")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 18
Basal Cell Carcinoma Arising Within a Favre-Racouchot Syndrome Lesion: A Rare Case and Literature Review
Authors Li H, Li S, Dong T, Liu J, Sun Y
Received 7 April 2025
Accepted for publication 30 June 2025
Published 9 July 2025 Volume 2025:18 Pages 1703—1708
DOI https://doi.org/10.2147/CCID.S531359
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Michela Starace
Hui Li, Shuhua Li, Tiantian Dong, Jun Liu, Yi Sun
Dermatology and Plastic-Cosmetic Medical Center, Weifang People’s Hospital, the First Affiliated Hospital of Shandong Second Medical University, Weifang, Shandong, People’s Republic of China
Correspondence: Yi Sun, Dermatology and Plastic-Cosmetic Medical Center, the First Affiliated Hospital of Shandong Second Medical University, 151 Guangwen Street, Weifang, Shandong, 261041, People’s Republic of China, Tel +86-0536-8192561, Email [email protected]
Abstract: Concurrence of Favre-Racouchot syndrome (FRS), a chronic dermatosis, and skin cancer is rare. In this study, we present an exceptionally rare case of basal cell carcinoma (BCC) arising within a FRS lesion. An 84-year-old female farmer had a mass in the lower left limb for 30 years without medical treatment. Over the past year, especially in the month prior to this visit, the mass enlarged significantly. On examination, a well-defined, rounded mass measuring approximately 4 cm in diameter was noted on the anterior aspect of the left calf. The mass had a rough surface with papillary hyperplasia and a mild erythema at the base. Open and closed comedones were observed, but no cysts or yellowish nodules were present. Histopathological analysis showed degradation and reduction of elastic fibers in the lesion dermis, along with the presence of comedones and cysts. Furthermore, scattered basaloid cell nests of varying sizes were present in the dermis, with peripheral tumor cells arranged in a palisading pattern. Peritumoral clefts were observed and the cell nuclei were hyperchromatic and occupied most of the cell. BCC associated with FRS was diagnosed. The patient underwent complete surgical excision. No recurrence was observed over an 18-month follow-up period. In conclusion, concurrence of BCC and FRS is rare. Delayed diagnosis of this condition can lead to more invasive disease progression. To improve early detection for timely treatment, clinicians should maintain a high index of suspicion for malignant transformation in patients with longstanding FRS, particularly those presenting with rapidly evolving lesions.
Keywords: Favre-Racouchot syndrome, malignant transformation, basal cell carcinoma, elastosis, comedone, cyst, cell atypia
Key Points
- An exceptionally rare case of basal cell carcinoma arising within a Favre-Racouchot syndrome (FRS) lesion was reported.
- The lesion had typical FRS histopathological features: degradation and reduction of elastic fibers, along with the presence of comedones and cysts. Additionally, scattered basaloid cell nests of varying sizes with peripheral cells arranged in a palisading pattern and cell atypia were observed in the dermis.
- Delayed diagnosis of the condition can lead to more invasive disease progression. To improve early detection for timely treatment, clinicians should maintain a high index of suspicion for malignant transformation in patients with longstanding FRS, particularly those presenting with rapidly evolving lesions.
Introduction
Favre-Racouchot syndrome (FRS) is a chronic dermatological condition characterized by elastosis, along with the presence of comedones and cysts; it primarily affects elderly Caucasian men with long-term sun exposure, with an estimated prevalence of 6% in individuals over 50 years of age.1,2 FRS predominantly affects the face, with involvement of the extremities being extremely rare. It is typically managed with topical retinoids, manual comedone extraction, or laser therapy.1 Basal cell carcinoma (BCC) is the most common type of skin cancer, arising from the basal layer of the epidermis. It occurs mostly in chronically sun-exposed areas of the skin, with over 90% of lesions found on the head, neck, and trunk, and approximately 5% on the upper and lower extremities.3,4
Co-existence of FRS and skin cancer has been rarely documented. Two recent case reports described skin squamous cell carcinoma (SCC) associated with FRS.5,6 A search of PubMed, Scopus, and Google Scholar databases using the keywords “Favre-Racouchot syndrome”, “Favre-Racouchot disease”, “Favre-Racouchot syndrome and basal cell carcinoma”, or “Favre-Racouchot disease and basal cell carcinoma” identified only one published case report on BCC associated with FRS.7 In this study, we present another case of BCC arising within a FRS lesion in the lower extremity.
