")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Budget Impact of Shifting the Treatment Setting of Unresectable Liver Metastases Associated with Primary Colorectal Cancer Using Y-90 Resin Microspheres from the Outpatient Hospital to the Office-Based Laboratory
Authors Sperling DC, Wallace K , von Oppen N, Weintraub JL
Received 19 September 2024
Accepted for publication 8 April 2025
Published 8 May 2025 Volume 2025:17 Pages 387—392
DOI https://doi.org/10.2147/CEOR.S492369
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Giorgio Lorenzo Colombo
David C Sperling,1 Katrine Wallace,2,3 Nanette von Oppen,2 Joshua L Weintraub1
1Department of Radiology, Columbia University Irving Medical Center, New York, NY, USA; 2Sirtex Medical, Woburn, MA, USA; 3School of Public Health, University of Illinois Chicago, Chicago, IL, USA
Correspondence: Katrine Wallace, School of Public Health, University of Illinois Chicago, 1601-3 W Taylor Street, MC 923, Chicago, IL, 60612, USA, Tel +1 773 551-5971, Email [email protected]
Purpose: In the wake of ever-increasing health care costs, solutions are sought to make health care more affordable, such as moving hospital outpatient procedures to office-based laboratory (OBL) settings. A budget impact model was constructed to estimate the health plan cost benefit of moving 50% of yttrium-90 resin microspheres (Y-90) selective internal radiation therapy (SIRT) procedures for unresectable liver metastases associated with primary colorectal cancer (CRC) from a traditional hospital outpatient setting (HOPPS) to an OBL setting.
Methods: The eligible population was estimated using an incidence-based approach for a hypothetical health plan with 1 million covered lives. Modeled costs were based on 2024 Medicare reimbursement rates. Three treatment scenarios were considered: 1) base case HOPPS, 2) hybrid (HOPPS/OBL), and 3) OBL settings. Budget impacts were estimated as the differences in annual total cost of treatment after switching 50% of Y-90 SIRTs from HOPPS to the hybrid (HOPPS/OBL) or OBL setting. Per-member-per-month (PMPM) budget impacts were also calculated. Sensitivity analyses were conducted by varying the proportions of patients shifting settings and the treatment setting they were shifting into.
Results: Annually, 28 patients were estimated to have metastatic CRC and unresectable liver metastases in a health plan of 1 million members. Average estimated per-patient cost savings would be $8,791 by switching one patient to a hybrid setting and $17,697 for a patient switched to the OBL. Switching 50% of eligible procedures resulted in PMPM cost benefits to the plan of $0.0102 for hybrid setting and $0.0206 for OBL. In sensitivity analyses, annual cost savings for the health plan were affected by both the proportion of patients shifted and the setting they were shifted into.
Conclusion: Shifting a percentage of the treatment of unresectable liver metastases with Y-90 SIRT to the OBL setting results in modest cost benefits for US health plans.
Plain Language Summary: • Due to the increasing costs of health care, simple changes that can reduce costs are sought.
• In this study, we created an economic model to determine if it would save money for US health insurance payors if half of the treatments for metastatic liver cancer, using a procedure called Y-90 selective internal radiation therapy (SIRT), were done in a doctor’s office instead of an outpatient hospital.
• The results showed that moving some of these treatments to the doctor’s office would save money for US health insurance plans.
• This finding could help to inform policy decisions to enable or expand payor funding channels for these types of procedures to be performed in doctor’s office settings.
Keywords: selective internal radiation therapy, mCRC, cost
Introduction
Colorectal cancer (CRC) was one of the top five most common cancers in 2023 for both incidence and mortality in the USA,1 and its incidence has been increasing in people under the age of 55 since the 1990s.2 Given this burden of disease, it is important that patients have access to therapeutic options across treatment settings.
