")
Back to Journals » Journal of Pain Research » Volume 17
Can Kinesiotaping Reduce Pain in Rib Fractures?: A Randomized Prospective Study
Authors Dal İ , Bektaş Ö, Kader S, Bodur G
Received 14 October 2024
Accepted for publication 10 December 2024
Published 12 December 2024 Volume 2024:17 Pages 4239—4247
DOI https://doi.org/10.2147/JPR.S500974
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Can Kinesiotaping Reduce Pain in Rib Fractures – Video abstract [500974]
Views: 79
İsmail Dal,1 Özgür Bektaş,2 Sibel Kader,3 Gözde Bodur3
1Department of Thoracic Surgery, Kastamonu University, Kastamonu, Turkey; 2Department of Physical Therapy and Rehabilitation, Kastamonu University, Kastamonu, Turkey; 3Department of Thoracic Surgery, Kastamonu Training and Research Hospital, Kastamonu, Turkey
Correspondence: İsmail Dal, Department of Thoracic Surgery, Kastamonu University, Kuzeykent, Ergenekon St. Nu: 9G1-1, City Center, Kastamonu, Turkey, Tel +905446533224, Email [email protected]
Introduction: The aim of this study is to investigate the effect of kinesiotaping on pain scores in patients with rib fractures following isolated thoracic trauma.
Materials and Methods: In this randomized prospective study, patients with isolated thoracic trauma and rib fractures were randomized into kinesiotaping and control groups between January 24, 2024, and October 1, 2024. Patients in the control group received standard analgesic treatment. In the kinesiotaping group, kinesiotaping bands were applied in addition to the standard treatment. Pain scores using the visual analog scale (VAS) were recorded at admission, the 24th hour, the 4th day, and the 7th day, and the results were statistically compared.
Results: A total of 118 patients were evaluated. Eighty-four patients did not meet the inclusion criteria. The 34 patients included in the study were randomized into kinesiotaping and control groups. The two groups were demographically homogeneous. On the 4th day, the mean VAS score was significantly lower in the kinesiotaping group (2.7 ± 1.2) compared to the control group (4.1 ± 1.9) (p = 0.037). No statistically significant difference in VAS scores was observed on the other days.
Conclusion: In patients with rib fractures, pain scores decreased more rapidly in those treated with analgesics plus kinesiotaping compared to those treated with analgesics alone.
Trial Registration: ClinicalTrials.gov, NCT06222320. Registered on January 15, 2024.
Keywords: rib fracture, pain, visual analog scale, kinesiotaping
Introduction
Thoracic trauma is common, and approximately 90% of all thoracic traumas are blunt traumas.1 In blunt thoracic traumas, the most frequently fractured bones are the ribs.1 Rib fractures are associated with acute and chronic pain, loss of work capacity, hemothorax, pneumothorax, pneumonia, and mortality.2 Rib fixation is indicated in cases of multiple rib fractures, where the stability of the thoracic wall is compromised, or when flail chest deformity causes paradoxical breathing. Surgical treatment is associated with longer hospital stays and higher costs.3 Conservative treatment is standard in uncomplicated rib fractures, with the goal of controlling pain and respiratory secretions.
Studies have shown that pain control using epidural analgesia, thoracic erector spinae block, or paravertebral block in rib fractures can reduce mortality.4–7 In the last decade, kinesiotaping has gained popularity as a method for managing pain associated with rib fractures. This technique was developed five decades ago by Kenzo Kase, drawing inspiration from traditional Japanese medicine.8 In kinesiotaping, a waterproof, elastic tape is applied to the patient’s skin. The tape is made of polymer elastic threads wrapped in 100% cotton fibers, nearly the same thickness as the epidermis, which helps to wick away moisture. The tape contains no medication, and its adhesive is activated by body heat. Theoretically, this method works through the gate control mechanism.9 The gate control mechanism suggests that stimulation of thick Aß sensory fibers from peripheral touch receptors suppresses pain signal transmission in the same area of the body.10 Additionally, kinesiotaping increases blood and lymphatic circulation and reduces muscle tension in the applied area.11
In recent years, conflicting results have been reported regarding the effectiveness of kinesiotaping for conditions such as rotator cuff-related shoulder pain,12 chronic wrist instability in athletes in sports like soccer, basketball, and volleyball,13–16 carpal tunnel syndrome,17 and thoracic trauma.18,19 However, the literature on kinesiotaping for thoracic trauma is extremely limited. In the US National Library of Medicine (NLM) database, two original articles on this topic were identified. In the study by Bakker et al,18 the effectiveness of kinesiotaping was investigated in a randomized prospective design. Nevertheless, the patient population in this study consisted of a heterogeneous group, with 6% of the patients having rib fractures. The other original article was conducted prospectively on patients with isolated rib fractures; yet, randomization was not applied.19
The aim of this study is to investigate the effect of kinesiotaping on pain scores in patients with rib fractures following isolated thoracic trauma, in a randomized and prospective manner.
