")
Back to Journals » Risk Management and Healthcare Policy » Volume 18
Association Between Weight-Adjusted Waist Circumference Index and Metabolic Disease-Associated Fatty Liver Disease: A Retrospective Study
Authors Tang T, Fan H, Yu Q, Rao X, Shi Y, Tong X, Feng L, Xu Z, Fu X, Chen J, Zhang X, Tang J, Wang H, Wang M
Received 16 March 2025
Accepted for publication 7 July 2025
Published 12 July 2025 Volume 2025:18 Pages 2387—2399
DOI https://doi.org/10.2147/RMHP.S524872
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Ting Tang,1,* Hua Fan,2,* Qingwen Yu,1 Xiyun Rao,1 Yongmin Shi,1 Xuhan Tong,1 Lanlan Feng,1 Zhao Xu,1 Xinyan Fu,1 Juan Chen,1 Xingwei Zhang,1 Jiake Tang,1 Hu Wang,1 Mingwei Wang1,3– 6
1Department of Cardiology, the Affiliated Hospital of Hangzhou Normal University, Hangzhou Normal University, Hangzhou, Zhejiang, 310015, People’s Republic of China; 2School of Clinical Medicine, The First Affiliated Hospital of Henan University of Science and Technology, Luoyang, Henan, 471003, People’s Republic of China; 3Zhejiang Key Laboratory of Medical Epigenetics, Hangzhou Normal University, Hangzhou, Zhejiang, 310015, People’s Republic of China; 4Engineering Research Center of Mobile Health Management System&Ministry of Education, Hangzhou Normal University, Hangzhou, Zhejiang, 310015, People’s Republic of China; 5Department of Cardiology, Hangzhou Lin’an Fourth People’s Hospital, Hangzhou, Zhejiang, 311321, People’s Republic of China; 6Department of Cardiology, Jiande First People’s Hospital, Hangzhou, Zhejiang, 311600, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hu Wang, Email [email protected] Mingwei Wang, Email [email protected]
Background: Metabolic disease-associated fatty liver disease has brought significant challenges to public health and social-economics. There is a need for a straightforward and effective method to screen for metabolic disease-associated fatty liver disease. The weight-adjusted waist circumference index offers a comprehensive reflection of visceral fat accumulation and skeletal muscle loss. This study aims to explore the relationship between weight-adjusted waist circumference index and hepatic steatosis and hepatic fibrosis.
Methods: This single-centered study screened 288 participants from the outpatient department of the Affiliated Hospital of Hangzhou Normal University (Hangzhou, China). Multiple linear regression models were utilized to assess the association between weight-adjusted waist circumference index and hepatic steatosis and hepatic fibrosis. The subgroup analysis was carried out according to sex, smoking, drinking, BMI, cardiovascular disease, diabetes and hypertension.
Results: Metabolic disease-associated fatty liver disease was diagnosed in 185 out of 288 patients. Multivariate linear regression analysis indicated a positive linear correlation between weight-adjusted waist circumference index and hepatic steatosis and hepatic fibrosis (P < 0.05). Analysis of subgroups revealed a stronger positive correlation between weight-adjusted waist circumference index and controlled attenuation parameter among participants aged 18– 59 years and smokers (P < 0.05). Positive correlations between weight-adjusted waist circumference index and hepatic fibrosis were observed in participants who were alcohol consumers, male, had a body mass index of > 28, and with diabetes (P < 0.05).
Conclusion: We report a significant linear positive correlation between weight-adjusted waist circumference index and metabolic disease-associated fatty liver disease, suggesting that weight-adjusted waist circumference index is a potential indicator for metabolic disease-associated fatty liver disease screening.
Keywords: hepatic steatosis, hepatic fibrosis, abdominal obesity, weight-adjusted waist index, metabolic-associated fatty liver disease, cross-sectional study
Background
Non-alcoholic fatty liver disease (NAFLD) has emerged as the predominant liver disorder worldwide, presenting a significant challenge to public health and socioeconomic systems.1 In Asia, the prevalence of NAFLD surpasses the global average, reaching 27.37%, and in China, the prevalence of NAFLD has increased from 17% in 2003 to 22.4% in 2012.2,3 NAFLD is intricately linked to metabolic abnormalities, especially overweight/obesity and type 2 diabetes mellitus (T2DM),4 with obesity directly contributing to its rising incidence.2,5 To better characterize these fatty liver conditions in the context of metabolic dysfunction, an international expert group proposed redefining NAFLD as metabolic-associated fatty liver disease (MAFLD).6,7 Compared with NAFLD, MAFLD is more adept at identifying individuals at a high risk of fatty liver disease.8 Importantly, MAFLD increases the risk of various complications, including intrahepatic complications such as cirrhosis and hepatocellular carcinoma, and extrahepatic complications such as cardiovascular disease and extrahepatic malignancies.2 Hence, accurate assessment of hepatic steatosis and hepatic fibrosis in MAFLD is essential. However, traditional diagnostic methods such as B-ultrasound and CT entail high costs,9 while the liver biopsy is invasive.10,11 And vibration-controlled transient elastography suffers from accuracy limitations.12–14 Consequently, there is an urgent need for an economical and simple MAFLD screening approach to alleviate the burden it imposes on individuals, families, and healthcare systems.
