.31 It is often accompanied by cancer, which will seriously affect human life expectancy.31 Our study found a positive correlation between severe depression and ovarian cancer. However, the broad confidence intervals and marginal p-values (eg, p for trend =0.05) suggested that the strength of this association was limited.
Inflammatory diseases of the nervous system, cytokine therapy, and elevated inflammatory markers were all closely related to Major depressive disorder (MDD).32 A meta-analysis showed that inflammation (measured by CRP or IL-6) predicted future depression.33 Inflammation might not only be the cause of depression, but also a factor hindering rehabilitation.32 A Mendelian randomization study suggested that the effects of increased soluble interleukin-6 receptor (sIL-6R) had a causal relationship with depression.34 The levels of C-reactive protein (CRP), interleukin-6 (IL-6) and other inflammatory factors in depression patients would increase, and their depressive symptoms were closely related to the increase of interleukin (IL)-1 receptor antagonist (RA).35,36 Studies showed that levels of inflammatory factors were significantly increased in ovarian cancer and they were closely related to the increased risk of ovarian cancer.37,38 There was direct evidence that inflammatory markers might be associated with the risk of epithelial ovarian cancer, and additional evidence suggested that inflammation was involved in the development of the disease.39 Among them, IL-6 played an important role in ovarian cancer metastasis through different signaling pathways involved in tumor metastasis, proliferation, and angiogenesis.40 At the same time, animal experiments confirmed that ovarian cancer cells were mainly planted in the surgical incision site, indicating that inflammation is the key to tumor cell planting.41 A meta-analysis suggested that antipsychotic use increased the risk of gynecological diseases.42 However, a case-control study showed that the use of selective serotonin reuptake inhibitors was associated with a decreased risk of ovarian cancer (OR, 0.85; 95% CI, 0.74–0.96).43 Depression can stimulate the elevation of IL-6 and TNF-α, increasing the risk of tumor progression and recurrence.44 Our study found a positive correlation between severe depression and ovarian cancer. Depression that occurs before cancer diagnosis indicates that depression is not just a sad response to diseases with poor prognosis.45 Depression before diagnosis of ovarian cancer might influence ovarian cancer outcomes through changes in the tumor immune microenvironment.46 A meta-analysis suggested that depression was an independent risk factor for cancer mortality.47 A prospective study showed that the mortality of patients diagnosed with depression before the diagnosis of ovarian cancer increased, suggesting that there was a certain correlation between depression and ovarian cancer mortality.48 A deficiency in the neurotransmitters (serotonin, norepinephrine, and dopamine) was linked to depression.45,49 However, we were unable to find the corresponding serological values on the NHANES official website. The greater BMI, waist circumference, and fat mass were consistent with the hyperphagia that distinguished atypical depression.50 Further adjusting lifestyle factors, especially BMI, but depression was still moderately associated with an increased risk of ovarian cancer (HR=1.26; 95% CI: 1.02, 1.56).21 A study showed an increased risk of ovarian cancer in women with persistent positive depressive states (HR=1.34; 95% CI: 1.01, 1.76).21 The study on the relationship between depression and gynecological cancers in the NHANES database (2009–2018) showed a positive correlation between depression and ovarian cancer (n=48), but unfortunately, this study did not conduct a weighted analysis.23 The official website of NHANES indicates that unweighted estimates may differ significantly from appropriately weighted estimates. Sample weights must be used to calculate estimates representing the non institutionalized population of American civilians.51 But all analyses in our study were weighted, and the results were more authentic. Depression can affect the physical and mental health of patients. Women with ovarian cancer are prone to depression. There is a certain correlation between them. Therefore, for women with cancer and depression, when necessary, gynecology and psychiatry departments can cooperate to provide patients with more suitable treatment options.52 In this study, PHQ-9 was used to score depressive symptoms and to classify the degree of depression, which was beneficial for the subsequent treatment of different degrees of depression. The results were more representative by a weighted analysis that expanded the number of ovarian cancer patients. By studying the relationship between depression and ovarian cancer, people pay more attention to the impact of psychological factors on human health, which is more in line with the “biological-psychological-social” medical model.
However, this study also had some limitations. The study was cross-sectional and could not determine a cause-and-effect relationship between depression and ovarian cancer. Longitudinal studies are necessary to explore causality between depression severity and ovarian cancer. Relying on questionnaire survey data might lead to recall and reporting biases. Besides, there were still some residual confounding factors such as medication use, treatment history, or psychological comorbidities that were not included, which were limitations of this study. In addition, this study could not study different types of ovarian cancer in detail.
