")
Back to Journals » OncoTargets and Therapy » Volume 18
Biomarker and Prognostic Value of Super-ARMS Detection for EGFR Mutation in Advanced NSCLC
Authors Liu H, Li H, Xiao L, Guo Y, Lin G
Received 22 January 2025
Accepted for publication 22 June 2025
Published 8 July 2025 Volume 2025:18 Pages 789—801
DOI https://doi.org/10.2147/OTT.S518837
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjay Singh
Huicong Liu,1,* Hui Li,2,* Lisha Xiao,1 Yubiao Guo,1 Gengpeng Lin1
1Department of Pulmonary and Critical Care Medicine, The First Affiliated Hospital of Sun Yat-sen University, Institute of Pulmonary Diseases, Sun Yat-sen University, Guangzhou, 510080, People’s Republic of China; 2Department of Pathology, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, 510080, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Gengpeng Lin, Department of Pathology, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, 510080, People’s Republic of China, Email [email protected]
Background: ctDNA is a non-invasive and convenient method for detecting EGFR mutations in non-small cell lung cancer (NSCLC). However, its sensitivity is lower than that of tissue-based testing. To enhance ctDNA detection efficiency, we identified the patient population most suitable for ctDNA testing, assessed the relationship between ctDNA and tumor markers, and examined the clinical significance of ctDNA in medical practice.
Methods: A single-center retrospective study was conducted, including 135 patients with NSCLC who underwent histological and liquid Super-ARMS tests. Of these, 92 patients with EGFR mutations detected in both tumor tissue and plasma were classified into the EGFRt+, p+ group, while 43 patients with EGFR mutations detected only in tumor tissue were classified into the EGFRt+, p− group. The clinical features and outcomes between these two groups were compared.
Results: The positivity rate of Super-ARMS test was 68.1% (92/135). The presence of EGFRt+, p+ in the Super-ARMS test was significantly associated with pleural effusion, bone, liver, and multiple organ metastases. Compared to the EGFRt+, p+ group, the EGFRt+, p− group had a significantly better PFS (P < 0.01). Carcinoembryonic antigen (CEA) levels demonstrated a strong predictive value for identifying plasma EGFR-mutated patients (AUC 0.828, sensitivity 68.8%, specificity 84.4%), while Maximum Standardized Uptake Value (SUVmax) also showed diagnostic value for plasma EGFR-mutated patients (AUC 0.78). Additionally, combination of TP53 and EGFR mutations in plasma provided improved risk stratification for PFS (P < 0.001).
Conclusion: Patients exhibiting metastasis, elevated levels of tumor markers and SUVmax are more suitable for plasma EGFR mutation testing in clinical NSCLC management. Moreover, a positive plasma ctDNA test not only guides targeted therapy but also predicts a worse prognosis.
Keywords: NSCLC, EGFR mutation, ctDNA, CEA, prognosis
Introduction
Non-small cell lung cancer (NSCLC), which accounts for over 80%1 of all lung cancers, is the primary cause of cancer-related deaths worldwide.2 NSCLC is a highly malignant tumor, with the majority of patients diagnosed at an advanced stage. The five-year survival rate is approximately 21%.3,4 For advanced NSCLC, conventional treatment methods primarily rely on chemotherapy and radiotherapy, though their efficacy is limited. In recent years, the prognosis of NSCLC patients has significantly improved with the use of epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs).5–7 EGFR-TKIs therapy is the standard first-line treatment for NSCLC patients with EGFR mutations. EGFR is the most common mutated target gene in NSCLC, with major mutation types including exon 19 deletions (19del), exon 21 missense mutations (L858R), and exon 20 mutations. Most mutations in exon 20 are associated with TKI resistance, particularly the T790M mutation. Unfortunately, fewer than 25% of patients benefit from targeted therapy, and resistance almost invariably develops during treatment.8 Therefore, early detection of target mutations and timely targeted treatment are crucial for NSCLC patients. At present, there are multiple methods for detecting EGFR mutations, with tissue samples analysis generally considered the “gold standard”.9 However, sequencing often requires invasive tumor tissue biopsy, which carries risks10 and have limitations in detecting tissue deficiencies and tumor heterogeneity.11–13
With advances in science and technology, circulating tumor DNA (ctDNA) testing has emerged as a non-invasive and easily reproducible method, becoming a prominent focus in oncology diagnosis and treatment. ctDNA-based genotyping can be performed at any stage of the disease, facilitating real-time detection and monitoring of genotypic changes. Some studies have shown that ctDNA testing can help predict early tumor recurrence and assess both the prognosis and therapeutic efficacy during and after treatment.14–18 Main detection technologies for ctDNA include droplet digital polymerase chain reaction (ddPCR), tissue amplification refractory mutation system (ARMS), and next-generation sequencing (NGS).19–21 Among these, ARMS-PCR is noted for its high sensitivity and specificity, offering a significantly higher detection rate for gene mutation compared to traditional PCR. It has become one of the most popular and important technologies for personalized molecular tumor detection due to its lower cost and shorter detection time compared to NGS.
Super-ARMS is an enhanced version of ARMS-PCR technology that preserves the key advantages of ARMS-PCR, including simplicity, speed, accuracy, high specificity, and ease of widespread adoption. It is especially effective for detecting EGFR gene mutations in blood samples.22,23 Research indicates that Super ARMS has sensitivity close to ddPCR and offers distinct advantages over methods like NGS and ddPCR for clinical implementation.24,25 Super-ARMS has been included in clinical expert consensus on liquid biopsy and, following clinical validation, has demonstrated effectiveness in guiding EGFR-targeted therapy.26,27 However, Super-ARMS detection is associated with a certain false-negative rate, its sensitivity is lower than that of tissue-based testing. And there are currently few studies on its clinical value in detecting EGFR mutation in plasma ctDNA of advanced NSCLC.
