")
Back to Journals » Nature and Science of Sleep » Volume 17
Bidirectional causal associations between frailty measures and sleep disturbances: a two-sample Mendelian randomization study
Authors Che L , Zang H, Bi Y, Wen B , Xu L
Received 20 September 2024
Accepted for publication 19 January 2025
Published 7 February 2025 Volume 2025:17 Pages 271—284
DOI https://doi.org/10.2147/NSS.S497173
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Lu Che,* Han Zang,* Yaodan Bi, Bei Wen, Li Xu
Department of Anesthesiology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, 100730, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Li Xu, Email [email protected]
Background: Observational studies have demonstrated a strong association between sleep disturbances and frailty. However, the causality remains inconclusive. We aimed to investigate the bidirectional causal relationships between frailty measures and sleep disturbances employing a two-sample Mendelian randomization (MR) analysis.
Methods: Two-sample MR analyses were performed based on large-scale genome-wide association studies (GWAS) of the European population for frailty index (FI) (N = 175,226), Fried Frailty Score (FFS) (N = 386,565), insomnia (N = 283,595), sleep duration (N = 445,966) and sleep apnea (N = 523,366). We conducted the causal estimates using the inverse variance-weighted method (IVW), with sensitivity analyses using MR-Egger, weighted median, weighted mode, and MR pleiotropy residual sum and outlier (MR-PRESSO) analysis. Cochran’s Q test was performed to assess heterogeneity.
Results: We found that genetically predicted FI was associated with shorter sleep duration and sleep apnea. The genetically predicted FFS was associated with insomnia, shorter sleep duration, and sleep apnea. In the reverse direction analysis, genetic liability to insomnia, short sleep duration, and long sleep duration were associated with an increase in FI. Genetic liability to short sleep duration and long sleep duration were associated with an increase in FFS.
Conclusion: Our study provided genetic evidence supporting the bidirectional causality between frailty measures and sleep disturbances. The findings contribute to the prevention and management of frailty and sleep disturbances.
Keywords: frailty, sleep disturbances, Mendelian randomization, the elderly
Introduction
Frailty, characterized by increased vulnerability resulting from age-related declines in reserve and function across multiple physiological domains, has emerged as a global health concern in the aging world population.1,2 Older people with frailty have an increased risk of fall, hospitalization, disability, and mortality.3–5 The frailty index (FI) and Fried Frailty Score (FFS) are two commonly used tools to comprehensively assess frailty.6,7 The FI quantifies frailty by considering a range of health-related deficits and capturing the cumulative impact of various physiological and clinical markers. FFS evaluates frailty based on specific criteria, including unintentional weight loss, exhaustion, low physical activity, slow walking speed, and diminished grip strength. Besides, sleep disorders pose a significant health challenge among the elderly. With sleep disruption often regarded as a common feature of “normal aging”, older adults frequently experience reduced ability to initiate and maintain sleep, along with deficits in sleep physiology.8 Similar to frailty, there exists substantial individual variability in sleep disturbances among older adults, indicating that not all individuals of the same chronological age suffer from similar degrees of sleep impairment.8
Sleep deprivation and loss impair physical performance, cognitive condition, and emotional well-being, thereby resulting in symptoms such as fatigue, which play an important role in frailty.9 Furthermore, poor sleep quality has been shown to be associated with increased systemic inflammation, leading to downstream consequences affecting various bodily functions, including endocrine, cardiovascular, and cognitive changes, thereby increasing the risk of frailty.10–14 Shared underlying pathophysiological pathways, such as inflammation and neurohormonal imbalance, may contribute to both frailty and sleep disorders. A recent systematic meta-analysis has identified 12 observational studies that demonstrated a significant association between insomnia and frailty in the older population.15 Meanwhile, a cross-sectional observational study suggested frailty was independently predicted by insomnia in older adults, adjusting for sociodemographic characteristics and comorbidity.16 Another meta-analysis examined that longer and shorter sleep duration were associated with increased risk of frailty.17 However, the causal associations between sleep disturbances and frailty remained inconclusive, because existing evidence from observational studies limited our understanding of the causal relationships and residual confounding factors.18,19 The issues of reverse causation and the possibility of bidirectional associations are not well established.20 Thus, it is difficult to identify the elaborate associations between sleep disturbances and frailty to improve individual management for the elderly population.
Randomized controlled trial (RCT) is regarded as the gold standard method to infer causality. However, RCT is expensive, time-consuming, and often limited to conduct, especially for investigations on sleep. To address the challenges of causal inference in this complex relationship, Mendelian randomization (MR) has emerged as a popular tool.21 MR uses genetic variants that are robustly associated with exposure as potentially unconfounded instruments to infer whether an observed association between the exposure and the outcome is causal or not from observational data. It becomes a faster, cheaper, and more feasible way to estimate the causal impact of the exposure on the outcome while diminishing limitations of conventional observational studies and RCTs, including confounding factors and reverse causation.
The main limitation of previous research was the measurement of frailty. Several definitions of the frailty syndrome have been proposed; however, current studies only examined the relationship using the FI.22,23 The FFS focuses on physical frailty, which differs from the FI comprising a series of health-related issues.24 In this study, we performed a bidirectional, two-sample MR to explore the causal relationships between frailty measures and sleep disturbances, as measured by the FI and FFS for more convincing and comprehensive conclusions.
Methods
Study Design Overview
We performed a bidirectional two-sample MR analysis to investigate the causal relationships between frailty measures and sleep disturbances (Figure 1). Our study was conducted in accordance with the Declaration of Helsinki revised in 2013, and the methods followed the STROBE-MR checklist.25,26 The study has been approved by the Institutional Review Board of the Peking Union Medical College Hospital (Ethics Approval Number: I-24ZM0035). As our MR study was based on publicly available summary statistics, the informed consent was found in the original studies.
 |
Figure 1 Overview of the MR study estimating the bidirectional association between frailty measures and sleep disturbances. Abbreviations: SNPs, single nucleotide polymorphisms; FI, frailty index; FFS, Fried Frailty Score. |
Data Sources
We extracted summary statistics on frailty measured by the FI from a meta-analysis of GWAS conducted in the UK Biobank (n = 164,610, mean age 64.1 years [SD = 2.8], 51.3% were female) and the Swedish TwinGene cohort (n = 10,616, mean age 58.3 years [SD = 7.9], 52.5% were female), comprising 175,226 individuals of European descent.27 The FI was developed using self-reported questionnaire data, which included over 40 components covering various domains of mental and physical health, and has been validated as a reliable tool for measuring frailty.27–29 The items were detailed in the Supplementary Table S1.29 Many of the loci have been previously linked to some traits and diseases, including body mass index (BMI), smoking, depression, neuroticism, and cardiovascular disease, adding crucial evidence to support associations with frailty.30 Summary statistics for FFS, a validated and standardized definition of frailty phenotype, were obtained from a recent large-scale GWAS with 386,565 participants of European ancestry enrolled in the UK Biobank (mean age 57 years [SD = 8], 54% were female).31 Most loci have been identified in GWAS of various traits, such as obesity, cardiovascular disease, diabetes, and cancer, revealing confirmatory evidence for relationships between these loci with frailty.32–34 Summary data for GWAS of insomnia and sleep apnea were obtained from the GWAS catalog, including 283,595 and 523,366 European participants.35,36 Many loci have been associated with some traits, which increase the risk of sleep apnea, including BMI or adiposity, airway dimensions, and hearing impairment.37–39 The summary statistics for sleep duration, including short (≤ 5 h) and long (≥ 10 h) sleep duration, were retrieved from a GWAS and meta-analyses.40 Only data from European ancestry (N = 445,966) were used in this MR study, including 278,003 participants from UK Biobank (mean age 56.8 years [SD = 8.0], 54.1% were female) and 167,963 participants from the Million Veteran Programme (mean age 66.8 years [SD = 11.6], 7.4% were female). These genetic loci for short or long sleep duration have been related to sleep, cognitive, and psychiatric traits as well as other disorders in the previous GWAS.41,42 The genome-wide significance was P < 5 * 10−8.
