")
Back to Journals » Journal of Inflammation Research » Volume 17
Association of Stress Hyperglycemia Ratio and in-Hospital Mortality in Patients with Sepsis: A Two Center Retrospective Cohort Study
Authors Ma C , Jiang W, Li J, Sun W , Zhang J, Xu P, Guo Y , Ning N, Li J, Zhao B, Mao E, Gao C
Received 5 May 2024
Accepted for publication 18 October 2024
Published 30 October 2024 Volume 2024:17 Pages 7939—7950
DOI https://doi.org/10.2147/JIR.S476898
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Chaoping Ma,1,* Weisong Jiang,2,* Juan Li,1,* Wenwu Sun,2,* Jiyuan Zhang,1 Peixian Xu,1 Yiran Guo,1 Ning Ning,2 Jiaoyan Li,2 Bing Zhao,2 Enqiang Mao,2 Chengjin Gao1
1Departments of Emergency, Xinhua Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, 200092, People’s Republic of China; 2Departments of Emergency, Ruijin Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, 200025, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chengjin Gao; Enqiang Mao, Email [email protected]; [email protected]
Introduction: In critically ill patients, the stress hyperglycemia ratio (SHR) was significantly associated with mortality. However, the relationship between SHR and mortality in septic patients is still unclear.In this study, patients with sepsis from two Chinese academic centers were identified and divided into quartiles based on SHR levels.
Methods: Multivariable regression analysis will be used to determine associations between SHR and clinical outcomes in sepsis patients.The Kaplan-Meier curve was used to predict mortality in various groups of septic patients.
Results: A total of 1835 septic patients were included in the study.The in-hospital, 30-day, and 60-day mortality rates for all septic patients were 22.8%, 18.7%, and 21.7%, respectively. Increased SHR was significantly associated with hospital mortality in multivariate regression analysis.These results were further confirmed in the adjusted analysis, where the hospital mortality and the 60-day mortality of the highest SHR quartile were significantly increased compared to the lowest SHR quartile. However, the highest SHR quartile was not associated with 30-day mortality.In addition, the risk of in-hospital mortality, 30-day mortality and 60-day mortality showed a consistent upward trend with increasing SHR quartile. The survival curve showed that the worst prognosis was in the fourth SHR quartile.
Discussion: In conclusion, SHR was significantly associated with hospital mortality in patients with sepsis. This finding indicates that the SHR may be useful in identifying septic patients at higher risk of hospital mortality.
Keywords: sepsis, stress hyperglycemia ratio, mortality, Hyperglycemia
A Letter to the Editor has been published for this article.
Introduction
Patients with sepsis, a manifestation of infection in which systemic signs of inflammation are present and vital organ function may be compromised, have a higher risk of death than those with uncomplicated infections.1 Sepsis has an impact on millions of people around the world every year. Despite a 52.8% decrease since 1990, sepsis still accounted for 19.7% of deaths worldwide in 2017 and continues to be a significant contributor to the global health burden.2 Therefore, it is essential to identify readily available determinants of adverse events to enable optimal management and improve quality of life in this patient population.3,4 These patients are particularly susceptible to hyperglycaemia and insulin resistance due to an array of pathophysiological changes associated with sepsis.5
Stress hyperglycaemia is a common occurrence in patients with trauma and critical illness. It results from insulin resistance (IR) due to acute stress, inflammatory response and severe disruption of glucose metabolism.Patients with sepsis often have blood glucose levels that are higher than average. Sepsis triggers a severe stress response that affects both central and peripheral systems, leading to hormonal and metabolic changes.During the period of sympathetic overactivity, catecholamines inhibit the release of insulin and promote the breakdown of glycogen, which reduces the uptake of glucose by tissues and leads to the activation of the pro-inflammatory pathway associated with hyperglycaemia.6 In this context, the stress hyperglycaemia ratio (SHR) has been developed as a new marker to reflect the true acute hyperglycaemic state, which is estimated based on the acute admission glucose level and the chronic glycaemic value [calculated by glycosylated haemoglobin (HbA1c)].7 Although previous studies have reported that SHR is an independent risk factor for mortality in certain populations, such as myocardial infarction, acute ischaemic stroke and perioperative patients,8–10 the relationship between SHR and prognosis in septic patients remains incompletely elucidated.