Case Report
The informed consent was obtained from the patient. An 84-year-old female farmer presented to our department in August 2023 with a rapidly enlarging mass on her left lower leg over the past month. The lesion started as a pea-sized brown papule 30 years ago. Over the past year, especially in the month prior to this visit, the mass enlarged significantly. The patient was previously in good health, with no history of smoking or known comorbidities, and had not received any treatment prior to presenting to our department. Physical examination revealed a well-defined, rounded mass measuring approximately 4 cm in diameter on the anterior aspect of the left calf. The surface was irregular and covered by dark to dark red crusts with papillary hyperplasia and mild erythema at its base (Figure 1a). Open and closed comedones were observed, but no cysts or yellowish nodules were present (Figure 1b). No superficial lymphadenopathy was detected. Cardiac, pulmonary, and abdominal examinations had no significant abnormalities.
 |
Figure 1 Clinical presentation and histopathological findings. (a) shows the lesion on the lower left limb. The mass had a rough, dark or dark red surface with papillary hyperplasia, and a mild erythema was observed at the base. Comedones were present in the lesion, indicated by arrows in (b). Histopathological analysis using Verhoeff’s Van Gieson staining showed degradation and reduction of elastic fibers in the dermis of the lesion (inside the right oval of (c)), compared to the normal skin area (inside the left oval), where the elastic fibers were stained dark or dark blue. A comedone (the red arrow in (c)) and cysts (black arrows in (c)) were also observed. |
Routine blood and urine analyses, liver and kidney function tests, chest X-ray, and abdominal ultrasound results were all normal. Histopathological analysis showed epidermal atrophy, and a reduction and degradation of elastic fibers in dermis, along with the presence of cysts and comedones (Figure 1c). These are typical features of FRS. Furthermore, scattered basaloid cell nests of varying sizes were present in the dermis (Figure 2a), focally distributed and connected to the epidermis. The peripheral tumor cells were arranged in a palisading pattern (Figure 2b). Peritumoral clefts were observed, and the tumor cell nuclei were hyperchromatic, occupying most of the cell (Figure 2c). These findings are consistent with superficial BCC.
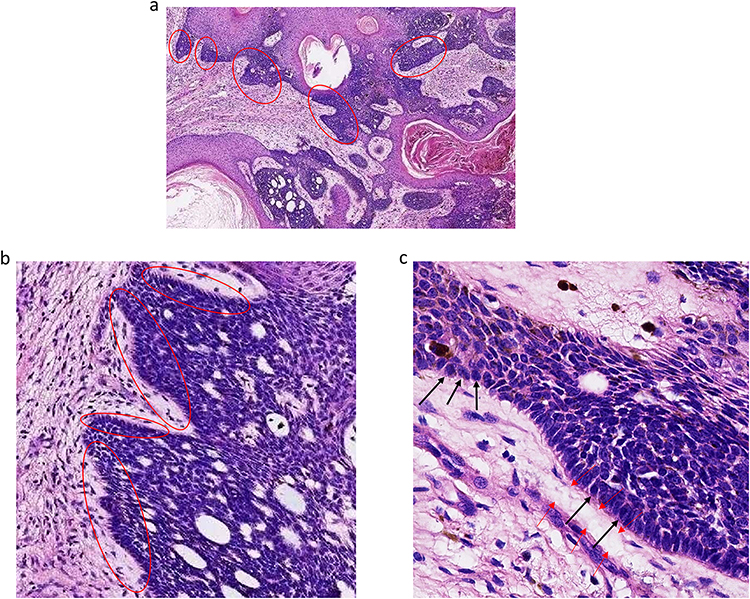 |
Figure 2 Histopathological findings revealed by H&E staining. As shown in (a), scattered basaloid cell nests of varying sizes (dark blue stained, inside the ovals) were present in the dermis, focally distributed and connected to the epidermis. Tumor cells at the periphery of the nests were arranged in a palisading pattern (inside the ovals in (b)). The tumor cell nuclei were stained dark blue (hyperchromatic) and occupied most of the cell, as indicated by the black arrows in (c). A peritumoral cleft is indicated by the red arrows (c). |
Based on the clinical manifestations and histopathological findings, BCC associated with FRS was diagnosed. The patient underwent complete surgical excision. No recurrence was observed over an 18-month follow-up period.