Conclusion
In conclusion, the finding showed that severe depression was positively correlated with ovarian cancer in a nationally representative sample. The results provided novelty in the area of ovarian cancer surveillance especially among women with tendency for depression. Women with severe depression should pay more attention to psychological counseling and regularly screen for tumor indicators and gynecological ultrasound. The impact of psychosocial factors on cancer development is significant, and interventions for treating women with depression may enrich current prevention strategies for ovarian cancer. However, the broad confidence intervals reflect limited power. Longitudinal studies are necessary to explore causality. Include medication use, Treatment history and psychological comorbidities in future research may be more meaningful for the results.
Abbreviations
NHANES, National Health and Nutrition Examination Survey; TCM, traditional Chinese medicine; IRRS, inflammation-related risk score; PHQ, Patient Health Questionnaire; PIR, poverty income ratio; MDD, Major depressive disorder; sIL-6R, soluble interleukin-6 receptor; CRP, C-reactive protein; IL-6, interleukin-6; RA, receptor antagonist; OR, odds ratio; CI, confidence interval; BMI, body mass index.
Data Sharing Statement
All the data of this study were available publicly on the NHANES website (https://wwwn.cdc.gov/nchs/nhanes/Default.aspx).
Ethics Declarations
The National Health and Nutrition Examination Survey was approved by the National Center for Health Statistics Research Ethics Review Board (https://www.cdc.gov/nchs/nhanes/irba98.htm). The patients/participants provided their written informed consent to participate in this study. The study received ethical approval from the Ethics Committee of Zhangjiagang TCM Hospital Affiliated to Nanjing University of Chinese Medicine (approval number: KY2024SZK0123).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Gusu Health Talent Plan Research Project (No. GSWS2023016); the Science and Technology Development Plan of Suzhou (No. SLT2022012, SKYD2022010); School-Land Collaborative Innovation Research Project of Jiangsu Pharmaceutical Vocational College (No.20239602); and the Youth Natural Science Foundation of Zhangjiagang TCM Hospital Affiliated to Nanjing University of Chinese Medicine (No. ZZYQ2206).
Disclosure
Li Yang and Shuang Zhang are co-first authors for this study. The authors declare no competing interests in this work. The authors also confirm that there are no funding sources or affiliations that may influence the design, analysis, or interpretation of the research.
References
1. Wang Z, Guo E, Yang B, et al. Trends and age-period-cohort effects on mortality of the three major gynecologic cancers in China from 1990 to 2019: cervical, ovarian and uterine cancer. Gynecol Oncol. 2021;163(2):358–363. doi:10.1016/j.ygyno.2021.08.029
2. Ovarian Cancer Research Alliance. Statistics. Available from: https://ocrahope.org/patients/about-ovarian-cancer/statistics/.
3. National Cancer Institute. Surveillance, epidemiology, and end results program. cancer stat facts: ovarian cancer. Available from: https://seer.cancer.gov/statfacts/html/ovary.html.
4. Zhang S, Cheng C, Lin Z, et al. The global burden and associated factors of ovarian cancer in 1990-2019: findings from the global burden of disease study 2019. BMC Public Health. 2022;22(1):1455. doi:10.1186/s12889-022-13861-y
5. Palmqvist C, Persson J, Albertsson P, Dahm-Kähler P, Johansson M. Societal costs of ovarian cancer in a population-based cohort - a cost of illness analysis. Acta Oncol. 2022;61(11):1369–1376. doi:10.1080/0284186X.2022.2140015
6. Shim EJ, Hahm BJ, Yu ES, et al. Prevalence, correlates, and impact of depressive and anxiety disorder in cancer: findings from a multicenter study. Palliat Support Care. 2018;16(5):552–565. doi:10.1017/S1478951517000736