As such, this study is designed to explore the predictive value of the SHR and to further determine whether it may have any clinical relevance in this population.
Methods
Participants
In this retrospective study, the clinically relevant data of patients from the Ruijin Hospital of the Shanghai Jiaotong University School of Medicine and the Xinhua Hospital of the Shanghai Jiaotong University School of Medicine were examined. Adult patients who met the diagnostic criteria for Sepsis 3.0 from September 2015 to May 2022 (Ruijin Hospital, Shanghai Jiaotong University School of Medicine) and from October 2012 to October 2022 (Xinhua Hospital, Shanghai Jiaotong University School of Medicine) were included.The protocol was approved by the institutional ethics board of each hospital (RJ-2022-312, XHEC-D-2023-074). The informed consent was waived because of the non-interventional, retrospective design of the study. Data analysis was performed in accordance with the 1964 helsinki Declaration and its later amendments.All personal information has been de-identified to protect patient confidentiality, with random codes replacing patient identifiers, thus eliminating the need for patient-informed consent and ethical approval. All patients were treated according to our local protocol, which included early administration of antibiotics and initiation of fluid resuscitation with crystalloids. The inclusion and exclusion criteria were as follows: (1) patients < 18 years of age, (2) less than 24 hours from admission to discharge or death, (3) history of malignancy or autoimmune disease, (4) patients for whom HbA1c or fasting blood glucose data were not available within 24 hours of admission.
Data Collection
For each patient, clinical variables are extracted from paper or electronic medical records. Baseline demographic information includes age, gender, comorbidities (hypertension, diabetes, cardiovascular disease, cerebrovascular disease and chronic kidney disease).Laboratory parameters include creatinine, total bilirubin, procalcitonin, C-reactive protein, haematocrit, white blood cells, platelets, blood glucose, and haemoglobin A1c (HbA1c). SHR was calculated as [(admission glucose (mmol/L))/(1.59×HbA1c (%)-2.59)].The participants were divided into four groups (Q1 (≤0.88), Q2 (0.88–1.06), Q3 (1.06–1.32), Q4 (>1.32)) according to the quartiles of SHR, and the Q1 group was used as the reference group. Other relevant data include the Acute Physiology and Chronic Health Evaluation II (APACHE II) score and the Sequential Organ Failure Assessment (SOFA) score.The use of mechanical ventilation (MV), ventilation duration and vasopressors were also reported. Outcomes include in-hospital mortality and length of stay (LOS).All laboratory indicators and severity of illness scores were extracted from data generated within the first 24 hours of the patient’s admission to hospital.
Outcomes
The primary endpoint of the present study was in-hospital mortality, and the secondary endpoint was mortality within 30 days and within 60 days of admission to the hospital.
Date Statistical
Continuous variables were expressed as mean ± standard deviation (SD) or median and interquartile range (IQR). Categorical variables were presented as numbers and percentages.The Kolmogorov–Smirnov test was employed to evaluate the normality of continuous parameters. The investigation of continuous variables was executed using a t-test or ANOVA if they showed a normal distribution, and using the Mann–Whitney U-test or Kruskal–Wallis test if they were non-normally distributed.A multivariable logistic regression analysis was conducted to assess the relationship between hospital mortality and SHR. The analysis calculated the odds ratio (OR) and 95% confidence interval (CI) for SHR and endpoints, while also adjusting for various models. The variables included in the multivariate model were as follows: Model 1 (Unadjusted), Model 2 (Adjusted for age and gender), and Model 3 (Adjusted for age, gender, creatinine, C-reactive protein, white blood cells, haematocrit, hypertension, cardiovascular issues, chronic kidney disease, and mechanical ventilation). Additionally, Kaplan-Meier survival analysis was performed to determine the incidence rate of endpoints among groups categorized by different levels of SHR, with differences assessed using Log rank tests.The SHR was entered into the models as continuous variables or ordinal variables (the first quartile of the SHR was taken as a reference group). The P values for trends were calculated using the quartile level.In addition, Cox regression analysis was used as a sensitivity analysis to explore the association between SHR and endpoints. This was performed based on age, gender, diabetes, hypertension, cardiovascular disease, mechanical ventilation, vasopressors, SOFA score, and APACHE II score.All data were statistically analysed using SPSS 26.0 (IBM Corp, New York, NY, USA). A P-value of less than 0.05 was regarded as statistically significant.
