")
Back to Journals » Journal of Pain Research » Volume 18
Association Between Opioid Use and Emergency Department Visits for Spine-Related Disorders
Authors Okeke C, Okoye G, Thornton JD
Received 25 January 2025
Accepted for publication 29 June 2025
Published 10 July 2025 Volume 2025:18 Pages 3493—3504
DOI https://doi.org/10.2147/JPR.S519382
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Timothy Atkinson
Chijioke Okeke,1,2 Godwin Okoye,3 J Douglas Thornton1,2
1The Prescription Drug Misuse Education and Research (PREMIER) Center, College of Pharmacy, University of Houston, Houston, TX, USA; 2Department of Pharmaceutical Health Outcomes and Policy, College of Pharmacy, University of Houston, Houston, TX, USA; 3Health Outcomes Division, College of Pharmacy, The University of Texas at Austin, Austin, TX, USA
Correspondence: J Douglas Thornton, Department of Pharmaceutical Health Outcomes and Policy, University of Houston College of Pharmacy, 4349 Martin Luther King Boulevard, Houston, TX, USA, Tel +1 713-743-7458, Email [email protected]
Background: Opioids are frequently prescribed to patients with spine-related disorders (SRD), including those undergoing spinal surgery and those with various back or neck pain. Previous studies assessing the association between opioid use and the risk of emergency department (ED) visits among SRD patients have been limited to specific patient subgroups. Using nationally representative sample, we estimated the association between opioid use and the frequency of all-cause ED visits among SRD patients in the United States.
Methods: This was a retrospective cross-sectional study design that utilized 2018– 2022 Medical Expenditure Panel Survey (MEPS) data. Patients with SRD were identified using ICD-10-CM codes matching for spine-related diagnoses. The primary exposure variable was opioid use, defined by the MEPS prescription drug file. The outcome was all-cause ED visits, which were measured as the number of ED visits observed between 2018 and 2022 as reported in the MEPS emergency room visits files. Descriptive weighted analyses were used to examine the characteristics of patients with SRD. We selected the zero-inflated negative binomial model, which had the best model fit based on the Akaike Information Criterion (AIC), to estimate the incident rate ratio of all-cause ED visits for opioid users compared to non-opioid users.
Results: The final sample consisted of 8078 adult patients (18632323 weighted sample) with SRD diagnoses, among whom approximately 21% received opioid prescriptions. The proportion of opioid users compared to non-opioid users varied by gender (opioid users: male 39.34%, female 60.66%; non-opioid users: male 42.45%, female 57.55%; P = 0.045) and insurance type (opioid users: private 61.51%, public 36.92%, uninsured 1.57%; non-opioid users: private 69.87%, public 26.49%, uninsured 3.64%; P < 0.001). Multivariable analysis revealed a significant association between opioid use and increased ED visits (IRR= 1.63, 95% CI: 1.39– 1.90).
Conclusion: We found that opioid use significantly increases the frequency of all-cause ED visits among SRD patients. These findings highlight the importance of cautious opioid prescribing among SRD patients.
Keywords: opioids, spine-related disorders, SRD, emergency department visits, medical expenditure panel survey, MEPS, hospitalization, prescribing behaviour
Introduction
Spine-related disorders (SRD), including neck and back pain, are common health conditions that pose a major healthcare burden globally.1,2 Back pain is reported as one of the most common reasons for hospitalization visits in the United States,3 and up to 16% of American adults report having neck discomfort every year.4 Among the several management options for spine-related illnesses, opioid pharmacotherapy has become a widely used treatment method for alleviating chronic pain.5 Opioids are frequently prescribed to patients with SRD, including those undergoing spinal surgery and those with various back or neck pain, which may or may not be specific.6,7
The increased utilization among SRD patients is evidenced by an increase in opioid expenditures for spine-related pains by over 40% in the past decade.8 In addition, orthopedics is currently ranked in the top five among opioid-prescribing specialties.9,10 However, prescription opioids contribute almost 40% to opioid overdose outcomes.11 The risk of hospitalization following opioid use among SRD patients has been assessed in some previous studies.1,12–17 Jain et al found chronic opioid use to be a risk factor for complications, readmissions and adverse events among SRD patients undergoing spinal surgery.18 A systematic review by Yerneni et al found that preoperative opioid use is overwhelmingly associated with negative spine surgical and functional outcomes, including hospitalization and emergency visits.17 Existing evidence has been limited to specific patient subgroups, such as patients who underwent spinal surgery.1,14–17 Moreso, most of the studies relied on administrative databases and thus were unable to capture uninsured SRD patients.