Materials and Methods
Study Design
This randomized prospective study was conducted in the thoracic surgery department of our hospital between January 24 and October 1, 2024. Ethical approval was obtained from the university’s clinical ethics committee with the reference number 2023-KAEK-181 before the study began. The study was registered on ClinicalTrials.gov with the registration number NCT06222320 on January 15, 2024. The study was conducted in compliance with the Declaration of Helsinki.
Patient Selection
Adult patients with rib fractures resulting from acute isolated thoracic trauma were included in the study.
Patients with multiple traumas, an Injury Severity Index (ISI) >16, a Glasgow Coma Scale (GCS) <15, those who presented to the hospital more than 24 hours after the trauma, patients with fractures in the first three ribs, patients with hemothorax and/or pneumothorax requiring intervention, patients referred from other institutions, and those with cognitive or language impairments were excluded from the study.
Patients were recruited by the responsible investigator. The study protocol was explained to the patients verbally, and a visual summary of the study was also shown. Patients who signed the informed consent form were included in the study. The “integer generator” tool of the random.org website was used to create randomization blocks. Patients were randomly assigned to the “kinesiotaping” and “control” groups using these blocks.
Interventions and Measurement Method
In the control group, standard IV analgesic medications were administered, including paracetamol 1000 mg three times a day and dexketoprofen 50 mg twice a day. If necessary, tramadol 100 mg was administered. The same medical treatments were applied to the kinesiotaping group as well.Pain scores were measured using the visual analog scale (VAS). VAS scores were measured face-to-face at the time of admission, at 24 hours, on the 4th day, and on the 7th day. Measurements were conducted in the emergency room, clinic, and outpatient clinic by the ward nurse or the responsible investigator. Participants were presented with an assessment scale featuring facial expressions to express their pain levels. This scale was designed so that each facial expression represented a specific level of pain.20 On the scale, a “smiling face” indicated no pain, while a “very sad face” represented unbearable pain. Participants were asked to select the facial expression that best represented their current pain level.
The treatment protocol used in this study was developed by the authors based on current studies and practices in the literature.18,19 The kinesiotaping technique was consistently applied by a single expert physiotherapist. Kinesiotaping was performed within the first 24 hours after the trauma. First, the painful area was identified and marked (Figure 1a). The patient’s arm on the treated side was raised to ensure that the skin in the painful area was taut. If the area was moist, it was dried, and if there was hair, it was shaved. Two parallel strips of tape were applied (Figure 1b). No additional tension was applied to the skin during the application. Then, two more strips of tape were applied with 50% tension, surrounding the painful area (Figure 1c) (Figure 2). After the tape was applied, it was rubbed for a few seconds to activate the adhesive. The patient was instructed on how to remove the tape and was informed that it would be removed after four days. Since kinesiotaping strips can remain on the skin for 3–5 days without compromising adhesive quality, the strips were removed on the 4th day in patients. No re-taping was performed afterward. No experimental intervention was performed after the fourth day.
 |
Figure 1 Kinesiotaping technique. (a): The treatment area is being marked. (b) and (c): Kinesiotaping strips are being applied. |
 |
Figure 2 Image of a patient with kinesiotaping applied. |
Complications were systematically monitored through daily clinical evaluations, routine laboratory tests, and scheduled radiological assessments to ensure accuracy and consistency in data collection. Hemothorax was diagnosed based on a decrease in hemoglobin levels and the presence of newly developed pleural effusion, primarily assessed via posterior-anterior chest radiographs. When required, thoracic ultrasound was used for confirmation. Pneumonia was diagnosed using criteria including a body temperature ≥38°C, purulent sputum, typical pneumonic infiltrates observed on chest radiographs, and leukocytosis (≥10,000/mm³). Atelectasis was diagnosed based on typical findings observed on chest radiographs, with confirmation by computed tomography (CT) when deemed necessary.