7. Yang C, Xia BR, Zhang ZC, Zhang YJ, Lou G, Jin WL. Immunotherapy for ovarian cancer: adjuvant, combination, and neoadjuvant. Front Immunol. 2020;11:577869. doi:10.3389/fimmu.2020.577869
8. Ding H, Zhang J, Zhang F, Xu Y, Liang W, Yu Y. Nanotechnological approaches for diagnosis and treatment of ovarian cancer: a review of recent trends. Drug Deliv. 2022;29(1):3218–3232. doi:10.1080/10717544.2022.2132032
9. Wang X, Su P, Hao Q, Zhang X, Xia L, Zhang Y. A Chinese classical prescription Guizhi-Fuling Wan in treatment of ovarian cancer: an overview. Biomed Pharmacother. 2022;153:113401. doi:10.1016/j.biopha.2022.113401
10. La Vecchia C. Ovarian cancer: epidemiology and risk factors. Eur J Cancer Prev. 2017;26(1):55–62. doi:10.1097/CEJ.0000000000000217
11. Stewart C, Ralyea C, Lockwood S. Ovarian cancer: an integrated review. Semin Oncol Nurs. 2019;35(2):151–156. doi:10.1016/j.soncn.2019.02.001
12. Sharma T, Banerjee BD, Thakur GK, Guleria K, Mazumdar D. Polymorphism of xenobiotic metabolizing gene and susceptibility of epithelial ovarian cancer with reference to organochlorine pesticides exposure. Exp Biol Med. 2019;244(16):1446–1453. doi:10.1177/1535370219878652
13. Yang J, Ma J, Jin Y, Cheng S, Huang S, Wang Y. Dietary inflammatory index and ovarian cancer risk: a meta-analysis. Nutr Cancer. 2022;74(3):796–805. doi:10.1080/01635581.2021.1931366
14. Brieger KK, Phung MT, Mukherjee B, et al. Ovarian cancer association consortium. high prediagnosis inflammation-related risk score associated with decreased ovarian cancer survival. Cancer Epidemiol Biomarkers Prev. 2022;31(2):443–452. doi:10.1158/1055-9965.EPI-21-0977
15. Macciò A, Madeddu C. Inflammation and ovarian cancer. Cytokine. 2012;58(2):133–147. doi:10.1016/j.cyto.2012.01.015
16. Smith TW, Weihs K. Emotion, social relationships, and physical health: concepts, methods, and evidence for an integrative perspective. Psychosom Med. 2019;81(8):681–693. doi:10.1097/PSY.0000000000000739
17. Hu T, Zhao X, Wu M, et al. Prevalence of depression in older adults: a systematic review and meta-analysis. Psychiatry Res. 2022;311:114511. doi:10.1016/j.psychres.2022.114511
18. Miller AH, Maletic V, Raison CL. Inflammation and its discontents: the role of cytokines in the pathophysiology of major depression. Biol Psychiatry. 2009;65(9):732–741. doi:10.1016/j.biopsych.2008.11.029
19. Ting EY, Yang AC, Tsai SJ. Role of interleukin-6 in depressive disorder. Int J Mol Sci. 2020;21(6):2194. doi:10.3390/ijms21062194
20. Reiche EM, Nunes SO, Morimoto HK. Stress, depression, the immune system, and cancer. Lancet Oncol. 2004;5(10):617–625. doi:10.1016/S1470-2045(04)01597-9
21. Huang T, Poole EM, Okereke OI, et al. Depression and risk of epithelial ovarian cancer: results from two large prospective cohort studies. Gynecol Oncol. 2015;139(3):481–486. doi:10.1016/j.ygyno.2015.10.004
22. Gross AL, Gallo JJ, Eaton WW. Depression and cancer risk: 24 years of follow-up of the Baltimore epidemiologic catchment area sample. Cancer Causes Control. 2010;21(2):191–199. doi:10.1007/s10552-009-9449-1
23. Wang C, Xu J, Li X, Jiang L. Depression as a risk factor for gynecological cancers: evidence from NHANES data. Int J Womens Health. 2025;17:615–625. doi:10.2147/IJWH.S504049
24. National Center for Health Statistics. Available from: https://www.cdc.gov/nchs/nhanes/about/?CDC_AAref_Val=https://www.cdc.gov/nchs/nhanes/about_nhanes.htm.
25. Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. JAMA. 1999;282(18):1737–1744. doi:10.1001/jama.282.18.1737
26. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
27. Smith K. Mental health: a world of depression. Nature. 2014;515(7526):181. doi:10.1038/515180a
28. McCallum SM, Batterham PJ, Calear AL, Sunderland M, Carragher N. Reductions in quality of life and increased economic burden associated with mental disorders in an Australian adult sample. Aust Health Rev. 2019;43(6):644–652. doi:10.1071/AH16276