Therefore, our study retrospectively collected data from 135 NSCLC patients with EGFR mutations confirmed by tumor biopsy sequencing to evaluate the performance of Super-ARMS in detecting EGFR gene mutations in plasma ctDNA. What’s more, in order to improve the ctDNA detection performance, we identified the patient population most suitable for ctDNA testing, assessed the relationship between ctDNA and tumor markers, and examined the clinical significance of ctDNA in medical practice. This research is of significant importance for improving the efficiency of EGFR mutation ctDNA detection and guiding clinical targeted therapies.
Methods
Patients
We collected data from 135 EGFR-mutant patients with histologically confirmed NSCLC who underwent Super-ARMS testing and EGFR-TKIs treatment at the First Affiliated Hospital of Sun Yat-sen University from 01/01/2019 to 30/12/2022. The detailed inclusion and exclusion criteria were shown in Supplementary Table 1. Baseline CT scans closest to the initiation of targeted drug therapy were reviewed by one clinical investigator and independently assessed by another for quality assurance, with the goal of determining the number and location of progressive disease sites. Metastatic sites were defined based on CT imaging, while progressive sites were defined as single lesions with at least a 20% increase in maximum dimension or the appearance of new lesions on CT imaging. Patients were grouped based on EGFR mutation results from histological and plasma ctDNA testing. Those with mutations detected by both methods were defined as the EGFRt+, p+ group, while those with mutations detected only by histology were defined as the EGFRt+, p− group. We had access to information that could identify individual participants during or after data collection, and personal data were de-identified before analysis. This experiment was approved by the IRB of The First Affiliated Hospital of Sun Yat-sen University (approval no. [2022]049). This study was conducted in accordance with the Declaration of Helsinki. Patient consent was waived for this retrospective design. According to the approval requirements of the Ethics Committee of First Affiliated Hospital of Sun Yat-sen University, this study is a retrospective study. And since all the patient data used are anonymous data, the Ethics Committee has approved that this study does not require the individual consent of the patients.
Tissue and Blood Sample Detection
All collected tissue specimens were soaked in 4% formaldehyde solution, then embedded and fixed into paraffin sections for NGS detection. Plasma DNA was analyzed using the Super-ARMS EGFR method. We collected 10 mL of body fluid samples from NSCLC patients and processed using a two-stage centrifugation method: first at 2000 × g for 10 min, followed by a second centrifugation at 8000 × g for 10 min. Samples with severe hemolysis or excessively high lipid levels are not usable. The resulting supernatant had a final volume of not less than 2 mL. Free DNA was extracted using the Body Fluid Free DNA Isolation Kit (Xiamen Aide Biomedical Technology Co., Ltd.). The concentration of the extracted DNA was determined by the Nano Drop 2000 Nucleic Acid and Protein Quantification Instrument. The OD260/OD280 ratio of the DNA should be between 1.8 and 2.0, and the OD260/OD230 ratio should be greater than 2. EGFR gene mutations were detected following the operating procedures, the reagent kit includes both internal and external quality control samples, as well as positive and negative controls, to conduct testing as per the instructions for the EGFR gene mutation quantitative detection kit with result interpretation based on the instruction manual. We used Super-ARMS to detect these text limited reference samples for 20 times. With 95% positive detection rate as the standard for determining the minimum detection limit, it was found that Super-ARMS could be detected normally when the mutated DNA concentration was as low as 0.2%.
18F-FDG PET/CT Image Acquisition and Analysis
PET/CT imaging was performed in 3D acquisition mode using a Gemini GXL 16 scanner (Philips, Best). The 18F-FDG PET tracer, provided by our cyclotron center (Cyclone 10/5Accelerator, IBA), had a radiochemical purity of over 95%. Patients fasted for at least 6 hours before receiving an intravenous injection of 5.55 MBq/kg of 18F FDG, followed by whole-body emission scanning. CT parameters were set to 120 kV, 100 mA, with collimation and slice spacing of 5.0/0.75 mm. PET imaging was performed in a row-by-row manner using the same position acquired in 3D mode. All images were independently assessed by two PET/CT physicians with 3–9 years of clinical diagnostic experience, without prior knowledge of clinicopathologic information. The inter-reader consistency was assessed using a statistical measure, kappa coefficient, to evaluate the agreement between the two PET/CT readers. In case of any disagreements, consensus was reached through discussion. For each site of involvement, including primary tumor, metastatic lymph nodes, and distant metastases, a region of interest (ROI) was carefully delineated around the suspected lesion site and the maximum standardized uptake value (SUVmax) was measured.
Data Collection
Retrospective data collection based on electronic medical records included patients’ age, sex, smoking status, tumor metastasis, tumor size, stage, tumor mutation typing, tumor markers, and treatment outcomes.
Treatment and Follow-up
All patients diagnosed with EGFR mutations were treated with EGFR-TKIs. The cutoff for data was 30/12/2022. Treatment efficacy data were collected, objective response rate (ORR) and progression-free survival (PFS) were calculated. PFS is defined as the time from treatment initiation to disease progression or death. ORR is the percentage of tumors that have shrunk or disappeared after tumor treatment is administered. ORR = [(Number of Complete Response (CR) cases + Number of Partial Response (PR) cases)/Total evaluable population] × 100%. The response of lung cancer to treatment is measured every three months using the RECIST criteria.
Statistical Analysis
All data were analyzed using SPSS26 and Graphpad8.0. Chi-square test and Fisher’s exact test were used to compare differences in categorical data between groups. Kaplan–Meier curves were drawn and Log rank test were used to compare survival rates. All univariate regression analyses with P value less than 0.1 were included in multivariate Cox proportional hazards model. The Cox proportional risk model was applied to estimate the hazard ratio (HR) for both multivariate and subgroup analyses. A two-sided P value of <0.05 was considered statistically significant.
