")
Back to Journals » Journal of Inflammation Research » Volume 18
Association Between Lactate Dehydrogenase/Albumin Ratio and in-Hospital Mortality in Patients with Acute Aortic Dissection
Authors Mutailifu S , Zhu Q, Wang M, Zhang D, Song S , Li N
Received 21 January 2025
Accepted for publication 26 April 2025
Published 14 May 2025 Volume 2025:18 Pages 6281—6292
DOI https://doi.org/10.2147/JIR.S515010
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qing Lin
Saimire Mutailifu,* Qing Zhu,* Menghui Wang, Delian Zhang, Shuaiwei Song, Nanfang Li
Hypertension Center of People’s Hospital of Xinjiang Uygur Autonomous Region; Xinjiang Hypertension Institute; NHC Key Laboratory of Hypertension Clinical Research; Key Laboratory of Xinjiang Uygur Autonomous Region; Hypertension Research Laboratory; Xinjiang Clinical Medical Research Center for Hypertension (Cardio-Cerebrovascular) Diseases, Urumqi, Xinjiang, 830001, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Nanfang Li, Hypertension Center of People’s Hospital of Xinjiang Uygur Autonomous Region; Xinjiang Hypertension Institute; NHC Key Laboratory of Hypertension Clinical Research; Key Laboratory of Xinjiang Uygur Autonomous Region; Hypertension Research Laboratory; Xinjiang Clinical Medical Research Center for Hypertension (Cardio-Cerebrovascular) Diseases, No. 91 TianChi Road, Urumqi, Xinjiang, 830001, People’s Republic of China, Tel +86-13999179937, Fax +86-09918564816, Email [email protected]
Background: Previous studies have identified the lactate dehydrogenase/albumin ratio (LAR) as an independent prognostic marker, significantly predicting in-hospital mortality in patients with inflammation and cancer. Building on this, the current study is designed to explore the association between LAR and mortality during hospitalization in patients with acute aortic dissection (AAD).
Methods: This retrospective study included patients diagnosed with AAD between January 1, 2010, and March 1, 2023. Patients were categorized into three groups based on LAR tertiles: T1 (< 5.01), T2 (5.01– 6.43), and T3 (> 6.43). Multivariable logistic regression analysis was used to calculate adjusted odds ratios (ORs) and 95% confidence intervals (CIs). In addition, subgroup analysis, receiver operating characteristic (ROC) curves, decision curve analysis (DCA), clinical impact curve analysis, Boruta algorithm, and the Kaplan-Meier analysis were applied to analyze the data.
Results: A total of 2083 patients were enrolled in the study, with an average age of 53.20 ± 12.35 years, and male patients constituted 77%. After adjusting for relevant variables, ORs for in-hospital mortality were found to be 2.12 (95% CI: 1.34– 3.36, p=0.001) for T2 and 2.30 (95% CI: 1.44– 3.68, p< 0.001) for T3, compared to T1. The ROC curve, DCA analysis, Boruta algorithm, and Kaplan-Meier analysis demonstrated that the LAR exhibited a high level of concordance and practical applicability in forecasting in-hospital mortality.
Conclusion: Elevated LAR is significantly associated with an increased risk of in-hospital mortality in patients with AAD. The results indicate that LAR may serve as a valuable predictor of adverse outcomes during hospitalization for these patients.
Keywords: acute aortic dissection, lactate dehydrogenase to albumin ratio, in-hospital mortality, inflammation, mortality risk
Introduction
Acute aortic dissection (AAD) is a rare but life-threatening cardiovascular condition in which a false lumen forms within the aorta, extending from the intima to the aortic media. The mortality rate among patients with AAD is high, ranging from 1% to 2% per hour within the first 24 to 48 hours after diagnosis.1 Research has indicated that the early morbidity and mortality rates for aortic events exceed 50%, and survivors of AAD may experience significant long-term health complications.2 Although therapies such as artificial vascular replacement and aortic stent grafts are available for AAD patients, the overall prognosis, especially for critically ill patients, remains poor. Consequently, assessing the risk of in-hospital mortality and conducting risk stratification is crucial for the effective development of risk-reduction strategies.