Selection and Validation of Instrumental Variables
The genetic variants selected as instrumental variables (IVs) must follow three assumptions: (1) genetic variants are reliably associated with the risk factor under investigation (relevance assumption); (2) genetic variants are not associated with any known or unknown confounding factor (independence assumption); (3) genetic variants influence the outcome only through the risk factor and not through any causal pathway (exclusion restriction assumption).43 To satisfy the relevance assumption, single nucleotide polymorphisms (SNPs) that met a significance threshold of P < 5 * 10−8 were selected as IVs, but long sleep duration in which only two SNPs reached the threshold and the significance threshold was set as P < 5 * 10−6 to obtain a more comprehensive result as previously reported.44,45 To meet the independence assumption, we identified potential confounders through the PhenoScanner Database (http://www.phenoscanner.medschal.cam.ac.uk/). Besides, to ensure variable independence and account for linkage disequilibrium (LD) effects, an LD parameter (r2) of 0.001 and a genetic distance of 10000 kb were utilized. For the exclusion restriction assumption, the selected SNPs related to outcome with P < 5 * 10−5 were removed from the IVs. Moreover, we removed palindromic SNPs from the instrumental SNPs chosen for analysis in the harmonization process. Regarding the strength of the IVs, the F statistic (F = β2/se2) was employed to exclude weak instrumental biases and ensure the instrumental strength. The SNPs with F statistic < 10 indicating a weak association were excluded from the MR analysis46 In addition, the R2-value (the proportion of variation explained by the genetic variant) of each genetic instrument was also calculated to ensure that the eligible SNPs were strong instruments.
Statistical Analysis for MR
Statistical analysis in this study was performed using R Software (version 4.3.3) through TwoSampleMR (version 0.5.11), MendelianRandomization (version 0.8.0), and MRPRESSO package (version 1.0). The primary analysis method employed was the inverse variance-weighted (IVW) approach.47 Additionally, MR Egger, weighted median, and weighted mode methods were utilized as complementary analyses.48–50 The estimates were reported as odds ratios (ORs) along with their corresponding 95% confidence intervals (CIs). Cochran’s Q test was performed to assess heterogeneity among individual causal effects, with significance defined as P < 0.05, indicating heterogeneity.51 We identified exposures with horizontal pleiotropy for MR-Egger regression and MR pleiotropy residual sum and outlier (MR-PRESSO) global test.49,52 Furthermore, scatterplots were employed to evaluate the robustness and stability, and leave-one-out analysis was conducted to indicate that the causal effect of exposure on outcome was not influenced by individual SNPs. If one or more outlier SNPs were found to affect the MR estimates, they were removed and MR analysis was performed again. The variables in our study were not independent; therefore, multiple testing adjustment was not applied in the MR analysis.
Results
To ensure that the samples for exposures were independent of those for outcomes, we manually reviewed the sample descriptions of each GWAS. Besides sleep duration, there was no sample overlap between the data of the frailty measures and other sleep disturbances. We conducted simulation studies to explore the potential impact of sample overlap on causal estimates as previously reported.53 The simulation studies indicated that while overlap could introduce bias, the effect size and direction in our analysis were unlikely to be substantially affected, with bias estimated to be less than 5%. Detailed information on SNPs used for our analyses is presented in the Supplementary Tables S2–S17. The F statistics of all SNPs were more than 10, and it meant there were no weak IVs. The results of leave-one-out sensitivity analysis, forest plot, scatter plot, and funnel plot were shown in Supplementary Figures S1–S16.
Causal Effects of Frailty measures on Sleep Disturbances
For the effect of FI on insomnia, it demonstrated that the genetic predisposition to FI was statistically significantly associated with increased risk of insomnia (OR 1.21, 95% CI: 1.10, 1.32, P < 0.001). It indicated that one standard deviation increase in quantile-normalized FI could elevate the risk of insomnia by 21%. However, the results of MR-Egger and weighted mode showed that FI was not related to the risk of insomnia (Figure 2). Heterogeneity among SNPs was detected by the Cochran’s Q test (Q = 28.364, P = 0.003). The results of the MR-PRESSO test revealed that IVs of FI and insomnia had horizontal pleiotropy after the removal of outlier SNPs (MR-PRESSO: P = 0.008), however, the MR-Egger regression did not find the presence of pleiotropy (MR-Egger intercept: P = 0.085) (Table 1). For the effect of FFS on insomnia, the IVW analysis suggested that the genetic predisposition to FFS was statistically significantly associated with insomnia (OR 1.28, 95% CI: 1.18, 1.38, P < 0.001). It revealed that one standard deviation increase in quantile-normalized FFS could elevate the risk of insomnia by 28%. The weighted median and weighted mode methods were consistent with this result. However, the MR-Egger method showed no evidence of a causal association between FFS and insomnia (OR 1.32, 95% CI: 0.99, 1.75, P = 0.072) (Figure 2). In addition, there was no heterogeneity by the Cochran’s Q test (Q = 30.104, P = 0.146). The MR-Egger regression and MR-PRESSO test did not detect any pleiotropy (MR-Egger intercept: P = 0.821; MR-PRESSO: P = 0.191) (Table 1).
 |
Table 1 The Causal Estimates Between Frailty Measures and Sleep Disturbances in the Sensitivity Analysis |
 |
Figure 2 MR estimates for the causal effect of frailty measures on sleep disturbances. Abbreviations: FI, frailty index; FFS, Fried Frailty Score; SNPs, single nucleotide polymorphisms; IVW, inverse variance-weighted method; CI, confidence interval; OR, odds ratio. |
In the analysis of the effect of FI on short sleep duration, our study indicated a genetic predisposition to FI increased the risk of short sleep duration (OR 1.89, 95% CI: 1.28, 2.79, P = 0.001) based on IVW method, which showed that one standard deviation increase in quantile-normalized FI could elevate the risk of insomnia by 89%, but MR-Egger and weighted mode methods were not significant (Figure 2). There was no heterogeneity and horizontal pleiotropy, according to Cochran’s Q (Q = 8.648, P = 0.124), MR-Egger intercept (P = 0.388), and MR-PRESSO (P = 0.194) tests (Table 1). The IVW method showed a causal relationship between FFS and short sleep duration (OR 2.65, 95% CI: 1.89, 3.72, P < 0.001). It demonstrated that one standard deviation increase in quantile-normalized FFS could elevate the risk of insomnia by 165%. The weighted median and weighted mode methods were consistent with this result (Figure 2). Besides, the Cochran’s Q test (Q = 25.275, P = 0.118) showed no significant heterogeneity). The MR-Egger regression (P = 0.396) and MR-PRESSO (P = 0.152) tests did not show the presence of pleiotropy (Table 1).