Results
The inclusion and exclusion criteria resulted in the enrollment of 1835 septic patients in this study. The selection flowchart is shown in Figure 1.
 |
Figure 1 Screening flowchart. |
Baseline Characteristics of Study Participants
Table 1 summarizes the baseline characteristics of patients grouped by in-hospital mortality status. The study analyzed 1835 septic patients, with an in-hospital mortality rate of 22.8% (418 patients). The median length of stay was shorter for deceased patients compared to survivors (13.0 vs 15.0 days; p < 0.001). Notably, the non-survivors had more severe illness, indicated by higher median scores of SOFA (8.0 vs 4.0; p < 0.001) and APACHE II (16.0 vs 11.0; p < 0.001). A higher proportion of the mortality group required mechanical ventilation (67% vs 18.4%; p < 0.001), had a longer median duration of ventilation (2 days vs 0; p < 0.001), and received vasopressors (73.7% vs 13.0%; p < 0.001). Significant associations were found between in-hospital mortality and several factors, including age, white blood cell, hematocrit, hemoglobin A1c, and creatinine. However, blood glucose levels did not significantly correlate with in-hospital mortality (7.4 mmol/L vs 6.9 mmol/L; p = 0.074). Furthermore, higher SHR were more common in the mortality group, particularly in the third (45.2% vs 39.5%; P = 0.037) and fourth quartiles (12.0% vs 6.7%; p < 0.001), whereas lower SHR (first quartile: 20.6% vs 26.0%, P = 0.023; second quartile: 22.2% vs 27.7%, P = 0.026) were associated with survival, suggesting that a lower SHR may serve as a protective factor in sepsis patients.These findings underscore the complexity of sepsis management. The correlation between SHR and survival suggests that not only traditional biomarkers but also novel indicators like SHR could be pivotal in predicting outcomes.
 |
Table 1 Baseline Characteristics of Patients Grouped by in-Hospital Mortality Status |
Association Between Characteristics and Outcomes of Participants Categorized by SHR
In Table 2, it was observed that the Q3 group exhibited the highest prevalence of patients with a comparatively elevated SHR (40.8%).In comparison to the Q1 group, patients in the other groups were more likely to be male and exhibited higher inflammatory markers, including CRP and white blood cells.This gender disparity and heightened inflammatory response may stem from various factors such as genetic predisposition, hormonal differences, and varying immune responses to environmental stimuli. Conversely, patients in the Q1 group were more likely to have diabetes. Notably, the Q3 and Q4 groups, which had a relatively higher SHR, also presented elevated APACHE II and SOFA scores, indicating significant physiological disturbances and multi-organ dysfunction. Furthermore, the Q3 and Q4 groups with a relatively higher SHR exhibited higher in-hospital mortality, 30-day mortality, 60-day mortality, and a greater likelihood of requiring mechanical ventilation and vasoactive drugs. The use of mechanical ventilation typically signifies respiratory failure, while vasoactive medications are administered to maintain adequate circulatory perfusion pressure and tissue oxygenation, both direct indicators of severe illness.In conclusion, the study’s results reveal significant differences in clinical characteristics, disease severity, and prognosis among different SHR groups. For clinicians, this information facilitates earlier identification of high-risk patient cohorts, enabling more proactive and effective treatment strategies to improve outcomes.