Both increased body mass index (BMI) and waist circumference (WC) contribute to the degree of fibrosis in MAFLD, as evidenced by established correlations.15 While BMI and WC are common obesity indices, BMI does not distinguish between subcutaneous fat from visceral fat.16 To better capture abdominal obesity, Park et al introduced a novel obesity anthropometric index—the weight-adjusted waist circumference index (WWI). Calculated as WC divided by the square root of body weight, WWI more accurately reflects centrally distributed obesity independent of weight.17 Furthermore, compared with BMI and WC, WWI has demonstrated consistent applicability among different racial and ethnic groups and exhibits superior accuracy in predicting cardiovascular disease mortality risk compared to BMI and WC.18,19 However, the research on the relationship between WWI and MAFLD is controversial. A previous study by Shen et al found that the relationship between WWI and hepatic fibrosis is nonlinear, and the relationship between WWI and hepatic steatosis is linear, A linear correlation between WWI and hepatic fibrosis was found by Hu et al20,21 Therefore, further investigation is needed to elucidate this relationship.
In order to understand the relationship between obesity and MAFLD more accurately, this study aims to investigate the relationship between WWI and MAFLD using data collected from the Affiliated Hospital of Hangzhou Normal University.
Method
Study Population
This unique cross-sectional study, conducted at a single center on behalf of the Chinese Medical Doctor Association Tasly Fatty Liver College, aimed to investigate the association between WWI and MAFLD. Outpatients were recruited from the Affiliated Hospital of Hangzhou Normal University between March 1, 2021, and October 1, 2023. This study is a retrospective research project that has obtained approval from the Ethics Committee of Hangzhou Normal University Affiliated Hospital and informed consent has been waived (No.2024 (E2) -KS- 024). The study complied with the provisions of the Declaration of Helsinki and protects the personal privacy of research subjects, ensuring data confidentiality.
Initially, 309 non-pregnant participants were recruited. We further excluded participants aged <18 years (n = 2), lacking controlled attenuation parameter (CAP) data (n = 4), lacking WC data (n = 6), lacking weight data (n = 1), and those with duplicated data (n = 3). Participants who ingested at least 210 g/week of alcohol (males) (n = 1) and 140 g/week (females) (n = 2) were also excluded. Subjects with viral hepatitis and cryptogenic fatty liver were also excluded (n = 2). Ultimately, 288 participants were included in this investigation (Figure 1).
 |
Figure 1 Flowchart of the sample selection from outpatient patients at the Affiliated Hospital of Hangzhou Normal University. |
Measurement of Hepatic Steatosis and Hepatic Fibrosis
MAFLD is defined as one of the following conditions when there is fatty deformation in the liver: (1) BMI ≥23 kg/m2 (Asian population), or WC >94 cm (males) and >80 cm (females); (2) Fasting blood glucose level ≥5.6 mmol/L (100 mg/dL), or blood glucose level ≥7.8 mmol/L (≥140 mg/dL) after 2 h of sugar loading, or glycated hemoglobin A1c (HbA1c) ≥5.7% (39 mmol/L), or T2DM or treatment of T2DM; (3) Blood pressure ≥130/85 mmHg or specific antihypertensive drug treatment. (4) Plasma triglyceride (TG) ≥1.70 mmol/L (150 mg/dL) or lipid-lowering treatment. (5) Plasma high-density lipoprotein cholesterol (HDL-C) ≤1.0 mmol/L (40 mg/dL) in males, ≤1.3 mmol/L (50 mg/dL) in females, or lipid-lowering treatment.22 In addition, hepatic steatosis and hepatic fibrosis were assessed among participants using the FibroScan® machine, measuring the CAP and liver stiffness measurements (E values). A median CAP value ≥274 dB/m was considered indicative of hepatic steatosis,23 while an E value ≥8.0 kPa signaled hepatic fibrosis.24 These thresholds were utilized to identify crucial parameters associated with MAFLD within the study cohort.
Definition of WWI
WWI is a measure of abdominal obesity and is calculated as the WC (cm) divided by the square root of body weight (kg), expressed as cm/kg2.17,19 WC and weight measurements were obtained by trained health technicians. Body weight was measured by a digital weight scale with a precision of 0.1 kg, while WC was measured by a retractable tape at the end of exhalation, with a precision of 0.1 cm.
WWI scores were divided into quartiles (quartile 1–quartile 4), with respective ranges of 7.14–10.16, 10.16–10.57, 10.57–11.10, and 11.10–12.58, respectively, and each quartile comprising 72 participants.
