")
Back to Journals » Journal of Inflammation Research » Volume 17
Association Between the Aggregate Index of Systemic Inflammation and Clinical Outcomes in Patients with Acute Myocardial Infarction: A Retrospective Study
Authors Jiang Y, Luo B, Lu W, Chen Y, Peng Y, Chen L, Lin Y
Received 22 July 2024
Accepted for publication 27 September 2024
Published 3 October 2024 Volume 2024:17 Pages 7057—7067
DOI https://doi.org/10.2147/JIR.S481515
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Yan Jiang,1,* Baolin Luo,2,* Wen Lu,1 Yaqin Chen,1 Yanchun Peng,2 Liangwan Chen,3,4 Yanjuan Lin2,3
1School of Nursing, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China; 2Department of Nursing, Fujian Medical University Union Hospital, Fuzhou, Fujian, People’s Republic of China; 3Department of Cardiovascular Surgery, Fujian Medical University Union Hospital, Fuzhou, Fujian, People’s Republic of China; 4Fujian Provincial Special Reserve Talents Laboratory, Fuzhou, Fujian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Liangwan Chen, Department of Cardiovascular Surgery, Fujian Medical University Union Hospital, Fuzhou, Fujian, People’s Republic of China, Email [email protected] Yanjuan Lin, Department of Nursing, Fujian Medical University Union Hospital, Fuzhou, Fujian, People’s Republic of China, Email [email protected]
Purpose: The Aggregate Index of Systemic Inflammation (AISI) has emerged as a novel marker for inflammation and prognosis, but its role in patients with acute myocardial infarction has not been studied. Therefore, this study aimed to investigate the impact of different AISI levels on the clinical outcomes of patients with acute myocardial infarction.
Patients and Methods: This study was a retrospective study, including 1044 patients with acute myocardial infarction (AMI) who were treated at the Fujian Medical University Affiliated Union Hospital, China from May 2017 to December 2022. The patients were divided into high and low AISI groups based on the median value (Q1 Group, ≤ 416.15, n=522; Q2 Group, ≥ 416.16, n=522), and the differences in baseline characteristics and clinical outcomes between the two groups were analyzed. The primary outcome included major adverse cardiovascular and cerebrovascular events (MACCEs), while the secondary outcomes included contrast-induced nephropathy (CIN) risk and all-cause rehospitalization rate.
Results: The findings of the single-factor analysis suggest that a significant association between high AISI levels and the occurrence of MACCEs in AMI patients. After adjusting for confounding factors, the results indicated that compared to Q1, patients in the Q2 group had a higher risk of all-cause mortality [adjusted odds ratio (aOR) 4.64; 95% CI 1.37– 15.72; p=0.032], new-onset atrial fibrillation (aOR 1.75; 95% CI 1.02– 3.00; p=0.047), and CIN (aOR 1.75; 95% CI 1.02– 3.01; p=0.043), with all differences being statistically significant.
Conclusion: In the population of AMI patients, an elevated AISI level is significantly associated with an increased risk of cardiovascular death and can serve as an early marker for adverse prognosis.
Keywords: acute myocardial infarction, inflammation index, clinical outcomes, MACCEs
Introduction
Coronary heart disease (CHD) is a highly prevalent disease, over 17.6 million people worldwide succumb to CHD annually. By 2030, this figure is projected to surpass 23.6 million.1 The recent experimental and clinical evidence emphasizes the significance of cellular and molecular pathways associated with inflammation and immunity in ischemic myocardial injury. The inflammatory response is upregulated prior to the onset of acute myocardial infarction, while it becomes excessively activated following the onset of acute myocardial infarction, suggesting AMI’s inflammatory nature to some extent.2 However, residual inflammation risk may impact patient outcomes in various ways: Patients’ long-term prognosis hinges on local inflammatory processes causing myocardial tissue damage and inflammatory activity influencing atherosclerotic plaque progression.3 Studies have linked blood cell derivatives with adverse cardiovascular outcomes risk in AMI patients through mediating inflammatory responses, thus emphasizing the importance of blood derivative-mediated inflammatory response size for AMI patient prognosis.4,5
Currently, the role of full blood cell counts in predicting the prognosis of patients with acute myocardial infarction (AMI) is frequently underestimated by clinicians and patients, and there remains a shortage of effective blood biomarkers for prognosis assessment. Composite inflammatory indices, which integrate multiple indicators, are recognized as providing a more comprehensive view of inflammation compared to single markers. In this context, the Aggregate Index of Systemic Inflammation (AISI) was introduced in 2018.6 AISI is a novel composite measure that evaluates systemic inflammation by combining various blood cell components, including neutrophils, lymphocytes, monocytes, and platelets.6 Initially designed to predict the risk of prolonged hospital stays in patients undergoing open-chest surgery, AISI has since demonstrated utility in forecasting clinical outcomes in diverse conditions such as diabetes, esophageal cancer, prostate cancer and so on, showing robust predictive value.6–10 The application of AISI in cardiovascular diseases has also attracted significant attention. Research has established a link between AISI levels and the severity of coronary artery disease, clinical stability, and prognosis.11 AISI has been identified as an independent risk factor for major adverse cardiovascular events (MACEs) in coronary artery disease patients, with higher AISI levels correlating with an increased risk of MACEs. Similar associations have been observed in hypertensive patients.12 It is hypothesized that the strong correlation between AISI and cardiovascular death risk may be attributable to the inflammatory effects of individual blood cells. Specifically, neutrophils, monocytes, platelets, and their derived cytokines are primarily involved in non-specific inflammatory pathways, whereas circulating lymphocytes are thought to be linked to specific inflammatory pathways.13 However, there is currently a lack of research exploring the relationship between AISI levels and clinical outcomes in AMI patients.
