")
Back to Journals » Patient Preference and Adherence » Volume 19
Barriers and Facilitators to Adherence to a Healthy Diet Across the Spectrum of Chronic Kidney Disease
Authors Trigueros-Flores XB, Luna-Hernández G, Santos-Lopez MF, Pérez-Galván L, Flores-Camacho KJ, Díaz-Canchola LM, Cueto-Manzano AM, Chávez-Chávez HE, Cerrillos-Gutiérrez JI, Rojas-Campos E , Martín-del-Campo F
Received 8 October 2024
Accepted for publication 3 January 2025
Published 16 January 2025 Volume 2025:19 Pages 123—137
DOI https://doi.org/10.2147/PPA.S494390
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Xochitl B Trigueros-Flores,1 Gabriela Luna-Hernández,2 María F Santos-Lopez,1 Lucía Pérez-Galván,1 Karen J Flores-Camacho,1 Laura M Díaz-Canchola,3 Alfonso M Cueto-Manzano,1 Hugo E Chávez-Chávez,3 Jose I Cerrillos-Gutiérrez,4 Enrique Rojas-Campos,1 Fabiola Martín-del-Campo1
1Unidad de Investigación Médica en Enfermedades Renales, Hospital de Especialidades CMNO, IMSS, Guadalajara, Jalisco, México; 2Centro Universitario de Ciencias de la Salud, Universidad de Guadalajara, Guadalajara, Jalisco, México; 3División de Medicina Interna, Hospital General Regional 180, IMSS, Guadalajara, Jalisco, México; 4División de Nefrología y Trasplantes, Hospital de Especialidades CMNO, IMSS, Guadalajara, Jalisco, México
Correspondence: Fabiola Martín-del-Campo, Unidad de Investigación Médica en Enfermedades Renales, Hospital de Especialidades, CMNO, IMSS, Belisario Domínguez No. 1000, Col. Independencia, Guadalajara, Jalisco, CP 44320, México, Tel +52 (33)1071-1190, Email [email protected]
Purpose: A healthy diet plays an important role for chronic kidney disease (CKD) treatment, but adherence to nutritional recommendations is frequently low. The aim of the present study was to describe barriers and facilitators to adherence to a healthy diet in people with CKD.
Patients and Methods: Cross-sectional study; 80 predialysis (n=20), hemodialysis (n=20), peritoneal dialysis (n=20) and transplant (n=20) patients matched by age and sex, were included. Nutritional evaluation included subjective global assessment, anthropometry, quality of food consumption (Mini-ECCA v.2), self-perception about diet and willingness to change. Barriers and facilitators were evaluated with a qualitative approach (semi-structured interviews). Concepts were converted into “in vivo” and “theoretical” codes, then, grouped into categories. A second analysis was performed with the ATLAS.ti software.
Results: Frequency of malnutrition was 50% in people receiving dialysis. Quality of food consumption was healthier on people with CKD stages 3b-5 (40%) and people with kidney transplant (65%) compared to peritoneal dialysis (25%) and hemodialysis (0%). The main themes influencing adherence to a healthy diet were: need for nutritional guidance, economy, dietary restrictions, willingness to change, relationship with consequences in disease control and health status, aversion for healthy foods, bad and good self-perception, family support, feelings and emotions, environment, eating habits and CKD itself. Lack of time, work, economy, food preferences and cravings were the main barriers in people with CKD stage 3b-5 and transplant, while low willingness to eat healthy foods and dietary restrictions were the main barriers in people receiving dialysis.
Conclusion: Personal, environmental, health professional-related, CKD related as well as feelings and emotions aspects that people with CKD face in a daily basis, act as barriers or facilitators when trying to follow a healthy diet. Individualizing nutritional treatment taking into account people with CKD perspectives and situations is of utmost importance to improve adherence to nutritional treatment.
Plain summary: In this article, the authors discuss the main barriers and facilitators that people with kidney disease face when trying to follow a healthy diet (from the people with CKD perspective). A healthy diet has been associated with lower progression of kidney disease and helps to prevent complications; however, adherence to nutritional recommendations is frequently low. People on dialysis had the unhealthier diet compared to people on predialysis or kidney transplant. People perceived dietary restrictions, lack of nutritional counseling and knowledge, economic constraints, lack of social and family support, negative effects of food on their health, dislike or aversion to healthy foods, lack of time and environment limitations as the main barriers to adhere to a healthy diet.
Additionally, since diets are considered complicated (especially renal diets), strategies to improve willingness to eat healthy, counseling about food variety and preparation, some liberalization of dietary restrictions (when possible) and considering family support could help people with CKD to increase skills to adhere to a healthier diet. Considering people with CKD perspectives is of utmost importance when planning nutritional treatment and counseling, to improve adherence and therefore, clinical outcomes.
Keywords: healthy diet, treatment adherence, qualitative research, chronic renal insufficiency
Introduction
According to the World Health Organization a healthy diet includes the consumption of fruits, vegetables, legumes, nuts and whole grains, to protect the body from chronic non-communicable diseases such as diabetes and hypertension, among others, which are also considered risk as factors for development of chronic kidney disease (CKD).1,2 Healthy diets have been shown to have a positive impact on prevention and treatment of people with CKD, increasing insulin sensitivity and lowering systemic inflammation, delaying progression, preventing metabolic complications and reducing risk of cardiovascular disease and death.3–6
In people with CKD, the loss of body homeostasis directly affects nutritional processes; therefore, it is important to make dietary changes to prevent and/or treat the metabolic complications as well as maintain the acid-base, electrolyte and fluid balance.4,7 These dietary modifications (sodium, potassium, protein and phosphorus) frequently limit the consumption of some healthy foods, hence the classic healthy diet could be not totally appropriate for all CKD subjects.2 Dietary restrictions make diet complex and difficult to adhere, due to multiple factors.8,9 Therefore, people with CKD need specialized nutritional counseling to adapt a healthy diet according to the stage and treatment they received, as well as considering personal and cultural needs.