Furthermore, inflammation has been linked to poor clinical outcomes in cardiovascular diseases.3,4 Studies have shown that inflammation, along with various noninvasive blood markers, is associated with the prognosis of AAD patients.5,6 Lactate dehydrogenase (LDH), a nonspecific biomarker of inflammation, is a cytoplasmic enzyme expressed in various tissues. He et al demonstrated that increased LDH levels serve as a prognostic indicator of poor outcomes during hospitalization for AAD patients.7 However, LDH levels may be affected by factors such as age, gender, medication use, and physical activity, which may limit its accuracy in assessing the prognosis of AAD.8,9
Serum albumin (ALB) plays a critical role in various functions, including antioxidant and anti-inflammatory properties.10,11 Studies have shown that low albumin levels are associated with poor prognosis in AAD patients.12,13 However, ALB levels can be affected by several factors, including liver dysfunction, malnutrition, chronic diseases, and persistent inflammation.14,15 As a result, relying solely on serum LDH or ALB for prognosis in AAD patients may not yield accurate results. The lactate dehydrogenase/albumin ratio (LAR), which can be easily derived from routine laboratory tests during initial admission, has emerged as a promising prognostic biomarker. Recent studies have highlighted its predictive value in inflammation-related diseases such as severe pneumonia, sepsis, and cancer.16–18 LAR not only reflects the body’s oxidative stress and inflammatory response levels but also serves as a comprehensive tool for evaluating an individual’s metabolic status and nutritional condition. Despite its growing potential, research on the effects of LAR on the outcomes for patients with AAD is quite limited.
Given this, we aimed to comprehensively evaluate the correlation between LAR and mortality outcomes in AAD. By analyzing this ratio, our goal was to provide clinicians with an additional tool for assessing disease severity and predicting outcomes in this critically ill patient population.
Methods
Study Population
This retrospective study utilized data from the Hypertension Expert Database, a big data platform for hypertension research.19 AAD diagnosis was made based on the International Classification of Diseases, 9th and 10th Revisions. A total of 2627 AAD patients were identified from January 1, 2010, to March 19, 2023. The exclusion criteria included: (1) patients under 18 years of age; (2) patients with chronic aortic dissection; (3) Patients with traumatic AAD or congenital aortic malformations; (4) patients who had undergone aortic dissection surgery upon admission; (5) patients with severe conditions such as end-stage renal failure, cirrhosis, or cancer; and (6) patients lacking sufficient data, specifically on LDH and ALB levels. After applying these inclusion and exclusion criteria, 2,083 patients were included for analysis (Figure S1). The Ethics Board of the People’s Hospital of the Xinjiang Uygur Autonomous Region (KY2022080903) approved this retrospective study. The study procedures were carried out by the Declaration of Helsinki. All data were de-identified before analysis, and strict confidentiality protocols were followed to protect patient privacy throughout the research process.
Data Collection and Definition
The baseline information of all patients was extracted from the electronic medical record system upon admission. The variables extracted include (1) demographics, including age, sex, body mass index (BMI), cigarette, and alcohol consumption. (2) vital signs within the first 24 hours of admission, including heart rate, SpO2, systolic blood pressure (SBP), and diastolic blood pressure (DBP). (3) laboratory indicators, such as blood glucose levels (GLU), total cholesterol (TC), triglyceride (TG), high and low-density lipoprotein cholesterol (HDL-C and LDL-C), Lactate, natriuretic peptides (BNP), C-reactive protein (CRP), serum creatinine (Crea), uric acid (UA), blood urea nitrogen (BUN), alanine aminotransferase (ALT), aspartate aminotransferase (AST), white blood cell count (WBC), lymphocyte count (Lymph), monocyte count (Mono), Neutrophil counts (Neut), LDH, ALB, Bicarbonate, and D-dimer levels. (4) Previous history, including coronary heart disease, diabetes mellitus, and stroke. Definitions and detailed measurements for various diseases can be found in the Supplementary Materials.