Therefore, we aimed to evaluate different AISI levels’ effects on biochemical and cardiovascular characteristics of AMI patients and determine whether AISI level is related to the risk of MACCEs in AMI patients.
Material and Methods
Study Design and Population
This study was a retrospective study, including 1044 patients with AMI who were treated at the Fujian Medical University Affiliated Union Hospital, China from May 2017 to December 2022. Inclusion criteria comprised: (1) age≥18 years; (2) all patients met the diagnostic criteria for acute myocardial infarction as per the Fourth Universal Definition of Myocardial Infarction (2018).14 Exclusion criteria included: (1) presence of other serious underlying diseases or severe complications; (2) incomplete clinical data. 1044 patients were included for analysis. Inclusion/exclusion flowchart for the study group is shown in Figure 1. The study was approved by the Ethics Committee of Fujian Medical University Affiliated Union Hospital (2023KY032) and adhered to ethical principles outlined in the Helsinki Declaration. Informed consent was provided by all participants.
 |
Figure 1 Inclusion/exclusion flowchart for the study group. |
Data Collection
The venous blood samples were collected within 24 hours of admission, all from a fasting state (fasting time > 8h). If multiple blood tests were conducted over a 24-hour period, the results of the initial test were utilized. The laboratory data for this study were measured by the Laboratory Center of Fujian Medical University Union Hospital and obtained from the electronic medical record system of Fujian Medical University Union Hospital. Baseline data included socio-demographic information, admission and discharge diagnoses, laboratory tests, medications, surgical characteristics, and discharge status.
Clinical Definition
Hypertension, diabetes mellitus (DM) and stroke were defined using the 10th Revision Codes of the International Classification of Diseases (ICD-10).15 The guidelines for the prevention and treatment of dyslipidemia in Chinese adults (2016), were used to define the diagnosis of hyperlipemia.16 Estimated glomerular filtration rate (eGFR) < 60mL/min/1.73m2 and calculated with MDRD formula.17 AISI was defined as the absolute value of neutrophils multiplied by the absolute value of monocytes multiplied by the absolute value of platelets divided by the absolute value of lymphocytes (AISI=Neutrophils * Platelets * Monocytes / Lymphocytes).
Outcomes Measured
The primary endpoint is the occurrence of major adverse cardiovascular and cerebrovascular events (MACCEs), encompassing all-cause in-hospital mortality, revascularization, new-onset atrial fibrillation of any etiology, venous thromboembolism, and stroke. All-cause in-hospital mortality refers to death from any cause during hospitalization. Revascularization is defined as secondary stent placement during hospitalization following initial stent placement. New-onset atrial fibrillation is characterized by the absence of prior history of atrial fibrillation and confirmed through routine electrocardiogram, ambulatory electrocardiogram monitoring, or inpatient electrocardiographic monitoring. Secondary endpoints include contrast-induced nephropathy (CIN) risk and all-cause readmission rate. CIN is defined as a relative increase ≥ 25% or an absolute increase ≥ 44.2 μmol/L in serum creatinine concentration within 48–72 hours post-exposure to contrast agent; it excludes acute kidney injury due to other causes. Readmission for any reason was verified through medical records review or direct communication with patients or attending physicians. The mean follow-up duration for this study was one year.