Metastatic disease to the liver is the most common form of malignancy in CRC.3 Surgical interventions provide potentially curative options for selected patients, but most have unresectable tumors and are not eligible for surgery.4 Selective internal radiation therapy (SIRT) with yttrium-90 resin microspheres (Y-90) is indicated for the treatment of unresectable metastatic liver tumors from primary CRC in patients that are refractory to, or intolerant of, chemotherapy.5
It has been demonstrated that administering Y-90 SIRT in an office-based laboratory (OBL) setting is both feasible and efficient,6 but an analysis of the cost savings of switching from a traditional hospital outpatient setting (HOPPS) to the OBL setting has not been previously undertaken.
We developed a budget impact model (BIM) to assess the incremental effect on total health plan expenditures within a US health plan. This involved estimating the conversion of a percentage of Y-90 SIRTs for unresectable liver metastases associated with primary CRC from a HOPPS to either an OBL or hybrid HOPPS/OBL setting.
Methods
Ethics
Review and approval by an institutional review board or ethics committee was not required for this research as the study did not involve patient interventions or include patient data.
Model Inputs
The size of the CRC population of interest within the plan was estimated using an incidence-based approach for a hypothetical health plan with 1 million covered lives.
The US payor perspective was adopted in this analysis. Therefore, only reimbursed medical expenditures were included in the cost estimates. Modeled costs were based on 2024 published reimbursement rates from the Center for Medicare and Medicaid Services (CMS),7 and included treatment costs associated with imaging, product administration, staff time, and materials acquisition. Three treatment settings were considered in the model: 1) the HOPPS (base case), 2) the OBL setting and 3) a hybrid setting where the pre-treatment work-up occurred in the HOPPS but the Y-90 SIRT procedure was administered in the OBL setting.
As this BIM was created as a proof-of-concept model to demonstrate immediate cost benefits to private US payors of moving Y-90 SIRT procedures to a new setting of care, the time horizon utilized for this model was 1 budget year.
Budget Impact - Model Outputs
The base case of the BIM was defined as 100% of eligible patients receiving treatment in the HOPPS. Economic outcomes are provided as: 1) average reimbursement cost per patient in each of the three treatment settings, 2) per-patient average reimbursement cost difference after switching from the HOPPS to the OBL or hybrid setting, and 3) per-member-per-month (PMPM) budget impact to the whole health plan of switching 50% of eligible patients to the OBL or hybrid setting from a HOPPS. The budget impact, on a PMPM basis, was calculated as the total budget impact divided by the number of covered lives, divided by 12 months.
Sensitivity Analyses
One-way sensitivity analyses were performed to quantify the impact in response to changes in key variables (percentage of patients who shifted treatment settings, and the setting to which the patients shifted). Tornado diagrams were created to show the increase or decrease in incremental budget impact on a PMPM basis after both the treatment setting and the percentages of procedures shifted. The sensitivity analysis examined ±25% additional shifts in both treatment settings from the main base case analysis of 50% of patients switching settings.
Tornado diagrams were created to show the increase or decrease in incremental budget impact on a PMPM basis associated with either 25% switch (25% decrease from the base case) or 75% switch (25% increase in the base case) in the input value used in the model. The magnitude of the increase or decrease is shown in a single row in the tornado diagram and rows are sorted to show the change in the incremental PMPM budget impact associated with the change in the model input value.
Results
Budget Impact Analyses
In a hypothetical 1-million-member insurance plan, using an incidence-based approach, 28 patients annually were estimated to have metastatic unresectable CRC with liver-only metastases and were therefore eligible for Y-90 SIRT (Supplementary Table 1).8–18
Individual patient reimbursement costs for the HOPPS were $54,967 versus $46,176 in the hybrid setting and $37,270 in the OBL setting (Supplementary Table 2). The average per-patient reimbursement cost benefit to the plan of switching Y-90 SIRT procedures in the plan from the HOPPS to the hybrid setting was $8,791 and the average per-patient reimbursement cost benefit of switching eligible Y-90 SIRT procedures to an OBL setting was $17,697.