Although the beneficial effects of a healthy diet have been demonstrated, people with CKD had a diet low in fruit and vegetables, as well as high in ultra-processed foods, which contribute to decrease in kidney function and higher mortality.10–12
People with CKD, dialysis and kidney transplant (KT) often face different barriers that limit self-care and adherence to a healthy life style, related not only to kidney disease and its treatment, but also to social, personal, environmental or psychological aspects.13,14 One of the most frequent problems found in the literature for self-care and disease management of people with CKD and RRT is the diet, as it involves major lifestyle changes.15
Social, economic and cultural factors of people with CKD daily life should not be left aside when planning nutritional interventions, as this may help to improve adherence to healthier diets and life-style.16 However, evaluation of barriers and facilitators for a healthy diet, from the patient’s perspective has been poorly explored;17,18 moreover, there is no study comparing this issue in people with CKD and on the different renal replacement therapies (RRT).
Therefore, the aim of the present study was to describe the barriers and facilitators to adherence to a healthy diet in people with CKD stage 3b-5, peritoneal dialysis (PD), hemodialysis (HD) or KT.
Materials and Methods
Study Design and Population
This is a cross-sectional study with explanatory sequential mixed methodology performed from July 2023 to January 2024. Adult clinically stable with CKD stages G3b to 5, PD (vintage >3 months), HD (vintage >3 months, sessions at least twice a week) or KT (first KT, >3 months after grafting), attending the nephrology service of a secondary care hospital were invited to participate. Subjects were matched by sex and age in each treatment group; those with lupus, vasculitis and collagenopathies, active infection, on antibiotic treatment, immunosuppressive medications (except in those with KT), liver disease, decompensated heart disease, cancer, AIDS and previous KT were excluded. The study complies with the Helsinki Declaration and was approved by the Research Ethics Committee of the National Committee for Scientific Research of the Mexican Social Security Institute, with the registration number R-2023-785-040. The transplants were conducted in accordance with the Declaration of Istanbul; in each transplant, an acceptance document is signed with the donor’s consent to perform the transplant before the Transplant Ethics Committee. All subjects signed an informed consent to participate in the study, which included the publication of anonymous direct responses and quotes.
Clinical and Nutritional Evaluations
A research trained physician obtained sociodemographic data through direct interview and performed the clinical evaluation consisting on vital signs measurement and physical examination. Previously trained dietitians performed a complete nutritional evaluation including a 7-points subjective global assessment; subjects with a global score of 1–2 points were considered as severe malnutrition, 3–5 points as mild-to-moderate malnutrition, and 6–7 as low risk or normal nutritional status.19 Anthropometric evaluation consisted on measurement of weight, height, mid-arm circumference and skinfold thickness (triceps and subscapular); dry weight was estimated by spectroscopic bioimpedance with the BCM-Body Composition Monitor (Fresenius Medical Care ®) to calculate body mass index.
Quality of Food Consumption
The Mini Food Intake Quality Survey (Mini-ECCA v.2) was used to evaluate quality of food consumption, which is a validated instrument for Mexican population.20 This tool is based on the frequency of 14 food and beverages consumption: water, vegetables, fish, sweetened beverages, fruits, type of fat used more often, healthy unprocessed fat and avocado, foods not prepared at home, type of meat, industrialized snacks, sweets and desserts, legumes, types of cereals and alcoholic beverages. For each question, three or four answer choices are given, generally on a Likert scale, using simultaneously photographs as a visual reference to estimate food quantity. Subjects were classified in three groups as previously reported: a) Healthy diet, b) Diet in need of improvement, and c) Unhealthy diet.20
Additionally, the Mediterranean Diet Adherence Score (MEDAS) was used to evaluate adherence to a healthy diet pattern. The MEDAS is composed of 14 dichotomous questions on adherence to habitual intake of foods: olive oil (use and amount), vegetables, fruits, red or processed meat, saturated fat (animal fat and margarine), sweet beverages and sodas, wine, legumes, fish and seafood, sweets and pastries, seeds and nuts, meat preferences (white vs red) and fried foods.21
Self-perception of diet quality, as well as willingness to change dietary behavior to a healthier diet, were evaluated with a 0–10 points Likert scale; the higher the score the healthier perception of diet and the better willingness to change diet behavior, respectively.
Barriers and Facilitators for a Healthy Diet
A semi-structured interview based on healthy food groups (fruits, vegetables, legumes, healthy unprocessed fat/avocado) was applied. The interviews were recorded by voice note with a smartphone; patients had freedom of time to answer the questions. Interviews were conducted in a hospital environment, where the subject was seated, calmed, stable and in most cases accompanied by a family member or primary caregiver who supported people with CKD in cases of hearing or understanding difficulties. The interviews were performed by four dietitians (XBTF, MFSL, LPG, KJFC) previously trained to respect the sensitivity of the interviewee, as well as to apply the interviews without influencing their responses. After asking about self-perception of diet quality and willingness to change, we asked about the barriers and facilitators to achieve a healthy intake of the healthy food groups. The interviews were applied following the evaluation of the Mini-ECCA v.2; therefore, the interviewer had a better context of the subject eating habits, which helped to direct the interview (Supplementary Table 1).
Quantitative Statistical Analysis
Nominal variables are shown as frequency (percentage), whereas dimensional ones as mean ± standard deviation or median (25–75% percentiles), as appropriate. Comparisons between groups were made with ANOVA (Bonferroni test was used for post-hoc comparisons) and x 2, as appropriate. A p value <0.05 was considered as significant.
Qualitative Statistical Analysis
A thematic content analysis was performed. The recorded interviews were Verbatim transcribed on Word by two trained dietitians (XBTF and MFSL); the words and concepts with the greatest repetition were highlighted and subsequently converted into codes, these codes were counted and then grouped into categories, until reaching saturation of data (when there is no new data or the data obtained is repetitive). Subsequently, after the manual analysis, data underwent a second analysis using the software ATLAS.ti (web version) to compare the previously obtained results with manual analysis. A second evaluator, expert in qualitative research (GLH), supervised both manual and software data analyses.