Variables
Based on previous studies, the following variables were screened to investigate the effect of multiple variables on the relationship between WWI and hepatic steatosis and hepatic fibrosis.15,23,25–30 Table 1 presents the variables along with their respective details.
 |
Table 1 Characteristics of the Participants |
Covariates for demographic and past medical history, such as age, sex, height, WC, weight, hypertension, T2DM, cardiovascular disease (CVD), alcohol consumption, and smoking, were collected from the Affiliated Hospital of Hangzhou Normal University. Alcohol consumption status was categorized as never or small drinking (<40 g/w), and light or above drinking (≥40 g/w). Additionally, BMI was calculated as body weight divided by the square of height, expressed in kg/m2.31 Furthermore, laboratory analyses included fasting elbow venous blood (3 mL) measurements of total cholesterol (TC, mmol/L), triglyceride (TG, mmol/L), aspartate aminotransferase (AST, IU/L), alanine aminotransferase (ALT, IU/L), serum uric acid (SUA, μmol/L), high-density lipoprotein cholesterol (HDL-C, mmol/L), and low-density lipoprotein cholesterol (LDL-C, mmol/L).
Statistical Analysis
All variables were summarized in union descriptive statistics, expressing continuous variables as mean ±standard deviation and dichotomized variables as values and percentages. Differences between WWI quartiles were assessed using chi-square tests, and single-factor ANOVA tests, while the Kruskal Wallis test was performed for non-normally distributed data. Sensitivity analysis was used to evaluate the robustness of WWI quartiles. Multiple linear regression analysis encompassing three models was employed to evaluate the relationship between WWI and hepatic steatosis and hepatic fibrosis. Notably, Model 1: unadjusted; Model 2: adjusted for age and gender; Model 3: adjusted for age, sex, BMI, hypertension, diabetes, CVD, alcohol consumption, smoking, TC, TG, ALT, AST, SUA, HDL-C, and LDL-C. We used a stratified multivariate logistic regression model to analyze the relationship between WWI and hepatic steatosis and hepatic fibrosis in subgroups. The covariates covered in the subgroup analysis included age, alcohol consumption, BMI, CVD, T2DM, sex, hypertension, and smoking. Statistical analyses were conducted using the SPSS software, with P ≤ 0.05 reflecting a statistically significant difference. This comprehensive approach ensures a rigorous exploration of the relationships under consideration.
Result
Participant Characteristics
Following rigorous screening, a total of 288 participants were included in this study. Table 1 illustrates the relationship between baseline data and WWI quartiles. All participants (182 males and 106 females) were of age ≥18 years. As WWI increased, a gradual rise in male participants and BMI and WC levels was observed (P < 0.05). Notably, a decrease in HDL-C levels was observed with increasing WWI (P < 0.05) (Table 1).
Association Between the WWI and CAP
Across all three models, a positive linear correlation was observed between WWI and hepatic steatosis (P < 0.05). Upon adjusting for all covariates in Model 3, each one-unit increase in WWI score corresponded to a 73.64 dB/m increase in CAP (β = 73.64; 95% CI 4.42; 10.78; P < 0.001). Furthermore, quartile analysis of WWI revealed a significant relationship between WWI and hepatic steatosis. In Model 1, the β values of CAP in Q2, Q3, and Q4 were 19.51, 32.61, and 33.62, respectively (P < 0.05). Similarly, in Model 2, the β-values of CAP in Q2, Q3, and Q4 were 19.59, 33.78, and 38.8, respectively, when compared to the lower quartile (Q1) (P < 0.05) (Table 2).
 |
Table 2 The Association Between WWI with CAP and E-Value |
Association Between the WWI and E Value
Model 1 demonstrated that the E value increases by 5.11 kPa for each unit of WWI score (β = 5.11; 95% CI: 4.56, 5.67; P < 0.000). Similarly, in Model 2, For every unit increase in WWI score the E value increases by 5.07 kPa (β = 5.07; 95% CI: 3.82, 6.32; P < 0.000). However, when considering the WWI quartile, no statistically significant positive association between WWI and hepatic fibrosis was observed across all models (P > 0.05) (Table 2).
Subgroup Analysis
Subgroup analyses were conducted to explore potential variations in the correlation between WWI with CAP/E values across different population characteristics. Stratified multivariate regression analyses were performed for various demographic factors including age groups, alcohol consumption, BMI, CVD, T2DM, sex, hypertension, and smoking (Figures 2 and 3).