 |
Table 2 Characteristics and Outcomes of Participants Categorized by SHR |
Association Between SHR and Mortality
The results of the multivariate regression analysis indicated that SHR was independently associated with in-hospital mortality (OR 1.874 [95% CI 1.398–2.512], P<0.001), 30-day mortality (OR 1.736, [95% CI 1.270–2.372], P=0.001), and 60-day mortality (OR 1.886, [95% CI 1.402–2.538], P<0.001). In both model 1 and model 2, the Q3 and Q4 groups with a relatively higher SHR exhibited higher in-hospital, 30-day, and 60-day mortality rates compared to the Q1 group. These results were further confirmed in the fully adjusted Model 3, with the OR for in-hospital mortality in the highest SHR quartile being 1.745 (95% CI: 1.06–2.871), and for 60-day mortality being 1.756 (95% CI: 1.068–2.886), both compared with the lowest quartile. However, there was no association between the highest SHR quartile and 30-day mortality (OR=1.427, 95% CI 0.856–2.378, p=0.173)(Table 3). Furthermore, the risk of in-hospital mortality, 30-day mortality, and 60-day mortality demonstrated a consistent upward trend with increasing SHR quartile, with all trend p-values below 0.05 (Table 3, Figure 2).To ensure the reliability of the results, the Kaplan–Meier analysis plot demonstrated a significant difference in mortality rates between the various SHR groups. Patients with a higher SHR exhibited a higher risk of in-hospital, 30-day, and 60-day mortality (log-rank P-values of 0.0369, 0.0445, and 0.0167, respectively) (Figure 3). In summary, this study offers a valuable perspective on the impact of short-term prognosis for patients through an in-depth analysis of the relationship between SHR and mortality at different time points. It suggests that clinical operations should dynamically monitor SHR indicators and provide appropriate treatment to maintain them within a reasonable range.
 |
Table 3 Multivariable Logistic Analysis of Associations Between SHR Quartiles and Mortality |
 |
Figure 2 Odds ratios for hospital mortality according to SHR quartiles after adjusting for Age, Gender, Cr, CRP, WBC, Hct, hypertension, cardiovascular disease, CKD, MV. Error bars indicate 95% CIs.The first quartile is the reference. |
 |
Figure 3 Shows the Kaplan-Meier survival analysis for hospital mortality according to SHR quartiles. The graph illustrates the relationship between SHR levels and the likelihood of hospital mortality, with each quartile representing a different level of risk. This analysis provides valuable insights into the impact of SHR on patient outcomes and can help inform clinical decision-making. Kaplan-Meier survival analysis showing in-hospital mortality (A) and 60-day mortality (B) and 30-day mortality (C). |
Subgroup Analysis
Furthermore, to confirm the relationship between SHR and in-hospital mortality, 30-day mortality, and 60-day mortality, stratified analyses were conducted based on age, gender, diabetes, hypertension, cardiovascular disease, mechanical ventilation, vasopressors, SOFA score, and APACHE II score. Figure 4 illustrates a significant relationship between SHR and mortality for patients aged over 65 years, with hypertension, without diabetes, without cardiovascular disease, without mechanical ventilation, and with an APACHEII score of 14 or below. Notably, the SHR appears to be more predictive in patients without ventilation and with hypertension (P for interaction <0.05).