Our study addresses this gap by including a more representative sample of the US population with SRD. Since most of the opioid-related adverse event cases end up in hospital-based emergency departments,18,19 examining the association between opioid use among SRD patients and the frequency of all-cause ED visits at a national level could provide valuable insights and estimates about this risk. This may help guide clinician prescribing behaviour and in making informed policy decisions. This study thus aims to estimate the association between opioid use and the frequency of ED visits among SRD patients in the US.
Methods
Study Design and Data Source
This retrospective cross-sectional study utilized the 2018–2022 Medical Expenditure Panel Survey (MEPS) data.20 MEPS is a series of extensive surveys carried out by the Agency for Healthcare Research and Quality (AHRQ). It follows a panel design, consisting of five interview rounds spread over a period of two calendar years. MEPS participants are chosen using the sampling system of the National Health Interview Survey, which identifies civilian, noninstitutionalized persons residing in the United States with particular characteristics to take part in the survey. The Household Component (MEPS-HC), which is a key part of MEPS, gathers self-reported information on many aspects of household members. This includes demographic details, health conditions and status, prescription medicine usage, emergency visits, inpatient stays, health insurance, income, and healthcare expenses.20 The Medical Conditions files encompass data on conditions reported by respondents, which were coded using the International Classification of Disease, 10th Edition (ICD-10-CM) by professional coders and subsequently converted to clinical classification codes by AHRQ.20 The Prescribed Medicines files are organized at the event level, with each record representing distinct prescribed medications that are categorized into a therapeutic class according to the Multum Lexicon therapeutic classification method and provided to the researchers in the MEPS.20 ED visits files include any visit made during the person’s reference period to a hospital emergency department.20 MEPS collects information on the health conditions requiring emergency room care, medical services provided, any surgical procedures performed, prescribed medicines, and the physicians and surgeons providing emergency room care. MEPS data are de-identified and fully compliant with the Health Insurance Portability and Accountability Act (HIPAA); hence were deemed human subjects exempt by the University of Houston Institutional Review Board.
Study Population
Participants with SRD were identified from the medical conditions files using the International Classification of Diseases, Tenth Edition (ICD-10-CM) codes for all SRD diagnoses.21–23 A comprehensive list of included SRD ICD-10-CM codes can be found in the (Supplementary Table S1).
Exposure Variable
The exposure variable was a binary indicator of receiving an opioid prescription or not during the study period. Multum Lexicon therapeutic class codes are available for self-reported medication use in MEPS prescription data.24 Prescriptions for opioid medications were determined using the Multum Lexicon therapeutic subclassification variables of “60” (narcotic analgesics) or “191” (narcotic analgesic combinations). The prescribed opioid group consisted of patients who reported having a prescription for at least one narcotic analgesic or narcotic analgesic combination at any time within the study period.25–27
Outcome Variable
The outcome variable was all-cause ED visit, which was measured as the number of all-cause ED visits observed in the MEPS emergency visits files during the study period.28 The ED visit data section of the MEPS survey obtains information on the health conditions requiring emergency room care, medical services provided, any surgical procedures performed, and the physicians and surgeons providing emergency room care.
Covariates
Covariates were identified using the conceptual framework of the Anderson Behavioral Model (ABM).29 The ABM offers a theoretical framework for understanding access to and use of health services, highlighting the factors that influence an individual’s decision to seek for care or not.29
This model is appropriate for this research project as it helped identify factors that are associated with utilizing care (ED care) in SRD. This model categorizes determinants of health service use into predisposing, enabling, and need factors. Predisposing factors refer to demographic and social characteristics that affect an individual’s likelihood of using health services. Enabling factors facilitate an individual’s ability to access health services, while need factors serve as motivation for seeking care. Our study included predisposing factors such as age in years (≤65 and >65), gender (male and female), race/ethnicity (Hispanic, Non-Hispanic Black, Non-Hispanic Whites, Non-Hispanic Others), and region (Northeast, Midwest, South, West). Data for predisposing factors were obtained from the consolidated MEPS file as responses to the survey questions.20 Enabling factors included are education status (college or more and high school or less), health insurance status (private, public, and uninsured), and provider type (facility, person, and person-in facility). In MEPS, a facility provider type refers to when respondents make a reference to receiving care from an institution; a person provider type refers to when respondents make a reference to receiving care from private practices, and a person-in-facility provider type refers to when respondents make a reference to receiving care from individual specialists within a facility. These responses are documented in the MEPS full-year consolidated files.20 Need factors included were functional limitations (Yes and No), work limitations (Yes and No), perceived physical health (excellent, fair, good, poor), and perceived mental health status (excellent, good, fair, and poor). The number of comorbidity (Elixhauser comorbidity score) was calculated as a composite score for each patient, based on the presence of 32 distinct chronic diseases, utilizing the algorithm referenced in the literature.30 Data for the included chronic diseases were obtained from the MEPS medical condition files.20 We also accounted for the yearly effect in our analysis.