Results
Patient Characteristics and the EGFR Mutation Status in Tissue and Plasma Samples
A total of 135 patients underwent both histological and plasm Super-ARMS mutation testing. There were 92 (68.1%, 0.595–0.760) patients in the EGFRt+, p+ group, and 43 (31.9%) patients in the EGFRt+, p− group. Using histological testing results for EGFR mutations as a reference, the sensitivity of Super-ARMS test was 68.1%. Notably, in patients with multiple metastatic NSCLC, the sensitivity of Super-ARMS EGFR testing can reach up to 85% (Supplementary Table 2). During the data collection process, no tissue negative but plasma positive patients were found. This indicates that in our study, the Super-ARMS did not produce any false positives. Univariate analysis indicated that patients with pleural effusion (P = 0.002), bone metastases (P = 0.004), liver metastases (P = 0.009) and multiple organ metastases (P = 0.005) had higher Super-ARMS detection sensitivity. Specific details were provided in Table 1 and detailed PFS curves were shown in Supplementary Figure 1. Furthermore, multivariate analysis demonstrated bone metastasis and CEA level were independent risk factors for positive EGFR ctDNA test in NSCLC (Supplementary Table 3).
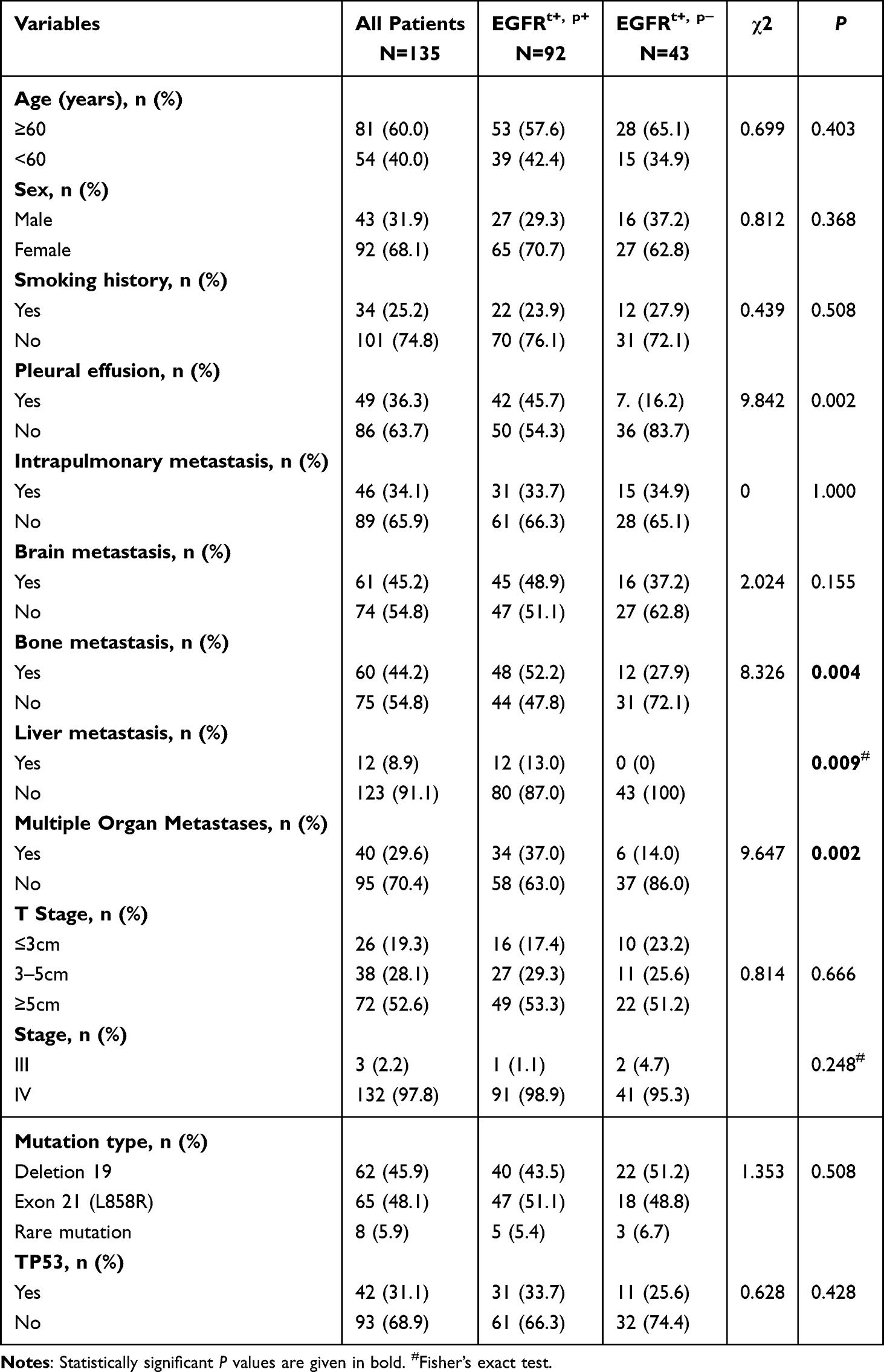 |
Table 1 Patient Characteristics |
Diagnostic and Prognostic Value of Tumor Markers
In order to evaluate the diagnostic efficacy of ctDNA for patients in the EGFRt+, p+ group, we constructed the receiver operating characteristic (ROC) curve and calculated the area under the ROC curve (AUC) of tumor markers in lung cancer. CEA demonstrated the highest accuracy in predicting ctDNA EGFR mutations (AUC 0.828, 95% CI 0.757–0.899, sensitivity 68.8%, specificity 84.4%, cutoff value 15.1) (Figure 1A). Further analysis categorized patients into high and low level groups based on cutoff value. Univariate analysis revealed that a high level of CEA or CFRA21-1 is associated with a poorer prognosis (P < 0.01) (Figure 1B and C), but CA125 at 44.3 had no predictive value for prognosis (Figure 1D) (P > 0.05).