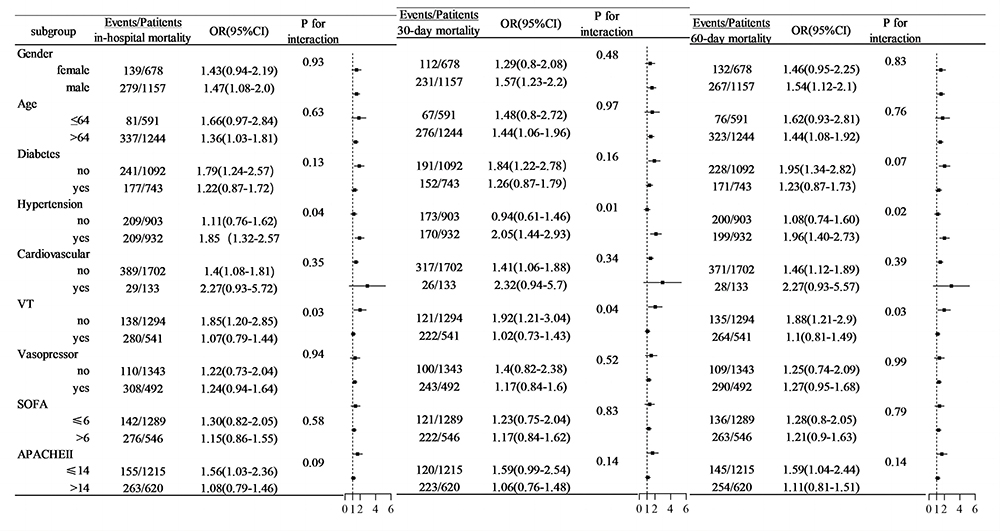 |
Figure 4 Forest plots of hazard ratios for mortality in different subgroups. |
Discussion
The objective of this study was to assess the association between SHR and clinical outcomes in patients with sepsis from a two center cohort. The findings of this study indicate that a higher SHR is significantly associated with hospital mortality in septic patients. Even after adjustment for confounding risk factors, the association between SHR and hospital mortality remained strong. Consequently, SHR may be a valuable decision-making tool for clinicians and may be an independent risk factor in patients with sepsis.
SHR is regarded as a potential indicator of critically ill patients. Robert et al first noted a significant rise in mortality specifically in the fourth and fifth SHR quintiles, with average SHR values of 1.14 and 1.38, respectively.7 Recent studies have identified various relationships between high SHR and mortality risk in critically ill individuals and pneumonia patients with CURB-65 scores of ≥2.11–13Nevertheless, there is a paucity of studies that have focused on sepsis.The results of the multivariate regression analysis revealed a significant and independent correlation between SHR and in-hospital mortality, 30-day mortality, and 60-day mortality.The impact of SHR is significant at multiple time points. This indicates that the risk factors reflected by SHR are persistent and cumulative, emphasizing the importance of long-term monitoring and management of such risk factors.Trend analysis further reinforces the notion of SHR as an effective predictor of mortality and provides a visual understanding of how risks vary with changes in SHR.
Despite the lack of clarity surrounding the definition of stress-induced hyperglycaemia in sepsis and the ongoing debate surrounding the necessity for strict blood glucose control as a treatment,14–16 some studies have indicated that glycotoxicity may play a significant role in the development of the disease.17,18 The mechanism of sepsis-related stress-induced hyperglycaemia is complex and involves not only the activation of the hypothalamic-pituitary-adrenal (HPA) axis and the release of cortisol from the adrenal glands,19 but also the disruption of glucose metabolism and insulin resistance under the influence of endotoxins and inflammatory factors.5 Studies have demonstrated that insulin resistance in patients with sepsis is directly proportional to the severity of the stress response. During sepsis, insulin-induced tyrosine phosphorylation of IRS-1 and subsequent activation of PI-3-kinase are impaired, resulting in defective GLUT-4 receptor translocations, decreased glucose uptake, skeletal muscle insulin resistance, and hepatic insulin resistance.20,21 Some researchers have proposed that mild to moderate stress-induced hyperglycaemia may have a protective effect during stress and critical illness.22,23 Controlling blood glucose in sepsis patients has always been a subject of controversy.24 Robert’s study indicates that SHR can provide uniform clinical risk stratification of stress hyperglycaemia in clinical practice by correcting for background blood glucose. This study indicates a significant correlation between SHR greater than 1.06 and mortality in sepsis patients. In particular, sepsis patients with SHR greater than 1.32 exhibited a significant increase in mortality rate. Consequently, it can be postulated that the control of SHR within a reasonable range may result in an improvement in patient prognosis.