Statistical Analysis
Descriptive weighted analyses were used to examine the characteristics of patients with SRD. For our multivariable analysis, we fitted four count regression models (Poisson, Negative Binomial, Zero-inflated Poisson, and Zero-inflated Negative Binomial models), and we selected the zero-inflated negative binomial model, which had the best model fit based on the Akaike Information Criterion (AIC) (Table 1). This model was utilized to estimate the incident rate ratio (IRR) of ED visits for opioid users compared to non-opioid users. The analyses were adjusted for the complex survey design of the MEPS data using cluster, strata, and weight variables in statistical procedures such as SURVEYFREQ and SURVEYMEANS. All statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, North Carolina) with a statistical significance level of 0.05.
 |
Table 1 Model Fit Parameters for Model Comparison |
Additional Analysis
We conducted a subgroup analysis, including only SRD patients with documented pharmacologic pain prescription records. Within this subgroup, we compared opioid users to non-opioid analgesic users with respect to all-cause emergency department (ED) visits, adjusting for all covariates. We also estimated the incidence rate ratio (IRR) and corresponding 95% confidence intervals for the exposure group.
Results
Sample Description
According to the national survey reported by MEPS, the total unweighted and weighted number of non-institutionalized US adults with neck and back pain during our study period were 8078 and 18632323 respectively (Figure 1). Approximately 69% of the participants in this study were aged less than 65 years. Majority of them are females (58%), non-Hispanic whites (74.67%), and with private insurance (68.18%). The majority of participants had finished college (64.25%), were from the southern region (34.29%), and made use of person-in-facility providers (48.38%) (Table 2).
 |
Table 2 Sample Description of SRD Patients by Opioid Utilization (MEPS Data, 2018–2022) |
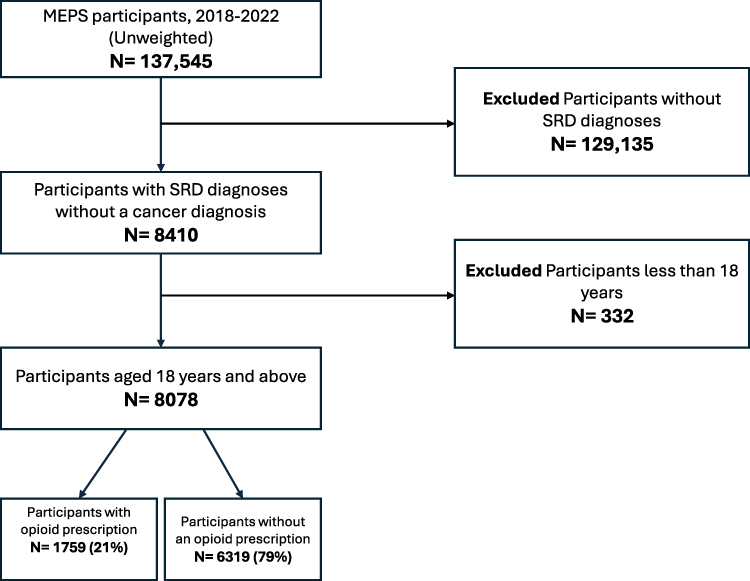 |
Figure 1 Study flow chart. This flow chart illustrates the stepwise selection of MEPS study participants for inclusion in the study. The chart includes the total number of MEPS participants assessed for eligibility, the number of participants excluded and the reasons for exclusion (lack of SRD diagnosis record, non-adults, record of cancer diagnosis), and the final number of participants included in the final analysis. |
Sample Description by Opioid Utilization (Unadjusted Bivariate Analyses)
Out of the 18632323 weighted individuals with neck and back pain, 3777192 (20.27%) were prescribed an opioid annually. The proportion of opioid users compared to non-opioid users varied by gender (opioid users: male 39.34%, female 60.66%; non-opioid users: male 42.45%, female 57.55%; P = 0.045) and insurance type (opioid users: private 61.51%, public 36.92%, uninsured 1.57%; non-opioid users: private 69.87%, public 26.49%, uninsured 3.64%; P < 0.001), number of comorbidities (opioid users: zero 16.31%, one 21.76% two 17.61%, three 15.88% four 11.69%, five or more 16.74%; non-opioid users: zero 31.09%, one 25.48% two 16.80%, three 11.63% four 7.58%, five or more 7.42%; P <0.001). All bivariate analyses are summarized in Table 2.