Discussion
Although FRS occurs predominantly in the Caucasian population,1,2 cases in other ethnicities have also been reported.8–11 In this study, we present a case of FRS in an elderly Chinese female farmer. Of note, the location of the lesion in our case is atypical for FRS, which primarily affects the face.1 However, extrafacial lesions, such as those on the forearms and trunk, have been documented.12,13 Our case provides additional evidence that FRS can present outside the facial region.
In the present study, we observed comedones but no cysts in the lesion on physical examination. Additionally, the lesion appeared dark red or dark upon presentation to our department, although the patient reported it was initially brown. Of note, these features closely align with those described in a previously published case report of BCC secondary to FRS.7 Khouna et al observed a pink-colored lesion with visible comedones but no cysts on physical examination.7 We speculate that the absence of cysts and the change in lesion color may be attributable to the presence of BCC. Nevertheless, the histopathological findings and differential diagnosis support a primary diagnosis of FRS.
FRS should be differentiated from other conditions with similar clinical features, most notably acne vulgaris and BCC. Acne vulgaris primarily affects adolescents and is typically localized to the face,14 in sharp contrast to our case. To provide a broader clinical context, it is worth noting that acne vulgaris also presents with comedones, cysts, and nodular lesions, often accompanied by significant inflammation, but is rarely associated with skin atrophy or elastosis.14–16 FRS can resemble nodular BCC, but BCC typically grows faster than FRS lesions.3 Although concurrent BCC was diagnosed in the present case, the lesion had a long history and evolved rapidly in the past year. In view of this, we considered the BCC as a secondary development, likely resulting from malignant transformation within the pre-existing FRS lesions, rather than being the primary condition. Other skin lesions to consider in the differential diagnosis of our case include infundibulocystic squamous cell carcinoma (infundibulocystic SCC), seborrhoeic keratosis and adnexal tumors. Infundibulocystic SCC arises from the follicular infundibulum and typically exhibits rapid growth (>1 cm/year),17,18 characteristics that argue against a diagnosis of FRS in our patient, whose lesion gradually developed into a 4 cm mass over a 30-year period. For the differential diagnosis between infundibulocystic SCC and BCC, key histological features include the presence of abundant eosinophilic cytoplasm and intercellular bridges in infundibulocystic SCC,17,18 in contrast to the scant cytoplasm and peripheral palisading of basophilic cells characteristic of BCC shown in our case. Additionally, infundibulocystic SCC lacks the peritumoral clefts, a distinctive feature of BCC.19 Seborrhoeic keratosis may exhibit comedo-like openings and milia-like cysts,20 which can resemble the features of Favre-Racouchot syndrome (FRS), potentially leading to misdiagnosis. However, acanthosis, papillomatosis, and pseudohorn cysts, the most common histopathologic features of seborrhoeic keratosis,20 were absent in our case. Proliferation of basaloid cells, as seen in seborrhoeic keratosis, may be mistaken for BCC; however, it is accompanied by squamous cell proliferation and lacks the peripheral palisading and peritumoral clefts that are characteristic features of BCC, as observed in our patient. Skin adnexal tumors (SATs) are a large and diverse group of benign and malignant neoplasms originating from hair follicles, sebaceous glands, eccrine sweat glands, and apocrine glands.21 Some benign skin adnexal tumors (SATs) may share one or two features with Favre-Racouchot syndrome (FRS);21 however, they typically lack solar elastosis. Histologically, SATs show pathological changes in adnexal structures,21 which are distinct from those seen in FRS. Basaloid epidermal proliferations in SATs also lack peripheral palisading and peritumoral clefts, features that aid in distinguishing them from BCC.