Statistical Analysis
To assess the impact of AISI level on the clinical outcomes of patients with acute myocardial infarction, the median was stratified into high and low AISI groups. Baseline data were presented as frequency and percentage, and the comparison between groups was analyzed using the χ2 test. Continuous variables were assessed for normality using the K–S test, P-P plot, Q-Q plot, and frequency histogram; they were reported as mean±standard deviation (for normally distributed data). Differences between groups were analyzed using independent samples t-test for normally distributed data or median and interquartile range (IQR) for non-normally distributed data. The Mann–Whitney U rank sum test was used to compare differences between groups. We first conducted univariate logistic regression analysis, followed by multivariate analysis to control for potential confounders. The confounders considered included gender, age, smoking status, cardiac ejection fraction, history of bypass surgery, use of calcium channel blockers, ACEI/ARB/ARNI, β-blockers, statins, dual antiplatelet therapy, red blood cell count, monocyte count, platelet count, alanine aminotransferase, serum albumin, and glomerular filtration rate. Variables such as white blood cell count, lymphocyte count, aspartate aminotransferase, total cholesterol, and low-density lipoprotein were excluded due to collinearity (variance inflation factor [VIF]>5). After adjusting for these confounders, we performed subgroup analyses for high-risk patients and constructed forest plots (Figures 2–4) based on the analysis results. Odds ratio (OR)/hazard ratio (HR) along with their respective 95% confidence intervals (CI) were used to quantify risk magnitude. All statistical analyses were conducted using SPSS 26.0 software (IBM, Armonk, New York, USA).
 |
Figure 2 Predictors of all-cause in hospital mortality in patients with acute myocardial infarction. Forest plot for the effects sizes of individual predictors of all-cause in hospital mortality in patients with acute myocardial infarction. Abbreviations: GFR, glomerular filtration rate; BMI, body mass index; HDL-C, High-density lipoprotein cholesterol; OR, Odds-ratio; PCI, percutaneous coronary intervention. |
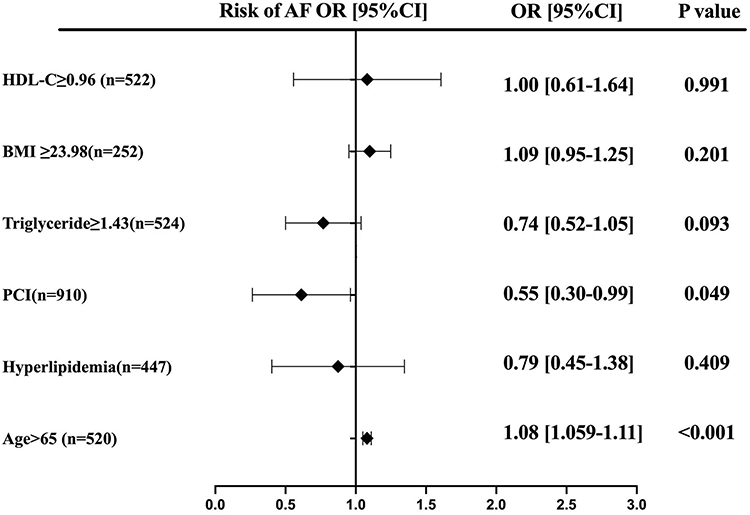 |
Figure 3 Predictors of atrial fibrillation in patients with acute myocardial infarction. Forest plot for the effects sizes of individual predictors of atrial fibrillation in patients with acute myocardial infarction. Abbreviations: AF, Atrial fibrillation; OR, Odds-ratio, HDL-C, High-density lipoprotein cholesterol; BMI, body mass index; PCI, percutaneous coronary intervention. |
 |
Figure 4 Predictors of CIN in patients with acute myocardial infarction. Forest plot for the effects sizes of individual predictors of CIN in patients with acute myocardial infarction. Abbreviations: ACEI/ARB/ARNI, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers or angiotensin receptor–neprilysin inhibitors; CIN, Contrast-induced nephropathy; OR, Odds-ratio; PCI, percutaneous coronary intervention. |
Results
Baseline Characteristics
This study included a total of 1044 patients, with an average age of 64.05±11.62 years. There were 186 female patients (17.6%), 899 patients received percutaneous coronary intervention (PCI) treatment (86.1%), 643 had hypertension (61.6%) and 411 had a history of diabetes (39.4%). The entire population was divided into two groups based on the AISI level (Q1 Group, ≤416.15, n=522; Q2 Group, ≥416.16, n=522). Patients in the high AISI group exhibited a lower left ventricular ejection fraction (LVEF) (Q1: 56.87±10.95 vs Q2: 53.61±11.07, p<0.001), and a smaller proportion had a history of CABG surgery (Q1: 2.7% vs Q2: 0.6%). We noticed that in terms of medication history, univariate analysis showed that patients with higher AISI levels used fewer therapeutic drugs (p<0.05), including antihypertensive drugs, dual antiplatelet therapy (DAPT), and lipid-lowering drugs, among others. Furthermore, individuals in the high AISI group exhibited elevated levels of white blood cells (WBC) (p<0.05), neutrophils (NEU) (p<0.05), monocytes (MONO) (p<0.05), and platelets (PLT) (p<0.05). They also demonstrated a tendency towards higher total cholesterol (TCHO) (p<0.05) and low-density lipoprotein cholesterol (LDL-C) (p<0.05), along with an increase in glomerular filtration rate (GFR) (p<0.05). Conversely, compared to those with high AISI levels, patients with lower AISI levels were more likely to have decreased aspartate aminotransferase (AST) (p<0.05) and alanine aminotransferase levels (ALT) (p<0.05) while exhibiting higher lymphocyte (LYM) (p<0.05) and albumin levels (ALB) (p<0.05). Additional data on the baseline characteristics of the study population can be found in Table 1.