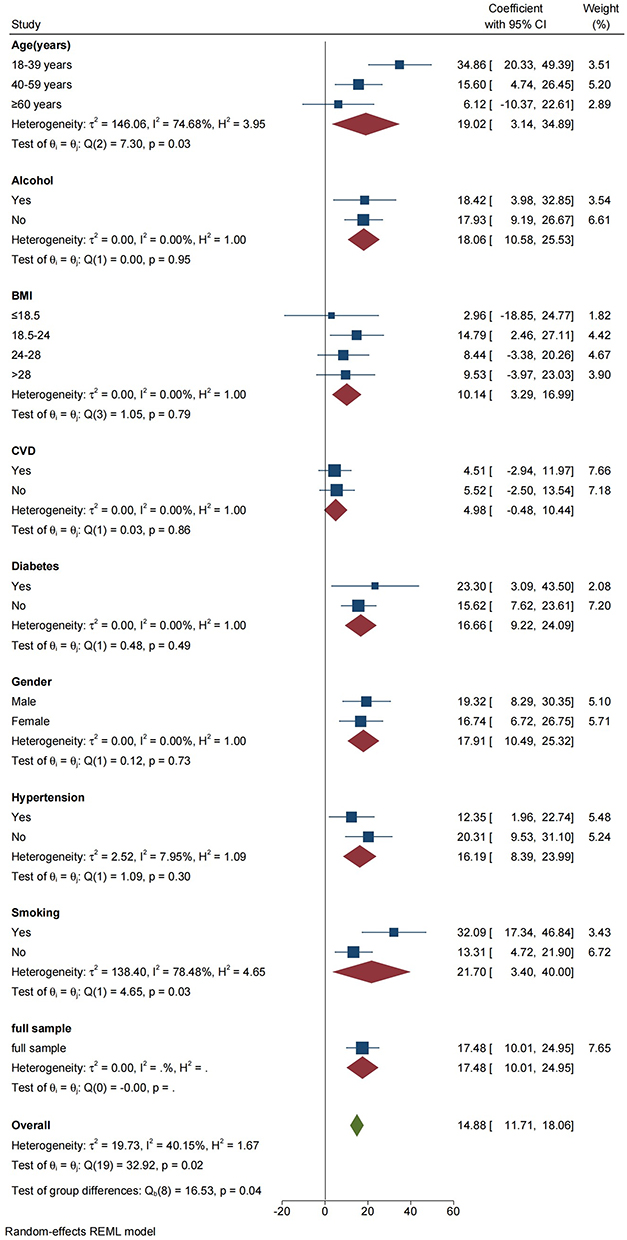 |
Figure 2 Subgroup analysis for the association between WWI and hepatic steatosis. |
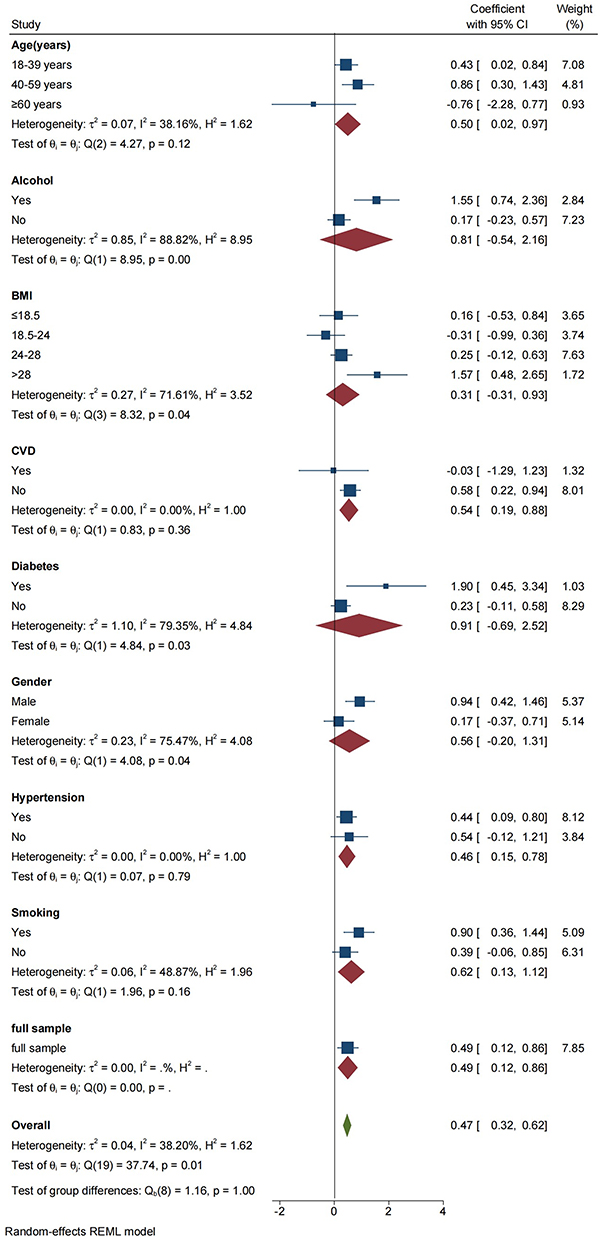 |
Figure 3 Subgroup analysis for the association between WWI and hepatic fibrosis. |
Notably, a stronger positive correlation between WWI and CAP was observed in smokers and individuals aged 18–59 years (P < 0.05) (Figure 2). Similarly, drinking, male, with BMI >28, and participants with T2DM exhibited a positive correlation between WWI and E values (P < 0.05) (Figure 3).