No significant association between FI and long sleep duration was observed (OR 1.1.5, 95% CI: 0.66, 1.98, P = 0.627), and the effects generated by four methods for the association were consistent (Figure 2). The sensitivity test did not find any evidence for heterogeneity (Cochran’s Q test: Q = 9.121, P = 0.167). There was no pleiotropy in the MR-Egger regression (P = 0.878) and MR-PRESSO test (P = 0.192) (Table 1). The causal relationship between FFS and long sleep duration was observed using IVW and weighted median methods (OR 3.06, 95% CI: 1.81, 5.18, P < 0.001; OR 3.46, 95% CI: 1.87, 6.41, P < 0.001), which reported that one standard deviation increase in quantile-normalized FFS could elevate the risk of insomnia by 206%. However, MR-Egger and weighted mode methods did not indicate the result (Figure 2). After the adjustment of outliers, the presence of heterogeneity was still observed in the Cochran’s Q test (Q = 36.680, P = 0.026). The MR-Egger regression (P = 0.800) revealed no pleiotropy among IVs, however, the MR-PRESSO test found the presence of pleiotropy (P = 0.039) (Table 1).
The MR study found that the genetic predisposition to FI was statistically significantly associated with sleep apnea (OR 1.21, 95% CI: 1.04, 1.41, P = 0.015; OR 1.25, 95% CI: 1.02, 1.53, P = 0.030) based on the IVW and weighted median methods (Figure 2). It revealed that one standard deviation increase in quantile-normalized FI could elevate the risk of insomnia by 21%. In addition, the MR results were robust in several sensitivity analyses. The Cochran’s Q test did not show any heterogeneity (Q = 3.898, P = 0.791. The MR-Egger regression (P = 0.140) and MR-PRESSO test (P = 0.683) did not find significant horizontal pleiotropy (Table 1). All four MR methods supported that sleep apnea was suggestively associated with the higher FFS (IVW, OR 1.57, 95% CI: 1.28, 1.94, P < 0.001) (Figure 2). It showed that one standard deviation increase in quantile-normalized FFS could elevate the risk of insomnia by 57%. Heterogeneity and horizontal pleiotropy were not found in the sensitivity analyses (Cochran’s Q test: Q = 26.166, P = 0.160; MR-Egger intercept: P = 0.099; MR-PRESSO: P = 0.192) (Table 1).
Causal Effects of Sleep Disturbances on Frailty Measures
For the effect of sleep disturbances on FI, the reverse MR study revealed that genetically predicted insomnia (β 0.43, 95% CI: 0.27, 0.59, P < 0.001), short sleep duration (β 0.12, 95% CI: 0.07, 0.18, P < 0.001) and long sleep duration (β 0.03, 95% CI: 0.00, 0.06, P = 0.030) were statistically significantly associated with an increase in FI, based on the IVW method, while no significant association was found for genetically predicted sleep apnea with FI (β 0.02, 95% CI: −0.11, 0.14, P = 0.774) based on the IVW method (Figure 3). All MR results remained robust across several sensitivity analyses. The results of Cochran’s Q test showed no significant heterogeneity (insomnia: Q = 24.072, P = 0.088; short sleep duration: Q = 20.913, P = 0.052; long sleep duration: Q = 11,638, P = 0.769; sleep apnea: Q = 7.479, P = 0.113). The results of the MR-Egger regression (insomnia: P = 0.096; short sleep duration: P = 0.490; long sleep duration: P = 0.431; sleep apnea: P = 0.108) and MR-PRESSO test (insomnia: P = 0.117; short sleep duration: P = 0.077; long sleep duration: P = 0.778; sleep apnea: P = 0.165) revealed no significant horizontal pleiotropy (Table 1).
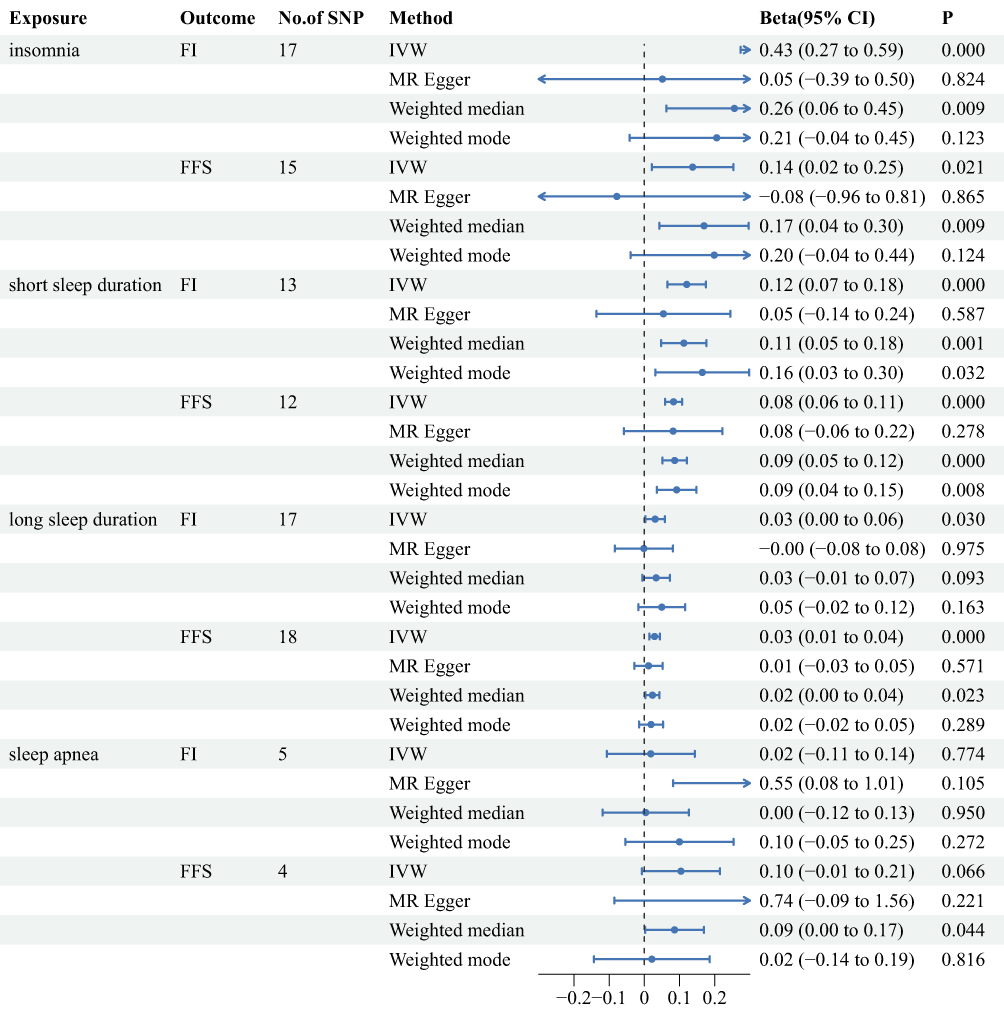 |
Figure 3 MR estimates for the causal effect of sleep disturbances on frailty measures. Abbreviations: FI, frailty index; FFS, Fried Frailty Score; SNPs, single nucleotide polymorphisms; IVW, inverse variance-weighted method; CI, confidence interval; OR, odds ratio. |
For the effect of sleep disturbances on FFS, the reverse MR study revealed that genetically predicted insomnia (β 0.14, 95% CI: 0.02, 0.25, P = 0.021), short sleep duration (β 0.08, 95% CI: 0.06, 0.11, P < 0.001) and long sleep duration (β 0.03, 95% CI: 0.01, 0.04, P < 0.001) were statistically significantly associated with an increase in FFS, based on the IVW method, while no significant association was found for sleep apnea with FFS (β 0.10, 95% CI: −0.01, 0.21, P = 0.066) (Figure 3). The Cochrane’s Q test and MR-PRESSO test regarding the association of insomnia with FFS suggested the presence of heterogeneity and horizontal pleiotropy (Cochran’s Q test: Q = 28.304, P = 0.013; MR-PRESSO: P = 0.016). In addition, heterogeneity was identified in the analysis between sleep apnea and FFS (Cochran’s Q test: Q = 8.826, P = 0.032). Other MR results remained robust across several sensitivity analyses. There was no significant heterogeneity by the Cochran’s Q test (short sleep duration: Q = 11.723, P = 0.385; long sleep duration: Q = 12.561, P = 0.765). There was no significant horizontal pleiotropy by MR-Egger regression (insomnia: P = 0.638; short sleep duration: P = 0.989; long sleep duration: P = 0.381; sleep apnea: P = 0.268) and MR-PRESSO test (short sleep duration: P = 0.502; long sleep duration: P = 0.796; sleep apnea: P = 0.099) (Table 1).