Outcome Measures
The primary outcome measure of the study is the VAS scores on the 4th day post-trauma in both groups. Since the Kinesio tapes were removed after 4 days, this value was determined as the primary outcome variable.
The secondary outcome variables of the study were complications that developed in the patients, the length of hospital stay, and the Visual Analog Scale (VAS) scores assessed on the 1st and 7th days.
Statistical Analysis
Categorical data were presented as numbers and percentages, while continuous data were expressed as means and standard deviations (SD). The Independent Samples T-test and the Mann–Whitney U-test were used to compare continuous variables. The Chi-square and Fisher’s exact tests were used to analyze categorical data. A p-value of <0.05 was considered statistically significant.The sample size was calculated using a web-based application (ClinCalc LLC, 2024) prior to the initiation of the study. With 80% power and an alpha level of 0.05, the sample size was determined to be 16 patients for each group. Statistical analyses were performed using IBM SPSS Statistics version 23.0 (IBM Corporation, Armonk, NY, USA).
Results
A total of 118 patients were evaluated during the study period (Figure 3). Of these, 84 patients were excluded based on specific criteria. The reasons for exclusion were as follows: 34 patients were excluded due to having multiple trauma, 21 patients were excluded because their hospital admission occurred more than 24 hours after the traumatic event, and 13 patients were excluded because their Injury Severity Index (ISI) was greater than 16. Additionally, 5 patients were excluded due to fractures in the first three ribs, 5 patients were excluded because they had a Glasgow Coma Scale (GCS) score of less than 15, and 2 patients were excluded due to being referred from external centers. Two more patients were excluded because they had a chest tube inserted, one patient was excluded as they were incapacitated due to being deaf and mute, and another patient declined to participate. All patients completed the study.
 |
Figure 3 Patient Selection. |
After applying these exclusion criteria, 34 patients remained eligible for the study. These patients were randomly assigned to either the kinesiotaping group (n=17) or the control group (n=17). All patients completed the study.
The mean age was 58.5 ± 19.3 years in the kinesiotaping group and 58.8 ± 13.5 years in the control group, with no statistically significant difference (p=0.951). The baseline demographic data for both groups are summarized in Table 1.
 |
Table 1 Baseline Demographic and Clinical Characteristics of the Kinesiotaping and Control Groups |
No statistically significant differences were found between the two groups in terms of laboratory and biochemical test results (Table 2).
 |
Table 2 Laboratory and Biochemical Parameters of the Kinesiotaping and Control Groups |
The mean VAS score at the 24th hour was 4.6 ± 1.7 in the kinesiotaping group and 4.5 ± 1.9 in the control group, with no statistically significant difference (p = 0.786) (Table 3). However, on the 4th day, the mean VAS score was significantly lower in the kinesiotaping group (2.7 ± 1.2) compared to the control group (4.1 ± 1.9), showing a statistically significant difference (p = 0.037) (Figure 4). By the 7th day, the mean VAS score was 2.6 ± 1.4 in the kinesiotaping group and 2.5 ± 0.9 in the control group, with no statistically significant difference (p = 0.794).
 |
Table 3 Clinical Outcomes in the Kinesiotaping and Control Groups |
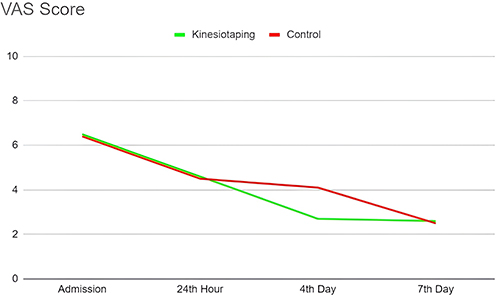 |
Figure 4 Comparison of VAS Scores Between Kinesiotaping and Control Groups. |
Complications were reported in 4 patients (23.5%) in the kinesiotaping group and in 3 patients (17.6%) in the control group, with no statistically significant difference (p = 1). In the kinesiotaping group, three patients developed hemothorax, which was not present at admission, and one patient developed atelectasis. In the control group, one patient developed both hemothorax and pneumonia (neither present at admission), one patient developed atelectasis, and another developed isolated pneumonia. None of the complications required invasive intervention, and antibiotic therapy was initiated for the patients with pneumonia.