Furthermore, the study conducted further analysis of risk stratification within each subgroup. The subgroup analysis demonstrated that the value of SHR in predicting in-hospital mortality was consistent among patients grouped by SOFA score.The impact of SHR on in-hospital mortality was more pronounced in elderly patients, possibly due to the higher prevalence of frailty in this population.25 Nevertheless, the study found that hypertension, rather than diabetes, alters the predictive power of the SHR. Figure 5 of this study illustrates that individuals without hyperglycemia exhibit higher mortality rates. This phenomenon might be attributed to the fact that diabetic patients undergo chronic inflammation and persistent oxidative stress, manifesting an adaptive response to stress-induced hyperglycemia.26 Furthermore, diabetic patients on insulin therapy may experience enhanced anti-inflammatory effects, resulting in improved prognoses.27 Hypertension itself can cause endothelial dysfunction, vascular rigidity, and organ damage, and is frequently associated with metabolic syndrome, thereby intensifying the detrimental impact of elevated SHR on survival outcomes.28 This implies that the control of blood pressure may have a considerable impact on the predictive efficacy of SHR for in-hospital mortality.Another interesting finding is that in patients not using mechanical ventilation, the predictive value of SHR appears to be higher.It implies that among critically ill patients who do not require ventilatory support, SHR may serve as an early warning sign for impending deterioration or failure of compensatory mechanisms.But the mechanism of this phenomenon needs further study.
 |
Figure 5 Shows the HbA1c levels of <6.5% or ≥6.5% and the rate of mortality based on admission glucose (A) and SHR (B). |
Limitations
Although the relationship between SHR and in-hospital mortality in patients with sepsis has been revealed, it is important to note that this study is not without significant limitations. Firstly, the retrospective design introduced biases and potentially uncontrollable factors, and despite adjustments, unmeasured variables could affect the results. Secondly, the study primarily concentrated on the relationship between SHR and in-hospital mortality, with a paucity of attention paid to the association with other indicators. Furthermore, the endpoints were not subjected to a comprehensive examination, with length of hospital stay, organ function, and out-of-hospital follow-up remaining under-investigated. Thirdly, the study only considered the blood glucose values of the initial admission, which precluded an assessment of the relationship between ambulatory SHR and disease progression. Further studies are required to ascertain whether the control of SHR will result in an improvement in the clinical prognosis in the future.
Conclusion
In conclusion, our research results show that when SHR is greater than 1.06, the short-term mortality of septic patients increases, which can be used as a valuable indicator for risk stratification of in-hospital mortality in critically ill septic patients. Monitoring SHR can facilitate decision making and disease management in clinical practice.
Patient Data Confidentiality Disclaimer
We hereby affirm our commitment to the strict confidentiality of patient data. We understand the sensitive nature of this information and the trust placed in us by our patients. To ensure the highest level of data protection, we adhere to the following principles:
- **Compliance with Laws and Regulations**: We strictly followed the “Declaration of Helsinki”, “International Ethical Guidelines for Research Involving Human Health” and other medical ethics standards, and fully respect the subjects’ rights to know and privacy, and effectively protect the subjects’ rights and well-being.
- **Limited Access and Use**: We restrict access to patient data to authorized personnel who require it for legitimate business purposes, such as providing medical care or managing patient records. We ensure that such personnel are appropriately trained on data privacy and confidentiality practices.
- **Secure Storage and Transmission**: We maintain appropriate administrative, technical, and physical safeguards to protect patient data from unauthorized access, use, disclosure, disruption, modification, or destruction. This includes the use of encryption for data in transit and at rest, as well as secure storage facilities and regular security audits.
- **Minimization of Data Collection**: We collect only the minimum amount of patient data necessary to fulfill our legitimate business purposes. We regularly review our data collection practices to ensure that they remain necessary and appropriate.