Discussion
Given the global impact and escalating risks associated with MAFLD, there is an urgent need for early screening and vigilant monitoring of this condition. Previous studies underscore the significance of BMI, WC, waist-to-height ratio, and triglyceride-glucose index in identifying MAFLD risk.32–34 Building upon this foundation, we investigated the connection between WWI and MAFLD. This study demonstrated a significant linear correlation between WWI and hepatic steatosis and fibrosis. In models 1, 2 and 3, for every unit of WWI score increase, the CAP value increases by 248.43 dB/m, 287.69 dB/m and 73.64 dB/m respectively. When considering the WWI quartile, there is a significant relationship between WWI and hepatic steatosis. In models 1, 2, for every unit of WWI score increase, the E value increases by 5.11 kPa and 5.07kPa respectively. Subgroup analysis further showed that WWI was significantly and positively associated with hepatic steatosis in smokers and individuals aged 18–59 years, whereas WWI was positively associated with hepatic fibrosis in participants who consumed alcohol, were male, had a BMI >28, and had T2DM.
Characterized by hepatic lipid accumulation and metabolic disturbances.22 The incidence of MAFLD has risen steadily worldwide in recent years.35 Lipid metabolism disorders are in turn closely related to obesity.4 Previous studies have established the contribution of increased BMI and WC to the degree of fibrosis in MAFLD.15 While BMI and WC are conventional metrics for obesity evaluation.31 It is crucial to recognize that obesity encompasses excess adipose tissues and not just weight gain.36 BMI cannot distinguish between muscle tissues and adipose tissues.37–39 WC is also an index that depends on the overall body weight.17 Conversely, WWI, derived from standardized body weight, offers a comprehensive assessment inclusive of both muscle and fat components. This measure accurately reflects high-fat mass and low muscle mass, while remaining insensitive to overall body weight fluctuations.19 A large number of studies have shown a positive correlation among WWI and T2DM, hyperuricemia, CVD (arteriosclerosis), and high risk of all-cause death, and WWI is positively correlated with hyperuricemia in patients with hypertension, negative correlation between SUA levels and coronary artery collateral opening. However, research on the relationship between WWI and MAFLD remains limited.17,40–43 Given that MAFLD is mainly characterized by abdominal obesity and visceral fat accumulation, and considering WWI’s positive correlation with abdominal fat and visceral fat.18,44,45 This study delved into the correlation between WWI and MAFLD to provide additional evidence for the prevention and screening of MAFLD. This analysis showed that WWI had a significant linear positive correlation with hepatic steatosis and fibrosis, underscoring the key role of abdominal obesity in the development of hepatic steatosis. Furthermore, WWI holds promise as a simple and effective indicator for early MAFLD screening.
Analyzing MAFLD characteristics and its relationship with metabolic disorders underscores the close relationship between MAFLD development and abdominal obesity, skeletal muscle loss, and significant visceral fat accumulation.44–46 This association is attributed to the anatomical proximity of visceral adipose tissue to the liver, facilitating the breakdown of visceral fat into non-esterified fatty acids (NEFA). NEFA can induce liver metabolic disorders, including glucose intolerance, dyslipidemia, hyperinsulinemia, and insulin resistance. Despite the potential of insulin to enhance NEFA re-lipidation, visceral fat resistance toward this process.47 In addition, liver disease can promote an inflammatory response.48 This conclusion not only emphasizes the correlation between visceral adiposity, insulin resistance, and hepatic inflammation but also supports our finding of a positive correlation between WWI and MAFLD.
This study possesses several advantages compared to previous studies on the relationship between WWI and MAFLD. This is the first study to use the new definition of MAFLD to analyzed patient data from the Affiliated Hospital of Hangzhou Normal University in China. Through rigorous adjustment for various potential covariates, a positive correlation between WWI and MAFLD was revealed, which is consistent with previous research results. In addition, through subgroup analysis, a stronger positive association between WWI and hepatic steatosis was found for the first time among smokers. Importantly, while previous studies by Shen et al found WWI’s relationship with hepatic fibrosis to be non-linear, and with hepatic steatosis to be linear, Hu et al found the opposite.20,21 This study demonstrates a linear positive correlation between WWI and MAFLD. This discrepancy could be attributed to population-specific characteristics captured in the study, bringing this findings closer to the characteristics of the local population.
Furthermore, subgroup analysis identified specific demographics with significant correlations between WWI and MAFLD, providing tailored clinical recommendations. Notably, there was a significant correlation between WWI and CAP for participants aged 18–59 years, compared with those aged >60 years. A study based on the Chinese population reported that the fat mass and visceral fat level increased in the 55–65-age group, but decreased in the 70–85-age group, which indicates that the younger population has higher fat mass and visceral fat levels.49 This may be due to the differences in fat mass and visceral fat among different races and cultures. Moore et al observed that people in China aged >65 years tend to have a healthier lifestyle.50 Notably, among smokers, a stronger positive correlation was observed between WWI and CAP. In addition, drinking, male gender, BMI >28, and participants with T2DM exhibited a positive relationship between WWI and hepatic fibrosis, which is consistent with established influences on MAFLD.4,51–54
However, this study has limitations. First, MAFLD diagnosis relied solely on CAP and E values, without liver biopsy confirmation. Second, the cross-sectional study design itself cannot determine the causal relationship between WWI and MAFLD. Third, Although we include covariates as much as possible, the development of hepatic steatosis and hepatic fibrosis involves many potential factors, so there may still be unmeasured confounding factors, then, only individuals aged ≥18 years were included, which limits generalizability to those aged <18 years. Finally, the study focused on patients from the affiliated hospital of hangzhou normal university, potentially limiting the applicability of our findings to other geographic regions or ethnic populations.