 |
Figure 1 ROC curve analyses and PFS of patients. (A) The sensitivity and specificity of tumor markers for predicting the presence of plasm EGFR mutation in patients with NSCLC. (B) PFS of patients in CEA≥15.1 group and<15.1 group. (C) PFS of patients in CA125≥44.3 group and<44.3 group. (D) PFS of patients in CFRA21-1≥3.16 group and<3.16 group. The cutoff value is defined based on the Youden index. |
Diagnostic and Prognostic Value of SUVmax
In the 135 NSCLC patients who underwent plasm Super-ARMS testing, 60 had an 18F FDG PET/CT scan. To identify patients with an increased probability of plasm EGFR mutations, ROC curve analysis was performed (Figure 2A). The SUVmax of distant metastases (SUVmax(M)) was identified as a predictive marker for plasm EGFR gene mutation. However, combining SUVmax(T), SUV max(N) and SUVmax(M)), or combining SUVmax(M) and CEA did not significantly improve AUC. Survival analysis based on the cutoff value grouping shows that patients with lower SUVmax(M) have better PFS (P = 0.044) (Figure 2B).
 |
Figure 2 ROC curve analyses and PFS of patients. (A) The sensitivity and specificity of SUVmax for predicting the presence of plasm EGFR mutation in patients with NSCLC. (B) PFS of patients in SUVmax(M)<4.8 group and SUVmax(M)≥ 4.8 group. The cutoff value is defined based on the Youden index. |
Dynamics of ctDNA and Tumor Markers
There were 26 of 135 patients who underwent a second Super-ARMS test, with a median interval of 4.5 months between tests. We examined the relationship between ctDNA changes and serum biomarkers, and the waterfall plot demonstrated that patients with two consistent ctDNA tests had less variation in CEA levels compared to those with positive-negative or negative-positive transitions (Supplementary Figure 2), which suggested the magnitude of CEA change may predict alterations in the Super-ARMS assay.
The Prognostic Value of ctDNA Testing
In the univariate analysis, the median survival times were 23.4 months in the EGFRt+, p− group and 15.37 months in the EGFRt+, p+ groups. Compared to the EGFRt+, p+ group, the EGFRt+, p− group had a better PFS (P = 0.001) (Figure 3A). Meanwhile, EGFRt+, p− had a higher ORR than the EGFRt+, p+ group (P = 0.005) (Figure 3B). Moreover, after adjusted for other factors, positive EGFR ctDNA test still increased the risk of disease progression (P < 0.05) (Table 2). We further performed subgroup analysis on the EGFRt+, p+ group, the EGFRt+, p− group, and the forest plot is shown in the Figure 4. These results indicate that ctDNA test results have important prognostic value in NSCLC receiving EGFR-TKIs treatment.
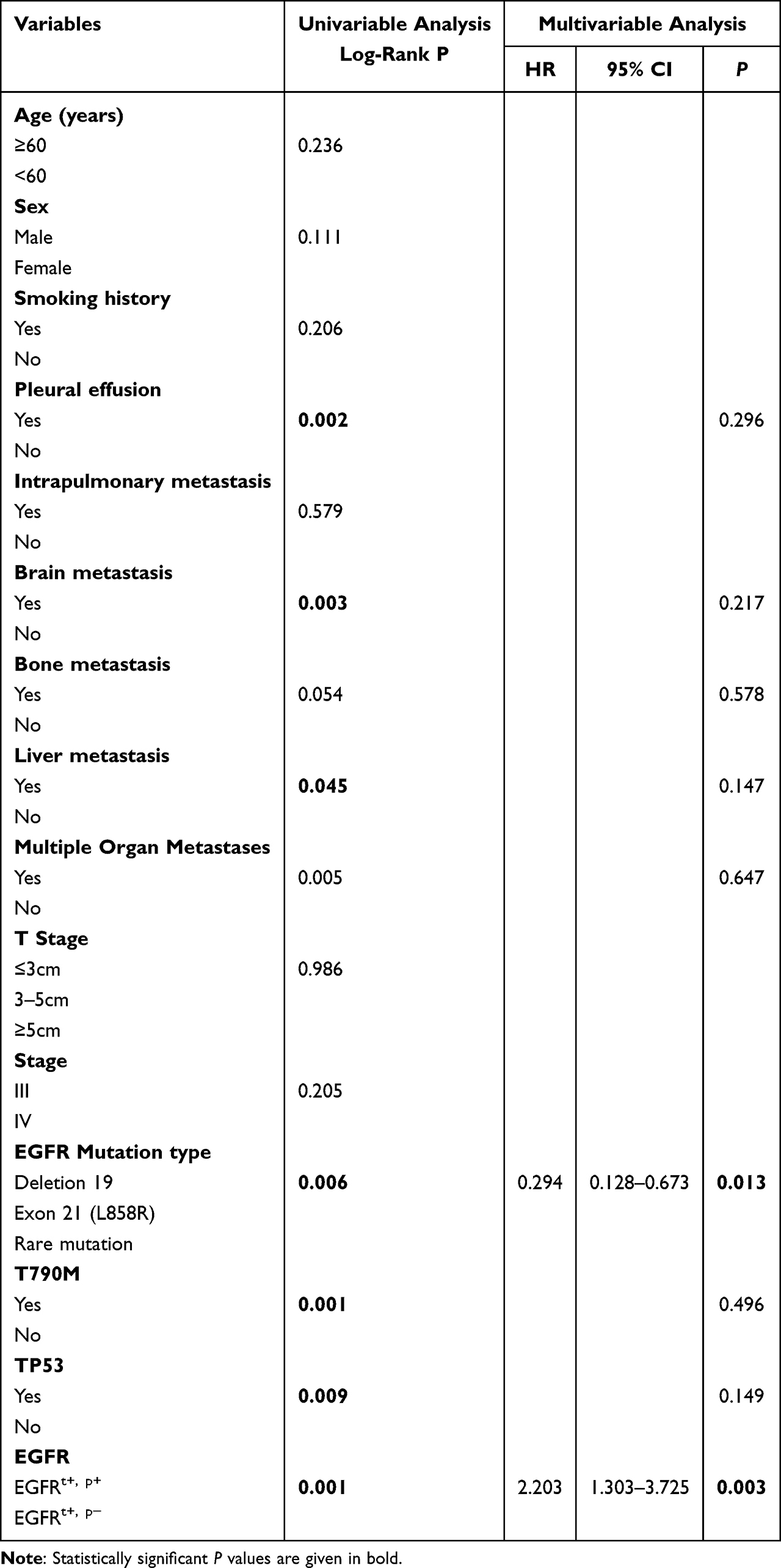 |
Table 2 Adjusted Association Between Patient Characteristics and PFS |
 |
Figure 3 PFS and ORR of patients. (A) PFS of patients in the EGFRt+, p+ group and EGFRt+, p− group. (B) ORR of patients in the EGFRt+, p+ group and EGFRt+, p− group. |
 |
Figure 4 A forest plot of HRs for PFS. |
The Prognostic Value of TP53 Mutation
In NSCLC, TP53 is the most commonly mutated gene. And our study showed that TP53 was an independent prognostic factor for PFS (P = 0.009) (Figure 5A). Furthermore, we included TP53 and EGFR mutation status in the stratified analysis. Patients were categorized into four groups: EGFRt+, p+ TP53 mutation group, EGFRt+, p+ TP53 wild group, EGFRt+, p− TP53 mutation group and EGFRt+, p− TP53 wild group, with median survival of 13.5 months, 12.13 months, 16.37 months and 26.93 months, respectively (Figure 5B). Further stratification showed that patients without TP53 mutation and in EGFRt+, p− group had better clinical outcomes compared to other patients (P < 0.001) (Figure 5C).
 |
Figure 5 Risk stratification by EGFRm status and TP53. (A) PFS of patients in the TP53 mutation group and TP53 wild type group. (B) PFS of patients in the EGFRt+, p+ TP53 mutation group, EGFRt+, p+ TP53 wild group, EGFRt+, p− TP53 mutation group and EGFRt+, p− TP53 wild group. (C) PFS of patients between the EGFRt+, p+ TP53 mutation group and others. |