Multivariable Analysis
Table 3 shows the adjusted association between opioid use and the number of ED visits among SRD patients after accounting for patient characteristics. We observed a difference in the expected increase in number of ED visits among SRD patients who use opioids compared to those who do not (IRR= 1.63, 95% CI: 1.39–1.90).
 |
Table 3 Multivariable Analysis Showing the Association Between Opioid Pharmacotherapy Use and the Frequency of Emergency Room Visits Among SRD Patients |
Additional Analysis
Table 4 presents the adjusted association between opioid use and the number of emergency department (ED) visits among SRD patients with documented pain prescriptions. After adjusting for patient characteristics, opioid users had a significantly higher rate of ED visits compared to non-opioid analgesic users (IRR = 1.46, 95% CI: 1.18–2.63), indicating a 46% increase in the expected number of ED visits among opioid users in this subgroup.
 |
Table 4 Sub-Group Analysis: Multivariable Analysis Showing the Association Between Analgesic Type and the Frequency of Emergency Room Visits Among SRD Patients |
Discussion
Our study examined the association between opioid use and the frequency of all-cause ED visits among SRD patients. The findings demonstrated that SRD patients who use opioids had a higher frequency of all-cause ED visits compared to those who do not. Our subgroup additional analyses showed an increased rate of all-cause ED visits among opioid users compared specifically to non-opioid analgesic users with SRD. There is limited observational research on hospitalization outcomes associated with opioid use among SRD patients, with most evidence derived from clinical trials and prior observational studies focusing primarily on specific patient subgroups. Most of these studies indicated that opioid exposure among SRD patients could lead to an increased rate of hospitalization, longer hospitalizations, and elevated rates of hospital readmission.1,14–16,19,31,32
Similar to our findings, patients with low back pain or neck discomfort who used opioids had worse adverse effects leading to hospitalization compared to those who used a placebo, according to the OPAL RCT15 or compared to those who did not use opioid medications as reported by the SPACE pragmatic trial.16 The 2017 American College of Physicians (ACP) recommends the use of non-opioids in the treatment of acute back pain, reserving opioids for unresponsive cases and short-term use.33 Our findings support this recommendation even though our analysis may not have accounted for case-by-case pain severity. In addition, Jones et al and Krebs et al both reported opioids not to be superior when compared with non-opioid medications in managing hip or chronic back pain,12,13 further emphasizing that opioid use may not offer additional benefits compared to non-opioid pain medications or non-pharmacologic therapies, such as physical therapy, structured exercise programs, cognitive behavioral therapy, acupuncture, yoga, and chiropractic care. These results reinforce current guidelines that recommend prioritizing non-opioid and non-pharmacological therapies as first-line treatments for most spine-related pain conditions.
Our study findings highlight the need to educate prescribers on safer and more effective prescribing strategies for SRD patients.34 The long-term benefit of this approach might go beyond mitigating the incidences of opioid-related adverse effects but also helping to reduce the increasing healthcare expenditures often attributed to ED visits caused by overdoses.
We acknowledge some limitations in our study. First, the implications of our findings may be constrained by insufficient data on previous outpatient therapy, and some other clinical characteristics that are associated with both our exposure and outcome. Our comparator group combines those who received other non-opioid pharmacotherapy and those who did not use any pain medications, and this may have impacted our effect size. However, the results from our subgroup analysis which included only SRD patients with pain prescription records was consistent with our main findings. Also, despite controlling for numerous patient factors, there may be other significant predictors of utilization not accounted for in this study such as prescriber-specific characteristics. Hence, our analyses may be liable to residual confounding. In addition, using secondary data cross-sectionally does not allow for the determination of a cause-and-effect relationship. However, it is possible to identify statistical association, which we were able to establish in this study. Future research should consider using longitudinal designs to more robustly assess this association. MEPS utilizes self-reported data, which may be susceptible to recall bias. However, in order to mitigate this bias, we incorporated the MEPS complex survey design in our analyses by applying the appropriate sampling weights, as well as clustering and stratification variables. This approach helps account for differential recall and response patterns across population subgroups. In addition, MEPS routinely validates portions of the self-reported data, such as prescription drug use and medical events, through provider and pharmacy verification. To enhance the validity of our measures, we used prescription drug files to define our exposure variable and the emergency department visit files to define our outcome variable, thereby relying on more objectively verified data. Despite these limitations, our study fills an important evidence gap by providing national estimates of the relationship between opioid use and ED visits among SRD patients in the US.