The base case scenario of 100% of eligible patients receiving Y-90 SIRT in the HOPPS is associated with an average total health plan expenditure of $1,533,891. The total plan expenditures after switching 50% of the base case to the alternative treatment settings would be $1,013,863 and $889,605, after switching to the hybrid and OBL settings, respectively. Switching 50% of the procedures from a traditional HOPPS setting to one of the alternative treatment settings was associated with modest PMPM cost savings for the plan, specifically a $0.0102 cost benefit for switches to the hybrid setting and a PMPM cost benefit of $0.0206 for switches to the OBL (Table 1).
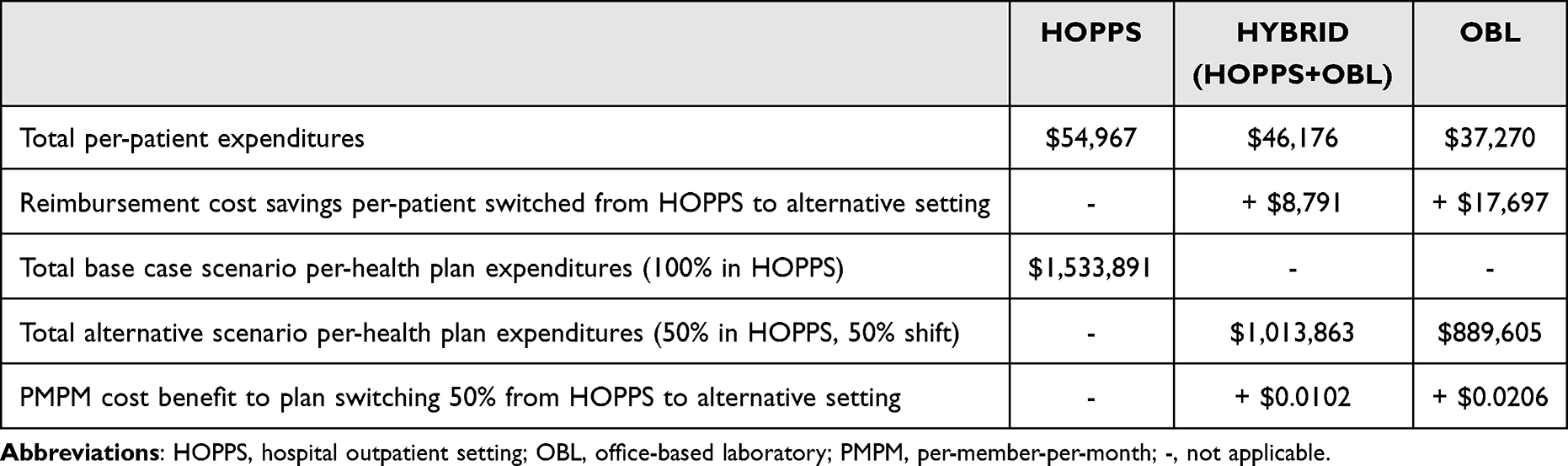 |
Table 1 Health plan expenditures and cost benefit to plan from switching 50% of Y-90 procedures from HOPPS to the hybrid (HOPPS/OBL) or OBL setting |
Sensitivity Analyses
Results of the one-way sensitivity analyses are presented in Figure 1, depicting the effect of varying the percentages of procedures shifting to each of two alternative treatment settings. Annual reimbursement cost savings for the health plan were affected by both the proportion of patients shifted and the treatment setting they were shifted into. In these sensitivity analyses, PMPM ranged from a cost benefit of $0.0051 for a 25% switch to a hybrid setting to $0.0309 for a 75% switch to an OBL setting. The higher the percentage of patients shifting resulted in a larger cost savings for the plan, and a greater percentage of patients shifting to the OBL setting over the hybrid setting also provided more cost benefit (Figure 1).