Discussion
For advanced patients with NSCLC, EGFR-TKIs has become a standard treatment, significantly improving survival outcomes.28 Consequently, the detection of EGFR mutations is crucial. Although tissue biopsy is considered the gold standard for EGFR mutation detection,29 it also has many limitations.30 Liquid biopsy has emerged as a clinically valuable alternative that addresses these limitations and offers a more comprehensive tumor mutation profile.31 However, low tumor cell counts in liquid-based cell samples result in relatively low sensitivity for liquid biopsy, highlighting the urgent need to improve sensitivity. In our study, the sensitivity of Super-ARMS analysis for baseline patients was 68.1%, which is slightly lower than that of previous studies (71.4–79.5%) using tissue assays to detect EGFR mutations for targeted therapy in NSCLC.32,33 This may be related to the sample size and patient inclusion selection bias.
The factors affecting the sensitivity of fluid-based assays are of considerable interest. As in previous studies,34–39 we found that clinical indicators, including pleural effusion and organ metastasis were associated with higher assay sensitivity, likely due to the larger amounts of ctDNA released into the blood in these patients.40 As a result, when patients have metastases, particularly bone and multiple metastases, suggesting the presence of a large tumor load, liquid biopsy may be considered an alternative to tissue biopsy for detecting EGFR mutations in patients with NSCLC. However, liquid biopsy is not a substitute for diagnostic tumor tissue biopsy, and repeat tumor tissue biopsy is recommended when the ctDNA test is negative.
Additionally, elevated levels of tumor markers, including CFRA21-1, CA125, and particularly CEA, were linked to the increased Super-ARMS sensitivity. Symonds et al found a significant correlation between ctDNA levels and tumor biomarkers in colorectal cancer.41,42 However, research on the relationship between tumor biomarkers and ctDNA in lung cancer remains limited. Our study is the first to demonstrate that elevated levels of CEA, CFRA21-1, and CA125 are associated with high sensitivity in Super-ARMS testing in patients with NSCLC. These biomarkers can be used to predict positive detection. Additional ROC curve analysis reveals that tumor markers, specifically CEA, have significant diagnostic value in patients with positive Super-ARMS EGFR mutation tests. In the study of ctDNA dynamic changes, multiple studies have revealed that during tumor treatment response assessment, changes in ctDNA and tumor markers often occur synchronously or sequentially.43–45 Our research also demonstrated that the dynamic change in CEA levels had predictive value for ctDNA testing. These results indicate that the level of tumor markers and their dynamic changes have predictive value for ctDNA detection results. The elevation of tumor markers usually reflects an increase in tumor size, possibly associated with distant metastasis, abnormal angiogenesis, or metabolic activity. These changes may all be linked to the increased cellular DNA entering the bloodstream. Therefore, in clinical practice, patients with lung cancer and higher levels of tumor markers are more suitable for ctDNA testing. Several studies have found a correlation between SUVmax and EGFR mutation,1,46,47 although the results are not entirely similar. Ottestad et al found that ctDNA correlates with 18F-FDG PET/CT.40,48 Our study further indicated that the SUVmax level holds predictive significance for ctDNA detection. This may be associated with higher SUVmax levels in patients, indicating active cell proliferation and apoptosis. These processes lead to increased DNA fragmentation, subsequently enhancing plasma ctDNA abundance, although the underlying mechanism remains elusive.
