")
Back to Journals » Psychology Research and Behavior Management » Volume 17
Association of Pain Intensity and Sensitivity with Suicidal Ideation in Adolescents with Depressive Disorder
Authors Shen Q , Zhang Q, Liu Y, Cui Y, Shang J , Yuan X, Geng F, Sun L, Liu Z, Yang R, Zhang K, Liu H
Received 10 April 2024
Accepted for publication 28 August 2024
Published 9 September 2024 Volume 2024:17 Pages 3121—3131
DOI https://doi.org/10.2147/PRBM.S473074
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Qingqing Shen,1– 3,* Qing Zhang,2,3,* Yunxiao Liu,1– 3,* Yingao Cui,1– 3 Jingwen Shang,1– 3 Xiaoping Yuan,2,3 Feng Geng,4 Liang Sun,5 Zhiwei Liu,5 Rongchun Yang,5 Kai Zhang,2,3 Huanzhong Liu2,3,6
1Department of Psychiatry, School of Mental Health and Psychological Sciences, Anhui Medical University, Hefei, Anhui, People’s Republic of China; 2Department of Psychiatry, Chaohu Hospital of Anhui Medical University, Hefei, Anhui, People’s Republic of China; 3Anhui Psychiatric Center, Anhui Medical University, Hefei, Anhui, People’s Republic of China; 4Department of Psychology and Sleep Medicine, the Second Affiliated Hospital of Anhui Medical University, Hefei, Anhui, People’s Republic of China; 5Department of Psychiatry, Fuyang Third People’s Hospital, Fuyang, Anhui, People’s Republic of China; 6Brain Bank Construction and Resource Utilization, Anhui Provincial Key Laboratory, Anhui, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kai Zhang; Huanzhong Liu, Department of Psychiatry, Chaohu Hospital of Anhui Medical University, Hefei, Anhui, People’s Republic of China, Email [email protected]; [email protected]
Purpose: The purpose of this study was to further explore the association of pain intensity and sensitivity with suicidal ideation in adolescents with depressive disorder by comparing the differences in pain intensity and sensitivity between adolescent patients with depressive disorders and healthy controls.
Patients and Methods: A consecutive enrollment method was used to select 158 adolescent patients with depressive disorders from three hospitals in Anhui Province as the MDD group, and 47 healthy adolescents were recruited as the Control group. The subjects’ suicidal ideation was assessed using the Positive and Negative Suicide Ideation scale (PANSI), and the intensity of somatic pain was assessed using the Numerical Rating Scale-11 (NRS-11). Subjects were assessed for forearm and tibial pain sensitivity using a hand-held pressure pain instrument, and experimental pain sensitivity measures included pressure pain threshold (PPT) and pressure pain tolerance (PTO). Differences in pain intensity and sensitivity between the MDD group and the Control group were compared, and the association of pain intensity and sensitivity with suicidal ideation was analyzed.
Results: The incidence of physical pain in adolescent depressive disorder was higher at 88.6%, which was significantly higher than the Control group (P< 0.001), and the pain intensity in the MDD group (3.77± 2.48) was significantly higher than the Control group (0.617± 0.99) (P < 0.001).The Pain tolerance was significantly higher in the MDD group (forearm 105.37 ± 41.46; tibia 121.29 ± 41.60) than in the Control group (forearm 91.92 ± 37.62; tibia 105.47 ± 35.52) (P < 0.05).Linear regression analysis showed that the greater the pain intensity and pain tolerance, the higher the total PANSI score.Binary logistic regression showed that pain intensity was an influencing factor for suicidal ideation.
Conclusion: Adolescents with depressive disorders have higher pain intensity and lower pain sensitivity than healthy adolescents. Increased pain intensity and pain tolerance were positively correlated with suicidal ideation.
Keywords: adolescents, depressive disorder, pain intensity, pain sensitivity, suicidal ideation
Introduction
Depressive disorder is a common illness that severely limits psychosocial functioning and reduces quality of life, The World Health Organization predicts that by 2030 depressive disorders will be the number one cause of disease burden globally.1 The prevalence of depressive disorders among 13 to 18-year-olds is 11%, according to the American epidemiological survey.2 Adolescence is a period of rapid social, emotional, and cognitive development, and a time of high prevalence of depressive disorders,3 Depressive disorders not only seriously affect adolescents’ physical and mental health and social functioning, but are also a high risk factor for suicidal behavior.4 Patients with depressive disorders are prone to pain, and frequent pain may lead to depression risk5 increase and act as a stressor to exacerbate depressive symptoms.6
The experience of pain is subjective and stems from personal experiences early in life and is influenced by genetic, gender, social, cultural, and psychological factors.Two-thirds of people with major depressive disorder experience at least one type of chronic pain.7 Some of these patients present to non-psychiatric clinics with only somatic symptoms, leading to misdiagnosis or underdiagnosis and delayed treatment.Patients with depressive disorders that are associated with pain have 20% more visits to the doctor than those without pain, and are more expensive to treat.8 Most adolescents who self-injure have no or low pain during self-injury,9 which manifests itself as reduced sensitivity to pain.Pain sensitivity can be measured by experimental methods.The contents of experimental pressure pain sensitivity tests include pressure pain threshold(PPT) and pressure pain tolerance(PTO),10 pain threshold refers to the minimum stimulus intensity that the individual can perceive the pain, and pain tolerance refers to the maximum pain stimulus intensity that the individual can withstand.11 Greater values of pain threshold and tolerance indicate lower pain sensitivity, while otherwise, smaller pain threshold and tolerance values indicate higher pain sensitivity.There are conflicting studies on pain sensitivity in patients with depressive disorders, with some studies showing lower pain sensitivity in patients,12–15 while other studies have found patients to have higher pain sensitivity,16–20 Experimental pain was assessed in the following patterns: stress pain, electrical pain stimulation, ischemic pain, hot and cold pain, and chemical pain,14 these different findings may be related to different methods of testing for pain sensitivity.