Results
Eighty subjects were interviewed, 20 in each group: CKD stage 3–5, PD, HD and KT. Table 1 shows the clinical and sociodemographic characteristics of people with CKD. No significant differences were found between groups, however, people with KT had a non-significant trend to have less hypertension antecedent and lower systolic blood pressure, than the other groups.
 |
Table 1 Sociodemographic and Clinical Results Between Groups |
Nutritional Characteristics and Quality of Food Consumption
People receiving HD and PD have the worst nutritional status according to subjective global assessment. People receiving HD also had the lowest muscle and fat mass (mid-arm circumference and subscapular skinfold thickness) as well as a non-significant trend for a lower body mass index than the others. People with CKD stage 3–5 and KT had the healthier diet compared to those receiving dialysis, from whom people receiving HD had the worst diet evaluated, either with the Mini-ECCA or MEDAS questionnaires. In general, subjects of all groups perceived their diet as “healthy” with a mean score of 7.3±1.9. People receiving HD had a non-significant trend to have a lower self-perception of diet quality. Interestingly, willingness to change their diet towards healthier habits was very high in all groups (Table 2).
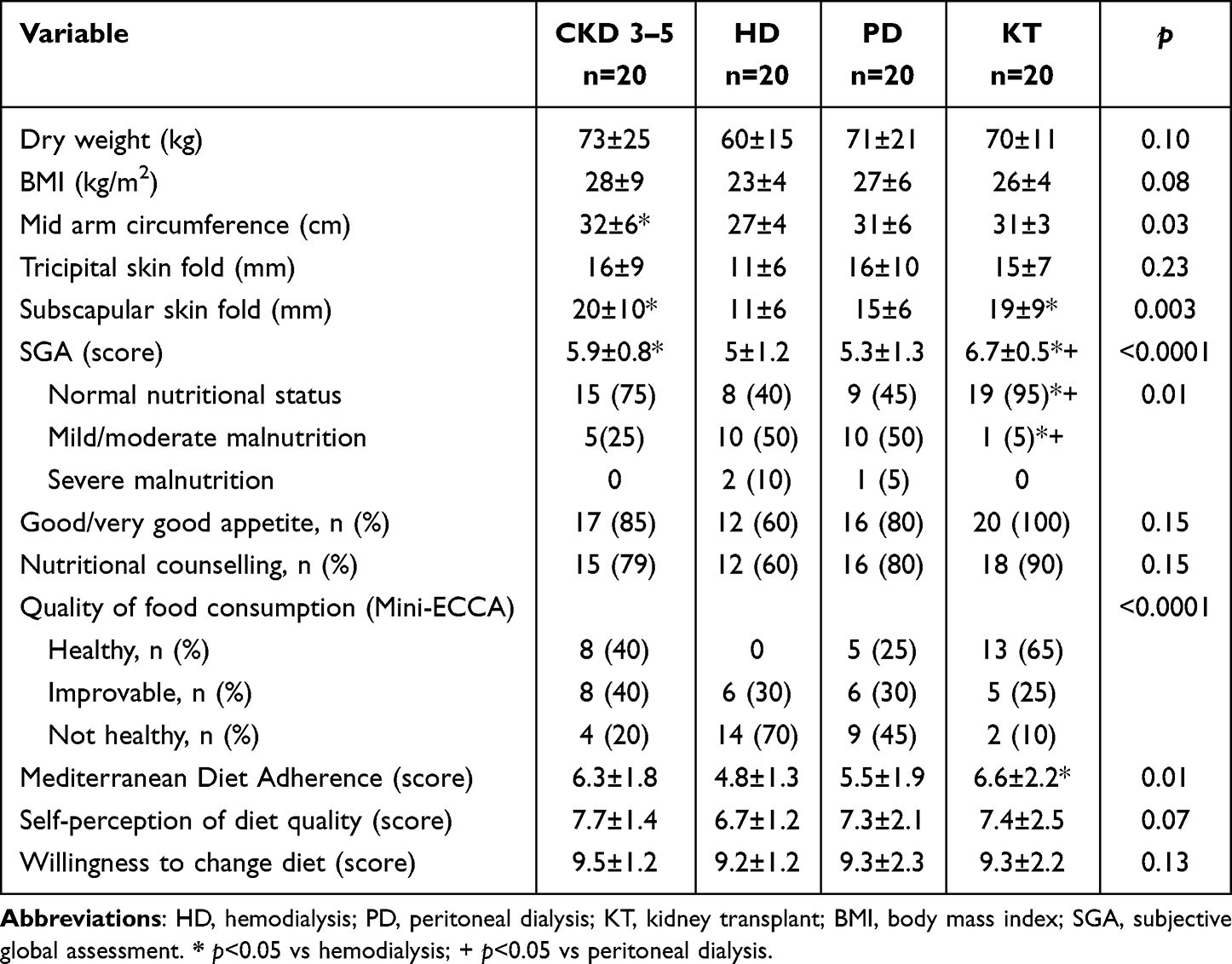 |
Table 2 Comparison Nutritional Variables and Quality of Food Consumption Between Groups |
Barriers and Facilitators to a Healthy Diet
In the first manual analysis of barriers and facilitators, a total of 29 codes for barriers and 21 for facilitators were obtained, which were further divided into 6 categories related to: person-related, health professional, comorbidities and symptoms, environment, emotions/feelings and disease.