Clinical Outcomes
A primary endpoint in this study was all-cause mortality in the hospital, with secondary endpoints including 7-day mortality and 28-day mortality during hospitalization. Additionally, we also assessed the Hospital LOS (Length of Stay) and ICU LOS.
Statistical Analysis
Data were presented as mean + standard deviation (SD) of continuous variables, interquartile ranges (IQR) of categorical variables, and percentages of categorical variables. Logistic regression was utilized to determine odds ratios (ORs) and 95% confidence intervals (CIs). To assess potential interactions, stratified analyses were carried out. Furthermore, Restricted cubic splines (RCS) were employed to assess the dose-response relationship, with additional two-stage comparisons focusing on the inflection points of the RCS curve. To evaluate the predictive power and clinical value of LAR, we utilized receiver operating characteristic (ROC) curves, decision curve analyses (DCAs), clinical impact curve analyses, the Boruta algorithm, and the Kaplan–Meier curves. All analyses were conducted using R version 4.2.3. P values <0.05 were considered statistically significant.
Results
Baseline Characteristics
Patients were divided into three groups based on their LAR tertiles, and a comparative analysis of baseline characteristics was conducted. The mean age of the patients was 53.20 ± 12.35 years, with 77% being male, as shown in Table 1. The 7-day, 28-day, and in-hospital mortality rates were 4.6%, 7.5%, and 8.3%, respectively. Notably, patients in the high LAR group (T3, ≥6.43) tended to be younger and had elevated levels of heart rate, WBC, Mono, Neut, CRP, AST, ALT, lactate, GLU, D-Dimer, LDH, BNP, UA, BUN, and Crea. However, despite these notable differences, no statistically significant variation was observed in the duration of hospital or ICU LOS across the tertiles (P > 0.05). The most significant finding was that participants with elevated LAR had higher mortality rates at 7 days, 28 days, and during hospitalization (all P<0.05) compared to those with lower LAR levels, as shown in Figure 1. In addition, baseline characteristics of Acute type A aortic dissection (ATAAD) and Acute type B aortic dissection (ATBAD) are shown in Table S1.
 |
Table 1 Characteristics of the Study Population Based on LAR Tertiles |
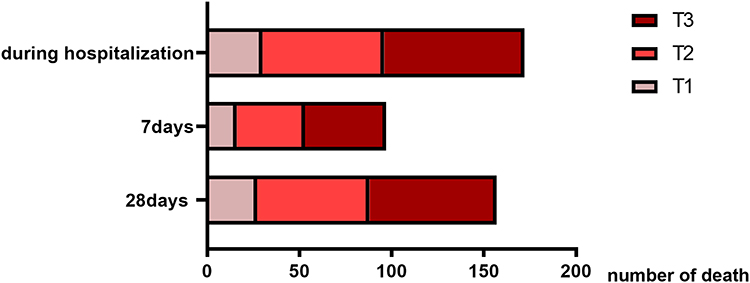 |
Figure 1 Number of deaths according to tertiles of LAR. |
Relationship Between LAR and Outcomes
Table 2 presents the results of a multivariate logistic regression analysis exploring the association between LAR and mortality rates. In the unadjusted crude model, a notable independent positive relationship was found between LAR and the risk of in-hospital mortality (OR, 2.72; 95% CI, 1.76–4.21). Additionally, patients with higher LAR had a 2.87-fold increased risk of 7-day mortality and a 173% increased risk of 28-day mortality compared to the low LAR 1group. After adjusting for all factors, the results further confirmed that the risk of mortality increases as LAR rises.
 |
Table 2 Relationship Between LAR and in-Hospital Mortality in Patients with AAD |
We also used the RCS model to investigate the dose-response relationship between LAR and all-cause mortality in AAD, revealing a significant non-linear association (Figure 2). Furthermore, we found that the risk of in-hospital death increased significantly when the LAR exceeded 5.74. Participants with LAR scores greater than 5.74 had a 87% higher risk of in-hospital death than those with scores of 5.74 or lower (Table 3).