Suicide is the second leading cause of death among 15- to 19-year-olds,21 The prevalence of suicidal ideation in adolescents is 10.72%-12.1%,4,22 Suicidal ideation refers to the intention to hurt yourself, but not to form a suicide plan, there is no action to prepare and actual harm their own behavior. Suicidal ideation is often the early psychological activity of suicidal behavior, and the risk of attempted suicide is highest 1 year after suicidal ideation,23 so identifying risk factors for suicidal ideation can provide targeted information for suicide prevention efforts. The interpersonal psychology theory of suicide proposes that suicidal individuals acquire suicidality by decreasing their fear of death and increasing pain tolerance.24 Studies have shown that individuals with suicidal and self-injurious behaviors exhibit higher pain threshold and tolerance.11,25,26 Several studies have confirmed a significant association between pain and suicidal behavior,27–29 In a survey conducted by the Canadian National Bureau of Investigation, suicidal ideation was twice as high in chronic pain patients as in the general population.30 However, the relationship between pain intensity and suicidal ideation in adolescent depressive disorder is not clear.31
Although previous studies have linked suicidal behavior and pain symptoms in patients with depressive disorders, it is not clear whether this association also exists in adolescents with depressive disorders, there are few studies on the relationship between pain sensitivity and suicidal ideation in Chinese patients with depressive disorders, and the brain is highly developed throughout adolescence, therefore, it is necessary to carry out research on the adolescent group.The present study aimed to further explore the association of pain intensity and sensitivity with suicidal ideation in adolescents with depressive disorder by comparing the differences in pain intensity and sensitivity in adolescents with depressive disorders with those in healthy adolescents.To this end, we propose the following hypothesis: adolescents with depressive disorders have higher physical pain intensity and lower pain sensitivity than the general adolescent population; At the same time, the greater the intensity of physical pain and the lower the sensitivity of pain, the greater the suicidal ideation.
Material and Methods
Participants
From August 2021 to September 2023, outpatient and inpatient depression disorders were recruited from Chaohu Hospital of Anhui Medical University, the Second Affiliated Hospital of Anhui Medical University, and Fuyang Third People’s Hospital by consecutive enrollment.Structured clinical interviews were conducted with patients by two professionally trained attending psychiatrists with undergraduate and higher degrees in accordance with the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), after the diagnosis of depressive disorder, the subjects were assessed with the related scale.The inclusion criteria were: (1) meeting the DSM-5 diagnostic criteria for depressive disorder; (2) age 12–18 years; and (3) being able to understand the questionnaire.Exclusion Criteria: (1) In recent one year, patients with severe physical disease, infectious disease and immune system disease, such as epilepsy, tumor, heart disease, brain organic disease and other diseases that can cause physical pain; (2) patients with other mental disorders were diagnosed at any time before enrollment, (3) patients receiving painkillers and non-steroidal anti-inflammatory drug therapy in the first 2 weeks of the study; (4) the patients with skin damage, redness, swelling or infection were unable to cooperate with the evaluation or non-cooperation. A total of 158 patients were ultimately recruited, including 86 from psychiatric outpatients and 72 from inpatients.
After both the recruitment information of the Control group was released through online channels such as public accounts and offline channels, a total of 57 adolescents who had routine health examination in hospitals were recruited in this study. Inclusion criteria: (1) no severe organic diseases in the last 1 year, such as epilepsy, tumor, heart disease, brain organic diseases and other diseases that may cause physical pain; (2) no history of mental disorders or family history of mental disorders, (3) age 12–18 years, (4) no history of neurodegenerative or neurovascular diseases, (5) no physical defects, and can complete pain stress test; (6) be able to understand the questionnaire.
First, the informed consent was obtained from the parents. After obtaining the approval, all the participants and their parents signed the informed consent form and fully understood the purpose of the study.The study was approved by the Ethics Committee of Chaohu Hospital of Anhui Medical University (Ethics No.: KYXM-202112-010). All study procedures were conducted in accordance with the Declaration of Helsinki.
Research Methodology
In this study, a self-administered questionnaire was used to collect general demographic information about the subjects, including gender, age, whether they were only children, height, and weight.
Depression severity in adolescents with depressive disorders was assessed using the 24-item The Hamilton Rating Scale for Depression (HAM-D). This scale consists of a total of 24 items, of which 14 items are rated on a 5-point scale from 0 (absent) to 4 (very severe), and 10 items on a 3-point scale from 0 (absent) to 2 (severe). HAM-D is divided into seven dimensions, they were anxiety/somatization (made up of items 10,11,12,13,15, and 17), day/night change (made up of items 18 only), retardation (made up of items 1,7,8, and 14 only), sleep disorders (made up of items 4.5, and 6), feelings of hopelessness (made up of items 22.23, and 24), cognitive disorder (made up of items 2,3,9,19,20, and 21 only), and weight (made up of items 16 only).Higher total scores indicate more severe depressive symptoms in patients, with a total score of 8 to 19 suggesting mild depression, 20 to 34 defined as moderate depression, and >35 suggesting the presence of severe depression.32
Suicidal ideation was assessed using the Positive and Negative Suicide Ideation Scale (PANSI).The PANSI scale consists of two dimensions, they were positive suicidal ideation (made up of 6 items 1,2,6,9,13,14) and negative suicidal ideation (made up of 8 items 3,4,5,7,8,10,11,12), using a 5-point Likert scale, with scores ranging from 1=“never”, 2= “rarely”, 3=“some of the time”, 4“often”, and 5=“all of the time”, The higher the score, the higher the degree of suicidal ideation.19 The PANSI has been shown to have good psychometric properties in adolescent populations, with high reliability and validity, and can be used to measure the severity of suicidal ideation in adolescent patients.33 In this study, according to the quartiles of the PANSI total score of adolescents with depressive disorder, they were divided into high suicidal ideation group (≥ P25) and low suicidal ideation group (<P25).