Conclusion
This study suggests that opioid use significantly increases the frequency of ED visits among SRD patients. These findings highlight the importance of cautious opioid prescribing and the need for alternative pain management strategies in SRD patients. Further research may explore the long-term effectiveness and safety of alternative pain management strategies among SRD patients.
Data Sharing Statement
The datasets used and/or analyzed during the current study are publicly available on AHRQ website (Medical Expenditure Panel Survey Home).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
Dr. Thornton is a consultant for the Plaintiff’s Steering Committee for Opioid Litigation and a member of the Texas Opioid Abatement Fund Council. No other authors reported a conflict of interest.
References
1. Deyo RA, Mirza SK, Martin BI. Back pain prevalence and visit rates: estimates from U.S. National Surveys, 2002. Spine. 2006;31(23):2724–2727. doi:10.1097/01.brs.0000244618.06877.cd
2. Shahidi B, Curran-Everett D, Maluf KS. Psychosocial, physical, and neurophysiological risk factors for chronic neck pain: a prospective inception cohort study. J Pain. 2015;16(12):1288–1299. doi:10.1016/j.jpain.2015.09.002
3. Becker A, Held H, Redaelli M, et al. Low back pain in primary care: costs of care and prediction of future health care utilization. Spine. 2010;35(18):1714–1720. doi:10.1097/BRS.0b013e3181cd656f
4. Wolsko PM, Eisenberg DM, Davis RB, Kessler R, Phillips RS. Patterns and perceptions of care for treatment of back and neck pain: results of a national survey. Spine. 2003;28(3):292–297. doi:10.1097/01.BRS.0000042225.88095.7C
5. Chang AK, Bijur PE, Esses D, Barnaby DP, Baer J. Effect of a single dose of oral opioid and nonopioid analgesics on acute extremity pain in the emergency department: a randomized clinical trial. JAMA. 2017;318(17):1661. doi:10.1001/jama.2017.16190
6. Armaghani SJ, Lee DS, Bible JE, et al. Preoperative opioid use and its association with perioperative opioid demand and postoperative opioid independence in patients undergoing spine surgery. Spine. 2014;39(25):E1524–E1530. doi:10.1097/BRS.0000000000000622
7. Oleisky ER, Pennings JS, Hills J, et al. Comparing different chronic preoperative opioid use definitions on outcomes after spine surgery. Spine J. 2019;19(6):984–994. doi:10.1016/j.spinee.2018.12.014
8. Herman PM, Broten N, Lavelle TA, Sorbero ME, Coulter ID. Health care costs and opioid use associated with high-impact chronic spinal pain in the United States. Spine. 2019;44(16):1154–1161. doi:10.1097/BRS.0000000000003033
9. Guy GP, Zhang K. Opioid prescribing by specialty and volume in the U.S. Am J Prev Med. 2018;55(5):e153–e155. doi:10.1016/j.amepre.2018.06.008
10. Menendez ME, Mellema JJ, Ring D. Attitudes and self-reported practices of hand surgeons regarding prescription opioid use. HAND. 2015;10(4):789–795. doi:10.1007/s11552-015-9768-5