Figure 1 shows the comparison of main barriers to a healthy diet between the groups. Barriers related to environment category were the most important in people with RRT, meanwhile person-related category factors were more important in people with CKD stage 3–5. Economy, taste/flavor/cravings and relation with negative effects in disease control were the main barriers in all groups. Dietary restrictions were common barriers in people with CKD stage 3–5, PD and KT, while people receiving PD identified also the low willingness to change as an important barrier. Finally, lack of time was common in people receiving KT and HD, however in HD it was mainly related with the disease and treatment while in KT with work.
 |
Figure 1 Barriers to a healthy diet by group.Each square represents a code of barriers; size of the square represents the importance of each code (frequency); and the color represents the category. (A) Barriers in people receiving hemodialysis. (B) Barriers in people receiving peritoneal dialysis. (C) Barriers in people with CKD stage 3–5. (D) Barriers in people with kidney transplant. |
Figure 2 shows the facilitators to a healthy diet by groups. Health professional related factors were considered the main facilitators for eating a healthy diet in all groups including nutritional guidance/education, dietary prescription, alternative preparations and variety of foods, release from diet and restrictions. Person-related factors had a central role in people with CKD 3–5, PD and HD, particularly better willingness to change and taste for food, while in people with KT accessible and available food as well as to adaptability to a healthy diet (environment) were important facilitators. Family support was a notable facilitator in people receiving HD. Although the category of feelings and emotions was not very representative in the facilitators analysis, it is worth noting that the encouragement to eat healthy was a common factor in all subjects.
 |
Figure 2 Facilitators to a healthy diet by group.Each square represents a code of facilitator; size of the square represents the importance of each code (frequency); and the color represents the category. (A) Facilitators in people receiving hemodialysis. (B) Facilitators in people receiving peritoneal dialysis. (C) Facilitators in people with CKD stage 3–5. (D) Facilitators in people with kidney transplant. |
In the second analysis of barriers and facilitators using the ATLAS.ti web version software, the interviews were analyzed in more depth, obtaining 12 main themes from the same categories of the first analysis. The principal themes and quotations are shown in Supplementary Table 2.
The barriers and facilitators found in our study were then divided into different themes, which are explained below.
Need for Nutritional Guidance and Knowledge
All groups expressed the need to obtain nutritional guidance, as well as knowledge and information about healthy eating as a facilitator, since most of them believe they have a healthy diet but our results showed this was not the case. They also expressed having no idea or notion of how to improve their diet.
That they teach me how to eat (nutritionists)… as it should be. That they tell me that it is good for me and that it is not good for me, all that
After the scare, you start to take care of yourself, you start to investigate more what is good, what is bad and... well, I have not improved because... the lack of knowledge
Other subject expressed the importance of guidance:
If someone doesn’t guide you, then you won’t know what to eat
Economy
One of the main barriers perceived by patients with RRT was the economic factor, since they considered it one of the most determining points for following a healthy diet. Some of them mentioned:
The economic part that does not allow one to buy what is needed for a diet
One (referring to himself) feeds according to how... as I said... within one’s reach and according to one’s needs
I would like to… (follow a healthy diet) but right now, as I say, we are in very bad shape economically and buying my things for the diet is a lot of expense for others
In addition, as expected they also mentioned that having financial solvency would be of great help in the following a healthy diet, being able to buy the elements needed for a healthy diet.
One subject said:
Well, just like I told you, have financial solvency because it is a lot of expense to have to come here. And now with the economic solvency, it is logical that... they would make things easier for us
Dietary Restriction
Other limitation that was present in all groups to following a healthy diet are the dietary restrictions that health professionals regularly impose on them, who report feeling restricted, leading to a low consumption of fruits, vegetables and legumes.
Some of them said:
The thing is that my diet is very rigorous in some foods that even if I wanted to eat them I can’t eat them (fruits)
Well, they took away a lot of things to eat from me
Eh.I have a very restricted diet, as for fruits, I can’t eat all of them
Yes, I like them, I love lentils but they told us that they hurt us a lot. I don’t know what they have a lot of iron or potassium I don’t know what they said
Willingness to Change
Despite the difficulty of the diet and factors that act as barriers, people with CKD and KT reported the greatest willingness to improve their diet, the desire to learn to eat correctly and to improve their health status as well as their quality of life. On the other hand, patients receiving dialysis had the lowest willingness to change.
I would be willing to be told “Hey, you know what? For you, for your body, for you…with your condition it is better that you eat this, this and remove this or increase this
Relation with Consequences in Disease Control and Health Status
Other highlighted barrier was the relationship that subjects attributed between food and negative health effects. They mentioned that eating some healthy foods can have negative impact on their health. This was reflected in the consequences that they perceived, such as alteration of the laboratory results such as increased phosphorus, potassium or glucose levels, or gastrointestinal symptoms. This perception leads them to conclude that eating this type of food affects both their health status and the control and management of their disease. While in PD and CKD patients the main barrier was poor appetite, in HD and KT subjects gastrointestinal symptoms were the most frequent barrier.
They said:
Well, the thing is that... in terms of beans, we... are limited here by the... their content. If you eat a lot of beans, the... phosphorus harms you, your phosphorus rises
I didn’t use them out of fear, because I… because I know that walnuts and almonds are a healthy protein, but potassium scares me because… remember that I’m going to get sick ‘oh I don’t want to’.
I think that when it comes to fruit, the sugar is what stops me from consuming more. “It would be too much sugar for my… way of thinking.
Beans hurt me, they inflame me
Despite this, all of the groups expressed that a motivation to eat healthier would be the positive effects that a healthy diet could have on them.
Aversion/Dislike for Healthy Foods
A simple, but proven to be a great limitation for the consumption of healthy foods, was the dislike or aversion. People with CKD and KT were the groups who most mentioned that they do not like the taste of food, especially vegetables and legumes. In the interviews, it was very common to find these types of phrases:
Mmmh…what’s stopping me.I hardly like vegetables very much
The thing is... I don’t like many of those foods either, I eat beans only once a week… I hardly like them, lentils almost never, and so on
The opposite occurred in patients undergoing dialysis, since the liking for healthy foods was mostly reflected in these groups.
Bad and Good Self-Perception
Self-perception of people with CKD ability to follow recommendations, indications or nutritional prescriptions can act as a barrier or facilitator, depending on the situation.
Encourage trying (healthy foods) because I am very bad at trying
I can do it... I can do it… I try to follow my diet
Family Support and Lack of Family Support
Social and family support is one of the pillars that facilitate or prevent adherence to a healthy diet. Participants expressed that having a person who supports and helps them to get healthy foods or simply prepare their meals, making easier to follow an adequate diet, as in many cases (especially those on PD and HD) are unable to take care of themselves most of the times. However, others mentioned that the lack of this support directly affected the quality of their diet, since not having someone to support them makes it more difficult to consume and get healthy foods. HD, PD and KT were the groups that highlighted the need for family support.