29. World Health Organization. Available from: https://www.who.int/health-topics/depression#tab=tab_1.
30. Xia W, Jiang H, Di H, et al. Association between self-reported depression and risk of all-cause mortality and cause-specific mortality. J Affect Disord. 2022;299:353–358. doi:10.1016/j.jad.2021.12.018
31. Nemeroff CB. The state of our understanding of the pathophysiology and optimal treatment of depression: glass half full or half empty? Am J Psychiatry. 2020;177(8):671–685. doi:10.1176/appi.ajp.2020.20060845
32. Krishnadas R, Cavanagh J. Depression: an inflammatory illness? J Neurol Neurosurg Psychiatry. 2012;83(5):495–502. doi:10.1136/jnnp-2011-301779
33. Colasanto M, Madigan S, Korczak DJ. Depression and inflammation among children and adolescents: a meta-analysis. J Affect Disord. 2020;277:940–948. doi:10.1016/j.jad.2020.09.025
34. Kelly KM, Smith JA, Mezuk B. Depression and interleukin-6 signaling: a Mendelian randomization study. Brain Behav Immun. 2021;95:106–114. doi:10.1016/j.bbi.2021.02.019
35. Osimo EF, Pillinger T, Rodriguez IM, Khandaker GM, Pariante CM, Howes OD. Inflammatory markers in depression: a meta-analysis of mean differences and variability in 5166 patients and 5083 controls. Brain Behav Immun. 2020;87:901–909. doi:10.1016/j.bbi.2020.02.010
36. Lehto SM, Niskanen L, Miettola J, Tolmunen T, Viinamäki H, Mäntyselkä P. Serum anti-inflammatory markers in general population subjects with elevated depressive symptoms. Neurosci Lett. 2010;484(3):201–205. doi:10.1016/j.neulet.2010.08.054
37. Li H, Sun L, Chen L, Kang Z, Hao G, Bai F. Effects of adiponectin, plasma D-dimer, inflammation and tumor markers on clinical characteristics and prognosis of patients with ovarian cancer. J Med Biochem. 2022;41(1):71–78. doi:10.5937/jomb0-26452
38. Michels N, van Aart C, Morisse J, Mullee A, Huybrechts I. Chronic inflammation towards cancer incidence: a systematic review and meta-analysis of epidemiological studies. Crit Rev Oncol Hematol. 2021;157:103177. doi:10.1016/j.critrevonc.2020.103177
39. Clendenen TV, Lundin E, Zeleniuch-Jacquotte A, et al. Circulating inflammation markers and risk of epithelial ovarian cancer. Cancer Epidemiol Biomarkers Prev. 2011;20(5):799–810. doi:10.1158/1055-9965.EPI-10-1180
40. Browning L, Patel MR, Horvath EB, Tawara K, Jorcyk CL. IL-6 and ovarian cancer: inflammatory cytokines in promotion of metastasis. Cancer Manag Res. 2018;10:6685–6693. doi:10.2147/CMAR.S179189
41. Jia D, Nagaoka Y, Katsumata M, Orsulic S. Inflammation is a key contributor to ovarian cancer cell seeding. Sci Rep. 2018;8(1):12394. doi:10.1038/s41598-018-30261-8
42. de Moraes FCA, Sudo RYU, Souza MEC, Fernandes MR, Dos Santos NPC. The incidence risk of gynecological cancer by antipsychotic use: a meta-analysis of 50,402 patients. BMC Cancer. 2024;24(1):712. doi:10.1186/s12885-024-12481-6
43. Mørch LS, Dehlendorff C, Baandrup L, Friis S, Kjaer SK. Use of antidepressants and risk of epithelial ovarian cancer. Int J Cancer. 2017;141(11):2197–2203. doi:10.1002/ijc.30919
44. Su JP, Liu HF, Zhang HL, He YJ, Nie Y. Effects of different degrees of depression on inflammatory response and immune function in patients with ovarian cancer. J Biol Regul Homeost Agents. 2018;32(5):1225–1230.
45. Botwinick IC, Pursell L, Yu G, Cooper T, Mann JJ, Chabot JA. A biological basis for depression in pancreatic cancer. HPB. 2014;16(8):740–743. doi:10.1111/hpb.12201
46. Hathaway CA, Townsend MK, Conejo-Garcia JR, et al. The relationship of lifetime history of depression on the ovarian tumor immune microenvironment. Brain Behav Immun. 2023;114:52–60. doi:10.1016/j.bbi.2023.08.006
47. Satin JR, Linden W, Phillips MJ. Depression as a predictor of disease progression and mortality in cancer patients: a meta-analysis. Cancer. 2009;115(22):5349–5361. doi:10.1002/cncr.24561
48. Li YZ, Qin X, Liu FH, et al. Prediagnosis depression rather than anxiety symptoms is associated with decreased ovarian cancer survival: findings from the ovarian cancer follow-up study (OOPS). J Clin Med. 2022;11(24):7394. doi:10.3390/jcm11247394
49. Currier MB, Nemeroff CB. Depression as a risk factor for cancer: from pathophysiological advances to treatment implications. Annu Rev Med. 2014;65(1):203–221. doi:10.1146/annurev-med-061212-171507
50. P.O.W.E.R. (Premenopausal, Osteopenia/Osteoporosis, Women, Alendronate, Depression) Study Group; Cizza G, Ronsaville DS, Kleitz H, et al. Clinical subtypes of depression are associated with specific metabolic parameters and circadian endocrine profiles in women: the power study. PLoS One. 2012;7(1):e28912. doi:10.1371/journal.pone.0028912
51. National Center for Health Statistics. Available from: https://wwwn.cdc.gov/nchs/nhanes/tutorials/Weighting.aspx.
52. Wu CY, Chan TF, Shi HY, Kuo YL. Psychiatric problems of anxiety and depression disorder are associated with medical service utilization and survival among patients with cervical cancer. Taiwan J Obstet Gynecol. 2021;60(3):474–479. doi:10.1016/j.tjog.2021.03.015
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.