Discussion
In this study, we employed MR to explore the bidirectional causal relationships between frailty measures and sleep disturbances, measured by FI and FFS. Our findings suggested a causal link that increased FI was associated with shorter sleep duration and sleep apnea. The genetically predicted FFS demonstrated a causal association with insomnia, shorter sleep duration, and sleep apnea. In the reverse MR analysis, we found that genetically predicted sleep disturbances, including insomnia, short sleep duration, and long duration causally contributed to an elevation in FI. Our study revealed that genetically predicted sleep disturbances, including short sleep duration and long duration, were causally related to increased risk of frailty measured by FFS. However, no significant effect was observed for sleep apnea on the risk of frailty. Furthermore, sensitivity analysis showed horizontal pleiotropy in the causal effect of FI on insomnia, FFS on long sleep duration, and insomnia on FFS, suggesting cautious interpretations of the results. Compared to previous studies, we applied two different measuring tools, which enhanced the accuracy of the results.22,23 Regarding sleep apnea and frailty, the study conducted by Deng et al demonstrated that sleep apnea increased the risk of frailty, whereas our study did not provide the finding.23 Besides, other findings were generally consistent with previous literature.
The study revealed a bidirectional association between frailty and insomnia. Existing literature focusing on the relationship between insomnia and frailty mostly reported that insomnia was associated with frailty, however, few studies have examined the effect of frailty on insomnia.15–17 Our results were consistent with the previous study that a 2-year longitudinal analysis demonstrated that insomnia was a prognostic risk factor for frailty and frailty also predicted severe insomnia symptoms, adjusting for socio-demographic variables, health conditions, and health behaviors.54 The current studies have highlighted the roles of chronic pain and depression in insomnia.55–57 Frailty as a count of mental and physical disorders, including multiple chronic conditions with pain and discomfort, could lead to difficulty falling or staying asleep. In addition, regular medication use for this might be also a risk factor for insomnia.58 While, insomnia is also thought to be a risk factor for depression and promote or exacerbate frailty.59 Furthermore, frail individuals may experience impaired thermoregulation due to a decrease in muscle mass and metabolic activity, which can disturb sleep by making it challenging to maintain an optimal core temperature.58,60–69
Our findings indicated a significant genetic correlation between frailty and sleep duration. We have observed that genetic susceptibility to frailty was shown to be a risk factor for short sleep duration, which has not been reported in previous studies. Furthermore, reverse direction analysis has shown that shorter sleep duration could increase the likelihood of frailty, which was the same as the results of other studies.17,70,71 In the reverse analysis, we found that long sleep duration was causally associated with frailty, which was consistent with the previous literature. A study comprising 7623 older adults demonstrated that long sleep duration was significantly associated with frailty incidence among older adults even after adjustment for confounding factors.72 Another community-based cohort study corroborated this finding, suggesting that older adults with long sleep duration had an elevated incidence of frailty.70
Furthermore, our study found that frailty was strongly correlated with sleep apnea; however, no causal effect of sleep apnea on frailty was observed. Researchers have indicated that participants with an intermediate or high risk of obstructive sleep apnea were more likely to be frail.73 A systematic review and meta-analysis demonstrated that sleep-disordered breathing was correlated with frailty.74 The inconsistent results were probably caused by some unknown confounders. The heterogeneity was identified in the analysis between sleep apnea and FFS, which may cause some bias, indicating cautious interpretations of the results. Another reason might be that the statistical power of our analysis was not sufficient to detect the weak effects of sleep apnea on frailty, suggesting a need for larger studies. Further understanding of the relationship between sleep apnea and frailty may guide the comprehensive management of patients with sleep apnea.
Our research demonstrated that the causal relationships between frailty measures and sleep disturbances is bidirectional. Although pathophysiological mechanisms underlying the associations remained uncertain, several shared pathways might be considered. Some studies have shown that both short sleep duration and long sleep duration were associated with increasing risk of sarcopenia.75 Sleep deprivation affects many important physiological functions of the body, such as protein synthesis, muscle growth, and hormone production, which could lead to sarcopenia.76,77 Furthermore, sarcopenia has been regarded as a strong indicator of reduced physical performance and played an essential role in the process of frailty.78 Frailty-related physical and cognitive decline decreases daily physical activity, which may interfere with normal sleep-wake cycles and contribute to sleep disorders.79 Simultaneously, sleep disturbances are linked to neurodegenerative changes and cognitive impairment, which could exacerbate frailty by reducing the ability to maintain physical and social functions.80 In addition, previous studies found that some adipokines, such as adiponectin, leptin, and ghrelin, played important roles in sleep disorders.81 An observational study showed a significant association between plasma adiponectin levels and obstructive sleep apnea.82 A systematic review and meta-analysis covering a total of 2250 participants indicated that short sleep duration is correlated with elevated ghrelin levels, while sleep deprivation had a significant effect on the levels of both leptin and ghrelin.83 There was a strong positive relationship between ghrelin and the apnea–hypopnea index or the Epworth sleepiness scale.84 Similarly, it has been shown that higher plasma adiponectin was an independent risk factor for frailty status.85,86 Also, researchers found that higher leptin levels increased the risk of exhaustion and muscle weakness, which led to frailty.87 Moreover, frailty can lead to a significant effect on sleep quality through changes in circadian rhythms and hormones, notably in cortisol and melatonin, which are crucial for sleep quality.61–64 The low testosterone has been found to be associated with frailty.66,67 Other studies have indicated the relationship between low level of testosterone and sleep quality.68,69 Therefore, the associations between frailty and impaired sleep may be also explained by testosterone. In addition, it has been shown that impaired sleep was associated with reduced growth hormone and insulin-like growth factor-1, which affected muscle metabolism, strength, and function, leading to frailty.76 Also, increasing evidence found possible associations between sleep disorders and glucose imbalance.88,89 Several studies concluded that sarcopenia was related to insulin resistance, diabetes, and metabolic syndrome.90,91 Insulin resistance exerts a strong effect on muscle mass by promoting muscle catabolism and inhibiting anabolism.92
Besides, inflammation was regarded as a potential pathway between frailty and sleep disturbances. Previous studies reported that sleep disturbances induced inflammatory responses, with increased levels of interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), and C-reactive protein (CRP).93–95 According to recent studies, elevated inflammatory marker levels, such as IL-6, TNF-α, and CRP, have been identified in individuals with frailty.96,97 Higher levels of inflammatory reactions might cause muscle loss and protein degradation, increasing the risk of frailty.98 Moreover, chronic inflammation was found to be associated with some diseases, such as depression and cardiovascular disease, thus impairing cognitive action and physical function.93,99 Therefore, the inflammatory process was considered a major mediator between frailty risk and sleep disturbances.98 Also, existing research demonstrated that sleep deprivation affected the innate and adaptive immune parameters, leading to changes in the defense system and increasing the risk for chronic disease.100,101 Additionally, there has been evidence suggesting that dysregulated autonomic function, such as decreased heart rate variability, is common in both sleep disturbances and frailty, leading to poor cardiovascular health and systemic homeostasis.102,103
Our study confirmed the bidirectional causality between frailty measures and sleep disturbances, even though some findings with small effect sizes, which are still instructive for clinical practice. For instance, sleep duration has been associated with cognitive decline, particularly in older adults.104,105 Thus, even small effect sizes may have a greater influence on vulnerable populations requiring attention in clinical practice. Future research should consider the distribution and impact of these effect sizes in different populations and how these effects could be enhanced by improving sleep quality. Existing interventions have proven effective in the recovery of insomnia and exert a positive effect on daily life.106,107 These results highlighted the role of assessing and improving sleep quality in frailty management, which could inform clinical and public health decision-making aiming to avoid the process of frailty.