The support of… well yes, of work and of… of my family
Because sometimes there is no one to help me (to provide unprocessed fats)
Feelings and Emotions
Emotions and feelings were found to influence food choices. These aspects included fear guiltiness for eating, feeling of exclusion or difference from others, frustration and anger, yearning for foods, feeling of obligation to eat and desire to improve.
Well... they scare me because many things they say harm me, like vegetables, which sometimes say, they contain a lot of water and I don’t have to consume a lot of water (fear)
I’m not supposed to consume much because of the phosphorus, but oh, I could eat beans every day, I like beans (yearning)
It’s very different because they taste different because I have to make them one way for me and another way for them (rest of the family) and sometimes I crave the others (exclusion/difference)
I’m fed up of what I eat (anger/frustration)
Well, as I say, you need to ‘give it a try’ because well, yes, yes... if you don’t pay attention, no, this doesn’t work (desire to improve)
They also told me the same thing, that it hurts me, I ate the avocado as they say here. Smuggled (guilt)
A little more would be... it’s just monotony, vegetables without anything, they’re... pure cooked... they don’t taste anything but water, to me they taste like water and I’m fed up... I couldn’t eat just vegetables, I mean if they told me ‘here’ is your plate of vegetables and eat... that’s just what you’re going to eat
I could not, yes I would eat it out of hunger but I would not be happy (obligation to eat)
Patients on RRT expressed fear; either of worsening their health or damaging the kidney graft; also people with CKD, HD and KT expressed annoyance at eating due to the monotony on their diets, showing the complex and different concerns of the patients across the stages of CKD.
Environment
The environment can also act as a barrier for them, since all groups expressed difficulty in obtaining healthy foods either because it is not common to have that type of food in their homes or because it is not available in stores, or even there are no nearby or accessible places to get healthy foods. At the same time, the factor that they found as a facilitator is the presence of stores and accessible places to purchase healthy foods.
At least in the community where I am, there are not all the facilities to... to go, right? The store is very far away
However, the environment of people with CKD not only takes into account the availability or accessibility of food, but also takes into account other factors such as lack of time or work, in the case of CKD stage 3–5 and KT (who worked most frequently) but also in HD, since they mentioned that hospital transport for their HD sessions are a barrier that takes away time for proper nutrition.
I’m out all day and I can no longer be at home making smoothie or cooking vegetables, everything is because ‘one’ has to work
Healthy and Unhealthy Eating Habits
Previous healthy or unhealthy eating habits were also important determinants in the acceptance or rejection of a healthy diet; people with CKD and PD reported maintaining some healthy eating habits in a regular basis and mentioned this as a facilitator to follow instructions. On the contrary, HD patients who did not have healthy eating habits were the ones who faced more difficulties.
A patient who had good habits before said:
It’s just that... like I used to take great care of myself, I’ve always had the habit of eating vegetables.
In contrast, other patient said:
Yes, I do need willpower sometimes for things because I do make a fool of myself with vegetables, with... things that I wasn’t used to that now... have changed drastically. But I have to get used to all that
Chronic Kidney Disease
Finally, we found that some people with CKD considered kidney disease itself as a barrier to adherence to a healthy diet. Interestingly, people receiving HD and PD mentioned that water in food was a limitation for consuming foods such as fruits or vegetables.
The disease that prohibits you many things
Interviewer: What would help you have a better diet?
Patient: Not having this disease
Well, right now everything depends on the kidney results.
Discussion
To the best of our knowledge, this study is the first to describe the barriers and facilitators to a healthy diet in people with CKD stage 3–5, HD, PD and KT, and our findings showed that most of these subjects had poor quality of diet. They are often challenged by multiple barriers to follow nutritional recommendations that differently affect each group of subjects depending on their problems, concerns and needs. Results of this study demonstrated the need for nutritional guidance and education in people with CKD, particularly in people receiving dialysis, who had the lowest quality of food consumption. In this regard, it is necessary to highlight the importance of nutritional education in CKD. Our findings showed that people with CKD, particularly in dialysis, believe they have a healthy diet, although the diet quality results show the opposite. This may be because patients and also health-care professionals may have an outdated view of what healthy eating is and their ideas may be contradictory to the modern approach of healthy eating in CKD, which is more personalized and less restrictive. People with CKD frequently faces low access to periodic nutritional counselling;22,23 additionally, there are a limited number of trained dietitians able to provide specialized treatment.24 Some studies have found that most people with CKD received insufficient nutritional information regarding food and fluid restrictions.9,17,25 Dietary restrictions limit the consumption of fruits, vegetables, legumes and seeds in people with CKD diet; making it one of the most difficult due to the numerous food restrictions.9,10 In a previous study, educational resources for people with CKD were analyzed, and 100% of them restricted fruits and vegetables for potassium control, while potassium additives available in ultra-processed foods were only restricted by 28%;26 this is disappointing as additives are highly bioavailable and, in consequence, have the greatest negative effect on serum potassium.27 These restrictions are contradictory to current advice and modern approaches, highlighting a clear need to change the perception about healthy eating on people with CKD and dietitians who prescribe these diets. A treatment with greater proximity in people with CKD, nutritional education from the early stages of the disease, self-awareness and up-to-date information can help to improve adherence.28 There is a need to focus dietary guidance and education on healthy foods, rather than isolated nutrients; release of some of these restrictions may help to motivate subjects to eat healthier because it was clear that people with CKD would like to eat healthy foods if guidance from health professionals, caregivers and handouts were easier to understand. All of these factors remark the need to eliminate misinformation that currently exists as well as having specialist renal dietitians supporting the correct messages.