Out of the 34 patients included in the study, only 1 patient required a total of 200 mg of IV tramadol, administered in 2 doses during hospitalization. The patient who needed to use tramadol was in the Kinesiotaping group. Aside from this, none of the patients required the use of opioid medications, either during their hospital stay or after discharge.
Discussion
In this study, it was found that pain scores were significantly lower on the 4th day in patients who received kinesiotaping after rib fractures. Additionally, kinesiotaping did not increase the length of hospital stay or complications.
Pain control is of primary importance in reducing pulmonary complications associated with rib fractures.21 It is well known that pain tends to decrease after the first two weeks of a rib fracture.22 Therefore, pain management is especially crucial during the acute phase. Various adjunctive methods are frequently investigated to provide early pain control in rib fractures alongside standard analgesic treatments. Kinesiotaping is one of the techniques used in the acute period to reduce pain from rib fractures. However, the literature on the application of kinesiotaping for rib fractures is limited.
In a case report by Köseoğlu Tohma et al,23 a 74-year-old frail patient with a fourth rib fracture developed after a sudden trunk rotation was treated with kinesiotaping. The patient’s pain was reported to have decreased following the application of kinesiotaping.
In the study by Akça et al, 30 patients with isolated rib fractures were prospectively examined.19 However, randomization was not applied, and the study focused on patients presenting to the emergency department without an indication for hospitalization, who were followed as outpatients. In this study, pain scores at the 15th minute and on the 4th day were significantly lower in the kinesiotaping group compared to the control group. Unlike this study, our research focused on a population of hospitalized patients with an indication for admission, the patients were randomized, and detailed blood tests were compared. Similar to Akça’s study, we also found lower pain scores on the 4th day in the kinesiotaping group.
In the randomized prospective study by Bakker et al, 57 patients completed the study.18 A more heterogeneous group of patients with shoulder and chest pain was selected. Only 6% of the randomized patients had a rib fracture, with the majority having a proximal humerus fracture (54.2%). In this study, pain scores were lower in the kinesiotaping group on the 4th day compared to the control group. However, unlike Akça’s study, no statistically significant difference in pain scores was found at the 15th minute. In our study, no measurement was taken at the 15th minute. The first measurement post-kinesiotaping was performed at the 24th hour. We found no significant difference in pain scores between the groups at the 24th hour.
Dedeoglu et al compared kinesiotaping plus sling with sling alone in clavicular shaft fractures.24 In this randomized prospective study, the time to return to work was significantly better in the kinesiotaping group. Constant score and American Shoulder and Elbow Surgeons (ASES) score were also better in the kinesiotaping group. This group showed better clinical functional outcomes and higher union rates.
In the randomized controlled single-blind study by Horoz et al, kinesiotaping was reported to reduce swelling and pain while improving functionality in distal radius fractures.25 In the study by Guasconi et al, the potential effect of kinesiotaping on reducing swelling in wrist fractures was investigated.26 In this clinical trial, which included a small patient population of 23 participants, it was reported that although not statistically significant, kinesiotaping might have a potential benefit in reducing swelling in the wrist by day 7.
Limitations
The study was conducted at a single center and involved patients who presented over a relatively short period of nine months. Additionally, there was only one thoracic surgeon working at the hospital at the time the study began. On days when the thoracic surgeon was on leave, patients were either referred to external centers or followed on an outpatient basis. As a result, some patients could not be evaluated for inclusion in the study. Moreover, none of the patients included in the study underwent rib fixation. Therefore, the effect of kinesiotaping in patients who receive rib fixation remains unknown. Another limitation of the study is the lack of blinding, which may have introduced bias into the evaluation of the outcomes.