Conclusion
In this study, a significant positive correlation was found between WWI and MAFLD. Specifically, individuals aged 18–59 years and smokers should be particularly vigilant regarding hepatic steatosis development. Moreover, individuals who drink, males, those with a BMI >28, and participants with diabetes should closely monitor the progression to hepatic fibrosis. These findings are of great significance to the prevention and intervention of MAFLD, and the follow-up study can further explore the relationship between WWI and MAFLD in populations with high-risk characteristics. Moving forward, given that WWI is an easily measurable indicator, we propose that WWI could serve as a simple and effective potential indicator for the early screening of MAFLD.
Data Sharing Statement
All study data can be requested from the corresponding author.
Consent for Publication
All authors agree to publication.
Acknowledgments
We thank EditorBar (https://www.editorbar.com/) for editing this manuscript.
Funding
This study was supported by Hangzhou biomedicine and health industry development support science and technology project (No. 2022WJCY024;No. 2021WJCY238; No. 2021WJCY047;No. 2021WJCY115); Hangzhou Natural Science Foundation of China under Grant(No.2024SZRZDH250001); Medical and Technology Project of Zhejiang Province (No. 2024KY1348); Hangzhou Normal University Dengfeng Project Clinical Medicine Revitalization Plan Jiande Hospital Special Project (No. LCYXZXJH001).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Younossi Z, Anstee QM, Marietti M, et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2018;15(1):11–20. doi:10.1038/nrgastro.2017.109
2. Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease—Meta‐analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64:73. doi:10.1002/hep.28431
3. Xiao J, Wang F, Wong N-K, et al. Global liver disease burdens and research trends: analysis from a Chinese perspective. J Hepatol. 2019;71:212–221. doi:10.1016/j.jhep.2019.03.004
4. Polyzos SA, Kountouras J, Mantzoros CS. Obesity and nonalcoholic fatty liver disease: from pathophysiology to therapeutics. Metabolism. 2019;92:82–97. doi:10.1016/j.metabol.2018.11.014
5. Brunt EM, Wong VW-S, Nobili V, et al. Nonalcoholic fatty liver disease. Nat Rev Dis Primers. 2015;1:15080. doi:10.1038/nrdp.2015.80
6. Eslam M, Sanyal AJ, George J. International consensus panel. MAFLD: a consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology. 2020;158:1999–2014.e1. doi:10.1053/j.gastro.2019.11.312
7. Younossi ZM, Rinella ME, Sanyal AJ, et al. From NAFLD to MAFLD: implications of a premature change in terminology. Hepatology. 2021;73:1194. doi:10.1002/hep.31420
8. Lin S, Huang J, Wang M, et al. Comparison of MAFLD and NAFLD diagnostic criteria in real world. Liver Int. 2020;40:2082–2089. doi:10.1111/liv.14548
9. Roldan-Valadez E, Favila R, Martínez-López M, Uribe M, Méndez-Sánchez N. Imaging techniques for assessing hepatic fat content in nonalcoholic fatty liver disease. Ann. Hepatol. 2008;7:212–220. doi:10.1016/S1665-2681(19)31850-2
10. Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Am J Gastroenterol. 2012;107:811. doi:10.1038/ajg.2012.128
11. Kalambokis G, Manousou P, Vibhakorn S, et al. Transjugular liver biopsy – indications, adequacy, quality of specimens, and complications – a systematic review. J Hepatol. 2007;47:284–294. doi:10.1016/j.jhep.2007.05.001
12. Petta S, Di Marco V, Cammà C, Butera G, Cabibi D, Craxì A. Reliability of liver stiffness measurement in non-alcoholic fatty liver disease: the effects of body mass index. Aliment Pharmacol Ther. 2011;33:1350–1360. doi:10.1111/j.1365-2036.2011.04668.x
13. Castéra L, Foucher J, Bernard P-H, et al. Pitfalls of liver stiffness measurement: a 5-year prospective study of 13,369 examinations. Hepatology. 2010;51:828–835. doi:10.1002/hep.23425
14. Wong VW-S, Vergniol J, Wong GL-H, et al. Liver stiffness measurement using XL probe in patients with nonalcoholic fatty liver disease. Am J Gastroenterol. 2012;107:1862–1871. doi:10.1038/ajg.2012.331
15. Tutunchi H, Naeini F, Ebrahimi-Mameghani M, Najafipour F, Mobasseri M, Ostadrahimi A. Metabolically healthy and unhealthy obesity and the progression of liver fibrosis: a cross-sectional study. Clin Res Hepatol Gastroenterol. 2021;45:101754. doi:10.1016/j.clinre.2021.101754