After the scale was completed, the pain of the patients was assessed by interview, the investigator asked subjects if they had pain that lasted for at least 6 weeks, and if they did they rated them as having pain.34 And subjects’ pain intensity was assessed using the Numerical Rating Scale-11 (NRS-11), which serves as a validated self-report measure of pain in adults, which is also widely used in adolescents with chronic pain.Subjects rate the pain they feel from 0 to 10 (0 = no pain, 10 = maximum pain intensity).35 The NRS-11 has good psychometric properties in measuring pain, showing high sensitivity and stability.36
After completing general data collection, scale assessment and pain assessment, we tested pain sensitivity using an experimental pressure pain test method using a handheld pressure pain instrument (FPX 50, Wagner Instruments, Greenwich, Conn., USA) to assess pain thresholds and pain tolerance.Four locations were selected for the study as pressure pain test points: bilaterally at the brachioradialis muscle on the lateral forearm and bilaterally at the medial border of the tibia 13 cm below the patella,11,37 The operator applied artificial pressure on the subject to tell the operator when they began to feel pain and could not tolerate the pain.The pain threshold and tolerance of both upper and lower limbs were measured respectively, and the pain threshold and tolerance were measured 3 times in each position with an interval of more than 10 minutes, and the mean pain threshold and mean pain tolerance values of the six measurements at the lateral brachioradialis muscle of the forearms were taken bilaterally and labeled PPT-1 and PTO-1, and the mean pain threshold and mean pain tolerance values of the six measurements at the medial border of the tibia at the infrapatellar level of 13 cm were taken bilaterally and labeled PPT-2 and PTO-2.
Statistical Analysis
Data analyses were carried out using SPSS, version 24.0 (IBM Corp, Armonk, NY, USA), all variables were summarized using standard descriptive statistics, mean ± standard deviation was used to express quantitative variable information, and data for categorical variables were presented in the form of frequency distribution (%). The Mann–Whitney U-test was used to analyze the differences between the different groups in terms of age, BMI, total score of suicidal ideation, total score of HAM-D, pain intensity and pain sensitivity; the chi-square test was used to analyze the differences between the different groups in terms of gender, whether they were only children, and whether they were in pain or not; and the Spearman correlation was used to analyze the correlation of pain intensity and pain sensitivity in the MDD group with the general information and the correlation of the total score of suicidal ideation with general information; and analyzing the correlation of the total score of suicidal ideation with general information; using the total score of suicidal ideation as the dependent variable, and the statistically significant variables in the univariate and correlation analyses as the independent variables (age, gender, BMI, whether or not they were only child, PTO-1, PTO-2, and pain intensity), using multivariate linear regression and binary logistic regression to explore the factors that influence suicidal ideation. P < 0.05 (two-tailed) was considered to be significant.
Results
Sociodemographic and Clinical Characteristics of the MDD and Control Groups
There were statistically significant differences between the two groups in terms of gender (χ2 =6.901, P=0.009), total score on the Suicidal Ideation Scale (Z=−9.782, P<0.001), and total HAM-D score (Z=−9.846, P<0.001). The two groups did not show statistically significant differences in ethnicity (χ2 =0.187, P=0.666), whether they were only children (χ2 =0.005, P=0.946), age (Z=−1.152, P=0.249) and BMI (Z=0.462, P=0.644). The specific results are shown in Table 1.
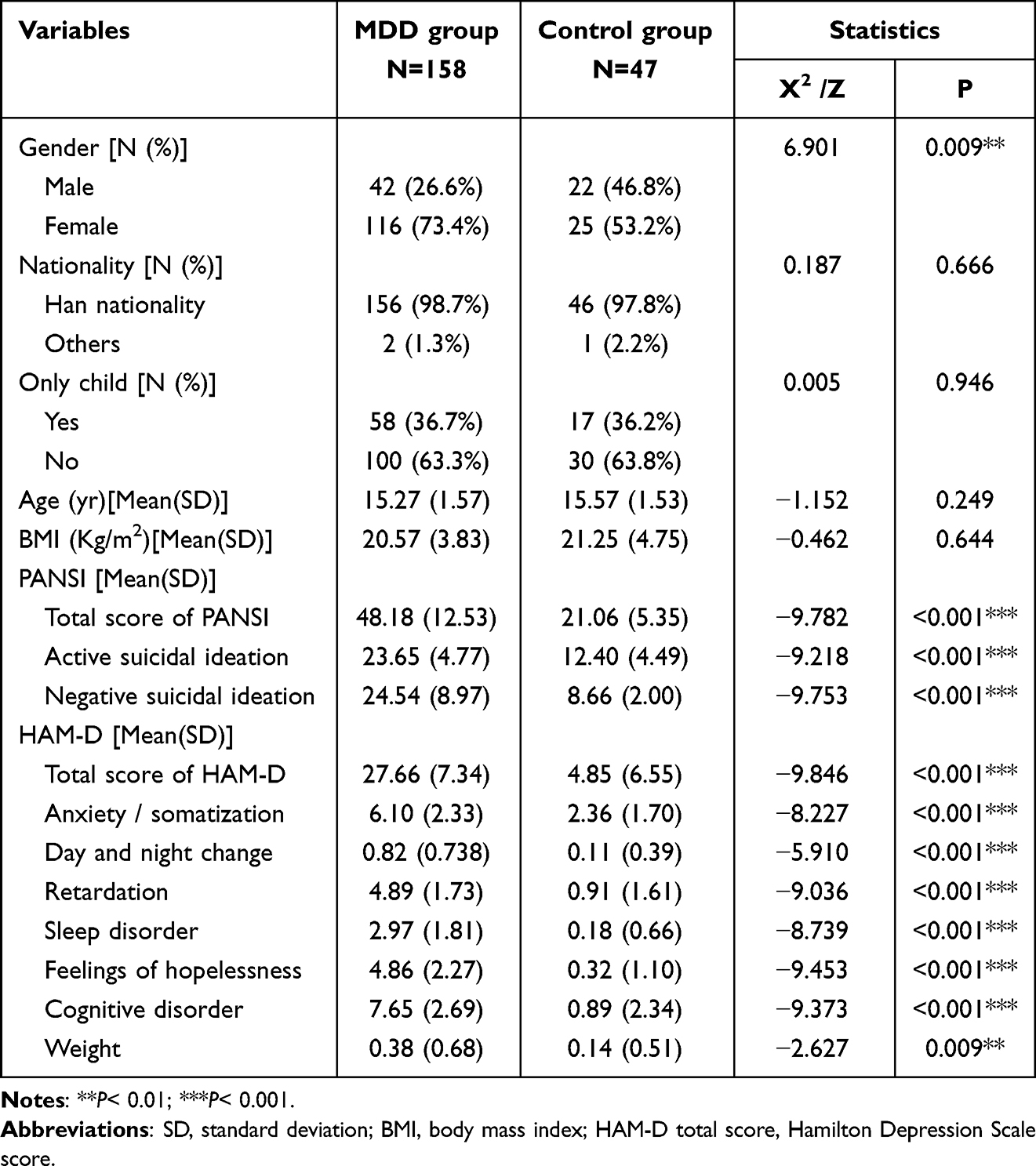 |
Table 1 Socio-Demographic and Clinical Characteristics of the MDD and Control Groups |
Pain Sensitivity and Pain Intensity in the MDD and Control Groups and Medication Use in the MDD Group
The incidence of somatic pain was significantly higher in the MDD group than in the Control group (P < 0.001), and the incidence of somatic pain in adolescent patients with depressive disorders was 88.6%. There was a statistical difference in pain sensitivity and pain intensity between the MDD group and the control population (P < 0.001). There was a statistical difference between the MDD group and the Control group in PTO-1 (Z=−2.012, P=0.044) and PTO-2 (Z=−2.312, P=0.021), ie, the MDD group was significantly higher than the Control group in terms of pain tolerance, and the MDD group was significantly lower than the Control group in terms of pain sensitivity. No statistical difference was seen between the two groups on PPT-1 (Z=−0.350, P=0.726) and PPT-2 (Z=−0.940, P=0.347).