 |
Table 1 Baseline Characteristics in Patients with Acute Myocardial Infarction |
AISI as a Predictor of Clinical Outcome
In the study population, the incidence of MACCEs was notably high, with 23 patients (2.2%) experiencing mortality. Univariate analysis revealed a strong association between high AISI levels and increased mortality risk, with this association remaining significant across various models (P<0.05). In Model 1, which adjusted for age and gender, each unit increase in AISI was associated with a 2.68-fold increase in the likelihood of death (OR 3.68; 95% CI 1.36–10.00, P<0.05). In Model 2, which accounted for all potential confounders, the risk of death remained elevated (OR 3.74; 95% CI 1.12–12.46; P<0.05). These results further confirm that higher AISI levels are positively correlated with an increased risk of mortality. Additionally, subgroup analysis of high-risk patients revealed that a BMI of ≥23.98 kg/m² was a significant risk factor for mortality, with the risk increasing as BMI increased (OR 1.31; 95% CI 1.01–1.71, P<0.05). Conversely, patients who underwent PCI had a 78% reduced risk of mortality compared to those who did not receive PCI (OR 0.22; 95% CI 0.08–0.66, P<0.05). Furthermore, a HDL-C level of ≥0.96 mmol/L was identified as a protective factor against mortality. For each unit increase in HDL-C, the likelihood of mortality decreased by 69% (OR 0.31; 95% CI 0.11–0.09, P<0.05) (Table 2 and Figure 2).
 |
Table 2 The Risk of Clinical Outcomes in Patients with Acute Myocardial Infarction |
In this study, a significant positive correlation was found between AISI levels and the incidence of AF (6.3% vs 10.5%, P<0.05). After controlling for age and sex in Model 1, the risk remained elevated (OR 1.90; 95% CI 1.19–3.02,P< 0.05). This association was further confirmed in Model 2, which adjusted for additional covariates (OR 1.71; 95% CI 1.01–2.91; P<0.05). Additionally, a more detailed analysis revealed that among patients aged ≥65 years, each additional year of age increased the likelihood of developing atrial fibrillation by 8% (OR 1.08; 95% CI 1.06–1.11; P<0.05). Furthermore, patients who underwent PCI had a 45% lower risk of developing atrial fibrillation compared to those who did not receive PCI treatment (OR 0.55; 95% CI 0.30–0.99; P<0.05) (Table 2 and Figure 3).
Furthermore, we found that the incidence of CIN in this study was 7.5%. Initially, without adjusting for any confounding factors, higher AISI scores were associated with an increased risk of CIN. After adjusting for age and sex, OR was 1.66 (95% CI 1.04–2.66; P<0.05). Further adjustments in Model 2, which included additional covariates, resulted in an adjusted odds ratio of 1.75 (95% CI 1.02–3.01; P<0.05), indicating an increased OR and suggesting that other covariates may influence the risk of CIN. Subgroup analyses revealed that being female was a protective factor against CIN, with women having a lower risk compared to men (OR 0.51; 95% CI 0.29–0.93; P<0.05). Additionally, patients who underwent PCI had a 52% lower risk of developing CIN compared to those who did not receive PCI treatment (OR 0.48; 95% CI 0.27–0.87; P<0.05). Conversely, age ≥65 years (OR 1.03; 95% CI 1.00–1.05; P<0.05) and preoperative use of β-blockers (OR 2.17; 95% CI 1.10–4.28; P<0.05) were identified as independent risk factors for CIN (Table 2 and Figure 4).