 |
Table 3 Threshold Effect Analysis of the Relationship Between the LAR and Mortality in Patients with AAD |
 |
Figure 2 Restricted cubic spline for the association between LAR and in-hospital mortality in patients with AAD. |
Subgroup Analysis
To confirm the relationship between LAR and in-hospital mortality, stratified according to factors such as gender, age, BMI, SBP, DBP, smoking status, type of AAD, and diabetes, we conducted detailed subgroup analyses. As shown in Table S2, the results were consistent with the findings mentioned above. (All P-values for interaction were >0.05). This further confirmed that the effects of LAR on in-hospital mortality and adverse outcomes in patients with AAD were independent of these stratified factors.
In ATAAD patients (Table S3), higher LAR tertiles (T3 vs T1) were strongly associated with in-hospital mortality even after full adjustment (OR = 2.19, 95% CI: 1.22–3.94; P =0.009), with a significant trend (P =0.012). In contrast, for ATBAD patients, the association weakened in Model 3 (T3 OR = 2.15, 95% CI: 0.92–5.02; P =0.079), and no significant trends were observed for 7-day mortality (P =0.633) (Table S4). Importantly, interaction tests between AAD subtypes and LAR effects were non-significant (P >0.05).
Variable Validation
We further used ROC curve analysis to assess the prognostic utility of various indicators, including LDH, ALB, and LAR, for in-hospital mortality (Figure 3A). The results showed that LAR exhibited the highest AUC values compared to LDH and ALB. Additionally, DCA and clinical impact curve analyses confirmed that LAR provides superior clinical benefits compared to the other measures (Figure 3B and C). We also have performed ROC curve analyses for CRP, WBC, and BNP. LAR demonstrated superior predictive performance (AUC = 0.608, cut-off = 5.164) compared to other markers (Figure S2). Finally, Boruta algorithm was performed to assess the variable importance of LAR. The results demonstrated that LAR retained the high variable importance, which was consistent across both 7-day and 28-day mortality rates (Figure 4). Therefore, our findings emphasize that LAR may have significant clinical utility in assessing in-hospital mortality in patients with AAD.
 |
Figure 3 ROC (A), DCA curve (B), and (C) for clinical impact curve. |
 |
Figure 4 Boruta-Based Feature Selection and Mortality Prediction Analysis: In-Hospital (A), 7-Day (B), and 28-Day (C) Outcomes. |
Kaplan–Meier Curves
To evaluate the cumulative 28-day survival across distinct LAR tertiles in patients with AAD, Kaplan–Meier survival curves were constructed and stratified by baseline LAR levels. The Kaplan–Meier curves revealed that individuals with high LAR had substantially poorer 28-day survival and that 28-day survival decreased with decreasing baseline LAR (Figure 5). In contrast to conventional biomarkers—including CRP, WBC, and BNP—whose prognostic stratification is presented in Figure S3.
 |
Figure 5 Kaplan–Meier curve of 28-day mortality for patients with AAD. |
Discussion
In our observational analysis, we found a significant positive association between LAR and in-hospital mortality in patients with AAD. This association remained strong even after adjusting for confounders and performing subgroup analyses, further supporting the reliability of our findings. Notably, individuals with LAR levels exceeding 5.74 exhibited an increased risk of mortality compared to those with levels below this this cutoff point. Furthermore, when compared to other indicators, LAR demonstrated superior clinical benefits. These results suggest that LAR may have significant clinical value in assessing the severity of AAD and predicting patient prognosis.