Conclusion
The study demonstrated that patients who received kinesiotaping experienced a faster reduction in pain scores compared to those who were treated with analgesics alone.
Kinesiotaping has minimal cost, is well-tolerated by patients, and can be easily applied in clinical practice, both for hospitalized patients and during outpatient follow-ups in the emergency department.
In the future, studies with larger patient populations, conducted in multiple centers, and utilizing blinding are needed.
Data Sharing Statement
The raw data of the study can be shared upon reasonable request. The following anonymized patient data can be shared: age, gender, height, weight, smoking status, anticoagulant status, type of trauma, ISI score, number of fractured ribs, hemogram and biochemistry parameters, pain scores, complications, and length of hospital stay. These data will be shared indefinitely via a permanent DOI link. For access to the data, the responsible researcher can be contacted via Email at: [email protected].
Ethics Approval
Before the start of the study, approval was obtained from Kastamonu University Clinical Research
Ethics
Committee with the number 2023-KAEK-181.
Consent to Participate
Yes.
Funding
The authors did not receive support from any organization for the submitted work.
Disclosure
The researchers participating in the study do not have any conflict of interest.
References
1. Franssen AJPM, Daemen JHT, Luyten JA, et al. Treatment of traumatic rib fractures: an overview of current evidence and future perspectives. J Thorac Dis. 2024;16(8):5399–5408. PMID: 39268098; PMCID: PMC11388240. doi:10.21037/jtd-23-1832
2. Nathens A, Fantus R. National Trauma Data Bank 2010 Annual Report. Chicago: American College of Surgeons; 2010.
3. de Moya M, Nirula R, Biffl W. Rib fixation: who, what, when? Trauma Surg Acute Care Open. 2017;2(1):e000059. PMID: 29766079; PMCID: PMC5877892. doi:10.1136/tsaco-2016-000059
4. Jensen CD, Stark JT, Jacobson LL, et al. Improved outcomes associated with the liberal use of thoracic epidural analgesia in patients with rib fractures. Pain Med. 2017;18(9):1787–1794. doi:10.1093/pm/pnw199
5. Flagel BT, Luchette FA, Reed RL, et al. Half-a-dozen ribs: the breakpoint for mortality. Surgery. 2005;138(4):717–723. doi:10.1016/j.surg.2005.07.022
6. Simon B, Ebert J, Bokhari F, et al. Management of pulmonary contusion and flail chest: an Eastern association for the surgery of trauma practice management guideline. J Trauma Acute Care Surg. 2012;73(5):S351–S361. doi:10.1097/TA.0b013e31827019fd
7. Elawamy A, Morsy MR, Ahmed MAY. Comparison of thoracic erector spinae plane block with thoracic paravertebral block for pain management in patients with unilateral multiple fractured ribs. Pain Physician. 2022;25(5):483–490.
8. Kase K, Wallis J, Kase T. Clinical Therapeutic Applications of the Kinesio Taping Method. Tokyo: Ken’ikai Co. Ltd.; 2003.
9. Williams S, Whatman C, Hume PA, Sheerin K. Kinesio taping in treatment and prevention of sports injuries: a meta-analysis of the evidence for its effectiveness. Sports Med. 2012;42(2):153–164. doi:10.2165/11594960-000000000-00000
10. Drouin JL, McAlpine CT, Primak KA, Kissel J. The effects of kinesiotape on athletic-based performance outcomes in healthy, active individuals: a literature synthesis. J Can Chiropr Assoc. 2013;57(4):356–365.