Economic restriction was a significant obstacle to follow a healthy diet, many people with CKD cannot afford foods that are usually recommended by healthcare professionals. These findings were similar to the barriers found by Johnson A. et al in African American subjects with low socioeconomic status.29 In a personalized treatment, dietary recommendations should be adapted to the economic possibilities of the subjects, including regional and seasonal foods and preparations; this may help not only to significantly decrease economic costs but also increase the acceptability and palatability of the diet.30
On the other hand, a high proportion of people with CKD showed a willingness to improve their diet and nutrition, with the purpose of improving health and quality of life. A healthy diet has been shown to improve metabolic and cardiovascular conditions, improving quality of life and decreasing mortality in people with CKD.31,32 In a previous study, people receiving dialysis that reported willing to change negative dietary behaviors, had lower levels of potassium, phosphorous and better nutritional status compared to those who were unwilling to change.33
Perception of negative consequences of food consumption on people with CKD has been poorly explored. They believed that eating some healthy foods (fruits, vegetables or legumes) could cause some damage or negatively impact on disease control, such as increasing phosphorus, potassium or glucose levels. However, in previous studies, it has been shown that a healthy diet, rich in fruits, vegetables, and legumes is not associated with potassium levels or hyperkalemia risk in people with CKD.34–36 On the other hand, unhealthy, ultra processed foods, are high in potassium, sodium, phosphorus and sugars,37 increasing risk of disturbances to a larger extent than other natural foods.27,38 Furthermore, variability in CKD etiology and treatment (pharmacologic and dialysis) differs across CKD populations so the effect of potassium intake on serum levels is also variable.34 These different beliefs could be the result of multiple restrictions and complex messages in nutritional counseling; therefore, improving education handouts and focusing on benefits of healthy foods could help to improve knowledge and decrease associated “fears” to food.
Feelings and emotions about diet are mostly an unexplored theme in people with CKD. Although the fear of complications (on HD patients) due to non-adherence to nutritional recommendations, has been previously explored,9 other feelings such as guiltiness for eating, feeling of exclusion or difference from others, frustration and anger, yearning for foods, obligation to eat and desire to improve, have not been explored previously. Understanding people with CKD feelings, emotions and concerns across the stages of the disease, is a key point to improve adherence to nutritional treatment, however more research is needed in this regard. A personalized dietary intervention should consider emotional needs, since they play a two-way role with food.39 People with CKD mood can influence on food intake and choice, and vice versa; a good mood can lead the subject to eat healthy.40
It is well known that family and social support improves adherence as it works as a facilitator that motivates people to reach goals,41–43 therefore, including the family or primary caregivers in dietary counseling may facilitate dietary change. It is also well known that people tend to eat more when they are with family and friends than when they are eating alone, so not only the support, but also the presence of family and friends during mealtime can increase food intake.44
Regarding people with CKD environment, the lack of access to healthy food, combined with socioeconomic factors, leads to food insecurity, whose presence has been related in other studies to lower adherence to treatments and diet.45,46 Lack of time and work were also factors in their environment that difficult a healthy eating, especially in those subjects with KT and in CKD stage 3–5, who had greater work activity; in addition, people receiving HD referred lack of time due to HD sessions and the transfer time to hospital, in concordance with previous reports.47 On the other hand, family role models and previous personal patterns (healthy nutritional habits) positively influence eating habits from early stages (childhood and adolescence), the attitude of subjects towards consuming fruits and vegetables can be determined by the attitudes of other family members.48
The novelty and strength of our study is that we not only evaluated barriers for adherence to a healthy diet, but also evaluated facilitators in different stages of CKD, which may open the door to further research to improve adherence to nutritional treatment.
This study has some limitations: due to its qualitative design, it depends on the skills of the researcher and the interviewers; however, all dietitians involved in the study were previously trained by experts’ researchers, to ensure the correctly application of the interviews and avoid bias influencing the subject’s responses. Another limitation of this study was the quality of the recordings in a hospital environment such as waiting rooms (for example, there were some interruptions due to noise unrelated to the interview or recording quality flaws). For this reason, the interviews were carefully obtained, confirming that they had the best possible audio quality, the best sound clarity and the less data lost. Finally, since our study includes mixed methods, our final sample size was 20 people per group; which was sufficient for qualitative analysis but limited the quantitative analysis, when groups were compared.
Conclusion
Multiple barriers and facilitators were common in people across the spectrum of CKD. Independently of the treatment, all subjects perceived that the economy, food taste/flavor and the relation of food intake with negative effects in disease control were the main barriers to eat a healthier diet. Even though dietary restrictions were perceived as important barriers, it was more frequently noticed in people with CKD 3–5, PD and KT than in HD. People receiving PD reported a low willingness to change as a barrier for a healthy diet contrarily than the others.
Facilitators to a healthy diet in all groups were mainly leaded by health care professional-related aspects, showing the need of dietitians with specialized training in nephrology, able to prescribe healthy diets with a modern approach (less restricted diet), implementing nutritional education and providing people with alternative food preparations and variety, according to economic and cultural available food. Considering the different needs and perceptions between people with CKD and RRT is of utmost importance to develop personalized intervention strategies to improve the diet adherence.
Data Sharing Statement
Data are available on request from the corresponding author.
Acknowledgments
We want to recognize the people who were present and collaborated during the completion of this research: Pilar Carolina Castro Mata, Saúl Rolón Neftalí Barbosa, Carolina García Ramírez and Nancy Gabriela Romero Ornelas.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted and agreed to be accountable for all aspects of the work.
Funding
The present study was funded by the Mexican Institute of Social Security, Priority Health Themes, Vulnerable Population and Emerging Themes 2023 (Application 2023-3-300). The funder had no role in the design, data collection, data analysis and reporting of this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization: WHO. Healthy diet. Available from:. https://www.who.int/news-room/fact-sheets/detail/healthy-diet.