There were 60 medicated patients and 98 unmedicated patients in the MDD group, and the medicated and unmedicated patients did not show statistical differences in pain intensity and pain sensitivity (PPT-1, PTO-1, PPT-1, PTO-2). The specific results are shown in Table 2.
 |
Table 2 Pain Sensitivity and Pain Intensity in the MDD and Control Groups and Medication Use in the MDD Group |
Spearman Correlation Analysis of Pain Sensitivity and Pain Intensity with General Information and Clinical Characteristics in the MDD Group
In this study, the general data and clinical symptom scales were correlated with pain sensitivity and pain intensity, and the results were as follows: the total score of suicidal ideation was negatively correlated with age and gender (r=−0.243, −0.175, all P<0.05), and was positively correlated with the total score of the HAM-D, the PTO-1, the PTO-2, and the pain intensity (r=0.480, 0.179, 0.245, 0.326, all P < 0.05); PPT-1, PTO-1, PPT-2, pain intensity were positively correlated with HAM-D total score (r=0.374,0.220,0.301,0.361, all P<0.05); PTO-2 was negatively correlated with only child (r=−0.213, P < 0.05); pain intensity was negatively correlated with age and gender (r =−0.229,-0.198, all P < 0.05). The specific results are shown in Table 3.
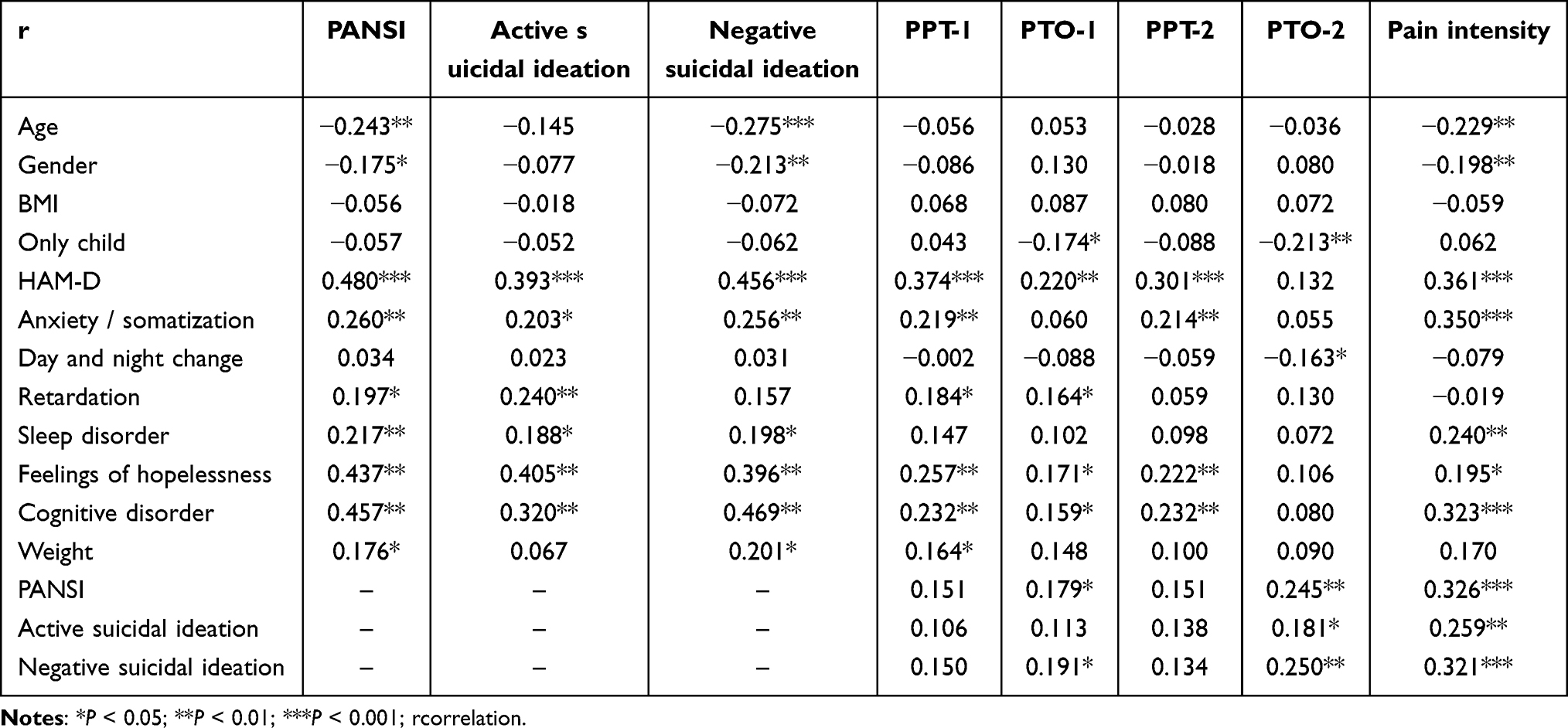 |
Table 3 Spearman Correlation Analysis of Pain Sensitivity and Pain Intensity with General Information and Clinical Characteristics in the MDD Group (r) |
Multiple Linear Regression of Suicidal Ideation in the MDD Group
In order to explore the influencing factors of suicidal ideation in the MDD group, the total score of suicidal ideation was used as the dependent variable, and the variables with statistical differences such as age and gender in Table 3 were used as the independent variables, and the results showed that PTO-2 and pain intensity had a positive and significant effect on the total score of suicidal ideation (P < 0.05), and age had a negative and significant effect on the total score of suicidal ideation (P < 0.05). The specific results are shown in Table 4.