16. Moltrer M, Pala L, Cosentino C, Mannucci E, Rotella CM, Cresci B. Body mass index (BMI), waist circumference (WC), waist-to-height ratio (WHtR) e waist body mass index (wBMI): which is better? Endocrine. 2022;76:578–583. doi:10.1007/s12020-022-03030-x
17. Park Y, Kim NH, Kwon TY, Kim SG. A novel adiposity index as an integrated predictor of cardiometabolic disease morbidity and mortality. Sci Rep. 2018;8:16753. doi:10.1038/s41598-018-35073-4
18. Kim JY, Choi J, Vella CA, Criqui MH, Allison MA, Kim NH. Associations between weight-adjusted waist index and abdominal fat and muscle mass: multi-ethnic study of atherosclerosis. Diabetes Metab J. 2022;46:747–755. doi:10.4093/dmj.2021.0294
19. Nh K, Park Y, Sg K. Weight-adjusted waist index reflects fat and muscle mass in the opposite direction in older adults. Age Ageing. 2021;50:780–786. doi:10.1093/ageing/afaa208
20. Shen Y, Wu Y, Fu M, Zhu K, Wang J. Association between weight-adjusted-waist index with hepatic steatosis and liver fibrosis: a nationally representative cross-sectional study from NHANES 2017 to 2020. Front Endocrinol. 2023;14:1159055. doi:10.3389/fendo.2023.1159055
21. Hu Q, Han K, Shen J, Sun W, Gao L, Gao Y. Association of weight-adjusted-waist index with non-alcoholic fatty liver disease and liver fibrosis: a cross-sectional study based on NHANES. Eur J Med Res. 2023;28:263. doi:10.1186/s40001-023-01205-4
22. Eslam M, Newsome PN, Sarin SK, et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol. 2020;73:202–209. doi:10.1016/j.jhep.2020.03.039
23. Eddowes PJ, Sasso M, Allison M, et al. Accuracy of fibroscan controlled attenuation parameter and liver stiffness measurement in assessing steatosis and fibrosis in patients with nonalcoholic fatty liver disease. Gastroenterology. 2019;156:1717–1730. doi:10.1053/j.gastro.2019.01.042
24. Roulot D, Czernichow S, Clésiau HL, Costes J-L, Vergnaud A-C, Beaugrand M. Liver stiffness values in apparently healthy subjects: influence of gender and metabolic syndrome. J Hepatol. 2008;48:606–613. doi:10.1016/j.jhep.2007.11.020
25. Hohenester S, Christiansen S, Nagel J, et al. Lifestyle intervention for morbid obesity: effects on liver steatosis, inflammation, and fibrosis. Am J Physiol Gastrointest Liver Physiol. 2018;315:G329–38. doi:10.1152/ajpgi.00044.2018
26. Bosserhoff A, Hellerbrand C. Obesity and fatty liver are ‘grease’ for the machinery of hepatic fibrosis. Dig Dis. 2011;29:377–383. doi:10.1159/000329800
27. Liu Y, Dai M, Bi Y, et al. Active smoking, passive smoking, and risk of Nonalcoholic Fatty Liver Disease (NAFLD): a population-based study in China. J Epidemiol. 2013;23:115–121. doi:10.2188/jea.JE20120067
28. Liang Y, Chen H, Liu Y, et al. Association of MAFLD with diabetes, chronic kidney disease, and cardiovascular disease: a 4.6-year cohort study in China. J Clin Endocrinol Metab. 2021;107:88–97. doi:10.1210/clinem/dgab641
29. Vilar-Gomez E, Calzadilla-Bertot L, Wai-Sun Wong V, et al. Fibrosis severity as a determinant of cause-specific mortality in patients with advanced nonalcoholic fatty liver disease: a multi-national cohort study. Gastroenterology. 2018;155:443–457.e17. doi:10.1053/j.gastro.2018.04.034
30. Gutiérrez-Cuevas J, Santos A, Armendariz-Borunda J. pathophysiological molecular mechanisms of obesity: a link between MAFLD and NASH with cardiovascular diseases. IJMS. 2021;22:11629. doi:10.3390/ijms222111629
31. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000;320:1240–1243. doi:10.1136/bmj.320.7244.1240
32. Fedewa MV, Nickerson BS, Esco MR. Associations of body adiposity index, waist circumference, and body mass index in young adults. Clin Nutr. 2019;38:715–720. doi:10.1016/j.clnu.2018.03.014
33. Zhang S, Du T, Zhang J, et al. The triglyceride and glucose index (TyG) is an effective biomarker to identify nonalcoholic fatty liver disease. Lipids Health Dis. 2017;16:15. doi:10.1186/s12944-017-0409-6
34. Sheng G, Xie Q, Wang R, Hu C, Zhong M, Zou Y. Waist-to-height ratio and non-alcoholic fatty liver disease in adults. BMC Gastroenterol. 2021;21:239. doi:10.1186/s12876-021-01824-3