2. Stevens PE, Ahmed SB, Carrero JJ; Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2024;105(4S):S117–S314. doi:10.1016/j.kint.2023.10.018
3. González-Ortiz A, Xu H, Avesani CM, et al. Plant-based diets, insulin sensitivity and inflammation in elderly men with chronic kidney disease. J Nephrol. 2020;33(5):1091–1101. doi:10.1007/s40620-020-00765-6
4. Carrero JJ, González-Ortiz A, Avesani CM, et al. Plant-based diets to manage the risks and complications of chronic kidney disease. Nat Rev Nephrol. 2020;16(9):525–542. doi:10.1038/s41581-020-0297-2
5. Quintela BCSF, Carioca AAF, De Oliveira JGR, Fraser SDS, Da Silva Junior GB. Dietary patterns and chronic kidney disease outcomes: a systematic review. Nephrology. 2021;26(7):603–612. doi:10.1111/nep.13883
6. Bach KE, Kelly JT, Palmer SC, Khalesi S, Strippoli GFM, Campbell KL. Healthy dietary patterns and incidence of CKD: a meta-analysis of cohort studies. CJASN. 2019;14(10):1441–1449. doi:10.2215/CJN.00530119
7. Ikizler TA, Burrowes JD, Byham-Gray LD, et al. KDOQI clinical practice guideline for nutrition in CKD: 2020 update. AJKD. 2020;76(3):S1–107. doi:10.1053/j.ajkd.2020.05.006
8. Saglimbene VM, Su G, Wong G, et al. Dietary intake in adults on hemodialysis compared with guideline recommendations. J Nephrol. 2021;34(6):1999–2007. doi:10.1007/s40620-020-00962-3
9. Okoyo Opiyo R, Nyawade SA, McCaul M, et al. Perceptions on adherence to dietary prescriptions for adults with chronic kidney disease on hemodialysis: a qualitative study. Diseases. 2020;8(3):29. doi:10.3390/diseases8030029
10. Pourafshar S, Sharma B, Kranz S, et al. Patterns of fruit and vegetable intake in adults with and without chronic kidney disease in the United States. J Ren Nutr. 2023;33(1):88–96. doi:10.1053/j.jrn.2022.06.007
11. Sullivan VK, Appel LJ, Anderson CAM, et al. Ultraprocessed foods and kidney disease progression, mortality, and cardiovascular disease risk in the CRIC study. AJKD. 2023;82(2):202–212. doi:10.1053/j.ajkd.2023.01.452
12. Osté MC, Duan MJ, Gomes-Neto AW, et al. Ultra-processed foods and risk of all-cause mortality in renal transplant recipients. AJCN. 2022;115(6):1646–1657. doi:10.1093/ajcn/nqac053
13. Cardol CK, Boslooper-Meulenbelt K, Van Middendorp H, Meuleman Y, Evers AWM, Van Dijk S. Psychosocial barriers and facilitators for adherence to a healthy lifestyle among patients with chronic kidney disease: a focus group study. BMC Nephrol. 2022;23(1):205. doi:10.1186/s12882-022-02837-0
14. Memory KE, Wilkinson TJ, Smith AC, Lightfoot CJ. A qualitative exploration of the facilitators and barriers to self-management in kidney transplant recipients. J Nephrol. 2022;35(7):1863–1872. doi:10.1007/s40620-022-01325-w
15. Escudero‐Lopez M, Martinez‐Andres M, Marcilla‐Toribio I, Moratalla‐Cebrian ML, Perez‐Moreno A, Bartolome‐Gutierrez R. Barriers and facilitators in self‐care and management of chronic kidney disease in dialysis patients: a systematic review of qualitative studies. J Clin Nurs. 2024;33:3815–3830. doi:10.1111/jocn.17193
16. Kistler B, Avesani CM, Burrowes JD, et al. Dietitians play a crucial and expanding role in renal nutrition and medical nutrition therapy. J Ren Nutr. 2024;34(2):91–94. doi:10.1053/j.jrn.2024.02.001
17. Tyson CC, Svetkey LP, Lin PH, et al. Self-perceived barriers and facilitators to dietary approaches to stop hypertension diet adherence among black americans with chronic kidney disease: a qualitative study. J Ren Nutr. 2023;33(1):59–68. doi:10.1053/j.jrn.2022.05.002
18. Meuleman Y, Ten Brinke L, Kwakernaak AJ, et al. Perceived barriers and support strategies for reducing sodium intake in patients with chronic kidney disease: a qualitative study. Int J Behav Med. 2015;22(4):530–539. doi:10.1007/s12529-014-9447-x
19. Moriana M, Civera M, Artero A, et al. Validez de la valoración subjetiva global como método de despistaje de desnutrición hospitalaria. Prevalencia de desnutrición en un hospital terciario. Endocrinología y Nutrición. 2014;61(4):184–189. doi:10.1016/j.endonu.2013.10.006
20. Bernal-Orozco MF, Salmeron-Curiel PB, Prado-Arriaga RJ, et al. Second version of a mini-survey to evaluate food intake quality (mini-ECCA v.2): reproducibility and ability to identify dietary patterns in university students. Nutrients. 2020;12(3):809. doi:10.3390/nu12030809
21. Li J, Guasch-Ferré M, Chung W, et al. The Mediterranean diet, plasma metabolome, and cardiovascular disease risk. Eur Heart J. 2020;41(28):2645–2656. doi:10.1093/eurheartj/ehaa209
22. Nerbass FB, Lima HDN, Vieira Neto OM, Sesso R, Lugon JR. Prevalence and determinants of predialysis dietitian follow-up: results from the Brazilian Dialysis Registry. J Ren Nutr. 2023;33(1):97–102. doi:10.1053/j.jrn.2022.04.005
23. Lee P, Kouba J, Jimenez EY, Kramer H. Medical nutrition therapy for chronic kidney disease: low access and utilization. AKDH. 2023;30(6):508–516. doi:10.1053/j.akdh.2023.12.001
24. Norouzi S, Liu KS, Bustamante E, et al. The kidney diet challenge: an experiential educational experience. Kidney 360. 2021;3(2):279–286. doi:10.34067/KID.0001162021
25. Palmer SC, Hanson CS, Craig JC, et al. Dietary and fluid restrictions in CKD: a thematic synthesis of patient views from qualitative studies. AJKD. 2015;65(4):559–573. doi:10.1053/j.ajkd.2014.09.012