 |
Table 4 Multiple Linear Regression with PANSI Total Score as Dependent Variable in the MDD Group |
Binary Logistic Regression Analysis with PANSI Total Score as Dependent Variable in the MDD Group
The total score of suicidal ideation (high suicidal ideation=1, low suicidal ideation=0) was used as the dependent variable, and the variables with statistical differences such as age and gender in Table 3 were used as the independent variables.The results showed that age and pain intensity were the contributing factors for suicidal ideation (P< 0.05).The specific results are shown in Table 5.
 |
Table 5 Binary Logistic Regression Analysis with PANSI Total Score as Dependent Variable in the MDD Group |
Discussion
The higher percentage of females than males in the MDD group in this study is related to the gender difference in the prevalence of depressive disorders in different growth and development periods. There is no gender difference in the prevalence in childhood, and it is even higher in boys than in girls, but in adolescence, females are gradually higher than males.38 An affective, biological, and cognitive model has been proposed to explain the gender differences that occur in depressive disorders; hormonal and neurodevelopmental changes during puberty vary by gender and females are more likely to be exposed to negative life events during this period, which may contribute to gender differences in depressive disorders during adolescence.39 This is consistent with our results that depressive disorders have gender differences across growth and developmental periods.
Pain and depression co-morbid in up to 80% of cases,40 In our study, there was a significant difference between the MDD group and the Control group in the presence of somatic pain and the intensity of pain, with the prevalence of somatic pain in the MDD group being 88.6%. The mechanisms regarding the co-morbidity of depression and pain are not fully understood and may be related to the activation of neurotransmitters, inflammatory cytokine imbalance and altered activity in brain regions related.41–43 Animal model studies and human brain imaging studies have demonstrated a strong correlation between emotion and pain, involving limbic brain circuits, medial prefrontal cortex, hippocampus, and amygdala.44–46 These brain regions activated by pain stimuli, known as the pain matrix, have been linked not only to pain stimuli, but also to emotions and behaviors, which provides a neural mechanistic basis for a better understanding of the effects of negative emotions on pain.47 Comparing the pain sensitivity of the MDD group with that of the Control group, PTO-1 and PTO-2 were significantly higher in the MDD group, whereas PPT-1 and PPT-2 did not show a difference from the Control group, but there was a trend for higher values in the MDD group than in the Control group. The results of a previous meta-analysis showed48 that patients with depressive disorders had increased pain thresholds and tolerance compared to controls, which is consistent with our results. Experimental pain results have shown that patients with depressive disorders have lower pain sensitivity than the healthy population, but subjective somatic pain intensity is more intense than the healthy population, which has been described in the literature as the “paradox of pain”.49 In this regard, Lautenbacher and Krieg hypothesized that patients with depressive disorders have an impaired sensory system as a whole, including hyperalgesia for experimental pain due to diminished spinal cord and brainstem transmission, and nociceptive hypersensitivity for endogenous pain sensation due to insufficient activation of inhibitory systems.50 Based on this hypothesis, Bär, K. J. et al explored the perception of different pain modalities in patients with depressive disorders and in healthy subjects, and found that patients with depressive disorders have diminished pain perception of external or “surface” stimuli and enhanced pain perception of endogenous or “deep somatic” stimuli. This helps to understand the paradox of pain perception in patients with depressive disorders.14 Some antidepressant medications have an effect on pain perception in patients,51,52 so we compared the pain intensity and sensitivity between medicated and unmedicated patients in the MDD group, and no statistical difference was seen, but there are differences in the type of medication, dosage, and usage of each patient, and the impact of these factors on the experimental results should not be ignored, which we did not record in detail, and this is an area that needs to be further improved in our study.