We also found that, even after adjusting for covariates in Model 1 and Model 2, the risk of undergoing repeat revascularization, venous thromboembolism, cerebrovascular events, and all-cause readmission remained similar between the Q2 and Q1 groups (P>0.05) (Table 2).
Discussion
As far as we know, this is the first larger study to use the novel inflammatory marker AISI as a predictor of clinical prognosis in patients with AMI, and this study confirms the clinical importance of AISI in patients with AMI.
AMI results from a complex interplay of pathological and physiological factors, including inflammation-mediated thrombus formation, plaque rupture, endothelial dysfunction, cardiac remodeling, and decreased cardiac function.18–22 Several studies have confirmed how elevated levels of systemic inflammation increase the risks associated with MACCEs following an AMI, emphasizing its close association with negative prognoses among affected individuals.21,23 However, further exploration is necessary regarding potential intercellular interactions influencing patient prognoses. The newly developed composite index AISI integrates four distinct components reflective of systemic inflammation and demonstrates superior predictive capabilities in terms of prognosis across conditions like hypertension and coronary heart disease.10,11 Higher AISI may indicate more pronounced inflammatory responses escalating adverse outcomes. Therefore, this study postulates that the association between AISI and the prediction of adverse cardiovascular events in AMI patients may be attributed to the pro-inflammatory effects of individual inflammatory cells.
Our study demonstrates that patients in the Q2 group face a higher risk of all-cause mortality compared to those in the Q1 group, aligning with current research.11 It is well-established that changes in microvascular permeability due to inflammatory responses are significant pathological alterations in AMI.24 Systemic inflammation can lead to abnormal platelet aggregation and adhesion to endothelial cells, resulting in localized ischemia, hypoxia, and microthrombus formation, which ultimately causes tissue necrosis.25 Abnormal decreases in lymphocyte counts indicate excessive lymphocyte death and subsequent immune system dysfunction. This lymphocyte apoptosis, coupled with increases in monocytes26 and neutrophils,25 collectively induces atherosclerotic plaque rupture and thrombosis, thereby increasing the risk of major adverse cardiovascular and cerebrovascular events (MACCEs) through inflammatory response activation. High AISI levels reflect disrupted immune function and intense inflammatory responses, contributing to an elevated risk of mortality in AMI patients. A study involving elderly AMI patients found that increased inflammatory responses were associated with a 3.09-fold increase in in-hospital mortality risk,27 further supporting this mechanism. Interestingly, our subgroup analysis revealed that HDL-L is a protective factor against mortality (P<0.05). This protective effect is attributed to the multiple roles of HDL-L particles in counteracting atherosclerosis.28 Additionally, our observations indicate that PCI intervention significantly reduces mortality risk by promoting blood flow restoration.29 These findings underscore the importance of focused monitoring for high-risk patients.
The pathophysiology of AF is complex, and our understanding of this condition remains limited.30 Recent research has highlighted that leukocyte-mediated inflammatory pathways can promote the differentiation, proliferation, and migration of atrial myocytes and fibroblasts, leading to abnormalities in the electrophysiological and mechanical functions of atrial myocytes, which can, in turn, trigger AF. Furthermore, AF itself can exacerbate the inflammatory response, creating a bidirectional relationship. For instance, AF can induce mechanical stress and ischemia-reperfusion injury in atrial myocytes, thereby activating inflammatory pathways.31 Some researchers have linked the occurrence of AF with preoperative systemic inflammatory markers, supporting a close relationship between inflammation and the onset of new AF.32,33 However, a study involving 1,450 patients undergoing cardiac surgery found no effect of preoperative inflammation levels on the incidence of postoperative AF.34 In our study, we observed that the incidence of AF increased with higher AISI levels. Specifically, each unit increase in AISI was associated with a 0.71-fold increase in the risk of AF in patients with AMI (P<0.05), further supporting the association between inflammation and the development of new-onset AF. Additionally, aging was identified as a prominent risk factor for the incidence, prevalence, and progression of AF. PCI treatment emerged as a protective factor against new-onset AF, as AMI can induce AF through inflammation and excessive chamber dilation, leading to increased oxygen demand. PCI, by improving hemodynamic status and alleviating myocardial ischemia and hypoxia, helps to mitigate these effects. Consequently, healthcare providers should pay special attention to patients not receiving PCI and consider initiating PCI treatment based on individual patient circumstances.