AAD is a serious acute disease that presents with severe symptoms, a high mortality rate, and numerous complications once it occurs. Therefore, identifying risk factors for dissection and intervening early to prevent adverse outcomes is critical. Many clinical investigations have explored the relationship between LDH levels and the occurrence and mortality of cardiovascular diseases in both the general population and specific patient groups.20,21 In addition, in patients with conditions such as congenital heart disease, CAD, heart failure, infective endocarditis, peripheral arterial disease, and stroke, low serum albumin levels serve as a potent and independent prognostic indicator, signaling a higher risk of adverse events.22–24 Previous research has also demonstrated that hyperlactatemia and hypoalbuminemia increase the the mortality risk in patients with AAD.7,13
The pathophysiology of AAD involves an extensive inflammatory response, tissue damage, and abnormal energy metabolism,25,26 which collectively influence changes in LDH and ALB levels. As a comprehensive indicator, the LAR provides a more holistic reflection of the patient’s overall health status and disease severity. In our study, using Boruta variable significance analysis, we identified LAR as a valuable new indicator for identifying patients with AAD upon emergency department admission and for determining prognosis. Furthermore, the predictive performance of LAR was superior to that of individual indicators, as demonstrated in the established ROC analysis. Elevated CRP, WBC, and BNP levels have been previously associated with adverse outcomes in AAD,27–29 our study aligns with these findings, and our analysis emphasizes that LAR may offer improved discriminative ability compared to these conventional markers, as evidenced by its higher AUC value. LAR also showed the best clinical benefit in DCA curves and clinical impact curves, further suggesting its potential utility in predicting adverse outcomes in patients with AAD. Several studies have already confirmed the prognostic utility of LAR in severe infections and malignant tumor diseases.30,31 In severe infections, Jeon et al demonstrated that LAR serves as a standalone predictor of mortality in ICU patients (AUC=0.642, 95% CI: 0.602–0.681, P < 0.001).16 Lee et al also indicated that LAR serves as a notable factor in predicting the risk of death during hospitalization for these individuals.32 A Chinese study on sepsis-associated acute kidney injury using RCS identified a cutoff of 5.57, with each log2-unit LAR increase linked to a 29% rise in 28-day mortality.17 The discrepancies underscore the necessity of interpreting LAR thresholds within their specific pathophysiological frameworks, as the mechanistic underpinnings of acute vascular injury in AAD differ fundamentally from those of systemic inflammation in sepsis-associated acute kidney injury. Additionally, a study involving 346 resectable esophageal squamous cell carcinoma patients who underwent esophagectomy found that LAR was a useful prognostic factor for cancer-specific survival.18 Wu et al further pointed out that LAR holds greater prognostic significance than LDH and ALB alone before the primary treatment of diffuse large B-cell lymphoma.33 Despite these findings, the prognostic relevance of LAR in AAD has not been extensively studied. Our study addresses this previously unexplored gap in the literature. Furthermore, we found that the LAR had a more pronounced prognostic value in ATAAD than in ATBAD. ATAAD patients exhibited heightened acute inflammation and tissue injury, whereas ATBAD was characterized by chronic metabolic dysregulation (Table S1). Although subgroup interactions lacked statistical significance, the lower mortality rate in ATBAD likely reduced the predictive precision of LAR. As a composite biomarker, LAR effectively captures acute pathophysiological derangements in ATAAD but demonstrates limited utility in ATBAD.