Pain thresholds have been found to be positively correlated with depression severity, and previously Lautenbacher and Krieg showed that there is a correlation between pain perception and illness severity in depressed patients, and that the severity of depressive symptoms affects the degree to which pain perception is altered, but this has not been confirmed.50 There is also a strong association between somatic pain intensity and depression severity. Previous studies have shown that changes in depression severity at earlier time points can predict subsequent pain severity and vice versa,53 depression is associated with higher pain intensity, and when depressive symptoms are reduced, patients’ pain intensity is also reduced,54 The results of the present study showed a positive correlation between total HAM-D score and pain intensity, which is consistent with previous studies.55 This may be related to the fact that increased levels of inflammatory factors promote the development of pain in adolescent patients with depressive disorders, and there is evidence that inflammatory factors play a key role in depressive disorders and pain, and patients with depression with pain usually show elevated levels of inflammatory factors, such as interleukin-6, tumor necrosis factor-α, etc.56,57 A study of Taiwanese patients with depressive disorders found that elevated serum P-selectin levels were the most significant predictor of co-occurring pain.58
The results showed a negative correlation between age and the total PANSI score in adolescents with depressive disorders, some studies suggests that the risk of suicide may be related to impulse control disorders in the brain, and that the risk of suicide is relatively high in younger patients with weaker brain function development.59,60 Previously, Melhem et al found that younger age was a predictor of suicide attempts,61 which is consistent with our findings. Chronic pain patients sometimes turn to suicide as a way to eliminate pain and burden,62 chronic pain patients are 2–3 times more likely to have suicidal ideation, suicide attempts, and completed suicides than patients without pain,31,63–65 Previous studies have shown that patients with high pain intensity are more likely to report suicidal ideation,66 In our study, the total score of suicidal ideation was significantly higher in the MDD group than in the Control group, and the total score of suicidal ideation increased with increasing pain intensity in the MDD group, which is explained by the fact that pain and suicidal ideation may share similar biological pathways, eg, serotonin transmission is associated with pain, which may ultimately lead to suicidal ideation.67
Our results showed a positive correlation between tibial pain tolerance and the total score of suicidal ideation, while this relationship was not reflected in the forearm. A possible explanation for this is that most patients with depressive disorders choose to use the wrist as the site of self-injury, whereas we chose the lateral brachioradialis muscle of the forearm as the site of pain tolerance measurement, which may not accurately mimic the pain that the patients experience when they self-injure. However, our experiment is still innovative, and among the literature we were able to retrieve, we are the first study to use both the forearm and the tibia as test sites for pain sensitivity in adolescent patients with depressive disorders. Decreased psychological pain tolerance and increased somatic pain tolerance are risk factors for suicide risk, and suicidality increases with increased tolerance to somatic pain,68,69 A study found that psychological pain tolerance was a predictor of suicidal ideation, and somatic pain tolerance mediated this relationship,70 In addition, repeated experience of psychological and physical pain can desensitize the response to prevent physical harm, resulting in suicidal ideation.71 This is consistent with our results.
Limitations of our study: this study was a cross-sectional study and could not clarify the causal relationship between pain intensity and sensitivity and clinical characteristics; the study population was regionally concentrated, with participants recruited from a single province, and the results may not be applicable to all Chinese adolescents with depressive disorders; some of the questionnaires were self-assessment questionnaires, which may be subject to recall bias; These patients are in different periods of depressive disorder, and therefore we only investigated whether patients were taking antidepressants, but did not detail the type, dose, and use of medications used by each patient, factors that might have had an impact on the results of the trial; the present study focused on the clinical characteristics and did not include biological factors were analyzed; information on the site, time, nature and frequency of pain was not collected in this study.
Conclusion
There were significant differences in pain intensity and pain sensitivity between adolescents with depressive disorder and healthy adolescents. As pain intensity and Pain tolerance increased, the total PANSI score increased, suggesting that increased pain intensity and pain sensitivity were associated with suicidal ideation.In future studies, we will include biological factors such as inflammatory factors for analysis, from a basic level to explore its physiological mechanisms; at the same time, we will follow-up the subjects, to monitor the dynamic changes in order to determine the cause-and-effect relationship between pain intensity and sensitivity and clinical characteristics. In clinical practice, early assessment of pain intensity and pain sensitivity can help clinicians understand patients’ suicidal ideation, psychiatrists need to pay attention to physical pain symptoms and pain sensitivity in adolescent depressive disorder patients to further predict the risk of suicide, and to conduct targeted intervention in later treatment.
Data Sharing Statement
The data used for this study are available from the corresponding author ([email protected]) on reasonable request.
Ethics Approval and Informed Consent
The survey strictly followed the principles of the Helsinki Declaration and was approved by the Ethics Committee of Chaohu Hospital of Anhui Medical University (KYXM-202112-010).Before filling out the questionnaire, we informed patients and families about the purpose of this study and ensure that their personal privacy would not be disclosed. The patient and family signed informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Research Fund of Anhui Institute of translational medicine (2022zhyx-B01) and International Academic Forum for Graduate Future Scientists of Psychiatric Medicine (2022gjxslt010).
Disclosure
The authors have no potential conflicts of interest to disclose in this work.
References
1. Malhi GS, Mann JJ. Depression. Lancet. 2018;392(10161):2299–2312.
2. Avenevoli S, Swendsen J, He J-P, Burstein M, Merikangas KR. Major depression in the national comorbidity survey-adolescent supplement: prevalence, correlates, and treatment. J Am Acad Child Adolesc Psyc. 2015;54(1).
3. Shorey S, Ng ED, Wong CHJ. Global prevalence of depression and elevated depressive symptoms among adolescents: a systematic review and meta-analysis. Br J Clin Psychol. 2022;61(2):287–305.
4. Nock MK, Green JG, Hwang I, et al. Prevalence, correlates, and treatment of lifetime suicidal behavior among adolescents: results from the national comorbidity survey replication adolescent supplement. JAMA Psych. 2013;70(3):300–310.
5. Borgman S, Ericsson I, Clausson EK, Garmy P. The relationship between reported pain and depressive symptoms among adolescents. J Sch Nurs. 2020;36(2):87–93.
6. Lee P, Zhang M, Hong JP, et al. Frequency of painful physical symptoms with major depressive disorder in Asia: relationship with disease severity and quality of life. J Clin Psychiatry. 2009;70(1):83–91.
7. Ohayon MM, Schatzberg AF. Chronic pain and major depressive disorder in the general population. J Psychiatr Res. 2010;44(7):454–461.
8. Bao Y, Sturm R, Croghan TW. A national study of the effect of chronic pain on the use of health care by depressed persons. Psychiatr Serv. 2003;54(5):693–697.
9. Nock MK, Prinstein MJ. Contextual features and behavioral functions of self-mutilation among adolescents. J Abnorm Psychol. 2005;114(1):140–146.
10. Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B, Riley JL. Sex, gender, and pain: a review of recent clinical and experimental findings. J Pain. 2009;10(5):447–485.
11. Kim DJ, Blossom SJ, Delgado PL, Carbajal JM, Cáceda R. Examination of pain threshold and neuropeptides in patients with acute suicide risk. Prog Neuropsycho Biol Psych. 2019;95:109705.