CIN is a common complication PCI, associated with a high incidence and mortality rate. The pathophysiology of CIN involves a complex interplay among various blood cells. Immune system dysregulation may adversely impact renal function, and systemic inflammation can alter renal blood flow.35 Platelets interact with leukocytes at sites of acute injury, exacerbating renal parenchymal cell damage through the production of pro-inflammatory cytokines, cytotoxic effects, and interactions with renal intrinsic cells.36,37 This suggests that higher levels of AISI correlate with increased inflammation and worsened renal injury. In our analysis, we observed a positive correlation between high AISI levels and CIN risk (P<0.05), which was confirmed even after adjusting for baseline confounding factors. These findings are consistent with other studies.38 Subgroup analyses of high-risk patients indicated that PCI acts as a protective factor against CIN (P<0.05), likely due to its improvement in renal hemodynamics, which reduces CIN risk. Conversely, preoperative use of β-blockers was identified as a risk factor for CIN, possibly due to increased toxicity to renal tubular cells. Additionally, age≥65 years was found to be associated with an increased risk of CIN, reflecting the decline in renal function with advancing age.39 Our study also found that male patients have a higher risk of CIN compared to female patients, potentially mediated by the beneficial effects of estrogen on the progression of renal disease.40,41 These findings underscore the need for healthcare providers to pay particular attention to older male patients.
Our study is subject to certain limitations. Firstly, this study is a single-center retrospective analysis, which inherently carries the risk of confounding factors, such as selection bias. To enhance the reliability of the findings, future research will aim to conduct prospective studies or validate the results across different populations. Second, a single blood draw is not a good proxy for a patient’s physical status, which may change considerably during the hospital stay. Lastly, this study was limited by a lack of follow-up. Despite these limitations, our study is the largest study to date and the first to explore the association between different levels of AISI and the prognosis of AMI patients. It provides evidence for improving patients’ clinical outcomes in the future.
Conclusion
AISI has the potential to serve as an early warning indicator for adverse prognosis in patients with acute myocardial infarction (AMI). This finding could facilitate the development of new therapeutic strategies aimed at managing low-level inflammation and myocardial injury. Additionally, AISI offers a practical and informative biomarker that can assist clinicians in evaluating and analyzing the condition of AMI patients. Its prognostic value can guide clinicians in assessing patient outcomes and making informed treatment decisions. However, further prospective studies and validation across diverse populations are needed to confirm the feasibility and generalizability of this approach.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request (Please contact Yanjuan Lin, [email protected]).
Acknowledgments
The authors thank all participants who were involved with this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research was funded by Fujian Province Center for Cardiovascular Medicine Construction Project (Grant number: NO.2021-76) and Key Laboratory of Cardio-Thoracic Surgery (Fujian Medical University), Fujian Province University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Benjamin EJ, Muntner P, Alonso A, et al. Heart Disease and Stroke Statistics-2019 Update: a Report From the American Heart Association. Circulation. 2019;139(10):e56–e528. doi:10.1161/CIR.0000000000000659
2. Crea F, Libby P. Acute Coronary Syndromes: the Way Forward From Mechanisms to Precision Treatment. Circulation. 2017;136(12):1155–1166. doi:10.1161/CIRCULATIONAHA.117.029870
3. Matter MA, Paneni F, Libby P, et al. Inflammation in acute myocardial infarction: the good, the bad and the ugly. Eur Heart J. 2024;45(2):89–103. doi:10.1093/eurheartj/ehad486
4. Ly HQ, Kirtane AJ, Murphy SA, et al. Association of platelet counts on presentation and clinical outcomes in ST-elevation myocardial infarction (from the TIMI Trials). Am J Cardiol. 2006;98(1):1–5. doi:10.1016/j.amjcard.2006.01.046
5. Karakayali M, Altunova M, Yakisan T, et al. The Relationship between the Systemic Immune-Inflammation Index and Ischemia with Non-Obstructive Coronary Arteries in Patients Undergoing Coronary Angiography. Arq Bras Cardiol. 2024;121(2):e20230540. doi:10.36660/abc.20230540
6. Paliogiannis P, Ginesu GC, Tanda C, et al. Inflammatory cell indexes as preoperative predictors of hospital stay in open elective thoracic surgery. ANZ J Surg. 2018;88(6):616–620. doi:10.1111/ans.14557
7. Tuzimek A, Dziedzic EA, Beck J, Kochman W. Correlations Between Acute Coronary Syndrome and Novel Inflammatory Markers (Systemic Immune-Inflammation Index, Systemic Inflammation Response Index, and Aggregate Index of Systemic Inflammation) in Patients with and without Diabetes or Prediabetes. J Inflamm Res. 2024;17:2623–2632. doi:10.2147/JIR.S454117
8. Wang HK, Wei Q, Yang YL, Lu TY, Yan Y, Wang F. Clinical usefulness of the lymphocyte-to-monocyte ratio and aggregate index of systemic inflammation in patients with esophageal cancer: a retrospective cohort study. Cancer Cell Int. 2023;23(1):13. doi:10.1186/s12935-023-02856-3
9. Xie W, Xu Z, Qiu Y, et al. A Novel Nomogram Combined the Aggregate Index of Systemic Inflammation and PIRADS Score to Predict the Risk of Clinically Significant Prostate Cancer. Biomed Res Int. 2023;2023:9936087. doi:10.1155/2023/9936087
10. Zinellu A, Collu C, Nasser M, et al. The Aggregate Index of Systemic Inflammation (AISI): a Novel Prognostic Biomarker in Idiopathic Pulmonary Fibrosis. J Clin Med. 2021;10(18):4134. doi:10.3390/jcm10184134
11. Luo WM Correlation between the Aggregate Index of System Inflammation and Severity and Prognosis of Coronary Artery Disease [dissertation]. China: Southern Medical University; 2024.