Many studies have revealed that ctDNA is an indicator of prognosis in patients undergoing treatment.49,50 In this study, we concluded that the disparities between histology and plasma EGFR mutations could predict the prognosis of advanced patients with NSCLC undergoing EGFR-TKI treatment within a practical clinical context. This is consistent with the FLAURA study, which found that in NSCLC treated with osimertinib, the plasma ctDNA EGFRm-negative group observed a longer median progression-free survival compared to the plasma ctDNA EGFRm-positive group (23.5 versus 15.2 months).51 This may be linked to patients with ctDNA-positive exhibiting a higher tumor burden, more extensive tumor dissemination, and enhanced immune escape.
In NSCLC, TP53 is the most mutated gene, and our study revealed that TP53 mutation is associated with the prognosis of patients with lung cancer. Moreover, the combination of TP53 and EGFR mutations provided a more precise differentiation in prognosis, which was congruent with the results obtained in Xiao Liang’s study.35 This may be because individuals with TP53 mutations have disrupted apoptosis and increased genomic instability, which drives treatment resistance and tumor progression. Overall, combining TP53 plasma NGS and EGFR mutations using liquid biopsy optimizes the management of NSCLC.
Our study has certain limitations. First, it is a retrospective study with a relatively small sample size. Particularly, in the investigation focusing on assessing the relationship between the dynamic alterations of ctDNA and tumor markers, the sample quantity is insufficient. Hence, large-sample prospective cohort studies are warranted. Second, the follow-up duration is relatively brief, with the study endpoint being PFS rather than overall survival, potentially resulting in an inadequate comprehension of patients’ survival states. Finally, this study is a single-center retrospective one, and a selection bias exists during the enrollment of study subjects. For example, patients with tumors may have differences in their prior treatment history and tumor heterogeneity, factors that could lead to bias in the results. Prospective and controlled studies need to be conducted to preclude biases stemming from relevant confounding factors and to manage irrelevant variables.
Conclusions
Patients exhibiting metastasis, elevated levels of tumor markers and SUVmax are more suitable for plasma EGFR mutation testing. Moreover, a positive plasma ctDNA test not only guides targeted therapy but also predicts a worse prognosis.
Abbreviations
EGFR, Epidermal Growth Factor Receptor; ctDNA, Circulating Tumor DNA; NSCLC, Non-Small Cell Lung Cancer; CEA, Carcinoembryonic Antigen; SUVmax, Maximum Standardized Uptake Value; PFS, Progression-Free Survival; EGFR-TKIs, Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors; AUC, Area Under the Curve.
Data Sharing Statement
Availability of data and materials, the datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This experiment was approved by the IRB of The First Affiliated Hospital of Sun Yat-sen University (approval no. [2022]049). All procedures in the present study were conducted in accordance with the IRB of The First Affiliated Hospital of Sun Yat-sen University approved protocols.
Acknowledgments
This study was carried out in the Critical Care Medicine, The First Affiliated Hospital of Sun Yat-sen University, located at No.58 Zhongshan Er Road, Yuexiu District, Guangzhou, Guangdong Province, P.R. China.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data, took part in drafting the article or revising it critically for important intellectual content, agreed to submit to the current journal, gave final approval to the version to be published, and agree to be accountable for all aspects of the work.
Funding
The present study was supported by Guangdong Finance Foundation for Industrial Technology Research and Development (grant no. 20160907).
Disclosure
The authors declare that they have no competing interests.
References
1. Gao XC, Wei CH, Zhang RG, et al. (18)F-FDG PET/CT SUV(max) and serum CEA levels as predictors for EGFR mutation state in Chinese patients with non-small cell lung cancer. Oncol Lett. 2020;20(4):61. doi:10.3892/ol.2020.11922
2. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
3. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin. 2021;71(1):7–33. doi:10.3322/caac.21654
4. Subbiah V, Cote GJ. Advances in targeting RET-dependent cancers. Cancer Discov. 2020;10(4):498–505. doi:10.1158/2159-8290.CD-19-1116
5. Cho BC, Chewaskulyong B, Lee KH, et al. Osimertinib versus standard of care EGFR TKI as first-line treatment in patients with EGFRm advanced NSCLC: FLAURA Asian Subset. J Thorac Oncol. 2019;14(1):99–106. doi:10.1016/j.jtho.2018.09.004
6. Planchard D, Popat S, Kerr K, et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29(Suppl 4):iv192–iv237. doi:10.1093/annonc/mdy275
7. Hanna N, Johnson D, Temin S, et al. Systemic therapy for stage IV non-small-cell lung cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2017;35(30):3484–3515. doi:10.1200/JCO.2017.74.6065
8. Boumahdi S, de Sauvage FJ. The great escape: tumour cell plasticity in resistance to targeted therapy. Nat Rev Drug Discov. 2020;19(1):39–56. doi:10.1038/s41573-019-0044-1