12. Adler G, Gattaz WF. Pain perception threshold in major depression. Biol Psych. 1993;34(10):687–689.
13. Lautenbacher S, Spernal J, Schreiber W, Krieg JC. Relationship between clinical pain complaints and pain sensitivity in patients with depression and panic disorder. Psychosom Med. 1999;61(6):822–827.
14. Bär K-J, Brehm S, Boettger MK, Boettger S, Wagner G, Sauer H. Pain perception in major depression depends on pain modality. Pain. 2005;117(1–2).
15. Schwier C, Kliem A, Boettger MK, Bär K-J. Increased cold-pain thresholds in major depression. J Pain. 2010;11(3):287–290.
16. Zambito Marsala S, Pistacchi M, Tocco P, et al. Pain perception in major depressive disorder: a neurophysiological case-control study. J Neurol Sci. 2015;357(1–2):19–21.
17. Hermesdorf M, Berger K, Baune BT, Wellmann J, Ruscheweyh R, Wersching H. Pain Sensitivity in Patients With Major Depression: differential Effect of Pain Sensitivity Measures, Somatic Cofactors, and Disease Characteristics. J Pain. 2016;17(5):606–616.
18. Nitzan U, Hecht M, Braw Y, et al. Initial Evaluation of Pain Intensity Among Depressed Patients as a Possible Mediator Between Depression and Pain Complaints. Front Psychiatry. 2019;10:48.
19. Osman A, Gutierrez PM, Kopper BA, Barrios FX, Chiros CE. The positive and negative suicide ideation inventory: development and validation. Psychol Rep. 1998;82(3 Pt 1):783–793.
20. Suarez-Roca H, Piñerua-Shuhaibar L, Morales ME, Maixner W. Increased perception of post-ischemic paresthesias in depressed subjects. J Psychosom Res. 2003;55(3):253–257.
21. Shain B. Suicide and Suicide Attempts in Adolescents. Pediatrics. 2016;138(1).
22. Li -Z-Z, Li Y-M, Lei X-Y, et al. Prevalence of suicidal ideation in Chinese college students: a meta-analysis. PLoS One. 2014;9(10):e104368.
23. Ten Have M, van Dorsselaer S, de Graaf R. Prevalence and risk factors for first onset of suicidal behaviors in the Netherlands Mental Health Survey and Incidence Study-2. J Affect Disord. 2013;147(1–3):205–211.
24. Chu C, Buchman-Schmitt JM, Stanley IH, et al. The interpersonal theory of suicide: a systematic review and meta-analysis of a decade of cross-national research. Psychol Bull. 2017;143(12):1313–1345.
25. Cáceda R, Kordsmeier NC, Golden E, Gibbs HM, Delgado PL. Differential processing of physical and psychological pain during acute suicidality. Psychother Psycho. 2017;86(2):116–118.
26. Koenig J, Thayer JF, Kaess M. A meta-analysis on pain sensitivity in self-injury. Psychol Med. 2016;46(8):1597–1612.
27. Pakniyat-Jahromi S, Korenis P, Sher L. Pain and suicide: what should we tell our trainees? Acta Neuropsychiatr. 2022;34(3):127–131.
28. Boska RL, Bishop TM, Ashrafioun L. Pain conditions and suicide attempts in military veterans: A case-control design. Pain Med. 2021;22(12):2846–2850.
29. Ryan PC, Lowry NJ, Boudreaux E, et al. Chronic pain, hopelessness, and suicide risk among adult medical inpatients. J AcadConsul Liaison Psych. 2024;65(2):126–135.
30. Ratcliffe GE, Enns MW, Belik S-L, Sareen J. Chronic pain conditions and suicidal ideation and suicide attempts: an epidemiologic perspective. Clin J Pain. 2008;24(3):204–210.
31. Tang NKY, Crane C. Suicidality in chronic pain: a review of the prevalence, risk factors and psychological links. Psychol Med. 2006;36(5):575–586.
32. Pan S, Liu Z-W, Shi S, et al. Hamilton rating scale for depression-24 (HAM-D24) as a novel predictor for diabetic microvascular complications in type 2 diabetes mellitus patients. Psychiatry Res. 2017;258:177–183.
33. Sinniah A, Oei TP, Chinna K, Shah SA, Maniam T, Subramaniam P. Psychometric Properties and Validation of the Positive and Negative Suicide Ideation (PANSI) Inventory in an Outpatient Clinical Population in Malaysia. Front Psychol. 2015;6:1934.
34. Agüera-Ortiz L, Failde I, Mico JA, Cervilla J, López-Ibor JJ. Pain as a symptom of depression: prevalence and clinical correlates in patients attending psychiatric clinics. J Affect Disord. 2011;130(1–2):106–112.
35. Ruskin D, Lalloo C, Amaria K, et al. Assessing pain intensity in children with chronic pain: convergent and discriminant validity of the 0 to 10 numerical rating scale in clinical practice. Pain Res Manag. 2014;19(3):141–148.
36. Euasobhon P, Atisook R, Bumrungchatudom K, Zinboonyahgoon N, Saisavoey N, Jensen MP. Reliability and responsivity of pain intensity scales in individuals with chronic pain. Pain. 2022;163(12):e1184–e1191.
37. Duan G, Xiang G, Zhang X, Yuan R, Zhan H, Qi D. A single-nucleotide polymorphism in SCN9A may decrease postoperative pain sensitivity in the general population. Anesthesiology. 2013;118(2):436–442.
38. Twenge JM, Nolen-Hoeksema S. Age, gender, race, socioeconomic status, and birth cohort differences on the children’s depression inventory: a meta-analysis. J Abnorm Psychol. 2002;111(4):578–588.
39. Hyde JS, Mezulis AH, Abramson LY. The ABCs of depression: integrating affective, biological, and cognitive models to explain the emergence of the gender difference in depression. Psychol Rev. 2008;115(2):291–313.
40. Poole H, White S, Blake C, Murphy P, Bramwell R. Depression in chronic pain patients: prevalence and measurement. Pain Pract. 2009;9(3):173–180.