12. Xiu J, Lin X, Chen Q, et al. The aggregate index of systemic inflammation (AISI): a novel predictor for hypertension. Front Cardiovasc Med. 2023;10:1163900. doi:10.3389/fcvm.2023.1163900
13. Bhat T, Teli S, Rijal J, et al. Neutrophil to lymphocyte ratio and cardiovascular diseases: a review. Expert Rev Cardiovasc Ther. 2013;11(1):55–59. doi:10.1586/erc.12.159
14. Thygesen K, Alpert JS, Jaffe AS, et al. Fourth Universal Definition of Myocardial Infarction. Circulation. 2018;138(20):e618–651. doi:10.1161/CIR.0000000000000617
15. American Medical Association. The Complete Official Codebook: ICD-10-CM. USA: Optum360, LLC; 2016.
16. Zhu JR, Gao RL, Zhao SP, et al. Guidelines for prevention and treatment of dyslipidemia in adults in China. Chin Circ J. 2016;31:937–953.
17. Levey AS, Coresh J, Greene T, et al. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med. 2006;145(4):247–254. doi:10.7326/0003-4819-145-4-200608150-00004
18. Björkegren JLM, Lusis AJ. Atherosclerosis: recent developments. Cell. 2022;185(10):1630–1645.
19. Mehta SR, Yusuf S, Peters RJ, et al. Effects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention: the PCI-CURE study. Lancet. 2001;358(9281):527–533. doi:10.1016/S0140-6736(01)05701-4
20. Massberg S, Brand K, Grüner S, et al. A critical role of platelet adhesion in the initiation of atherosclerotic lesion formation. J Exp Med. 2002;196(7):887–896. doi:10.1084/jem.20012044
21. Harrington RA. Targeting inflammation in coronary artery disease. N Engl J Med. 2017;377(12):1197–1198. doi:10.1056/NEJMe1709904
22. Chen Y, Li X, Lin X, et al. Complement C5a induces the generation of neutrophil extracellular traps by inhibiting mitochondrial STAT3 to promote the development of arterial thrombosis. Thromb J. 2022;20(1):24. doi:10.1186/s12959-022-00384-0
23. Schmitz T, Harmel E, Heier M, Peters A, Linseisen J, Meisinger C. Inflammatory plasma proteins predict short-term mortality in patients with an acute myocardial infarction. J Transl Med. 2022;20(1):457. doi:10.1186/s12967-022-03644-9
24. Taqueti VR, Di Carli MF, Jerosch-Herold M, et al. Increased microvascularization and vessel permeability associate with active inflammation in human atheromata. Circ Cardiovasc Imaging. 2014;7(6):920–929. doi:10.1161/CIRCIMAGING.114.002113
25. Kim KH, Barazia A, Cho J, Real-time imaging of heterotypic platelet-neutrophil interactions on the activated endothelium during vascular inflammation and thrombus Formation in live mice. J Vis Exp. 2013;74:50329. doi:10.3791/50329
26. Ankeny RF, Hinds MT, Nerem RM. Dynamic shear stress regulation of inflammatory and thrombotic pathways in baboon endothelial outgrowth cells. Tissue Eng Part A. 2013;19(13–14):1573–1582. doi:10.1089/ten.tea.2012.0300
27. Chen Y, Chen S, Han Y, Xu Q, Zhao X. Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio are Important Indicators for Predicting in-Hospital Death in Elderly AMI Patients. J Inflamm Res. 2023;16:2051–2061. doi:10.2147/JIR.S411086
28. Barter PJ, Nicholls S, Rye KA, et al. Antiinflammatory properties of HDL. Circ Res. 2004;95(8):764–772. doi:10.1161/01.RES.0000146094.59640.13
29. Mylotte D, Morice MC, Eltchaninoff H, et al. Primary percutaneous coronary intervention in patients with acute myocardial infarction, resuscitated cardiac arrest, and cardiogenic shock: the role of primary multivessel revascularization. JACC: Cardiovasc Interv. 2013;6(2):115–125. doi:10.1016/j.jcin.2012.10.006