- **Data Retention and Disposal**: We retain patient data only for the period necessary to fulfill our legal and business obligations. Once this period has expired, we dispose of the data in a secure and responsible manner.
- **Breach Notification**: In the event of a breach of patient data confidentiality, we will promptly notify affected patients and relevant authorities in accordance with applicable laws and regulations.
- **Third-Party Providers**: We carefully select and monitor third-party providers who may have access to patient data. We require such providers to comply with our data privacy and confidentiality policies and practices.
- **Patient Rights**: We respect the rights of patients to access, correct, and request the deletion of their personal information in accordance with applicable laws and regulations.
By adhering to these principles, we strive to maintain the trust of our patients and to ensure the confidentiality and security of their data.
Data Sharing Statement
The datasets that were used and evaluated in this study can be obtained from the corresponding author upon making a reasonable request.
Ethical Statements
The protocol was approved by the institutional ethics boards of each hospital. Informed consent was waived because of the non-interventional, retrospective design of the study.Data analysis was performed in accordance with the 1964 helsinki Declaration and its later amendments.
Author Contributions
Chaoping Ma, Weisong Jiang, Juan Li and Wenwu Sun have contributed equally to this work and share the first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Key Supporting Subject Researching Project of Shanghai Municipal Health Commission (No. 2023ZDFC0106);the Science and Technology of Shanghai Committee (23Y31900100, 23Y31900102 and 21MC1930400);National Natural Science Foundation of China (No. 82172138);Innovation Research Project of Shanghai Science and Technology Commission (No. 21Y11902400).
Disclosure
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as potential conflicts of interest.
References
1. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
2. Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the global burden of disease study. Lancet. 2020;395(10219):200–211. doi:10.1016/S0140-6736(19)32989-7
3. Cohen J, Vincent JL, Adhikari NK, et al. Sepsis: a roadmap for future research. Lancet Infect Dis. 2015;15(5):581–614. doi:10.1016/S1473-3099(15)70112-X
4. Pierrakos C, Vincent JL. Sepsis biomarkers: a review. Crit Care. 2010;14. doi:10.1186/cc8872
5. Marik PE, Raghavan M. Stress-hyperglycemia, insulin and immunomodulation in sepsis. Intensive Care Med. 2004;30(5):748–756. doi:10.1007/s00134-004-2167-y
6. Dungan K, Braithwaite SS, Preiser JC. Stress hyperglycemia. Lancet. 2009;373:1798–1807. doi:10.1016/S0140-6736(09)60553-5
7. Roberts GW, Quinn SJ, Valentine N, et al. Relative hyperglycemia, a marker of critical illness: introducing the stress hyperglycemia ratio. J Clin Endocrinol Metab. 2015;100(12):4490–4497. doi:10.1210/jc.2015-2660
8. Xu W, Song Q, Wang X, et al. Association of stress hyperglycemia ratio and in-hospital mortality in patients with coronary artery disease: insights from a large cohort study. Cardiovasc Diabetol. 2022;21(217). doi:10.1186/s12933-022-01645-y
9. Huang YW, Yin XS, Li ZP. Association of the stress hyperglycemia ratio and clinical outcomes in patients with stroke: a systematic review and meta-analysis. Front Neurol. 2022;13:999536. doi:10.3389/fneur.2022.999536
10. Lin Z, Liang X, Zhang Y, et al. Positive association between stress hyperglycemia ratio and pulmonary infection in patients with ST-segment elevation myocardial infarction undergoing percutaneous coronary intervention. Cardiovasc Diabetol. 2023;22(76). doi:10.1186/s12933-023-01799-3