26. Picard K, Griffiths M, Mager DR, Richard C. Handouts for low-potassium diets disproportionately restrict fruits and vegetables. J Ren Nutr. 2021;31(2):210–214. doi:10.1053/j.jrn.2020.07.001
27. Picard K, Picard C, Mager DR, Richard C. Potassium content of the American food supply and implications for the management of hyperkalemia in dialysis: an analysis of the branded product database. Semin Dial. 2024;37(4):307–316. doi:10.1111/sdi.13007
28. Warner MM, Tong A, Campbell KL, Kelly JT. Patients’ experiences and perspectives of telehealth coaching with a dietitian to improve diet quality in chronic kidney disease: a qualitative interview study. JAND. 2019;119(8):1362–1374. doi:10.1016/j.jand.2019.01.023
29. Johnson AE, Boulware LE, Anderson CA, et al. Perceived barriers and facilitators of using dietary modification for CKD prevention among African Americans of low socioeconomic status: a qualitative study. BMC Nephrol. 2014;15(1):194. doi:10.1186/1471-2369-15-194
30. Shafiee M, Al-Bazz S, Lane G, Szafron M, Vatanparast H. Exploring healthy eating perceptions, barriers, and facilitators among urban indigenous peoples in Saskatchewan. Nutrients. 2024;16(13):2006. doi:10.3390/nu16132006
31. Floria I, Kontele I, Grammatikopoulou MG, Sergentanis TN, Vassilakou T. Quality of life of hemodialysis patients in Greece: associations with socio-economic, anthropometric and nutritional Factors. IJERPH. 2022;19(22):15389. doi:10.3390/ijerph192215389
32. Kelly JT, Palmer SC, Wai SN, et al. Healthy dietary patterns and risk of mortality and ESRD in CKD: a meta-analysis of cohort studies. CJASN. 2017;12(2):272–279. doi:10.2215/CJN.06190616
33. Orozco-González CN, Cortés-Sanabria L, Márquez-Herrera RM, et al. Willingness to change diet and exercise behavior is associated with better lifestyle in dialysis patients close to a kidney transplant. Clin Nutr ESPEN. 2022;47:277–282. doi:10.1016/j.clnesp.2021.11.032
34. Picard K, Barreto Silva MI, Mager D, Richard C. Dietary potassium intake and risk of chronic kidney disease progression in predialysis patients with chronic kidney disease: a systematic review. Adv Nutr. 2020;11(4):1002–1015. doi:10.1093/advances/nmaa027
35. Ramos CI, González-Ortiz A, Espinosa-Cuevas A, Avesani CM, Carrero JJ, Cuppari L. Does dietary potassium intake associate with hyperkalemia in patients with chronic kidney disease? NDT. 2021;36(11):2049–2057. doi:10.1093/ndt/gfaa232
36. Pan J, Xu X, Wang Z, Ma T, Dong J. Dietary potassium and clinical outcomes among patients on peritoneal dialysis. Nutrients. 2023;15(19):4271. doi:10.3390/nu15194271
37. Uribarri J. Phosphorus metabolism and management in chronic kidney disease: phosphorus homeostasis in normal health and in chronic kidney disease patients with special emphasis on dietary phosphorus intake. Semin Dial. 2007;20(4):295–301. doi:10.1111/j.1525-139X.2007.00309.x
38. Waheed AA, Pedraza F, Lenz O, Isakova T. Phosphate control in end-stage renal disease: barriers and opportunities. NDT. 2013;28(12):2961–2968. doi:10.1093/ndt/gft244
39. Macht M. How emotions affect eating: a five-way model. Appetite. 2008;50(1):1–11. doi:10.1016/j.appet.2007.07.002
40. AlAmmar WA, Albeesh FH, Khattab RY. Food and mood: the corresponsive effect. Curr Nutr Rep. 2020;9(3):296–308. doi:10.1007/s13668-020-00331-3
41. Pesantes MA, Del Valle A, Diez-Canseco F, et al. Family support and diabetes: patient’s experiences from a public hospital in Peru. Qual Health Res. 2018;28(12):1871–1882. doi:10.1177/1049732318
42. Gomes LC, Coelho ACM, Gomides DDS, Foss-Freitas MC, Foss MC, Pace AE. Contribution of family social support to the metabolic control of people with diabetes mellitus: a randomized controlled clinical trial. Appl Nurs Res. 2017;36:68–76. doi:10.1016/j.apnr.2017.05.009
43. Wickrama KAS, Ralston PA, O’Neal CW, et al. Life dissatisfaction and eating behaviors among older African Americans: the protective role of social support. J Nutr Health Aging. 2012;16(9):749–753. doi:10.1007/s12603-012-0404-6
44. Ruddock HK, Brunstrom JM, Higgs S. The social facilitation of eating: why does the mere presence of others cause an increase in energy intake? Physiol Behav. 2021;240:113539. doi:10.1016/j.physbeh.2021.113539
45. Andersen CC, Cabeza De Baca T, Votruba SB, et al. Food insecurity moderates the relationship between momentary affect and adherence in a dietary intervention study. Obesity. 2022;30(2):369–377. doi:10.1002/oby.23335
46. Heerman WJ, Wallston KA, Osborn CY, et al. Food insecurity is associated with diabetes self‐care behaviours and glycaemic control. Diabet Med. 2016;33(6):844–850. doi:10.1111/dme.12896
47. Griva K, Ng HJ, Loei J, Mooppil N, McBain H, Newman SP. Managing treatment for end-stage renal disease – a qualitative study exploring cultural perspectives on facilitators and barriers to treatment adherence. Psychol Health. 2013;28(1):13–29. doi:10.1080/08870446.2012.703670
48. Christiansen KMH, Qureshi F, Schaible A, Park S, Gittelsohn J. Environmental factors that impact the eating behaviors of low-income African American Adolescents in Baltimore City. JNEB. 2013;45(6):652–660. doi:10.1016/j.jneb.2013.05.009
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.