There are some advantages in this study. First, to the best of our knowledge, this is the first MR study employing the GWAS to investigate the bidirectional relationships between frailty measures and sleep disturbances, using two different frailty definitions, based on FI and FFS. Second, the genetic data were from a large sample European population, which strengthened the reliability of results and avoided possible heterogeneity. Furthermore, the IVW estimates were examined by multiple MR sensitivity analyses to detect heterogeneity and horizontal pleiotropy. Nevertheless, several limitations should be considered in the current study. First, the GWAS data we utilized were derived from European countries, and the causalities might not be generalizable for other populations. The previous study indicated that 81% of individuals in GWAS were European descent and it limited the generalizability of existing genetic findings to global populations.108 Although reducing bias due to population stratification, it is necessary to acknowledge that our conclusions are more applicable to European ancestry and require further validation in non-European ancestry, which is the common limitation and challenge in the GAWS. Future studies should involve a much broader range of populations to improve the generalizability of genomics. Second, there was some overlap with the UK Biobank samples. Although we evaluated potential bias by calculating type I error rates, which would not affect the MR estimates, the results should be treated cautiously. Third, we only employed FI and FFS as assessment tools for quantifying frailty, and more studies including other frailty screening instruments are needed to confirm our findings. Fourth, the characteristics we focused on were widely representative and recognized indicators of sleep disturbances including insomnia, sleep duration and sleep apnea, which could not fully reflect the complexity and diversity of sleep disturbances. Fifth, although we utilized a large GWAS database, limited SNPs were selected for long sleep duration reaching the genome-wide significance (P < 5 * 10−8). We have chosen a relaxed threshold (P < 5 * 10−6) for identifying genetic variants, which might influence the validity of genetic instruments and increase the risk of weak instrument bias. To address this, we implanted multiple measures, such as F statistic and R2 value to assess and ensure the reliability of conclusions. Sixth, it is necessary to acknowledge that we employed multiple complementary methods to elevate the validity of the MR assumptions and to reduce bias, however, identifying all sources of heterogeneity remains challenging. Heterogeneity and horizontal pleiotropy still existed in the sensitivity analyses after removing outliners, which could introduce bias. Last, we usually assume that the association between genetic instrumental variables and exposure or outcome is linear in MR analyses.109,110 When exposure or outcome is binary, we need to hypothesize that causality is linear and homogeneous across individuals, which may be less reasonable in binary variables. The binary nature may cause challenges in the validity of MR assumptions. And our results should be interpreted as causal estimations in continuous variables, which were represented by binary variables.109,110 In summary, our findings should also be interpreted with caution, and future studies are required to verify the causality.
Conclusions
In summary, the study provided bidirectional causal associations between frailty and sleep disturbances. A better understanding of the relationships between frailty and sleep disturbances could contribute to better prediction and intervention at sleep performance for potential risk of frailty and guide more comprehensive management. Further and more multiple studies are still needed to examine the causality inferred in our study.
Abbreviations
MR, Mendelian randomization; GWAS, Genome-wide association studies; FI, Frailty index; FFS, Fried Frailty Score; IVW, Inverse variance-weighted; MR-PRESSO, Mendelian randomization pleiotropy residual sum and outlier; RCT, Randomized controlled trial; SNPs, Single nucleotide polymorphisms; IVs, Instrumental variables; LD, Linkage disequilibrium; ORs, Odds ratios; CIs, Confidence intervals; IL-6, Interleukin-6; TNF-α, Tumor necrosis factor-α; CRP, C-reactive protein.
Data Sharing Statement
The data used in this study were obtained from public GWAS data. The data generated and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
The study has been approved by the Institutional Review Board of the Peking Union Medical College Hospital (Ethics Approval Number: I-24ZM0035) and the informed consent was found in the original studies.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by the National High Level Hospital Clinical Research Funding [2022-PUMCH-B-119].
Disclosure
Lu Che and Han Zang are co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146–156. doi:10.1093/gerona/56.3.M146
2. Dent E, Martin FC, Bergman H, Woo J, Romero-Ortuno R, Walston JD. Management of frailty: opportunities, challenges, and future directions. Lancet. 2019;394(10206):1376–1386. doi:10.1016/S0140-6736(19)31785-4
3. Vermeiren S, Vella-Azzopardi R, Beckwée D, et al. Frailty and the prediction of negative health outcomes: a meta-analysis. J Am Med Dir Assoc. 2016;17(12):1163.e1161–1163.e1117. doi:10.1016/j.jamda.2016.09.010
4. Ensrud KE, Ewing SK, Taylor BC, et al. Comparison of 2 frailty indexes for prediction of falls, disability, fractures, and death in older women. Arch Intern Med. 2008;168(4):382–389. doi:10.1001/archinternmed.2007.113
5. Hewitt J, Long S, Carter B, Bach S, McCarthy K, Clegg A. The prevalence of frailty and its association with clinical outcomes in general surgery: a systematic review and meta-analysis. Age Ageing. 2018;47(6):793–800. doi:10.1093/ageing/afy110
6. Shi SM, Olivieri-Mui B, McCarthy EP, Kim DH. Changes in a frailty index and association with mortality. J Am Geriatr Soc. 2021;69(4):1057–1062. doi:10.1111/jgs.17002
7. Kojima G, Iliffe S, Walters K. Frailty index as a predictor of mortality: a systematic review and meta-analysis. Age Ageing. 2018;47(2):193–200. doi:10.1093/ageing/afx162
8. Mander BA, Winer JR, Walker MP. Sleep and human aging. Neuron. 2017;94(1):19–36. doi:10.1016/j.neuron.2017.02.004
9. Troynikov O, Watson CG, Nawaz N. Sleep environments and sleep physiology: a review. J Therm Biol. 2018;78:192–203. doi:10.1016/j.jtherbio.2018.09.012
10. Cochen V, Arbus C, Soto ME, et al. Sleep disorders and their impacts on healthy, dependent, and frail older adults. J Nutr Health Aging. 2009;13(4):322–329. doi:10.1007/s12603-009-0030-0
11. Carvalhas-Almeida C, Cavadas C, Álvaro AR. The impact of insomnia on frailty and the hallmarks of aging. Aging Clin Exp Res. 2023;35(2):253–269. doi:10.1007/s40520-022-02310-w
12. Wang C, Holtzman DM. Bidirectional relationship between sleep and Alzheimer’s disease: role of amyloid, tau, and other factors. Neuropsychopharmacology. 2020;45(1):104–120.