No studies have yet investigated the impact of elevated LAR on in-hospital mortality in patients with AAD. However, previous studies on LDH and ALB provide some insights that may help explain this relationship. First, elevated LDH levels indicate hypoxia, as the onset of AAD causes damage and hypoxia in the surrounding tissues. In response to this hypoxic environment, LDH efficiently converts pyruvate, the final product of glycolysis, into lactate, further exacerbating the hypoxic condition.7 Second, excess LDH can induce oxidative stress.34,35 Third, LDH influences the production of various inflammatory mediators, including cytokines (such as TNF-α and IL-6) and nitric oxide (NO), by generating excessive lactic acid.36 Liu et al also emphasized the role of inflammation-related mechanisms in the risk of multiple organ dysfunction syndrome in patients with ATAAD.36 ALB, with its free thiol group, reacts strongly with oxidants.37 In response to acute stressors, the body may experience hypoalbuminemia, where plasma albumin levels fall below normal.38 Reduced ALB disrupts the normal function and stability of lysophosphatidic acid, leading to damage to the vascular endothelium.38 The significance of reduced serum albumin levels in cardiovascular disease arises not only from its oncotic properties but also from its anti-inflammatory and antioxidant functions.22,39 Furthermore, ALB can reflect the body’s nutritional status. Consequently, the LAR serves as a powerful tool for comprehensively assessing an individual’s metabolic profile, oxidative stress levels, inflammatory response, and nutritional status.17,30
According to our knowledge, this research is the initial to comprehensively investigate the association between LAR and mortality at different time points upon admission in critically ill Chinese patients with AAD. A key finding of this research is that when LAR exceeds 5.74, it is closely associated with in-hospital mortality and adverse outcomes in AAD patients, suggesting that it may serve as a simple and effective prognostic tool for assessing the risk of poor outcomes. However, along with these advantages, we have to recognize some limitations. First, this retrospective analysis retained inherent biases despite our statistical adjustments, and we could not fully mitigate inter-institutional variability in laboratory measurements, potentially introducing heterogeneity in LAR values across clinical centers. Second, we did not perform long-term clinical follow-up on the surviving patients, resulting in a lack of data regarding their long-term prognosis. Finally, our research exclusively focused on the initial LAR of non-surgical treatment patients at the time of admission, and it is unclear whether changes in LAR during follow-up could also predict mortality. Therefore, while our findings suggest an association between LAR and AAD, further prospective validation in larger, multi-center cohorts, especially for ATBAD, is essential before clinical implementation.
Conclusions
The present study found that elevated LAR was strongly associated with an increased risk of in-hospital mortality in patients with AAD. Notably, we observed that the risk of mortality increased even further when LAR exceeded 5.74. Our results indicate that LAR may serve as a concise and reliable tool for the clinical evaluation of prognosis in AAD patients.
Data Sharing Statement
The datasets used and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
As the study was retrospective, informed consent was waived.
Acknowledgments
All authors would like to thank all collaborators of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Major Science and Technology Special Project of Xinjiang Uygur Autonomous Region (2022A03012-2) and Major Science and Technology Special Project of Xinjiang Uygur Autonomous Region (2022A03012).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Milewicz DM, Ramirez F. Therapies for thoracic aortic aneurysms and acute aortic dissections. Arterioscler Thromb Vasc Biol. 2019;39(2):126–136. doi:10.1161/ATVBAHA.118.310956
2. Azoulay A, Serrand C, Belarbi A, et al. Acute type B aortic dissection: insights from a single-center retrospective experience over 12 years. J Endovasc Ther;2024. 15266028241258401. doi:10.1177/15266028241258401
3. Koene RJ, Prizment AE, Blaes A, et al. Shared risk factors in cardiovascular disease and cancer. Circulation. 2016;133(11):1104–1114.