41. Finan PH, Smith MT. The comorbidity of insomnia, chronic pain, and depression: dopamine as a putative mechanism. Sleep Med Rev. 2013;17(3):173–183.
42. Sheng J, Liu S, Wang Y, Cui R, Zhang X. The Link between Depression and Chronic Pain: neural Mechanisms in the Brain. Neural Plast. 2017;2017:9724371.
43. Meerwijk EL, Ford JM, Weiss SJ. Brain regions associated with psychological pain: implications for a neural network and its relationship to physical pain. Brain Imaging Behav. 2013;7(1).
44. Whittle S, Lichter R, Dennison M, et al. Structural brain development and depression onset during adolescence: a prospective longitudinal study. Am J Psychiatry. 2014;171(5):564–571.
45. Khan SA, Keaser ML, Meiller TF, Seminowicz DA. Altered structure and function in the hippocampus and medial prefrontal cortex in patients with burning mouth syndrome. Pain. 2014;155(8):1472–1480.
46. Cullen KR, Westlund MK, Klimes-Dougan B, et al. Abnormal amygdala resting-state functional connectivity in adolescent depression. JAMA Psychiatry. 2014;71(10):1138–1147.
47. Baliki MN, Apkarian AV. Nociception, pain, negative moods, and behavior selection. Neuron. 2015;87(3):474–491.
48. Dickens C, McGowan L, Dale S. Impact of depression on experimental pain perception: a systematic review of the literature with meta-analysis. Psychosom Med. 2003;65(3):369–375.
49. Rodriguez-Raecke R, Ihle K, Ritter C, Muhtz C, Otte C, May A. Neuronal differences between chronic low back pain and depression regarding long-term habituation to pain. Eur J Pain. 2014;18(5):701–711.
50. Lautenbacher S, Krieg JC. Pain perception in psychiatric disorders: a review of the literature. J Psychiatr Res. 1994;28(2):109–122.
51. Schüler P, Seibel K, Chevts V, Schaffler K. Analgesic effect of the selective noradrenaline reuptake inhibitor reboxetine. Nervenarzt. 2002;73(2):149–154.
52. Enggaard TP, Klitgaard NA, Gram LF, Arendt-Nielsen L, Sindrup SH. Specific effect of venlafaxine on single and repetitive experimental painful stimuli in humans. Clin Pharmacol Ther. 2001;69(4):245–251.
53. Kroenke K, Wu J, Bair MJ, Krebs EE, Damush TM, Tu W. Reciprocal relationship between pain and depression: a 12-month longitudinal analysis in primary care. J Pain. 2011;12(9):964–973.
54. Gerrits MMJG, van Marwijk HWJ, van Oppen P, van der Horst H, Penninx BWJH. Longitudinal association between pain, and depression and anxiety over four years. J Psychosom Res. 2015;78(1):64–70.
55. Williams LS, Jones WJ, Shen J, Robinson RL, Kroenke K. Outcomes of newly referred neurology outpatients with depression and pain. Neurology. 2004;63(4):674–677.
56. Omoigui S. The biochemical origin of pain: the origin of all pain is inflammation and the inflammatory response. Part 2 of 3 - inflammatory profile of pain syndromes. Med Hypotheses. 2007;69(6):1169–1178.
57. Raison CL, Capuron L, Miller AH. Cytokines sing the blues: inflammation and the pathogenesis of depression. Trends Immunol. 2006;27(1):24–31.
58. Bai Y-M, Chiou W-F, T-P S, C-T L, Chen M-H. Pro-inflammatory cytokine associated with somatic and pain symptoms in depression. J Affect Disord. 2014;155:28–34.
59. Stanley B, Michel CA, Galfalvy HC, et al. Suicidal subtypes, stress responsivity and impulsive aggression. Psychiatry Res. 2019;280:112486.
60. Minzenberg MJ, Lesh TA, Niendam TA, et al. Control-related frontal-striatal function is associated with past suicidal ideation and behavior in patients with recent-onset psychotic major mood disorders. J Affect Disord. 2015;188:202–209.
61. Melhem NM, Porta G, Oquendo MA, et al. Severity and variability of depression symptoms predicting suicide attempt in high-risk individuals. JAMA Psychiatry. 2019;76(6):603–613.
62. Stenager E, Christiansen E, Handberg G, Jensen B. Suicide attempts in chronic pain patients. A register-based study. Scand J Pain. 2014;5(1):4–7.
63. Fishbain DA, Goldberg M, Rosomoff RS, Rosomoff H. Completed suicide in chronic pain. Clin J Pain. 1991;7(1):29–36.
64. Breslau N, Schultz L, Lipton R, Peterson E, Welch KMA. Migraine headaches and suicide attempt. Headache. 2012;52(5):723–731.
65. Hooley JM, Franklin JC, Nock MK. Chronic pain and suicide: understanding the association. Curr Pain Headache Rep. 2014;18(8):435.
66. de Heer EW, Ten Have M, van Marwijk HWJ, et al. Pain as a risk factor for suicidal ideation. A population-based longitudinal cohort study. Gen Hosp Psych. 2020;63:54–61.
67. van Heeringen K, Mann JJ. The neurobiology of suicide. Lancet Psych. 2014;1(1):63–72.
68. Van Orden KA, Witte TK, Gordon KH, Bender TW, TE J Jr. Suicidal desire and the capability for suicide: tests of the interpersonal-psychological theory of suicidal behavior among adults. J Consult Clin Psych. 2008;76(1):72–83.
69. Franklin JC, Hessel ET, Prinstein MJ. Clarifying the role of pain tolerance in suicidal capability. Psychiatry Res. 2011;189(3):362–367.
70. Yeşiloğlu C, Tamam L, Demirkol ME, Namlı Z, Karaytuğ MO. Associations between the suicidal ideation and the tolerance for psychological pain and tolerance for physical pain in patients diagnosed with major depressive disorder. Neuropsychiatr Dis Treat. 2023;19:2283–2294.
71. Smith PN, Cukrowicz KC. Capable of suicide: a functional model of the acquired capability component of the Interpersonal-Psychological Theory of Suicide. Suicide Life Threat Behav. 2010;40(3):266–275.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.