 |
Figure 1 Sensitivity analysis for change in average PMPM budget impact for varying treatment settings and proportion of switches. Abbreviations: HOPPS, hospital outpatient setting; OBL, office-based laboratory; PMPM, per-member-per-month. Notes: Change in PMPM budget impact from the base case (50% switch). Tornado diagrams were created to show the increase or decrease in incremental budget impact on a PMPM basis associated with either 25% switch (25% decrease from the base case) or 75% switch (25% increase in the base case) in the input value used in the model. The magnitude of the increase or decrease is shown in a single row in the tornado diagram and rows are sorted to show the change in the incremental PMPM budget impact associated with the change in the model input value. |
Discussion
In this study, we estimated the cost savings for a US payor generated by shifting a percentage of Y-90 SIRT procedures for unresectable liver metastases associated with primary CRC from a traditional HOPPS to an OBL setting. It has been demonstrated that administering Y-90 SIRT in the OBL setting is both feasible and efficient but an analysis of the cost savings of switching from a traditional HOPPS to the OBL setting has not been previously undertaken.6
This is also the first study to evaluate the hybrid setting, which is applicable to many OBL centers that do not have the single-photon emission computed tomography (SPECT)/computed tomography (CT) equipment onsite that is needed for the pre-treatment mapping of embolization procedures. We found that switching any amount of Y-90 SIRT procedures to one of the alternative treatment settings resulted in cost savings for the plan.
This model was developed according to established health economic guidelines,19 but we acknowledge a few limitations. The budget impact estimates are for a hypothetical 1-million-member health plan and may not be generalizable to other health plans. Results for an actual health plan may differ based on several factors, including the size of the treated patient population, costs of treatments and other health care resources, use of patient access restrictions (eg, cost-sharing, prior authorization), and market shares of treatments.
This analysis was done using 2024 CMS standard published rates,7 so it is an average scenario of Medicare reimbursement for the entire USA. Thus, this analysis is a conservative estimate, and may underrepresent the cost savings of switching to the OBL setting for other lines of business (eg, commercial insurance) or in higher-cost health care markets in the country.
Additionally, this model estimates the number of advanced-stage patients who would be potentially eligible for Y-90 SIRT based on existing US epidemiology incidence data. Other inclusion criteria such as the proportion of unresectable, liver-only metastases, are based on estimates from the literature. As such, patients selected for this analysis may not represent the totality of patients eligible for Y-90 SIRT in the USA.
Conclusions
BIMs are used to determine the financial impact of making a change (ie, a new drug, a new device, or in this case, a change of treatment setting) on the budgets of healthcare payors. This model found that shifting 50% of the treatment of unresectable liver metastases with SIRT with Y-90 resin microspheres to the OBL setting results in modest cost savings for US health plans, but shifting any percentage of these procedures will result in reimbursement cost savings for the plan.
Abbreviations
BIM, budget impact model; CMS, Center for Medicare and Medicaid Services; CRC, colorectal cancer; CT, computed tomography; HOPPS, hospital outpatient setting; OBL, office-based laboratory; PMPM, per-member-per-month; SIRT, selective internal radiation therapy; SPECT, single-photon emission computed tomography; Y-90, yttrium-90 resin microspheres.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Sirtex Medical.
Disclosure
Katrine Wallace and Nanette von Oppen were employees of Sirtex Medical at the time this study was undertaken. David C Sperling is a lecturer for Sirtex Medical and a consultant for Siemens Healthineers. Joshua L Weintraub is a proctor of SIR-Spheres (Sirtex Medical, Woburn, MA, USA). The authors report no other conflicts of interest in this work.
References
1. SEER. Cancer Stat Facts: common Cancer Sites. Available from: https://seer.cancer.gov/statfacts/html/common.html.
2. Cancer. Key Statistics for Colorectal Cancer. Available from: https://www.cancer.org/cancer/types/colon-rectal-cancer/about/key-statistics.html.