13. Irwin MR, Opp MR. Sleep health: reciprocal regulation of sleep and innate immunity. Neuropsychopharmacology. 2017;42(1):129–155. doi:10.1038/npp.2016.148
14. Ballesio A, Zagaria A, Ottaviani C, Steptoe A, Lombardo C. Sleep disturbance, neuro-immune markers, and depressive symptoms in older age: conditional process analysis from the English Longitudinal Study of Aging (ELSA). Psychoneuroendocrinology. 2022;142:105770. doi:10.1016/j.psyneuen.2022.105770
15. Wen Q, Yan X, Ren Z, Wang B, Liu Y, Jin X. Association between insomnia and frailty in older population: a meta-analytic evaluation of the observational studies. Brain Behav. 2023;13(1):e2793. doi:10.1002/brb3.2793
16. Fan J, Liu Y, Wang Q, Zhao H, Kong L, Li J. Association of insomnia and multidimensional frailty in community-dwelling older adults: a cross-sectional survey. J Clin Nurs. 2022;31(1–2):167–173. doi:10.1111/jocn.15893
17. Pourmotabbed A, Boozari B, Babaei A, et al. Sleep and frailty risk: a systematic review and meta-analysis. Sleep Breath. 2020;24(3):1187–1197. doi:10.1007/s11325-020-02061-w
18. Tang JY, Luo H, Tse M, Lum TY, Wong GH, Li SX. The relationship between insomnia symptoms and frailty in community-dwelling older persons: a path analysis. Sleep Med. 2021;84:237–243. doi:10.1016/j.sleep.2021.05.039
19. Liu M, Hou T, Nkimbeng M, et al. Associations between symptoms of pain, insomnia and depression, and frailty in older adults: a cross-sectional analysis of a cohort study. Int J Nurs Stud. 2021;117:103873. doi:10.1016/j.ijnurstu.2021.103873
20. Seib C, Anderson D, Lee K. Prevalence and correlates of sleep disturbance in postmenopausal women: the Australian Healthy Aging of Women (HOW) Study. J Womens Health. 2014;23(2):151–158. doi:10.1089/jwh.2013.4472
21. Davey Smith G, Hemani G. Mendelian randomization: genetic anchors for causal inference in epidemiological studies. Hum Mol Genet. 2014;23(R1):R89–98. doi:10.1093/hmg/ddu328
22. Lu ZX, Sang N, Liu RC, et al. The causal relationship between sleep disturbances and the risk of frailty: a two-sample Mendelian randomization study. Eur J Ageing. 2024;21(1):9. doi:10.1007/s10433-024-00804-2
23. Deng Z, Hu Y, Duan L, et al. Causality between sleep traits and the risk of frailty: a Mendelian randomization study. Front Public Health. 2024;12:1381482. doi:10.3389/fpubh.2024.1381482
24. Balomenos V, Ntanasi E, Anastasiou CA, et al. Association between sleep disturbances and frailty: evidence from a population-based study. J Am Med Dir Assoc. 2021;22(3):551–558.e551. doi:10.1016/j.jamda.2020.08.012
25. Skrivankova VW, Richmond RC, Woolf BAR, et al. Strengthening the reporting of observational studies in epidemiology using Mendelian randomization: the STROBE-MR statement. JAMA. 2021;326(16):1614–1621. doi:10.1001/jama.2021.18236
26. Skrivankova VW, Richmond RC, Woolf BAR, et al. Strengthening the reporting of observational studies in epidemiology using Mendelian randomisation (STROBE-MR): explanation and elaboration. BMJ. 2021;375:n2233. doi:10.1136/bmj.n2233
27. Atkins JL, Jylhävä J, Pedersen NL, et al. A genome-wide association study of the frailty index highlights brain pathways in ageing. Aging Cell. 2021;20(9):e13459. doi:10.1111/acel.13459
28. Searle SD, Mitnitski A, Gahbauer EA, Gill TM, Rockwood K. A standard procedure for creating a frailty index. BMC Geriatr. 2008;8:24. doi:10.1186/1471-2318-8-24
29. Williams DM, Jylhävä J, Pedersen NL, Hägg S. A frailty index for UK Biobank participants. J Gerontol A Biol Sci Med Sci. 2019;74(4):582–587. doi:10.1093/gerona/gly094
30. Buniello A, MacArthur JAL, Cerezo M, et al. The NHGRI-EBI GWAS catalog of published genome-wide association studies, targeted arrays and summary statistics 2019. Nucleic Acids Res. 2019;47(D1).
31. Ye Y, Noche RB, Szejko N, et al. A genome-wide association study of frailty identifies significant genetic correlation with neuropsychiatric, cardiovascular, and inflammation pathways. GeroScience. 2023;45(4):2511–2523. doi:10.1007/s11357-023-00771-z
32. Ramsay SE, Arianayagam DS, Whincup PH, et al. Cardiovascular risk profile and frailty in a population-based study of older British men. Heart. 2015;101(8):616–622.
33. Chen C, Winterstein AG, Fillingim RB, Wei YJ Body weight, frailty, and chronic pain in older adults: a cross-sectional study. BMC Geriatr. 2019;19(1):143.
34. Handforth C, Clegg A, Young C. The prevalence and outcomes of frailty in older cancer patients: a systematic review. Ann Oncol. 2015;26(6):1091–1101.
35. Schoeler T, Speed D, Porcu E, Pirastu N, Pingault JB, Kutalik Z. Participation bias in the UK Biobank distorts genetic associations and downstream analyses. Nat Hum Behav. 2023;7(7):1216–1227. doi:10.1038/s41562-023-01579-9
36. Campos AI, Ingold N, Huang Y, et al. Discovery of genomic loci associated with sleep apnea risk through multi-trait GWAS analysis with snoring. Sleep. 2023;46(3). doi:10.1093/sleep/zsac308
37. Fawcett KA, Barroso I The genetics of obesity: FTO leads the way. Trends Genet. 2010;26(6):266–274.
38. Koch AL, Brown RH, Woo H, et al. Obstructive Sleep Apnea and Airway Dimensions in Chronic Obstructive Pulmonary Disease. Ann Am Thorac Soc. 2020;17(1):116–118.
39. Chopra A, Jung M, Kaplan RC, et al. Sleep apnea is associated with hearing impairment: the hispanic community health Study/Study of latinos. J Clin Sleep Med. 2016;12(5):719–726.
40. Austin-Zimmerman I, Levey DF, Giannakopoulou O, et al. Genome-wide association studies and cross-population meta-analyses investigating short and long sleep duration. Nat Commun. 2023;14(1):6059. doi:10.1038/s41467-023-41249-y
41. Dashti HS, Jones SE, Wood AR, et al. Genome-wide association study identifies genetic loci for self-reported habitual sleep duration supported by accelerometer-derived estimates. Nat Commun. 2019;10(1):1100.
42. Cross-Disorder Group of the Psychiatric Genomics Consortium. Identification of risk loci with shared effects on five major psychiatric disorders: a genome-wide analysis. Lancet. 2013;381(9875):1371–1379. doi:10.1016/S0140-6736(12)62129-1
43. Larsson SC, Butterworth AS, Burgess S. Mendelian randomization for cardiovascular diseases: principles and applications. Eur Heart J. 2023;44(47):4913–4924. doi:10.1093/eurheartj/ehad736
44. Ma T, Chen M, Cheng X, Bai Y Assessment of bidirectional relationships between frailty and mental disorders: a bidirectional mendelian randomization study. J Am Med Dir Assoc. 2024;25(3):506–513.e529.
45. Long Y, Tang L, Zhou Y, Zhao S, Zhu H. Causal relationship between gut microbiota and cancers: a two-sample Mendelian randomisation study. BMC Med. 2023;21(1):66.