4. Cai X, Song S, Hu J, et al. Systemic inflammation response index as a predictor of stroke risk in elderly patients with hypertension: a cohort study. J Inflamm Res. 2023;16:4821–4832. doi:10.2147/JIR.S433190
5. Li M, Xu S, Yan Y, et al. Association of biomarkers related to preoperative inflammatory and coagulation with postoperative in-hospital deaths in patients with type A acute aortic dissection. Sci Rep. 2021;11(1):18775. doi:10.1038/s41598-021-98298-w
6. Tang Z, Liu H, Shao Y. Efficacy of CRP in combination with D-dimer in predicting adverse postoperative outcomes of patients with acute Stanford type A aortic dissection. J Cardiothorac Surg. 2022;17(1):71. doi:10.1186/s13019-022-01818-6
7. He H, Chai X, Zhou Y, et al. Association of lactate dehydrogenase with in-hospital mortality in patients with acute aortic dissection: a retrospective observational study. Int J Hypertens. 2020;2020:1347165. doi:10.1155/2020/1347165
8. C HE, G HJ, H LZ, et al. High levels of serum lactate dehydrogenase correlate with the severity and mortality of idiopathic pulmonary arterial hypertension. Exp Ther Med. 2015;9(6):2109–2113. doi:10.3892/etm.2015.2376
9. Qian X, Sheng Y, Jiang Y, et al. Association between lactate dehydrogenase and ventilator-associated pneumonia risk: an analysis of the MIMIC database 2001-2019. BMC Pulm Med. 2024;24(1):273. doi:10.1186/s12890-024-03084-9
10. Caironi P, Gattinoni L. The clinical use of albumin: the point of view of a specialist in intensive care. Blood Transfus. 2009;7(4):259–267. doi:10.2450/2009.0002-09
11. Quinlan GJ, Martin GS, Evans TW. Albumin: biochemical properties and therapeutic potential. Hepatology. 2005;41(6):1211–1219. doi:10.1002/hep.20720
12. Xu S, Wu Z, Liu Y, et al. Influence of preoperative serum albumin on acute kidney injury after aortic surgery for acute type A aortic dissection: a retrospective cohort study. J Clin Med. 2023;12(4):1581. doi:10.3390/jcm12041581
13. Gao Y, Li D, Cao Y, et al. Prognostic value of serum albumin for patients with acute aortic dissection: a retrospective cohort study. Medicine. 2019;98(6):e14486. doi:10.1097/MD.0000000000014486
14. Chen Y, Ba J, Peng C, et al. Impact of lactate/albumin ratio on prognostic outcomes in patients with concomitant heart failure and chronic kidney disease. Intern Emerg Med. 2024;19(6):1625–1636. doi:10.1007/s11739-024-03656-x
15. Caironi P, Langer T, Gattinoni L. Albumin in critically ill patients: the ideal colloid? Curr Opin Crit Care. 2015;21(4):302–308. doi:10.1097/MCC.0000000000000223
16. Jeon SY, Ryu S, Oh SK, et al. Lactate dehydrogenase to albumin ratio as a prognostic factor for patients with severe infection requiring intensive care. Medicine. 2021;100(41):e27538. doi:10.1097/MD.0000000000027538
17. Liang M, Ren X, Huang D, et al. The association between lactate dehydrogenase to serum albumin ratio and the 28-day mortality in patients with sepsis-associated acute kidney injury in intensive care: a retrospective cohort study. Renal Failure. 2023;45(1):2212080. doi:10.1080/0886022X.2023.2212080
18. Feng JF, Wang L, Yang X, et al. Prognostic value of lactate dehydrogenase to albumin ratio (LAR) in patients with resectable esophageal squamous cell carcinoma. Cancer Manage Res. 2019;11:7243–7251. doi:10.2147/CMAR.S208320
19. Li N, Zhu Q, Dang Y, et al. Development and implementation of a dynamically updated big data intelligence platform using electronic medical records for secondary hypertension. Rev Cardiovasc Med. 2024;25(3):104. doi:10.31083/j.rcm2503104
20. Morello F, Ravetti A, Nazerian P, et al. Plasma lactate dehydrogenase levels predict mortality in acute aortic syndromes: a diagnostic accuracy and observational outcome study. Medicine. 2016;95(6):e2776. doi:10.1097/MD.0000000000002776
21. Kim J, Kim YW, Kim TY. Diagnostic value of serum lactate dehydrogenase level measured in the emergency department in predicting clinical outcome in out-of-hospital cardiac arrest: a multicenter, observational study. J Clin Med. 2023;12(8):3006.