9. Goldman JW, Noor ZS, Remon J, Besse B, Rosenfeld N. Are liquid biopsies a surrogate for tissue EGFR testing? Ann Oncol. 2018;29(suppl_1):i38–i46. doi:10.1093/annonc/mdx706
10. Overman MJ, Modak J, Kopetz S, et al. Use of research biopsies in clinical trials: are risks and benefits adequately discussed? J Clin Oncol. 2013;31(1):17–22. doi:10.1200/JCO.2012.43.1718
11. Gerlinger M, Rowan AJ, Horswell S, et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N Engl J Med. 2012;366(10):883–892. doi:10.1056/NEJMoa1113205
12. Chen Z, Fillmore CM, Hammerman PS, Kim CF, Wong KK. Non-small-cell lung cancers: a heterogeneous set of diseases. Nat Rev Cancer. 2014;14(8):535–546. doi:10.1038/nrc3775
13. Lokhandwala T, Bittoni MA, Dann RA, et al. Costs of diagnostic assessment for lung cancer: a medicare claims analysis. Clin Lung Cancer. 2017;18(1):e27–e34. doi:10.1016/j.cllc.2016.07.006
14. Abbosh C, Birkbak NJ, Wilson GA, et al. Phylogenetic ctDNA analysis depicts early-stage lung cancer evolution. Nature. 2017;545(7655):446–451. doi:10.1038/nature22364
15. Chaudhuri AA, Chabon JJ, Lovejoy AF, et al. Early detection of molecular residual disease in localized lung cancer by circulating tumor DNA profiling. Cancer Discovery. 2017;7(12):1394–1403. doi:10.1158/2159-8290.CD-17-0716
16. Dudley JC, Schroers-Martin J, Lazzareschi DV, et al. Detection and surveillance of bladder cancer using urine tumor DNA. Cancer Discovery. 2019;9(4):500–509. doi:10.1158/2159-8290.CD-18-0825
17. Garcia-Murillas I, Schiavon G, Weigelt B, et al. Mutation tracking in circulating tumor DNA predicts relapse in early breast cancer. Sci Trans Med. 2015;7(302):302ra133. doi:10.1126/scitranslmed.aab0021
18. Phallen J, Sausen M, Adleff V, et al. Direct detection of early-stage cancers using circulating tumor DNA. Sci Trans Med. 2017;9(403). doi:10.1126/scitranslmed.aan2415
19. Xu F, Wu J, Xue C, et al. Comparison of different methods for detecting epidermal growth factor receptor mutations in peripheral blood and tumor tissue of non-small cell lung cancer as a predictor of response to gefitinib. Onco Targets Ther. 2012;5:439–447. doi:10.2147/OTT.S37289
20. Taniguchi K, Uchida J, Nishino K, et al. Quantitative detection of EGFR mutations in circulating tumor DNA derived from lung adenocarcinomas. Clin Cancer Res. 2011;17(24):7808–7815. doi:10.1158/1078-0432.CCR-11-1712
21. Forshew T, Murtaza M, Parkinson C, et al. Noninvasive identification and monitoring of cancer mutations by targeted deep sequencing of plasma DNA. Sci Trans Med. 2012;4(136):136ra168. doi:10.1126/scitranslmed.3003726
22. Liang Z, Cheng Y, Chen Y, et al. EGFR T790M ctDNA testing platforms and their role as companion diagnostics: correlation with clinical outcomes to EGFR-TKIs. Cancer Lett. 2017;403:186–194. doi:10.1016/j.canlet.2017.06.008
23. Chen Y, Zhao X, Wang L, et al. Super-ARMS: a new method for plasma ESR1 mutation detection. Clin Chim Acta. 2021;520:23–28. doi:10.1016/j.cca.2021.05.021
24. Engelman JA, Zejnullahu K, Gale CM, et al. PF00299804, an irreversible pan-ERBB inhibitor, is effective in lung cancer models with EGFR and ERBB2 mutations that are resistant to gefitinib. Cancer Res. 2007;67(24):11924–11932. doi:10.1158/0008-5472.CAN-07-1885
25. He C, Wei C, Wen J, et al. Comprehensive analysis of NGS and ARMS-PCR for detecting EGFR mutations based on 4467 cases of NSCLC patients. J Cancer Res Clin Oncol. 2022;148(2):321–330. doi:10.1007/s00432-021-03818-w
26. Feng WN, Gu WQ, Zhao N, et al. Comparison of the SuperARMS and droplet digital PCR for detecting EGFR mutation in ctDNA from NSCLC patients. Transl Oncol. 2018;11(2):542–545. doi:10.1016/j.tranon.2018.02.007
27. Wu W, Cao Z, Zhang W, Zhang L, Hou L, Wu C. Comparison of the SuperARMS and ARMS for detecting EGFR mutations in liquid-based cytology specimens from NSCLC patients. Diagn Pathol. 2020;15(1):9. doi:10.1186/s13000-019-0910-5
28. Rolfo C, Mack PC, Scagliotti GV, et al. Liquid biopsy for advanced Non-Small Cell Lung Cancer (NSCLC): a statement paper from the IASLC. J Thorac Oncol. 2018;13(9):1248–1268. doi:10.1016/j.jtho.2018.05.030
29. Esagian SM, Grigoriadou G, Nikas IP, et al. Comparison of liquid-based to tissue-based biopsy analysis by targeted next generation sequencing in advanced non-small cell lung cancer: a comprehensive systematic review. J Cancer Res Clin Oncol. 2020;146(8):2051–2066. doi:10.1007/s00432-020-03267-x
30. Lim M, Kim CJ, Sunkara V, Kim MH, Cho YK. Liquid biopsy in lung cancer: clinical applications of circulating biomarkers (CTCs and ctDNA). Micromachines. 2018;9(3):100. doi:10.3390/mi9030100
31. Leighl NB, Page RD, Raymond VM, et al. Clinical utility of comprehensive cell-free DNA analysis to identify genomic biomarkers in patients with newly diagnosed metastatic non-small cell lung cancer. Clin Cancer Res. 2019;25(15):4691–4700. doi:10.1158/1078-0432.CCR-19-0624
32. Long C, Li K, Liu Z, et al. Real-world analysis of the prognostic value of EGFR mutation detection in plasma ctDNA from patients with advanced non-small cell lung cancer. Cancer Med. 2023;12(7):7982–7991. doi:10.1002/cam4.5582
33. Cao Z, Wang J, Qin N, et al. Clinical value of droplet digital PCR and super-ARMS detection of epidermal growth factor receptor gene mutation in plasma circulating tumor DNA of patients with advanced lung adenocarcinoma. Zhongguo fei ai za zhi. 2020;23(2):84–90. doi:10.3779/j.issn.1009-3419.2020.02.03