30. Li J, Solus J, Chen Q, et al. Role of inflammation and oxidative stress in atrial fibrillation. Heart Rhythm. 2010;7(4):438–444. doi:10.1016/j.hrthm.2009.12.009
31. Friedrichs K, Klinke A, Baldus S. Inflammatory pathways underlying atrial fibrillation. Trends Mol Med. 2011;17(10):556–563. doi:10.1016/j.molmed.2011.05.007
32. Heijman J, P MA, Veleva T, et al. Atrial Myocyte NLRP3/CaMKII Nexus Forms a Substrate for Postoperative Atrial Fibrillation. Circ Res. 2020;127(8):1036–1055. doi:10.1161/CIRCRESAHA.120.316710
33. Nomani H, Reiner Ž, Reiner Ž, et al. Statin Therapy in Post-Operative Atrial Fibrillation: focus on the Anti-Inflammatory Effects. J Cardiovasc Dev Dis. 2021;8(3):24. doi:10.3390/jcdd8030024
34. Navani RV, Baradi A, Colin Huang KL, et al. Preoperative Platelet-to-Lymphocyte Ratio Is Not Associated With Postoperative Atrial Fibrillation. Ann Thorac Surg. 2020;110(4):1265–1270. doi:10.1016/j.athoracsur.2020.02.008
35. Radi ZA. Immunopathogenesis of Acute Kidney Injury. Toxicol Pathol. 2018;46(8):930–943. doi:10.1177/0192623318799976
36. Jansen MPB, Florquin S, Roelofs JJTH. The role of platelets in acute kidney injury. Nat Rev Nephrol. 2018;14(7):457–471. doi:10.1038/s41581-018-0015-5
37. Cao C, Yao Y, Zeng R. Lymphocytes: versatile Participants in Acute Kidney Injury and Progression to Chronic Kidney Disease. Front Physiol. 2021;12:729084. doi:10.3389/fphys.2021.729084
38. Karauzum I, Karauzum K, Hanci K, Gokcek D, Kalas B, Ural E. The Utility of Systemic Immune-Inflammation Index for Predicting Contrast-Induced Nephropathy in Patients with ST-Segment Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention. Cardiorenal Med. 2022;12(2):71–80. doi:10.1159/000524945
39. Palli E, Makris D, Papanikolaou J, Garoufalis G, Zakynthinos E. Contrast-induced nephropathy in aged critically ill patients. Oxid Med Cell Longev. 2014;2014:756469.
40. Dubey RK, Jackson EK. Estrogen-induced cardiorenal protection: potential cellular, biochemical, and molecular mechanisms. Am J Physiol Renal Physiol. 2001;280(3):F365–F388. doi:10.1152/ajprenal.2001.280.3.F365
41. Neugarten J, Golestaneh L, Kolhe NV. Sex differences in acute kidney injury requiring dialysis. BMC Nephrol. 2018;19(1):131. doi:10.1186/s12882-018-0937-y
42. Jahangir A, Lee V, Friedman PA, et al. Long-term progression and outcomes with aging in patients with lone atrial fibrillation: a 30-year follow-up study. Circulation. 2007;115(24):3050–3056. doi:10.1161/CIRCULATIONAHA.106.644484
43. Ma LY, Wu YZ, Wang W, Chen WW. Interpretation of the report on cardiovascular diseases in China (2017). Chin J Cardiova Med. 2018;23(1):3–6.
44. Kornej J, Borschel CS, Benjamin EJ, Schnabel RB. Epidemiology of atrial fibrillation in the 21st Century: novel methods and new insights. Circ Res. 2020;127(1):4–20. doi:10.1161/CIRCRESAHA.120.316340
45. Ahmed HM, Miller M, Nasir K, et al. Primary Low Level of High-Density Lipoprotein Cholesterol and Risks of Coronary Heart Disease, Cardiovascular Disease, and Death: results From the Multi-Ethnic Study of Atherosclerosis. Am J Epidemiol. 2016;183(10):875–883. doi:10.1093/aje/kwv305
46. Staerk L, Sherer JA, Ko D, Benjamin EJ, Helm RH. Atrial fibrillation: epidemiology, pathophysiology, and clinical outcomes. Circ Res. 2017;120(9):1501–1517. doi:10.1161/CIRCRESAHA.117.309732
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.