22. Arques S. Serum albumin and cardiovascular disease: state-of-the-art review. Ann Cardiol Angeiol. 2020;69(4):192–200. doi:10.1016/j.ancard.2020.07.012
23. Wu CY, Hu HY, Huang N, et al. Albumin levels and cause-specific mortality in community-dwelling older adults. Prev Med. 2018;112:145–151. doi:10.1016/j.ypmed.2018.04.015
24. Zhao L, Wu L, Wang Z, et al. The lactate-to-albumin ratio relationship with all-cause mortality in cerebral infarction patients: analysis from the MIMIC-IV database. Front Neurol. 2024;15:1334097. doi:10.3389/fneur.2024.1334097
25. Tian C, Chen Y, Xu B, et al. Association of triglyceride-glucose index with the risk of incident aortic dissection and aneurysm: a large-scale prospective cohort study in UK biobank. Cardiovasc Diabetol. 2024;23(1):282. doi:10.1186/s12933-024-02385-x
26. Zhao Y, Fu W, Wang L. Biomarkers in aortic dissection: diagnostic and prognostic value from clinical research Chin Med J. 2024;137(3):257–269. doi:10.1097/CM9.0000000000002719
27. Vrsalovic M, Vrsalovic Presecki A, Aboyans V. N-terminal pro-brain natriuretic peptide and short-term mortality in acute aortic dissection: a meta-analysis. Clinical Cardiology. 2020;43(11):1255–1259. doi:10.1002/clc.23436
28. Vrsalović M, Vrsalović Presečki A. Admission C-reactive protein and outcomes in acute aortic dissection: a systematic review. Croatian Med J. 2019;60(4):309–315. doi:10.3325/cmj.2019.60.309
29. Yamamoto K, Saito Y, Hashimoto O, et al. Biomarkers for risk stratification in patients with type A acute aortic dissection. Am J Cardiol. 2024;212:103–108. doi:10.1016/j.amjcard.2023.11.053
30. Meng T, Ding W, Lv D, et al. Lactate dehydrogenase to albumin ratio (LAR) is a novel predictor of fatal outcome in patients with SFTS: an observational study. Front Public Health. 2024;12:1459712. doi:10.3389/fpubh.2024.1459712
31. Arici MO, Kivrak SD, Kocer M, et al. Predictive and prognostic value of inflammatory and nutritional indexes in patients with breast cancer receiving neoadjuvant chemotherapy. Medicina. 2024;60(11):1849. doi:10.3390/medicina60111849
32. Lee BK, Ryu S, Oh SK, et al. Lactate dehydrogenase to albumin ratio as a prognostic factor in lower respiratory tract infection patients. Am J Emerg Med. 2022;52:54–58. doi:10.1016/j.ajem.2021.11.028
33. Wu W, Miao L, Zhao L, et al. Prognostic value of lactate dehydrogenase, serum albumin and the lactate dehydrogenase/albumin ratio in patients with diffuse large B-cell lymphoma. Hematology. 2024;29(1):2293514. doi:10.1080/16078454.2023.2293514
34. Rho JM. Inhibition of lactate dehydrogenase to treat epilepsy. N Engl J Med. 2015;373(2):187–189. doi:10.1056/NEJMcibr1503558
35. Colgan SM, Mukherjee S, Major P. Hypoxia-induced lactate dehydrogenase expression and tumor angiogenesis. Clin Colorectal Cancer. 2007;6(6):442–446. doi:10.3816/CCC.2007.n.014
36. Liu H, Li H, Han L, et al. Inflammatory risk stratification individualizes anti-inflammatory pharmacotherapy for acute type A aortic dissection. Innovation. 2023;4(4):100448. doi:10.1016/j.xinn.2023.100448
37. Zoanni B, Brioschi M, Mallia A, et al. Novel insights about albumin in cardiovascular diseases: focus on heart failure. Mass Spectrom Rev. 2023;42(4):1113–1128. doi:10.1002/mas.21743
38. Levitt DG, Levitt MD. Human serum albumin homeostasis: a new look at the roles of synthesis, catabolism, renal and gastrointestinal excretion, and the clinical value of serum albumin measurements. Int J Gen Med. 2016;9:229–255. doi:10.2147/IJGM.S102819
39. Ronit A, Kirkegaard-Klitbo DM, Dohlmann TL, et al. Plasma albumin and incident cardiovascular disease: results from the CGPS and an updated meta-analysis. Arterioscler Thromb Vasc Biol. 2020;40(2):473–482. doi:10.1161/ATVBAHA.119.313681
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.