11. Wilson N. Drug and opioid-involved overdose deaths—United States, 2017–2018. MMWR. 2020;69.
12. Jones CMP, Day RO, Koes BW, et al. Opioid analgesia for acute low back pain and neck pain (the OPAL trial): a randomised placebo-controlled trial. Lancet. 2023;402(10398):304–312. doi:10.1016/S0140-6736(23)00404-X
13. Krebs EE, Gravely A, Nugent S, et al. Effect of opioid vs nonopioid medications on pain-related function in patients with chronic back pain or hip or knee osteoarthritis pain: the SPACE randomized clinical trial. JAMA. 2018;319(9):872. doi:10.1001/jama.2018.0899
14. Martell BA, O’Connor PG, Kerns RD, et al. Systematic review: opioid treatment for chronic back pain: prevalence, efficacy, and association with addiction. Ann Internal Med. 2007;146(2):116–127. doi:10.7326/0003-4819-146-2-200701160-00006
15. Schoenfeld AJ, Nwosu K, Jiang W, et al. Risk factors for prolonged opioid use following spine surgery, and the association with surgical intensity, among opioid-naive patients. J Bone Jt Surg. 2017;99(15):1247–1252. doi:10.2106/JBJS.16.01075
16. Jain N, Phillips FM, Weaver T, Khan SN. Preoperative chronic opioid therapy: a risk factor for complications, readmission, continued opioid use and increased costs after one- and two-level posterior lumbar fusion. Spine. 2018;43(19):1331–1338. doi:10.1097/BRS.0000000000002609
17. Yerneni K, Nichols N, Abecassis ZA, Karras CL, Tan LA. Preoperative opioid use and clinical outcomes in spine surgery: a systematic review. Neurosurgery. 2020;86(6):E490–E507. doi:10.1093/neuros/nyaa050
18. Soares WE, Melnick ER, Nath B, et al. Emergency department visits for nonfatal opioid overdose during the COVID-19 pandemic across six US health care systems. Ann Emerg Med. 2022;79(2):158–167. doi:10.1016/j.annemergmed.2021.03.013
19. Weiss AJ, Elixhauser A, Barrett ML, Steiner CA, Bailey MK, O’Malley L. Opioid-related inpatient stays and emergency department visits by state, 2009–2014. 2017.
20. Agency for Healthcare Research and Quality (AHRQ). Medical Expenditure Panel Survey. Available from: https://search.ahrq.gov/search?q=spine%20&siteDomain=meps.ahrq.gov.
21. Alvarado AM, Chung E, Deutsch H. Effects of the 2016 CDC opioid prescription guidelines on opioid use and worker compensation case length in patients with back pain. Acta Neurochir. 2023;165(8):2139–2144. doi:10.1007/s00701-023-05694-4
22. Gliedt JA, Walker RJ, Lu K, Dawson AZ, Egede LE. The relationship between patient satisfaction and healthcare expenditures in adults with spine related disorders: an analysis of the 2008 to 2015 Medical Expenditures Panel Survey (MEPS). Spine. 2021;46(20):1409–1417. doi:10.1097/BRS.0000000000004047
23. Martin BI, Gerkovich MM, Deyo RA, et al. The association of complementary and alternative medicine use and health care expenditures for back and neck problems. Med Care. 2012;50(12):1029–1036. doi:10.1097/MLR.0b013e318269e0b2
24. Martin BI. Expenditures and health status among adults with back and neck problems. JAMA. 2008;299(6):656. doi:10.1001/jama.299.6.656
25. Axon DR, Slack M, Barraza L, Lee JK, Warholak T. Nationally representative health care expenditures of community-based older adults with pain in the United States prescribed opioids vs those not prescribed opioids. Pain Med. 2021;22(2):282–291. doi:10.1093/pm/pnaa114
26. Asfaw A, Quay B, Bushnell T, Pana-Cryan R. Injuries that happen at work lead to more opioid prescriptions and higher opioid costs. J Occup Environ Med. 2022;64(12):823. doi:10.1097/JOM.0000000000002709
27. Moriya AS, Xu L. The complex relationships among race/ethnicity, social determinants, and opioid utilization. Health Serv Res. 2021;56(2):310–322. doi:10.1111/1475-6773.13619
28. Medical Expenditure Panel Survey (MEPS) data. Available from: https://meps.ahrq.gov/mepsweb/about_meps/survey_back.jsp.
29. Andersen R. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav. 1995;36(1):1–10. doi:10.2307/2137284
30. Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36(1):8–27. doi:10.1097/00005650-199801000-00004
31. Kurteva S, Abrahamowicz M, Gomes T, Tamblyn R. Association of opioid consumption profiles after hospitalization with risk of adverse health care events. JAMA Network Open. 2021;4(5):e218782. doi:10.1001/jamanetworkopen.2021.8782
32. Friebel R, Maynou L. Trends and characteristics of hospitalisations from the harmful use of opioids in England between 2008 and 2018: population-based retrospective cohort study. J R Soc Med. 2022;115(5):173–185. doi:10.1177/01410768221077360
33. Qaseem A, Wilt TJ, McLean RM, Forciea MA. Clinical Guidelines Committee of the American College of Physicians. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166(7):514. doi:10.7326/M16-2367
34. Miron O, Barda N, Balicer R, Kor A, Lev‐Ran S. Association of opioid use disorder with healthcare utilization and cost in a public health system. Addiction. 2022;117(11):2880–2886. doi:10.1111/add.15963
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.