35. Loomba R, Sanyal AJ. The global NAFLD epidemic. Nat Rev Gastroenterol Hepatol. 2013;10:686–690. doi:10.1038/nrgastro.2013.171
36. Wells J. A Hattori chart analysis of body mass index in infants and children. Int J Obes. 2000;24:325–329. doi:10.1038/sj.ijo.0801132
37. Weber DR, Moore RH, Leonard MB, Zemel BS. Fat and lean BMI reference curves in children and adolescents and their utility in identifying excess adiposity compared with BMI and percentage body fat. The American Journal of Clinical Nutrition. 2013;98:49–56. doi:10.3945/ajcn.112.053611
38. Hainer V, Aldhoon-Hainerová I. Obesity paradox does exist. Diabetes Care. 2013;36:S276–81. doi:10.2337/dcS13-2023
39. Antonopoulos AS, Oikonomou EK, Antoniades C, Tousoulis D. From the BMI paradox to the obesity paradox: the obesity–mortality association in coronary heart disease. Obesity Rev. 2016;17:989–1000. doi:10.1111/obr.12440
40. Xiong Y, Shi W, Huang X, et al. Association between weight-adjusted waist index and arterial stiffness in hypertensive patients: the China H-type hypertension registry study. Front Endocrinol. 2023;14:1134065. doi:10.3389/fendo.2023.1134065
41. Zhao P, Shi W, Shi Y, et al. Positive association between weight-adjusted-waist index and hyperuricemia in patients with hypertension: the China H-type hypertension registry study. Front Endocrinol. 2022;13:1007557. doi:10.3389/fendo.2022.1007557
42. Yu S, Wang B, Guo X, Li G, Yang H, Sun Y. Weight-adjusted-waist index predicts newly diagnosed diabetes in Chinese rural adults. J Clin Med. 2023;12:1620. doi:10.3390/jcm12041620
43. Huang Z, Sun A. Metabolism, inflammation, and cardiovascular diseases from basic research to clinical practice. Cardiol Plus. 2023;8:4–5. doi:10.1097/CP9.0000000000000037
44. Després J. Is visceral obesity the cause of the metabolic syndrome? AnnMed. 2006;38:52–63. doi:10.1080/07853890500383895
45. Julián MT, Ballesta S, Pera G, et al. Abdominal obesity and dsyglycemia are risk factors for liver fibrosis progression in NAFLD subjects: a population-based study. Front Endocrinol. 2023;13:1051958. doi:10.3389/fendo.2022.1051958
46. Fontana L, Eagon JC, Trujillo ME, Scherer PE, Klein S. Visceral fat adipokine secretion is associated with systemic inflammation in obese humans. Diabetes. 2007;56:1010–1013. doi:10.2337/db06-1656
47. Zierath JR, Livingston JN, Thörne A, et al. Regional difference in insulin inhibition of non-esterified fatty acid release from human adipocytes: relation to insulin receptor phosphorylation and intracellular signalling through the insulin receptor substrate-1 pathway. Diabetologia. 1998;41:1343–1354. doi:10.1007/s001250051075
48. Xiong S, Li W, Yin S, et al. Assessing the value of liver fibrosis scores in hypertension: findings from a cross-sectional study. Cardiology Plus. 2024;9:251. doi:10.1097/CP9.0000000000000104
49. Amdanee N, Di W, Liu J, et al. Age-associated changes of resting energy expenditure, body composition and fat distribution in Chinese Han males. Physiological Reports. 2018:
50. Muntner P, Gu D, Wildman RP, et al. Prevalence of physical activity among Chinese adults: results from the international collaborative study of cardiovascular disease in Asia. Am J Public Health. 2005;95:1631–1636. doi:10.2105/AJPH.2004.044743
51. Mallat A, Lotersztajn S. Cigarette smoke exposure: a novel cofactor of NAFLD progression? J Hepatol. 2009;51:430–432. doi:10.1016/j.jhep.2009.05.021
52. Åberg F, Färkkilä M. Drinking and obesity: alcoholic liver disease/nonalcoholic fatty liver disease interactions. Semin Liver Dis. 2020;40:154–162. doi:10.1055/s-0040-1701443
53. Younossi ZM, Golabi P, de AL, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: a systematic review and meta-analysis. J Hepatol. 2019;71:793–801. doi:10.1016/j.jhep.2019.06.021
54. Xiong M, Li J, Yang S, et al. Influence of gender and reproductive factors on liver fibrosis in patients with chronic hepatitis b infection. Clin Transl Gastroenterology. 2019;10:e00085. doi:10.14309/ctg.0000000000000085
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Fibroblast Growth Factor-21 as a Potential Therapeutic Target of Nonalcoholic Fatty Liver Disease
Raptis DD, Mantzoros CS, Polyzos SA
Therapeutics and Clinical Risk Management 2023, 19:77-96
Published Date: 22 January 2023