3. Tauriello DV, Calon A, Lonardo E, Batlle E. Determinants of metastatic competency in colorectal cancer. Mol Oncol. 2017;11(1):97–119. doi:10.1002/1878-0261.12018
4. Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review (CSR) 1975-2016. Available from: https://seer.cancer.gov/csr/1975_2016.
5. Sirtex. SIR-Spheres Package Insert. 2019. Available from: https://www.sirtex.com/media/55rprxv2/ssl-us-14-sir-spheres-microspheres-ifu-us.pdf.
6. Hickey RM, Maslowski JM, Aaltonen ET, et al. Yttrium-90 radioembolization in the office-based lab. J Vasc Interv Radiol. 2020;31(9):1442–1448. doi:10.1016/j.jvir.2020.05.002
7. CMS. 2024 Medicare Fee Schedule. Available from: https://www.cms.gov/medicare/physician-fee-schedule/search.
8. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–48. doi:10.3322/caac.21763
9. Bond MJG, Kuiper BI, Bolhuis K, et al. Intersurgeon variability in local treatment planning for patients with initially unresectable colorectal cancer liver metastases: analysis of the liver expert panel of the Dutch colorectal cancer group. Ann Surg Oncol. 2023;30(9):5376–5385. doi:10.1245/s10434-023-13510-7
10. Hackl C, Neumann P, Gerken M, Loss M, Klinkhammer-Schalke M, Schlitt HJ. Treatment of colorectal liver metastases in Germany: a ten-year population-based analysis of 5772 cases of primary colorectal adenocarcinoma. BMC Cancer. 2014;14(1):810. doi:10.1186/1471-2407-14-810
11. Isoniemi H, Uutela A, Nordin A, et al. Centralized repeated resectability assessment of patients with colorectal liver metastases during first-line treatment: prospective study. Br J Surg. 2021;108(7):817–825. doi:10.1093/bjs/znaa145
12. Kennedy AS, Ball D, Cohen SJ, et al. Multicenter evaluation of the safety and efficacy of radioembolization in patients with unresectable colorectal liver metastases selected as candidates for (90)Y resin microspheres. J Gastrointest Oncol. 2015;6(2):134–142. doi:10.3978/j.issn.2078-6891.2014.109
13. Kobayashi K, Inoue Y, Kitano Y, et al. Optimizing the selection of technically unresectable colorectal liver metastases. Surgery. 2023;173(2):442–449. doi:10.1016/j.surg.2022.10.013
14. Kumar R, Price TJ, Beeke C, et al. Colorectal cancer survival: an analysis of patients with metastatic disease synchronous and metachronous with the primary tumor. Clin Colorectal Cancer. 2014;13(2):87–93. doi:10.1016/j.clcc.2013.11.008
15. Patkar S, Chopde A, Shetty N, et al. Multimodality liver directed treatment for colorectal liver metastasis: array of complementary options can improve outcomes - A single centre experience from India. Front Oncol. 2023;13:1073311. doi:10.3389/fonc.2023.1073311
16. Van Cutsem E, Cervantes A, Adam R, et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol. 2016;27(8):1386–1422. doi:10.1093/annonc/mdw235
17. Villard C, Abdelrafee A, Habib M, et al. Prediction of survival in patients with colorectal liver metastases- development and validation of a prognostic score model. Eur J Surg Oncol. 2022;48(12):2432–2439. doi:10.1016/j.ejso.2022.06.021
18. Villard C, Habib M, Nordenvall C, Nilsson PJ, Jorns C, Sparrelid E. Conversion therapy in patients with colorectal liver metastases. Eur J Surg Oncol. 2021;47(8):2038–2045. doi:10.1016/j.ejso.2021.02.019
19. Husereau D, Drummond M, Augustovski F, et al. Consolidated health economic evaluation reporting standards 2022 (CHEERS2022) statement: updated reporting guidance for health economic evaluations. Available from: https://www.equator-network.org/reporting-guidelines/cheers/.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.