46. Pierce BL, Ahsan H, Vanderweele TJ. Power and instrument strength requirements for Mendelian randomization studies using multiple genetic variants. Int J Epidemiol. 2011;40(3):740–752. doi:10.1093/ije/dyq151
47. Burgess S, Scott RA, Timpson NJ, Davey Smith G, Thompson SG. Using published data in Mendelian randomization: a blueprint for efficient identification of causal risk factors. Eur J Epidemiol. 2015;30(7):543–552. doi:10.1007/s10654-015-0011-z
48. Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. 2016;40(4):304–314. doi:10.1002/gepi.21965
49. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44(2):512–525. doi:10.1093/ije/dyv080
50. Hartwig FP, Davey Smith G, Bowden J. Robust inference in summary data Mendelian randomization via the zero modal pleiotropy assumption. Int J Epidemiol. 2017;46(6):1985–1998. doi:10.1093/ije/dyx102
51. Burgess S, Butterworth A, Thompson SG. Mendelian randomization analysis with multiple genetic variants using summarized data. Genet Epidemiol. 2013;37(7):658–665. doi:10.1002/gepi.21758
52. Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet. 2018;50(5):693–698. doi:10.1038/s41588-018-0099-7
53. Burgess S, Davies NM, Thompson SG Bias due to participant overlap in two-sample Mendelian randomization. Genet Epidemiol. 2016;40(7):597–608.
54. Nemoto Y, Sato S, Kitabatake Y, et al. Bidirectional relationship between insomnia and frailty in older adults: a 2-year longitudinal study. Arch Gerontol Geriatr. 2021;97:104519. doi:10.1016/j.archger.2021.104519
55. Craner JR, Flegge LG. Insomnia symptoms and chronic pain: outcomes of an interdisciplinary pain rehabilitation program. Pain Pract. 2022;22(2):171–181. doi:10.1111/papr.13075
56. Todd J, Austin H, Clarke P, Notebaert L. Chronic pain, insomnia and their mutual maintenance: a call for cognitive bias research. J Pain. 2022;23(9):1530–1542. doi:10.1016/j.jpain.2022.03.241
57. Lin T, Zhao Y, Xia X, Ge N, Yue J. Association between frailty and chronic pain among older adults: a systematic review and meta-analysis. Eur Geriatr Med. 2020;11(6):945–959. doi:10.1007/s41999-020-00382-3
58. Patel D, Steinberg J, Patel P. Insomnia in the elderly: a review. J Clin Sleep Med. 2018;14(6):1017–1024. doi:10.5664/jcsm.7172
59. Vargas I, Perlis ML. Insomnia and depression: clinical associations and possible mechanistic links. Curr Opin Psychol. 2020;34:95–99. doi:10.1016/j.copsyc.2019.11.004
60. Fan Y, Wang Y, Gu P, Han J, Tian Y How Temperature Influences Sleep. Int J Mol Sci. 2022;23(20).
61. Cai R, Gao L, Gao C, et al. Circadian disturbances and frailty risk in older adults. Nat Commun. 2023;14(1):7219. doi:10.1038/s41467-023-42727-z
62. Blacher E, Tsai C, Litichevskiy L, et al. Aging disrupts circadian gene regulation and function in macrophages. Nat Immunol. 2022;23(2):229–236. doi:10.1038/s41590-021-01083-0
63. Oh G, Koncevičius K, Ebrahimi S, et al. Circadian oscillations of cytosine modification in humans contribute to epigenetic variability, aging, and complex disease. Genome Biol. 2019;20(1):2. doi:10.1186/s13059-018-1608-9
64. Maggio M, Cappola AR, Ceda GP, et al. The hormonal pathway to frailty in older men. J Endocrinol Invest. 2005;28(11 Suppl Proceedings):15–19.
65. Maggio M, Cattabiani C, Lauretani F, et al. The concept of multiple hormonal dysregulation. Acta Biomed. 2010;81(Suppl 1):19–29.
66. Swiecicka A, Eendebak R, Lunt M, et al. Reproductive hormone levels predict changes in frailty status in community-dwelling older men: European Male Ageing Study prospective data. J Clin Endocrinol Metab. 2018;103(2):701–709. doi:10.1210/jc.2017-01172
67. Peng X, Hou L, Zhao Y, et al. Frailty and testosterone level in older adults: a systematic review and meta-analysis. Eur Geriatr Med. 2022;13(3):663–673. doi:10.1007/s41999-022-00614-8
68. Agrawal P, Singh SM, Able C, Kohn TP, Herati AS. Sleep disorders are associated with testosterone deficiency and erectile dysfunction-a U.S. claims database analysis. Int J Impot Res. 2024;36(1):78–82. doi:10.1038/s41443-022-00649-2
69. Patel P, Shiff B, Kohn TP, Ramasamy R. Impaired sleep is associated with low testosterone in US adult males: results from the National Health and Nutrition Examination Survey. World J Urol. 2019;37(7):1449–1453. doi:10.1007/s00345-018-2485-2
70. Moreno-Tamayo K, Manrique-Espinoza B, Morales-Carmona E, Salinas-Rodríguez A. Sleep duration and incident frailty: the rural frailty study. BMC Geriatr. 2021;21(1):368. doi:10.1186/s12877-021-02272-0
71. Nakakubo S, Makizako H, Doi T, et al. Long and short sleep duration and physical frailty in community-dwelling older adults. J Nutr Health Aging. 2018;22(9):1066–1071. doi:10.1007/s12603-018-1116-3
72. Chen S, Wang Y, Wang Z, et al. Sleep duration and frailty risk among older adults: evidence from a retrospective, population-based cohort study. J Nutr Health Aging. 2022;26(4):383–390. doi:10.1007/s12603-022-1766-z
73. Mehawej J, Saczynski JS, Kiefe CI, et al. Association between risk of obstructive sleep apnea and cognitive performance, frailty, and quality of life among older adults with atrial fibrillation. J Clin Sleep Med. 2022;18(2):469–475. doi:10.5664/jcsm.9622
74. Sun R, Xie Y, Jiang W, Wang E, Li X. Effects of different sleep disorders on frailty in the elderly: a systematic review and meta-analysis of observational studies. Sleep Breath. 2023;27(1):91–101. doi:10.1007/s11325-022-02610-5
75. Pourmotabbed A, Ghaedi E, Babaei A, et al. Sleep duration and sarcopenia risk: a systematic review and dose-response meta-analysis. Sleep Breath. 2020;24(4):1267–1278.
76. Piovezan RD, Abucham J, dos Santos RV, Mello MT, Tufik S and Poyares D. The impact of sleep on age-related sarcopenia: possible connections and clinical implications. Ageing Res Rev. 2015;23. doi:10.1016/j.arr.2015.07.003 210–220.
77. Chien MY, Wang LY, Chen HC The Relationship of Sleep Duration with Obesity and Sarcopenia in Community-Dwelling Older Adults. Gerontology. 2015;61(5):399–406.
78. Ye L, Liang R, Liu X, Li J, Yue J and Zhang X. Frailty and sarcopenia: A bibliometric analysis of their association and potential targets for intervention. Ageing Res Rev. 2023;92:102111. doi:10.1016/j.arr.2023.102111
79. Sullivan Bisson AN, Robinson SA, Lachman ME Walk to a better night of sleep: testing the relationship between physical activity and sleep. Sleep Health. 2019;5(5):487–494.
80. Brownlow JA, Miller KE, Gehrman PR Insomnia and Cognitive Performance. Sleep Med Clin. 2020;15(1):71–76.
81. Wei Z, Chen Y, Upender RP. Sleep disturbance and metabolic dysfunction: the roles of adipokines. Int J mol Sci. 2022;23(3):1706.