11. Kinesio HK: The original from Dr. Kenzo Kaze since 1979. Available from: http://www.kinesiotaping.com/about/.
12. de Oliveira FCL, Pairot de Fontenay B, Bouyer LJ, Desmeules F, Roy JS. Kinesiotaping for the rehabilitation of rotator cuff-related shoulder pain: a randomized clinical trial. Sports Health. 2021;13(2):161–172. PMID: 32986531; PMCID: PMC8167348. doi:10.1177/1941738120944254
13. Biz C, Nicoletti P, Tomasin M, Bragazzi NL, Di Rubbo G, Ruggieri P. Is kinesio taping effective for sport performance and ankle function of athletes with chronic ankle instability (CAI)? A systematic review and meta-analysis. Medicina. 2022;58(5):620. PMID: 35630037; PMCID: PMC9146435. doi:10.3390/medicina58050620
14. Parreira PC, Costa LC, Hespanhol LC Jr, Lopes AD, Costa LO. Current evidence does not support the use of kinesio taping in clinical practice: a systematic review. J Physiother. 2014;60(1):31–39. doi:10.1016/j.jphys.2013.12.008
15. Wang Y, Gu Y, Chen J, et al. Kinesio taping is superior to other taping methods in ankle functional performance improvement: a systematic review and meta-analysis. Clin Rehabil. 2018;32(10):1472–1481. doi:10.1177/0269215518780443
16. Dolphin M, Brooks G, Calancie B, Rufa A. Does the direction of kinesiology tape application influence muscle activation in asymptomatic individuals? Int J Sports Phys Ther. 2021;16(1):135–144. doi:10.26603/001c.18799
17. Gräf JK, Lüdtke K, Wollesen B. Physio- und sporttherapeutische Interventionen zur Behandlung eines Karpaltunnelsyndroms: eine systematische Übersichtsarbeit [Physiotherapy and sports therapeutic interventions for treatment of carpal tunnel syndrome: a systematic review]. Schmerz. 2022. 36(4):256–265. German. PMID: 35286465; PMCID: PMC9300529. doi:10.1007/s00482-022-00637-x
18. Bakker ME, Bon VJJ, Huybrechts BPM, Scott S, Zwartsenburg MMS, Goslings JC. Kinesiotaping for acute pain due to uncomplicated traumatic injury of the shoulder or chest wall. Am J Emerg Med. 2022;58:197–202. PMID: 35700617. doi:10.1016/j.ajem.2022.05.057
19. Akça AH, Şaşmaz Mİ, Kaplan Ş. Kinesiotaping for isolated rib fractures in emergency department. Am J Emerg Med. 2020;38(3):638–640. PMID: 31937442. doi:10.1016/j.ajem.2019.11.049
20. Faiz KW. VAS--visuell analog skala [VAS--visual analog scale]. Tidsskr nor Laegeforen. 2014. 134(3):323. Norwegian. PMID: 24518484. doi:10.4045/tidsskr.13.1145
21. Simon BJ, Cushman J, Barraco R, et al. Pain management guidelines for blunt thoracic trauma. J Trauma Acute Care Surg. 2005;59(5):1256–1267. doi:10.1097/01.ta.0000178063.77946.f5
22. Karangelis D, Tagarakis G, Karkos C, et al. Rib fractures and pain peak 2 weeks down the line: myth or a fact? Am J Emerg Med. 2011;29(2):229. doi:10.1016/j.ajem.2010.09.005
23. Köseoğlu Tohma E, Özyemişçi Taşkıran Ö. Fragility fracture of the fourth rib in a patient with a cardiac pacemaker: an uncommon case. Arch Osteoporos. 2021;16(1):129. PMID: 34505183; PMCID: PMC8428503. doi:10.1007/s11657-021-00999-2
24. Dedeoglu SS, Imren Y, Karslioglu B, Keskin A, Atar S, Bilsel K. Kinesiotaping therapy for midshaft clavicular fractures: a randomised trial study. Acta Orthop Belg. 2022;88(1):143–150. PMID: 35512165. doi:10.52628/88.1.18
25. Horoz L, Cigdem-Karacay B, Cakmak MF. Effect of Kinesio taping on edema and wrist functions in patients with distal radius fracture followed conservatively with a cast: a randomized controlled single-blinded study. J Hand Ther. 2024;37(3):479–488. PMID: 38969599. doi:10.1016/j.jht.2024.05.003
26. Guasconi M, Zilli Riboni D, Civardi A, et al. The use of adhesive elastic tape for hand oedema control in patients with a wrist fracture treated in a cast: a pilot study. Int J Orthop Trauma Nurs. 2024;53:101059. PMID: 38261469. doi:10.1016/j.ijotn.2023.101059
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.