34. Lee H, Han J, Choi YL. Real-world analysis of the EGFR mutation test in tissue and plasma samples from non-small cell lung cancer. Diagnostics. 2021;11(9):1695. doi:10.3390/diagnostics11091695
35. Liang X, Zhang W, Li J, et al. Clinical implications of ctDNA for EGFR-TKIs as first-line treatment in NSCLC. J Cancer Res Clin Oncol. 2023;149(3):1211–1220. doi:10.1007/s00432-022-03952-z
36. Pender A, Hughesman C, Law E, et al. EGFR circulating tumour DNA testing: identification of predictors of ctDNA detection and implications for survival outcomes. Transl Lung Cancer Res. 2020;9(4):1084–1092. doi:10.21037/tlcr-19-581
37. Kuo CY, Lee MH, Tsai MJ, Yang CJ, Hung JY, Chong IW. The factors predicting concordant Epidermal Growth Factor Receptor (EGFR) mutation detected in liquid/tissue biopsy and the related clinical outcomes in patients of advanced lung adenocarcinoma with EGFR mutations. J Clin Med. 2019;8(11):1758. doi:10.3390/jcm8111758
38. Lee Y, Park S, Kim WS, et al. Correlation between progression-free survival, tumor burden, and circulating tumor DNA in the initial diagnosis of advanced-stage EGFR-mutated non-small cell lung cancer. Thorac Cancer. 2018;9(9):1104–1110. doi:10.1111/1759-7714.12793
39. Kim TM, Jung SH, An CH, et al. Subclonal genomic architectures of primary and metastatic colorectal cancer based on intratumoral genetic heterogeneity. Clin Cancer Res. 2015;21(19):4461–4472. doi:10.1158/1078-0432.CCR-14-2413
40. Jee J, Lebow ES, Yeh R, et al. Overall survival with circulating tumor DNA-guided therapy in advanced non-small-cell lung cancer. Nat Med. 2022;28(11):2353–2363. doi:10.1038/s41591-022-02047-z
41. Osumi H, Shinozaki E, Ooki A, et al. Correlation between circulating tumor DNA and carcinoembryonic antigen levels in patients with metastatic colorectal cancer. Cancer Med. 2021;10(24):8820–8828. doi:10.1002/cam4.4384
42. Symonds EL, Pedersen SK, Murray D, et al. Circulating epigenetic biomarkers for detection of recurrent colorectal cancer. Cancer. 2020;126(7):1460–1469. doi:10.1002/cncr.32695
43. Zheng J, Wang Y, Hu C, et al. Predictive value of early kinetics of ctDNA combined with cfDNA and serum CEA for EGFR-TKI treatment in advanced non-small cell lung cancer. Thorac Cancer. 2022;13(22):3162–3173. doi:10.1111/1759-7714.14668
44. Yang W, Zou J, Li Y, et al. Longitudinal circulating tumor DNA profiling in metastatic colorectal cancer during anti-EGFR therapy. Front Oncol. 2022;12:830816. doi:10.3389/fonc.2022.830816
45. Kruger S, Heinemann V, Ross C, et al. Repeated mutKRAS ctDNA measurements represent a novel and promising tool for early response prediction and therapy monitoring in advanced pancreatic cancer. Ann Oncol. 2018;29(12):2348–2355. doi:10.1093/annonc/mdy417
46. Ko KH, Hsu HH, Huang TW, et al. Value of 18F-FDG uptake on PET/CT and CEA level to predict epidermal growth factor receptor mutations in pulmonary adenocarcinoma. Eur J Nucl Med Mol Imaging. 2014;41(10):1889–1897. doi:10.1007/s00259-014-2802-y
47. Mak RH, Digumarthy SR, Muzikansky A, et al. Role of 18F-fluorodeoxyglucose positron emission tomography in predicting epidermal growth factor receptor mutations in non-small cell lung cancer. Oncologist. 2011;16(3):319–326. doi:10.1634/theoncologist.2010-0300
48. Ottestad AL, Johansen H, Halvorsen TO, et al. Associations between detectable circulating tumor DNA and tumor glucose uptake measured by (18)F-FDG PET/CT in early-stage non-small cell lung cancer. BMC Cancer. 2023;23(1):646. doi:10.1186/s12885-023-11147-z
49. Reichert ZR, Morgan TM, Li G, et al. Prognostic value of plasma circulating tumor DNA fraction across four common cancer types: a real-world outcomes study. Ann Oncol. 2023;34(1):111–120. doi:10.1016/j.annonc.2022.09.163
50. Guo K, Shao C, Han L, et al. Detection of epidermal growth factor receptor (EGFR) mutations from preoperative circulating tumor DNA (ctDNA) as a prognostic predictor for stage I-III non-small cell lung cancer (NSCLC) patients with baseline tissue EGFR mutations. Transl Lung Cancer Res. 2021;10(7):3213–3225. doi:10.21037/tlcr-21-530
51. Gray JE, Okamoto I, Sriuranpong V, et al. Tissue and plasma EGFR mutation analysis in the FLAURA trial: osimertinib versus comparator EGFR tyrosine kinase inhibitor as first-line treatment in patients with EGFR-mutated advanced non-small cell lung cancer. Clin Cancer Res. 2019;25(22):6644–6652. doi:10.1158/1078-0432.CCR-19-1126
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Establishment and Validation of a Predictive Nomogram for Postoperative Survival of Stage I Non-Small Cell Lung Cancer
Wang ZH, Deng L
International Journal of General Medicine 2022, 15:7287-7298
Published Date: 14 September 2022
Molecular Characteristics and the Effect of KRAS Mutation on the Prognosis of Immunotherapy in Non-Small Cell Lung Cancer in Xinjiang, China
Gu G, Yu B, Wan H, Lu S, Zhu X, Zhao Y, Fuxi Y, Liu C
OncoTargets and Therapy 2022, 15:1021-1032
Published Date: 21 September 2022
Prognostic Significance of Pretreatment Plasma D-dimer Levels in EGFR-Positive Advanced Non-Small Cell Lung Cancer Patients Receiving Osimertinib: A Multicentre Retrospective Study
Liu Q, Tan L, He J, Ning R, Zeng A, Chen Y
International Journal of General Medicine 2023, 16:5481-5491
Published Date: 23 November 2023