Major risk factors for FRS include chronic sun exposure, cigarette smoking, and radiation therapy.1,2 The patient we treated did not smoke and had no history of radiation therapy. Therefore, long-term occupational sun exposure appears to be the primary contributor to the lesion. Concurrence of FRS and skin malignancies has been rarely reported. Krajewski et al described a case of FRS co-existing with SCC in a 70-year-old Caucasian male farmer. The patient had multiple FRS lesions on the cheeks, lower lip and nose. Histopathological examination of the nose biopsy confirmed SCC.5 Another study reported SCC originating within FRS lesions in two immunocompromised Caucasian individuals: an 80-year-old woman who took immunosuppressive drugs for rheumatoid arthritis and a 70-year-old man with a history of chronic lymphatic leukemia.6 Both patients had FRS lesions unilaterally in the right temporal area associated with SCC confirmed by histopathological analysis. In a previously published case study of BCC arising within FRS, the patient was also elderly, at 63 years of age.7 Immunity declines with age in elderly individuals, which may contribute to the concurrence of FRS and skin cancers, including SCC and BCC. Sun exposure is a major risk factor for FRS, SCC and BCC. Paradoxically, a few studies suggested a potential protective role of solar elastosis against malignant skin neoplasms.22,23 How skin cancers develop within FRS lesions remains to be fully explored.
The standard treatment for BCC involves complete removal of the lesion by excision or Mohs surgery.3,4 Our patient underwent complete excision, leading to a satisfactory outcome without recurrence over an follow-up period of 18 months. Although the absence of a post-excision image may be considered a limitation of this study, the histopathological findings clearly demonstrated the diagnostic features of BCC associated with FRS. Furthermore, standard surgical treatment was performed, and follow-up findings reflected a favorable outcome. Another limitation is that mucin within the clefts was not analyzed using mucin-specific staining; however, this would not affect the diagnosis of BCC.
Conclusion
Concurrence of BCC and FRS is rare. Delayed diagnosis of this condition can lead to more invasive disease progression. To improve early detection for timely treatment, dermatologists and clinicians should maintain a high index of suspicion for malignant transformation in patients with longstanding FRS, particularly those presenting with rapidly evolving lesions.
Data Sharing Statement
All data are included in the article.
Ethical Approval and Statement
Ethical approval was not required for this case report as the patient is de-identified. Informed consent was obtained from the patient.
Consent for Publication
Informed consent for publication was obtained from the patient.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Paganelli A, Mandel VD, Kaleci S, Pellacani G, Rossi E. Favre-Racouchot disease: systematic review and possible therapeutic strategies. J Eur Acad Dermatol Venereol. 2019;33(1):32–41. doi:10.1111/jdv.15184
2. Kaya TI, Tursen U, Yazici AC, Ikizoglu G. A simple open comedone extraction technique for Favre-Racouchot disease. Photodermatol Photoimmunol Photomed. 2005;21(5):275–277. doi:10.1111/j.1600-0781.2005.00165.x
3. Naik PP, Desai MB. Basal cell carcinoma: a narrative review on contemporary diagnosis and management. Oncol Ther. 2022;10(2):317–335. doi:10.1007/s40487-022-00201-8
4. Hoellwerth M, Brandlmaier M, Koelblinger P. Therapeutic approaches for advanced basal cell carcinoma: a comprehensive review. Cancers. 2024;17(1):68. doi:10.3390/cancers17010068
5. Krajewski PK, Chlebicka I, Stefaniak AA, Szepietowski JC. Coexistence of Favre-Racouchot disease, cutis rhomboidalis nuchae and skin neoplasms. Postepy Dermatol Alergol. 2021;38(5):906–908. doi:10.5114/ada.2020.95605