82. Zeng F, Wang X, Hu W, Wang L. Association of adiponectin level and obstructive sleep apnea prevalence in obese subjects. Medicine. 2017;96(32):e7784. doi:10.1097/MD.0000000000007784
83. Lin J, Jiang Y, Wang G, et al. Associations of short sleep duration with appetite-regulating hormones and adipokines: a systematic review and meta-analysis. Obes Rev. 2020;21(11):e13051. doi:10.1111/obr.13051
84. Ursavas A, Ilcol YO, Nalci N, Karadag M, Ege E. Ghrelin, leptin, adiponectin, and resistin levels in sleep apnea syndrome: role of obesity. Ann Thorac Med. 2010;5(3):161–165. doi:10.4103/1817-1737.65050
85. Nagasawa M, Takami Y, Akasaka H, et al. High plasma adiponectin levels are associated with frailty in a general old-old population: the Septuagenarians, Octogenarians, Nonagenarians Investigation with Centenarians study. Geriatr Gerontol Int. 2018;18(6):839–846. doi:10.1111/ggi.13258
86. Tsai JS, Wu CH, Chen SC, et al. Plasma adiponectin levels correlate positively with an increasing number of components of frailty in male elders. PLoS One. 2013;8(2):e56250. doi:10.1371/journal.pone.0056250
87. Lana A, Valdés-Bécares A, Buño A, Rodríguez-Artalejo F, Lopez-Garcia E. Serum leptin concentration is associated with incident frailty in older adults. Aging Dis. 2017;8(2):240–249. doi:10.14336/AD.2016.0819
88. Seelig E, Keller U, Klarhöfer M, et al. Neuroendocrine regulation and metabolism of glucose and lipids in primary chronic insomnia: a prospective case-control study. PloS One. 2013;8(4).
89. Cappuccio FP, D’Elia L, Strazzullo P, Miller MA Quantity and quality of sleep and incidence of type 2 diabetes: a systematic review and meta-analysis. Diabetes Care. 2010;33(2):414–420.
90. Lee CG, Boyko EJ, Strotmeyer ES, et al. Association between insulin resistance and lean mass loss and fat mass gain in older men without diabetes mellitus. J Am Geriatr Soc. 2011;59(7):1217–1224.
91. Moon SS Low skeletal muscle mass is associated with insulin resistance, diabetes, and metabolic syndrome in the Korean population: the korea national health and nutrition examination survey (KNHANES) 2009-2010. Endocr J. 2014;61(1):61–70.
92. Guillet C, Boirie Y Insulin resistance: a contributing factor to age-related muscle mass loss?. Diabetes Metab. 2005 31 Spec No 2:5s20-25s26.
93. Irwin MR. Sleep and inflammation: partners in sickness and in health. Nat Rev Immunol. 2019;19(11):702–715. doi:10.1038/s41577-019-0190-z
94. Park H, Tsai KM, Dahl RE, et al. Sleep and inflammation during adolescence. Psychosom Med. 2016;78(6):677–685. doi:10.1097/PSY.0000000000000340
95. Piber D, Cho JH, Lee O, Lamkin DM, Olmstead R, Irwin MR. Sleep disturbance and activation of cellular and transcriptional mechanisms of inflammation in older adults. Brain Behav Immun. 2022;106:67–75. doi:10.1016/j.bbi.2022.08.004
96. Picca A, Coelho-Junior HJ, Calvani R, Marzetti E, Vetrano DL. Biomarkers shared by frailty and sarcopenia in older adults: a systematic review and meta-analysis. Ageing Res Rev. 2022;73:101530. doi:10.1016/j.arr.2021.101530
97. Xu Y, Wang M, Chen D, Jiang X, Xiong Z. Inflammatory biomarkers in older adults with frailty: a systematic review and meta-analysis of cross-sectional studies. Aging Clin Exp Res. 2022;34(5):971–987. doi:10.1007/s40520-021-02022-7
98. Ma L, Sha G, Zhang Y, Li Y. Elevated serum IL-6 and adiponectin levels are associated with frailty and physical function in Chinese older adults. Clin Interv Aging. 2018;13:2013–2020. doi:10.2147/CIA.S180934
99. Couzin-Frankel J. Inflammation bares a dark side. Science. 2010;330(6011):1621. doi:10.1126/science.330.6011.1621
100. Garbarino S, Lanteri P, Bragazzi NL, Magnavita N and Scoditti E. Role of sleep deprivation in immune-related disease risk and outcomes. Commun Biol. 2021;4(1). doi:10.1038/s42003-021-02825-4
101. Besedovsky L, Lange T and Haack M. The Sleep-Immune Crosstalk in Health and Disease. Physiol Rev. 2019;99(3). doi:10.1152/physrev.00010.2018), 1325–1380.
102. Tobaldini E, Costantino G and Solbiati M, et al. Sleep, sleep deprivation, autonomic nervous system and cardiovascular diseases. Neurosci & Biobehav Rev. 2017;74. doi:10.1016/j.neubiorev.2016.07.004 321–329.
103. Dorey TW, Jansen HJ, Moghtadaei M, Jamieson KL, Rose RA. Impacts of frailty on heart rate variability in aging mice: roles of the autonomic nervous system and sinoatrial node. Heart Rhythm. 2021;18(11):1999–2008. doi:10.1016/j.hrthm.2021.07.069
104. Ma Y, Liang L, Zheng F, Shi L, Zhong B and Xie W. Association Between Sleep Duration and Cognitive Decline. JAMA Netw Open. 2020;3(9). doi:10.1001/jamanetworkopen.2020.13573), e2013573.
105. Yaffe K, Falvey CM and Hoang T. Connections between sleep and cognition in older adults. The Lancet Neurol. 2014;13(10). doi:10.1016/S1474-4422(14)70172-3), 1017–1028.
106. Redeker NS, Yaggi HK, Jacoby D, et al. Cognitive behavioral therapy for insomnia has sustained effects on insomnia, fatigue, and function among people with chronic heart failure and insomnia: the HeartSleep Study. Sleep. 2022;45(1):zsab252. doi:10.1093/sleep/zsab252
107. Yin X, Gou M and Xu J, et al. Efficacy and safety of acupuncture treatment on primary insomnia: a randomized controlled trial. Sleep Med. 2017;37. doi:10.1016/j.sleep.2017.02.012 193–200.
108. Popejoy AB and Fullerton SM. Genomics is failing on diversity. Nature. 2016;538(7624). doi:10.1038/538161a), 161–164.
109. Howe LJ, Tudball M, Davey Smith G and Davies NM. Interpreting Mendelian-randomization estimates of the effects of categorical exposures such as disease status and educational attainment. Int J Epidemiol. 2022;51(3). doi:10.1093/ije/dyab208), 948–957.
110. Burgess S and Labrecque JA. Mendelian randomization with a binary exposure variable: interpretation and presentation of causal estimates. Eur J Epidemiol. 2018;33(10). doi:10.1007/s10654-018-0424-6), 947–952.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Preliminary Screening Tool for High-Risk Frailty in Older Adults Patients with Pulmonary Tuberculosis
Li HJ, Zhou YY, Yu HH, Jiang J, Cai YW
Clinical Interventions in Aging 2025, 20:57-68
Published Date: 22 January 2025
Exploring the Causal Relationship Between Frailty and Chronic Obstructive Pulmonary Disease: Insights From Bidirectional Mendelian Randomization and Mediation Analysis
Cheng Z, Wu J, Xu C, Yan X
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:193-205
Published Date: 25 January 2025