11. Zhang C, Shen HC, Liang WR, et al. Relationship between stress hyperglycemia ratio and all cause mortality in critically ill patients: results from the MIMIC-IV database. Front Endocrinol. 2023;14:1111026. doi:10.3389/fendo.2023.1111026
12. Li L, Zhao M, Zhang Z, et al. Prognostic significance of the stress hyperglycemia ratio in critically ill patients. Cardiovasc Diabetol. 2023;22(275). doi:10.1186/s12933-023-02005-0
13. Liu B, Chen Y, Yu L, Zhou M. Stress hyperglycemia ratio is associated with systemic inflammation and clinical outcomes in diabetic inpatients with pneumonia on admission. J Diabetes. 2023;15(7):545–556. doi:10.1111/1753-0407.13398
14. van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345(19):1359–1367. doi:10.1056/NEJMoa011300
15. Wiener RS, Wiener DC, Larson RJ. Benefits and risks of tight glucose control in critically ill adults: a meta-analysis. JAMA. 2008;300(8):933–944. doi:10.1001/jama.300.8.933
16. Wu Z, Liu J, Zhang D, et al. Expert consensus on the glycemic management of critically ill patients. J Intensive Med. 2022;2(3):131–145. doi:10.1016/j.jointm.2022.06.001
17. Luo X, Wu J, Jing S, Yan LJ. Hyperglycemic stress and carbon stress in diabetic glucotoxicity. Aging Dis. 2016;7(1):90–110. doi:10.14336/AD.2015.0702
18. López-Acosta O, Ruiz-Ramírez A, Barrios-Maya MÁ, et al. Lipotoxicity, glucotoxicity and some strategies to protect vascular smooth muscle cell against proliferative phenotype in metabolic syndrome. Food Chem Toxicol. 2023;172:113546. doi:10.1016/j.fct.2022.113546
19. Marik PE, Zaloga GP. Adrenal insufficiency in the critically ill: a new look at an old problem. Chest. 2002;122(5):1784–1796. doi:10.1378/chest.122.5.1784
20. Kanety H, Feinstein R, Papa MZ, Hemi R, Karasik A. Tumor necrosis factor alpha-induced phosphorylation of insulin receptor substrate-1 (IRS-1). Possible mechanism for suppression of insulin-stimulated tyrosine phosphorylation of IRS-1. J Biol Chem. 1995;270(40):23780–23784. doi:10.1074/jbc.270.40.23780
21. Pessin JE, Saltiel AR. Signaling pathways in insulin action: molecular targets of insulin resistance. J Clin Invest. 2000;106(2):165–169. doi:10.1172/JCI10582
22. Mizock BA. Alterations in fuel metabolism in critical illness: hyperglycemia. Best Pract Res Clin Endocrinol Metab. 2001;15(4):533–551. doi:10.1053/beem.2001.0168
23. Marik PE, Bellomo R. Stress hyperglycemia: an essential survival response! Crit Care. 2013;17(305). doi:10.1186/cc12514
24. Alhatemi G, Aldiwani H, Alhatemi R, Hussein M, Mahdai S, Seyoum B. Glycemic control in the critically ill: Less is more. Cleve Clin J Med. 2022;89(4):191–199. doi:10.3949/ccjm.89a.20171
25. Kojima G, Iliffe S, Walters K. Frailty index as a predictor of mortality: a systematic review and meta-analysis. Age Ageing. 2018;47(2):193–200. doi:10.1093/ageing/afx162
26. Bahadoran Z, Mirmiran P, Ghasemi A. Role of nitric oxide in insulin secretion and glucose metabolism. Trends Endocrinol Metab. 2020;31(2):118–130. doi:10.1016/j.tem.2019.10.001
27. Dandona P, Aljada A, Mohanty P, et al. Insulin inhibits intranuclear nuclear factor kappaB and stimulates IkappaB in mononuclear cells in obese subjects: evidence for an anti-inflammatory effect? J Clin Endocrinol Metab. 2001;86(7):3257–3265. doi:10.1210/jcem.86.7.7623
28. Katsimardou A, Imprialos K, Stavropoulos K, Sachinidis A, Doumas M, Athyros V. Hypertension in metabolic syndrome: novel insights. Curr Hypertens Rev. 2020;16(1):12–18. doi:10.2174/15734021156661904151618
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.