6. Leeuwis-Fedorovich NE, Starink M, van der Wal AC. Multifocal squamous cell carcinoma arising in a Favre-Racouchot lesion - report of two cases and review of the literature. J Dermatol Case Rep. 2015;9(4):103–106. doi:10.3315/jdcr.2015.1215
7. Khouna A, Zerrouki N, Dikhaye S, et al. An unusual association of Favre and Racouchot Syndrome with basal cell carcinomas of the face. J Med - Clin Res & Rev. 2018;2(6):1–2. doi:10.33425/2639-944X.1069
8. Wei Z, Wang F, Zheng S. Favre-Racouchot Syndrome. JAMA Dermatol. 2024;160(4):462–463. doi:10.1001/jamadermatol.2023.5768
9. Kakhandaki AA, Raveendra L, Venkataramana PA, Khandre JS. Favre-racouchot syndrome with bilateral mechanical ptosis: an unusual presentation. J Cutan Aesthet Surg. 2014;7(2):135–136. doi:10.4103/0974-2077.138366
10. Zheng LQ, Han XC, Huang Y, Li HW, Niu XD. Favre-Racouchot syndrome concurrent with chronic granulomatous reaction. J Dermatol. 2014;41(7):642–644. doi:10.1111/1346-8138.12467
11. Zhang R, Zhu W. Favre-Racouchot syndrome associated with eyelid papilloma: a case report. J Biomed Res. 2012;26(6):474–477. doi:10.7555/JBR.26.20110093
12. Cardoso F, Nakandakari S, Zattar GA, Soares CT. Actinic comedonal plaque-variant of Favre-Racouchot syndrome: report of two cases. An Bras Dermatol. 2015;90(3 Suppl 1):185–187. doi:10.1590/abd1806-4841.20153543
13. John SM, Hamm H. Actinic comedonal plaque-a rare ectopic form of the Favre-Racouchot syndrome. Clin Exp Dermatol. 1993;18(3):256–258. doi:10.1111/j.1365-2230.1993.tb02181.x
14. Rao A, Douglas SC, Hall JM. Endocrine disrupting chemicals, hormone receptors, and acne vulgaris: a connecting hypothesis. Cells. 2021;10(6):1439. doi:10.3390/cells10061439
15. Eichenfield DZ, Sprague J, Eichenfield LF. Management of acne vulgaris: a review. JAMA. 2021;326(20):2055–2067. doi:10.1001/jama.2021.17633
16. Layton AM, Morris C, Cunliffe WJ, Ingham E. Immunohistochemical investigation of evolving inflammation in lesions of acne vulgaris. Exp Dermatol. 1998;7(4):191–197. doi:10.1111/j.1600-0625.1998.tb00323.x
17. Kim SM, Kim H, Kim HS, Cho SH, Lee JD. Infundibulocystic squamous cell carcinoma. Ann Dermatol. 2015;27(3):319–321. doi:10.5021/ad.2015.27.3.319
18. Hasegawa T, Iino S, Sekine S, et al. An aggressive case of infundibulocystic squamous cell carcinoma on the upper lip: a hybrid pathology of well-differentiated and infiltrative variants. Dermatol Pract Concept. 2023;13(4):e2023254. doi:10.5826/dpc.1304a254
19. Niculet E, Bobeica C, Craescu M, et al. Multimodal considerations concerning basal cell carcinoma clefting - profile of structural and aggressive traits - perspectives. Clin Cosmet Investig Dermatol. 2022;15:2087–2095. doi:10.2147/CCID.S385213
20. Moscarella E, Brancaccio G, Briatico G, Ronchi A, Piana S, Argenziano G. Differential diagnosis and management on seborrheic keratosis in elderly patients. Clin Cosmet Investig Dermatol. 2021;14:395–406. doi:10.2147/CCID.S267246
21. Płachta I, Kleibert M, Czarnecka AM, Spałek M, Szumera-Ciećkiewicz A, Rutkowski P. Current diagnosis and treatment options for cutaneous adnexal neoplasms with follicular differentiation. Int J Mol Sci. 2021;22(9):4759. doi:10.3390/ijms22094759
22. Yeh C, Schwartz RA. Favre-Racouchot disease: protective effect of solar elastosis. Arch Dermatol Res. 2022;314(3):217–222. doi:10.1007/s00403-021-02202-5
23. Walther U, Kron M, Sander S, et al. Risk and protective factors for sporadic basal cell carcinoma: results of a two-centre case-control study in southern Germany. Clinical actinic elastosis may be a protective factor. Br J Dermatol. 2004;151(1):170–178. doi:10.1111/j.1365-2133.2004.06030.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.